Embed Size (px)
Citation preview
University of Groningen
Hydrocephalus shuntsMetzemaekers, Joannes Dionysius Maria
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:1998
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Metzemaekers, J. D. M. (1998). Hydrocephalus shunts: a clinical and laboratory study. Groningen: s.n.
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 21-03-2020

HYDROCEPHALUS SHUNTS
A clinical and laboratory study
This study was financially supported by grants from: Het Van Leersumfonds, Biomedic, Codman, Cordis and Promedics.
Hydrocephalus shunts. A clinical and laboratory study.Jan D.M. Metzemaekers, GroningenThesis University Groningen
ISBN 90-367-0975-xNUGI 743
© Copyright 1998 by Jan D.M. Metzemaekers, GroningenAll rights reserved. No part of this book may be reproduced in any form or by any electronic ormechanical means, including information storage and retrieval systems, without permission in writ-ing from the publisher.
Typesetting : COMPUTEKST grafische tekstverwerking, GroningenPhototypesetting : PEACH belichtingsstudio bv, GroningenPrinting : Dijkhuizen Van Zanten bv, Groningen
II

RIJKSUNIVERSITEIT GRONINGEN
HYDROCEPHALUS SHUNTS
A CLINICAL AND LABORATORY STUDY
Proefschrift
ter verkrijging van het doctoraatin de Medische Wetenschappen
aan de Rijksuniversiteit Groningenop gezag van de Rector Magnificus Dr. D.F.J. Bosscher
in het openbaar te verdedigen op woensdag 30 september 1998
om 14 .45 uur
door
Joannes Dionysius Maria Metzemaekers
geboren op 14 november 1957te Breda

Promotores Prof. dr. J.J.A. MooijProf. dr. J.W.F. BeksProf. dr. K.G. Go
Referent Dr. Ir. H.L. Journée

Promotiecommissie Prof. dr. D.A. BoschProf. dr. J.H.A. De KeyserProf. dr. R.P. Zwierstra
Paranimfen Monique Metzemaekers & Maarten Coppes

Contents
Chapter 1 General introduction page1.1 Introduction 11.2 History of the surgical treatment for hydrocephalus 2
Chapter 2 Clinical study on hydrocephalus shunts 42.1 General data 42.1.1 Patients and data collection 42.1.2 Etiology of hydrocephalus and most prevalent pre-operative symptoms 42.1.3 Surgical procedure 42.1.3.1 Surgeon 42.1.3.2 Duration of operative procedure 52.1.3.3 Drainage route 62.1.3.4 Peri-operative antibiotics 62.1.4 Shunt systems 62.1.4.1 Valves 62.1.4.2 Shunt components 62.1.5 Pre-operative external ventricular drainage 62.1.6 Cerebrospinal fluid analysis 62.1.7 Statistical analysis 8
2.2 Results 82.2.1 Number of revisions and interval until revision 82.2.2 Causes of shunt dysfunction 82.2.2.1 Proximal dysfunction 82.2.2.2 Valve dysfunction 92.2.2.3 Distal dysfunction 92.2.2.4 Infection 92.2.2.4.1 Definition of infection 92.2.2.4.2 Epidemiology of infection 102.2.2.4.3 Treatment of infection 112.2.2.4.4 Peri-operative antibiotics and infection 112.2.3 Revisions and etiology of hydrocephalus 112.2.4 Surgical procedure and revision rate 122.2.4.1 Surgeon 122.2.4.2 Duration of operative procedure 122.2.4.3 Drainage route 122.2.5 Shunt system and first revision 122.2.5.1 Valves 122.2.5.2 Shunt components 142.2.6 CSF composition and revision 152.2.7 Morbidity 162.2.8 Mortality 16
VII
2.3 Discussion 182.3.1 Shunt revision rate per patient 192.3.2 Causes of shunt dysfunction 192.3.2.1 Proximal dysfunction 192.3.2.2 Valve dysfunction 202.3.2.3 Distal dysfunction 202.3.2.4 Infection 202.3.2.4.1 Infection and epidemiology 202.3.2.4.2 Treatment of infection 212.3.2.4.3 Prevention of infection 222.3.3 Revisions in various age groups 232.3.4 Revisions related to underlying etiology of hydrocephalus 232.3.5 Operative procedure and incidence of shunt revisions 242.3.5.1 Surgeon 242.3.5.2 Duration of the surgical procedure 242.3.5.3 Drainage route 242.3.6 Shunt system versus revision 242.3.6.1 Valves 242.3.6.2 Shunt components 262.3.7 Cerebrospinal fluid composition versus revision operations 272.3.8 Morbidity 272.3.9 Mortality 28
2.4 Conclusions 292.4.1 Summary of previous conclusions 29
2.5 Future directions 30
