Embed Size (px)
Citation preview

www.elsevier.com/locate/braindev
Brain & Development 32 (2010) 244–247
Case report
Unilaterally and rapidly progressing white matter lesion andelevated cytokines in a patient with Tay–Sachs disease
Tomomi Hayase a, Jun Shimizu a, Tamako Goto a, Yasuyuki Nozaki a, Masato Mori a,Naoto Takahashi a, Eiji Namba b, Takanori Yamagata a,*, Mariko Y. Momoi a
a Department of Pediatrics, Jichi Medical University, 3311-1 Yakushiji, Shimotsuke, Tochigi 329-0498, Japanb Research Center for Bioscience and Technology, Tottori University, 86 Nishimachi, Yonago, Tottori 683-8503, Japan
Received 7 November 2008; received in revised form 25 December 2008; accepted 31 January 2009
Abstract
We report the case of a girl with Tay–Sachs disease who had convulsions and deteriorated rapidly after an upper respiratoryinfection at the age of 11 months. At the age of 16 months, her seizures became intractable and magnetic resonance imaging ofthe brain showed high signal intensity on T2-weighted images and marked swelling in the white matter and basal nucelei of the righthemisphere. Her seizures and right hemisphere lesion improved with glycerol and dexamethasone treatment. When dexamethasonewas discontinued, her symptoms worsened and lesions later appeared in the left hemisphere. Her cerebrospinal fluid showed elevatedlevels of the cytokines TNF-a and IL-5. It is considered that inflammation contributes to disease progression in Tay–Sachs disease.� 2009 Elsevier B.V. All rights reserved.
Keywords: Tay–Sachs disease; MRI; Dexamethasone; Cytokine; IL-5; TNF-a
1. Introduction
Tay–Sachs disease, GM2 gangliosidosis, is caused by adefect in hexosaminidase A. Enzyme activity deficiencyleads to accumulation of the substrate, GM2 ganglioside,in neuronal lysosomes, leading to cell death. Clinicalfeatures are deterioration starting in early infancy,hypersensitivity to sound, convulsions, bilateral cherry-red spots on the fundus of the eyes, and macrocephaly.The main magnetic resonance imaging (MRI) findingsare symmetrical high intensity on T2-weighted imagesof the basal ganglia and cortex; later, the white matterbecomes involved [1–5].
We report a patient with Tay–Sachs disease with aunilaterally and rapidly progressing white matter lesionand elevated cytokines in the cerebrospinal fluid (CSF).
0387-7604/$ - see front matter � 2009 Elsevier B.V. All rights reserved.
doi:10.1016/j.braindev.2009.01.007
* Corresponding author. Tel.: +81 285 58 7366; fax: +81 285 446123.
E-mail address: [email protected] (T. Yamagata).
2. Case report
The patient, a three-year-old girl and the first child ofnonconsanguineous parents, was born at 39 weeks ofgestation weighing 3160 g. Her eye fixation had beenpoor. After the age of 3 months, she showed hypersensi-tivity to sound. She could control her head after 4months of age and could sit without support at about10 months of age. After that, her development graduallydeteriorated and her smiles and responses decreased. At12 months, she showed acute deterioration following anupper respiratory infection with high-grade fever. Afterthat time, she could not sit or control her head. Fromthe age of 14 months, she showed frequent clonic hem-iconvulsions on her left side that did not respond to car-bamazepine. She was admitted to our hospital at 15months of age with a partial seizure that continued forseveral hours. On admission, she had no sign of infec-tion. Her body weight was 10.63 kg and her head cir-cumference was 48 cm (+1.53SD). Left-side-dominant

T. Hayase et al. / Brain & Development 32 (2010) 244–247 245
clonic convulsions of the limbs, lips, and eyelids wereobserved. Her muscles were hypotonic and she couldnot control her head or follow objects. Deep tendonreflexes were increased and horizontal nystagmus wereobserved. Hepatosplenomegaly was absent.
Tay–Sachs disease was diagnosed because leukocyteb-hexosaminidase A activity was 34.1 nmol/mg pro-tein/h (control range = 153–371 nmol/mg protein/h)and total leukocyte b-hexosaminidase activity was1474.9 nmol/mg protein/h (control range = 734–1628 nmol/mg protein/h). As well, the patient washomozygous for the G to T substitution at the spliceacceptor site in intron 5 of the b-hexosaminidase A gene(inv5,-1G to T/inv5,-1G to T).
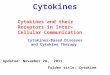
At the age of 14 months, the white matter and basalnuclei showed mildly high signal intensity on T2-weighted MR images and the thalamus showed lowintensity bilaterally (Fig. 1a). On admission at 15months, T2-weighted MR images showed swelling andhigh signal intensity in the white matter and basal nucleiof the right hemisphere and a midline shift to the leftside (Fig. 1b).