Chapter 3 Cerebrospinal fluid dynamics and hydrocephalus shunts 313.1 Cerebrospinal fluid dynamics 313.1.1 CSF flow and production 313.1.2 CSF absorption 323.1.3 CSF composition 323.1.4 Pressure in CSF and other compartments 33
3.2 Pressure, resistance and flow in a shunt system 343.2.1 Pressure 343.2.2 Flow 353.2.3 Resistance 353.2.3 Viscosity 353.2.4 Siphoning 363.2.5 Measuring flow in shunt systems 36
3.3 Shunt materials 37
VIII
3.4 Valve mechanics and valve types 383.4.1 Valve mechanics 383.4.2 Valve types most commonly used in our clinical study 40
3.5 Protein concentration and shunt functioning 41
3.6 Blood and shunt functioning 43
Chapter 4 Laboratory study on hydrocephalus shunt valves 444.1 Valve testing in a laboratory setting 444.1.1 Methods and materials 444.1.1.1 Tested valves 444.1.1.2 Pump-driven versus pressure-driven test rigs 464.1.1.3 Conditions for in vitro testing of shunt valves 464.1.1.4 Test rig set-up 474.1.1.5 Flow generator 484.1.1.6 Pressure modulation unit 484.1.1.7 Pressure measurements 504.1.1.8 Flow resistance devices 504.1.1.9 Prevention of air bubbles 514.1.1.10 Composition of test solutions 514.1.1.11 Recording protocol 514.1.1.12 Data-processing 534.1.2 Results 544.1.2.1 Valves 544.1.2.2 Pressure diagrams per valve type 544.1.2.3 Results per valve 554.1.2.4 Dynamical properties 57
4.2 Discussion 624.2.1 Summary of test results 624.2.2 Performance (saline) compared to the manufacturer’s specifications 644.2.3 Effect of protein on valve performance 654.2.4 Effect of red blood cells on valve functioning 654.2.5 Opening characteristics 664.2.6 Closing characteristics 664.2.7 Effect of modulation 674.2.8 Concluding remarks 68
4.3 Conclusions 69
Chapter 5 General discussion 705.1 Comparison between clinical and laboratory results 70
5.2 Future recommendations 71
IX
Appendix APressure diagrams per valve 75
Appendix BDynamical characteristics 83
Summary 91
Samenvatting 95
References 99
Nawoord 105
Curriculum Vitae 107
X
Chapter 1 General introduction
1.1 Introduction
In the Netherlands, about 650 cerebrospinal fluid (CSF) shunt insertions for hydrocepha-lus and about 500 shunt revisions take place each year127. Therefore, the treatment ofhydrocephalus consitutes an important part of the neurosurgical practice. At the begin-ning of this study there was a meeting of Dutch Neurosurgeons, where it became clearthat there was hardly any communication between surgeons about the treatment of hydro-cephalus. There was no clear overview of the shunt systems that were used and the com-plications that occurred. The choice for a certain system was based on remarks such as:‘this system is easy to work with’ and ‘I hardly see any complications of this system inpractice’. Furthermore, there was no consensus on the surgical technique and the implica-tions of raised protein and erythrocyte concentrations in the CSF. The need for a multi-centre clinical study on the functioning of CSF shunts was obvious.
From December 1989 until January 1992 data were collected on 400 patients undergo-ing primary shunt insertions for hydrocephalus. These patients were recruted from eightneurosurgical centres. The follow-up period of these patients was at least two and a halfyears. Next to this clinical study, a laboratory study was conducted in which the eight mostfrequently inserted hydrocephalus valves from the clinical study were tested in severalways.
The aim of the study is:* to give an overview of shunt systems used in Dutch neurosurgery and their concomi-
tant complications* to show if increased protein or erythrocyte concentrations in a laboratory setting
impair valve performance compared to the performance during perfusion with saline,and, to compare the results of saline perfusion with the manufacturer’s specifications.
* to find a correlation between the properties of the valve as found in the laboratory andthe behavior of the valves in clinical practice.
1
1.2 History of surgical treatment for hydrocephalus
The only reliable therapy for progressive hydrocephalus has been surgery. Since theadvent of neurological surgery late in the 19th century, the removal of intracranial massleasions such as tumors and developmental cysts has produced cures in a limited numberof selected patients. Simultaneously with the attempt to cure the condition, the develop-ment of many ingenious procedures to divert the CSF to effective absorptive sites origi-nated87. Ventricular puncture was nearly always followed by death in the 18th century.Lumbar puncture, first described by Quincke in 1891 as a treatment for hydrocephalus104,has survived till today, not only as a diagnostic procedure but as a temporary measure forthe management of communicating hydrocephalus. Carotid artery ligation was recom-mended by Fraser and Dott (1922)57 and Dandy (1918)35 introduced choroid plexectomyin an attempt to reduce CSF formation. Putnam103 and Scarf111 introduced endoscopiccoagulation of the plexus which was applied widely before 1950. In order to avoid infection, closed ventricular drainage was already attempted near theend of the 19th century. The fluid was usually diverted to the subcutaneous or subduralspaces. Miculicz used a ”nail” of glasswool, others used gold tubes, catgut or linenstrands, gold and glass tubes, rubber tubes or coiled siver wires37. Drainage to the vascu-lar system was pioneered by Payr in 1908 using autologous or homologous donor veins tothe sagittal sinus and later tot the jugular vein97.Third ventriculostomy was introduced to bypass the obstruction of CSF flow due to aque-duct occlusion. Dandy described the procedure that opened the floor of the third ventriclefrom a subfrontal approach which required division of an optic nerve in 192236. Later onhe modified the technique performing a lateral subtemporal approach by which the floorof the third ventricle behind the infundibulum could be opened directly to the interpedun-cular cistern. This approach reduced mortality to 15%. Torkildsen introduced intracranialCSF diversion with small plastic or rubber tubes from the lateral ventricles extra-cranial-ly and subcutaneously back to the cisterna magna, as early as before 1939122. And al-though 6 of the original 13 patients died, subsequent authors described improved succesrates43.An extensive experience with ventricular and lumbar subarachnoid shunting to the uretherwas reported by Matson in 1949 and 195682,83. Although there was no operative mortal-ity, the procedure required a nefrectomy. Complications, both obstructive and infectious,and the predisposition of patients to dehydration and electrolyte imbalance, limited itsapplication and dictated eventual abdominal or atrial drainage. In 1945 methylsilicones were found to be remarkably inert within biologial systems andthe Dow Corning formulation of silicone elastomer (Silastic) was found to be particular-ly useful6. Matson recognized the importance of a one-way valve in a shunt system andhe experimented with a magnetic shunt system in the early 1950’s. In 1952 Nulsen andSpitz reported the successful use of a ventriculojugular shunt using a spring and stainlesssteel ball valve95. Valve malfunction and occlusion of the venous catheter by thrombuswere frequent problems. John Holter, technician in a machineshop and father of a hydro-
2

cephalic child, designed a multiple slit-valve out of silicone in 1955128. This silicone val-ve was not ready in time for his son who received first a spring ball valve. Afterwards hedid benefit from the silicone shunt valve, but encountered further problems and diedunfortunately of hydrocephalus complications43. Almost at the same time, Robert Pudenzcarried out animal experiments demonstrating that the venous catheter works best withinthe right atrium. Working in the laboratory with many materials (silicone elastomer, poly-ethylene, polyvenylcloride, Teflon, rubber and stainless steel) he showed clearly that sili-cone was the best biomaterial6. His initial Teflon sleef valve was replaced by a distal slitand core valve (Heyer valve). Both the Pudenz/Heyer and the Spitz/Holter system provid-ed a far better solution to the CSF shunt problem than had been obtained so far. Sikkensreported a satisfactory result following shunting from the lateral ventricle into the venacava using a ball valve incorporated into a methyl methacrylate housing117. This “dutch”valve has never been commercialized, though.Ventriculoatrial (VA) shunting became standard practice in the 1960’s. Pleural shunting declined because of chronic pleural effusion and lumboperitoneal shunt-ing via laminectomy declined because of the risk of scoliosis74. The VA shunts had to belengthened regularly and the consequences of thrombo-embolism and shunt infectionwere particularly severe. Ames considered the peritoneal cavity as the ideal location fordrainage and reabsorption of large volumes of CSF. In 1967, he reported a large series ofpatients treated with ventriculoperitoneal (VP) shunts4. In the 1970’s a gradual shifttoward VP shunt systems was seen worldwide.From the 1970’s, attempts are made to produce permanent internal fistulae by endoscop-ic or stereotactic methods. Backlund performed 13 stereotactic prostheses in 7 patients,controlling hydrocephalus in 4 patients16. Over the last decade endoscopic techniques andskills improved significantly, reducing the need for shunts.In 1975 El Shafei described his clinical experience with a technique for shunting CSFfrom the lateral ventricle into the proximal segment of an occluded common facial orexternal jugular vein47. He stated that 30 out of 36 patients benefited from this procedure.During the last two decades an enormous amount of hardware has been developed for therelatively simple task of CSF diversion. Despite the development of valves with a com-plex architecture, programmable and non-programmable, shunt complications are still amatter of great concern.