Fig. 1. T2-weighted MR images from a patient with Tay–Sachs disease. (a) Abasal nuclei and low intensity in the thalamus were seen bilaterally. (b) At 15matter and basal nuclei of the right hemisphere and a midline shift to the leftand dexamethasone. Swelling and high signal intensity on right hemisphere weintensity of the right white matter had worsened; basal nuclei showed swellinmatter of the left hemisphere showed marked swelling and high signal intensitAt 35 months of age. Diffuse high signal intensity in the white matter.
On admission, her white blood cell count was 18,000/ml, her hemoglobin was 11.1 g/dl, and her platelet countwas 41.9 � 104/ml. Serum aspartate aminotransferase(151 mU/ml) and lactate dehydrogenase (699 mU/ml)were elevated, whereas alanine aminotransferase was18 mU/ml. Serum creatinine phosphokinase was53 mU/ml, total protein was 6.4 g/dl, glucose was94 mg/dl, and total cholesterol was 205 g/dl. In theCSF, the cell count was 1/mm3 and protein was19 mg/dl; myelin basic protein was below 40.0 pg/ml.
Having received written informed consent from thepatient’s parents, we evaluated cytokine levels in theCSF of one week after dexamethasone treatment wasfinished by multiplex bead-based assay (Bio-PlexTM sus-pension array, Bio-Rad, Hercules, CA; Table 1). Con-trol data were the average levels of cytokines in theCSF of 10 patients with febrile convulsions. Interleukin(IL)-5 and tumor necrosis factor (TNF)-a were elevatedto 5.49 pg/ml (control average = 0.45 ± 0.16) and4.35 pg/ml (control average = 0.62 ± 0.22), respectively.Serum cytokines were not measured and CSF cytokineswere not followed after this.
t 14 months of age. Mildly high signal intensity in the white matter andmonths of age. Marked swelling and high signal intensity in the white
side were observed. (c) After the intravenous administration of glycerolre improved. (d) At the time of seizure relapse. Swelling and high signalg and high signal intensity bilaterally. (e) At 19 months of age. White
y. The right hemisphere lesion persisted but swelling was diminished. (f)

Table 1Concentrations of cytokines in the cerebrospinal fluid (CSF) of apatient with Tay–Sachs disease on admission to the hospital. The levelsof IL-5 and TNF-a were mildly elevated.
Cytokine Level (pg/ml) Average (pg/ml)IL-4 1.22 1.06 ± 0.44IL-6 3.70 3.23 ± 5.18IL-8 46.46 51.88 ± 41.07IL-10 0.50 0.88 ± 0.99GM-CSF 80.68 68.01 ± 17.43IFN-c 2.11 1.62 ± 1.12TNF-a 4.35 0.62 ± 0.22
IL-1b 0.34 0.28 ± 0.17IL-5 5.49 0.45 ± 0.16
IL-7 1.87 1.8 ± 0.7IL-12 2.82 1.18 ± 1.57IL-13 1.38 0.58 ± 0.36G-CSF 10.92 21.18 ± 18.4MCP-1 759.72 778.51 ± 461.71MIP-1b 40.30 33.68 ± 14.36
246 T. Hayase et al. / Brain & Development 32 (2010) 244–247
Intravenous phenytoin had no effect on her seizures;however, the frequency of her seizures decreased mark-edly following intravenous administration of 4 g/kg/dglycerol and 0.6 mg/kg/d dexamethasone, divided fourtimes (Fig. 2). Swelling and high signal intensity onT2-weighted images of the right hemisphere improved(Fig. 1c). Three weeks after dexamethasone and glycerolwere tapered off, frequent left-side partial seizuresreturned. At that time, the swelling and high signalintensity of the right white matter worsened, and bilat-eral basal nuclei showed swelling and high signal inten-sity (Fig. 1d).
Because she had an episode of sepsis and had recov-ered just before the worsening, steroids were not usedand glycerol was administered alone for 2 weeks. How-ever, her seizures did not improve and MR imagesshowed no changes. At the age of 19 months, white mat-ter of the left hemisphere showed marked swelling andhigh signal intensity on T2-weighted images, while theright hemisphere lesion persisted but swelling dimin-ished (Fig. 1e). At the age of 35 months, MRI showeddiffuse white matter high intensity on T2-weightedimages (Fig. 1f).
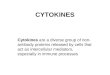
Fig. 2. Clinical course of the patient. CBZ, carbamazepine; PHT,phenytoin; ZNS, zonisamide. On the line of MRI, a–f indicate the dayof MRI examination of Fig 1a–f, respectively. � indicates the day ofCSF cytokine level examination.