3
Chapter 2 Clinical study on hydrocephalus shunts
2.1 General data
2.1.1 Patients and data collectionData were collected on 400 patients undergoing primary shunt operations for hydrocepha-lus between December 1989 and January 1992. These patients were operated on in eightdifferent Dutch neurosurgical centres (table 2.1.1).
When the surgical procedure had been completed, the surgeon filled out a patient formand sent it to the study coordinator. After the surgery there was a follow-up period. At theend of the follow-up period, the study coordinator collected the adjuvant data on eachpatient. The data were collected from the patient’s medical record and/or through contact-ing the patient’s neurologist or general practitioner.
Of the patients 222 were male, 178 female. We divided the study population in threeage groups: 0-1 year of age = group A (71? and 54/), 1-15 years of age = group B (21?
and 18/) and over 16 years of age = group C (130? and 106/). The minimum follow-up period was two years and 175 days, the maximum follow-up period was five years and65 days. The mean follow-up period was three years and 294 days. A shorter follow-upperiod was unavoidable in case of mortality during the follow-up period.
2.1.2 Etiology of hydrocephalus and most prevalent pre-operative symptoms Overall, tumor is the most prevalent cause of hydrocephalus (104). Next are normal pres-sure hydrocephalus (59) and meningomyelocele (39) (table 2.1.2). But for each age groupa more specific preponderance in etiology could be discerned. In group A meningomyelo-cele is the most important cause of hydrocephalus (37), followed by perinatal hemorrhage(31) and aqueductal syndrome (19). In group B the majority of cases is caused bytumor(24). Tumor is most prevalent in group C (75), but in this last group normal pres-sure hydrocephalus (59) as well as subarachnoid hemorrhage (44) are also frequent caus-es of hydrocephalus.
Symptoms at presentation were an enlarged head (104), headache (88), NPH symp-toms and impaired consciousness (75).
2.1.3 Surgical procedure2.1.3.1 SurgeonThe shunts were inserted by 46 neurosurgeons or neurosurgical residents. The number of
4
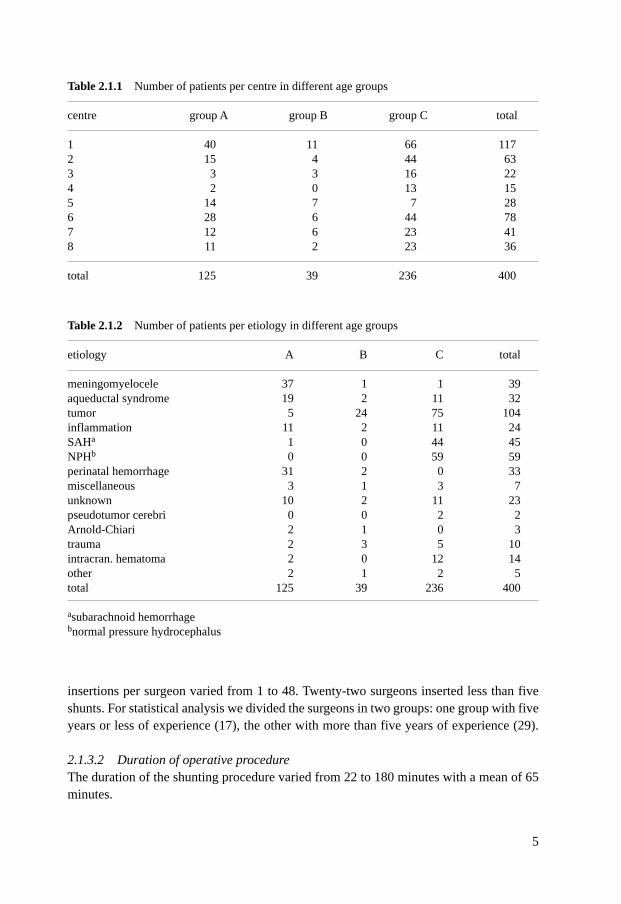
insertions per surgeon varied from 1 to 48. Twenty-two surgeons inserted less than fiveshunts. For statistical analysis we divided the surgeons in two groups: one group with fiveyears or less of experience (17), the other with more than five years of experience (29).