3. Discussion
Several papers have reported MRI findings of GM2
gangliosidosis [1–5]: symmetrical T2 high intensity andT1 low intensity in the basal ganglia; caudate nucleus,globus pallidus and putamen, and T2 low intensityand T1 high intensity in the thalamus. With the progres-sion of the disease, the cortex, cerebellum, and whitematter show T2 high intensity symmetrically. Later, dif-fuse T2 high intensity in the white matter and cerebralatrophy are observed [2].
The pathological basis of these findings is consideredto be the accumulation of GM2 ganglioside within thecytoplasm of the neurons in the basal ganglia and thecerebral cortex, which induces neuronal cell body disten-sion and neuronal cell death [6]. After that, extensiveneural cell loss and white matter degeneration lead tobrain atrophy [1,2]. In our patient, the first MRI showedsome of these findings, such as T2 high intensity in thebasal ganglia and white matter and T2 low intensityand T1 high intensity in the thalamus. One month later,her brain MRI showed atypical findings of asymmetricalswelling and T2 high intensity in the white matter andbasal nucelei of the right hemisphere. These atypicalcourse of this patient was not originated from genotype,because the homozygous mutation of inv5,-1G to T onthe b-hexosaminidase A gene detected in this patientwas common mutation in Japanese Tay–Sachs patients[7]. Hemiconvulsion–hemiplegia–epilepsy (HHE) syn-drome shows similar MRI findings of cerebral hemi-sphere swelling. The proposed pathophysiologicalmechanism of the HHE syndrome is a neuronal injuryinduced by excitotoxicity and cytotoxic edema causedby a prolonged focal seizure [8]. In some types ofencephalopathy, cytokines were involved for diseaseprogression [9]. In our patient, exitotoxicity may takesome part to induce brain edema because she continuedpartial seizure for long time. However, effectiveness ofdexamethasone to reduce the swelling suggested thatinflammation, probably cytokines, contributed forhemisphere swelling in this patient. And we detectedthe elevation of TNF-a and IL-5 in the CSF. Becausethere was no sign of infection around the time of severehemisphere swelling (Fig. 1b), elevation of cytokineswere supposed to be induced relating to the pathophys-iology of Tay–Sachs disease.
It has been reported that inflammation contributes tothe progression of gangliosidosis in both patients andmouse models. Microglial activation and inflammatorycell infiltration were detected in the central nervous sys-tems (CNS) of autopsied patients and a murine modelof GM2 gangliosidosis in which progression of CNSinflammation parallels disease progression [10,11]. Ele-vated levels of TNF-a, transforming growth factor-1,and IL-1b were detected in the brain of the Sandhoffmodel mouse. The investigators postulated that accumu-

T. Hayase et al. / Brain & Development 32 (2010) 244–247 247
lated glycosphingolipid and fragmented cellular particlesaltered receptor signaling, thereby activating microglia/inflammatory cells and chronic inflammation. Cerebralcortex gene expression profiles of a Tay–Sachs and aSandhoff disease patient showed elevated expression ofclass II histocompatibility antigens and a large fractionof genes attributed to activated macrophages/microgliaand other inflammatory processes [12]. In Hexb�/�micethat were GM2 gangliosidosis (Sandhoff disease) modelmice, increased expression of MIP1a in the astrocyteswas accompanied by significant infiltration of macro-phage-like populations into the CNS [13,14]. An autoim-mune response in Hexb�/�mice has also been reported.Hexb�/�mice were positive for anti-ganglioside autoan-tibodies and showed an age dependent increase in autoan-tibody titers. It was suggested that material stored withinthe lysosomes of cells of Hexb�/� mice could trigger anautoimmune response [15]. IgG deposition was observedon the cell surface of neurons in the CNS of Hexb�/�mice. In addition, non-steroidal anti-inflammatory drugs(NSAIDs) were reported to delay disease progress inSandhoff disease mice [16].
In our patient, CSF levels of TNF-a and IL-5 weremildly elevated. TNF-a is involved in the induction ofacute inflammatory events and the transition to and per-sistence of chronic inflammation. IL-5 is mainly relatedto eosinophilic activation and allergy reaction [17,18].The contribution of IL-5 in this patient is unclear; how-ever, allergy reaction may have played some roles in theacute swelling that was reduced by glucocorticoid treat-ment. We could not analyze the level of MIP-1a in thispatient and the relationship between TNF-a, IL-5, andMIP-1a is not known.
Asymmetrical and reversible cerebral swelling, theeffectiveness of dexamethasone for treating this lesion,the elevation of TNF-a and IL-5 in the CSF, and herrapid deterioration following a viral infection suggestthat inflammation contributed to disease progress in thispatient. In order to elucidate the contribution of inflam-mation to GM2 gangliosidosis, future studies shouldevaluate the levels of cytokines in the CSF of thesepatients and assess the patients’ responses to glucocorti-coid and NSAID therapy.
References
[1] Assadi M, Baseman S, Janson C, Wang DJ, Bilaniuk L, Leone P.Serial 1H-MRS in GM2 gangliosidoses. Eur J Pediatr2008;167:347–52.
[2] Mugikura S, Takahashi S, Higano S, Kurihara N, Kon K,Sakamoto K. MR findings in Tay–Sachs disease. J Comput AssistTomogr 1996;20:551–5.
[3] Fukumizu M, Yoshikawa H, Takashima S, Sakuragawa N,Kurokawa T. Tay–Sachs disease: progression of changes onneuroimaging in four cases. Neuroradiology 1992;34:483–6.
[4] Ozkara HA, Topcu M. Sphingolipidoses in Turkey. Brain Dev2004;26:363–6.
[5] Yoshikawa H, Yamada K, Sakuragawa N. MRI in the early stageof Tay–Sachs disease. Neuroradiology 1992;34:394–5.
[6] Huang JQ, Trasler JM, Igdoura S, Michaud J, Hanal N, GravelRA. Apoptotic cell death in mouse models of GM2 gangliosidosisand observations on human Tay–Sachs and Sandhoff diseases.Hum Mol Genet 1997;6:1879–85.
[7] Tanaka A, Sakuraba H, Isshiki G, Suzuki K. The major mutationamong Japanese patients with infantile Tay–Sachs disease aG-to-T transversion at the acceptor site of intron 5 of the beta-hexosaminidase alpha gene. Biochem Biophys Res Commun1993;30:539–46.
[8] Auvin S, Devisme L, Maurage CA, Soto-Ares G, Cuisset JM,Leclerc F, et al. Neuropathological and MRI findings in an acutepresentation of hemiconvulsion–hemiplegia: a report with path-ophysiological implications. Seizure 2007;16:371–6.
[9] Mizuguchi M, Yamanouchi H, Ichiyama T, Shiomi M. Acuteencephalopathy associated with influenza and other viral infec-tions. Acta Neurol Scand 2007;115(Suppl 186):45–56.
[10] Jeyakumar M, Thomas R, Elliot-Smith E, Smith DA, van derSpoel AC, d’Azzo A, et al. Central nervous system inflammationis a hallmark of pathogenesis in mouse models of GM1 and GM2gangliosidosis. Brain 2003;126:974–87.
[11] Wada R, TiVt CJ, Proia RL. Microglial activation precedes acuteneurodegeneration in Sandhoff disease and is suppressed by bonemarrow transplantation. Proc Natl Acad Sci USA 2000;97:10954–9.
[12] Myerowitz R, Lawson D, Mizukami H, Mi Y, Tifft CJ, Proia RL.Molecular pathophysiology in Tay–Sachs and Sandhoff diseasesas revealed by gene expression profiling. Hum Mol Genet2002;11:1343–50.
[13] Tsuji D, Kuroki A, Ishibashi Y, Itakura T, Kuwahara J,Yamanaka S, et al. Specific induction of macrophage inflamma-tory protein 1-alpha in glial cells of Sandhoff disease model miceassociated with accumulation of N-acetylhexosaminyl glycocon-jugates. J Neurochem 2005;92:1497–507.
[14] Wu YP, Proia RL. Deletion of macrophage-inflammatory protein1 alpha retards neurodegeneration in Sandhoff disease mice. ProcNatl Acad Sci USA 2004;101:8425–30.
[15] Yamaguchi A, Katsuyama K, Nagahama K, Takai T, Aoki I,Yamanaka S. Possible role of autoantibodies in the pathophys-iology of GM2 gangliosidoses. J Clin Invest 2004;113:200–8.
[16] Jeyakumar M, Smith DA, Williams IM, Borja MC, Neville DC,Butters TD, et al. NSAIDs increase survival in the Sandhoffdisease mouse: synergy with N-butyldeoxynojirimycin. Ann Neu-rol 2004;56:642–9.
[17] Rothenberg ME, Hogan SP. The eosinophil. Annu Rev Immunol2006;24:147–74.
[18] Itakura A, Kikuchi Y, Kouro T, Ikutani M, Takaki S, AskenasePW, et al. Interleukin 5 plays an essential role in elicitation ofcontact sensitivity through dual effects on eosinophils and B-1cells. Int Arch Allergy Immunol 2006;140(Suppl 1):8–16.