2.1.3.2 Duration of operative procedureThe duration of the shunting procedure varied from 22 to 180 minutes with a mean of 65minutes.
5
Table 2.1.1 Number of patients per centre in different age groups
centre group A group B group C total
1 40 11 66 1172 15 4 44 633 3 3 16 224 2 0 13 155 14 7 7 286 28 6 44 787 12 6 23 418 11 2 23 36
total 125 39 236 400
Table 2.1.2 Number of patients per etiology in different age groups
etiology A B C total
meningomyelocele 37 1 1 39aqueductal syndrome 19 2 11 32tumor 5 24 75 104inflammation 11 2 11 24SAHa 1 0 44 45NPHb 0 0 59 59perinatal hemorrhage 31 2 0 33miscellaneous 3 1 3 7unknown 10 2 11 23pseudotumor cerebri 0 0 2 2Arnold-Chiari 2 1 0 3trauma 2 3 5 10intracran. hematoma 2 0 12 14other 2 1 2 5total 125 39 236 400
asubarachnoid hemorrhagebnormal pressure hydrocephalus
2.1.3.3 Drainage routeThe frontal (158: 139 R, 7 L, 12 both) and parietal (156: 137 R, 19 L) drainage routeswere equally used. The occipital route (86: 74 R, 8 L, 4 both) was less frequently used. In348 patients a ventriculoperitoneal (VP) shunt was inserted, while 45 patients got a ven-triculoatrial (VA) shunt. The El Shafei procedure47-52 was performed in six patients. Inthis procedure CSF is drained to the jugular vein in a retrograde way. In one patient theexact route of drainage remained unknown.
2.1.3.4 peri-operative antibiotics334 patients (83,5%) were on antibiotics in the perioperative period. The antibiotics usedwere: floxapen (155), cotrimoxazol (96), cefuroxim (38), kefsol (27), cloxacillin (6), ce-facidal (3) and vancomycin (1). A combination of antibiotics was given in one case. Intwo cases the type of antibiotic remained unknown.
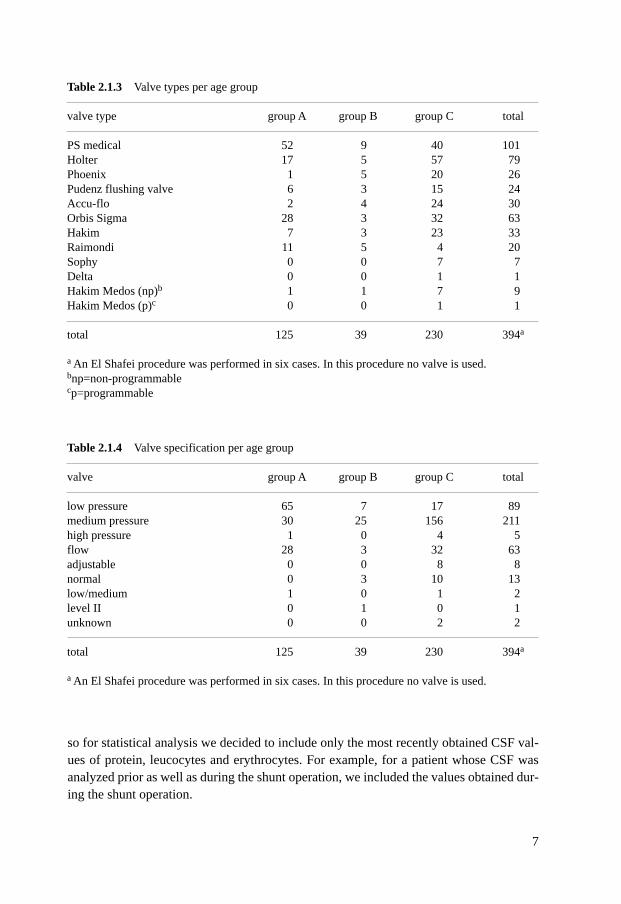
2.1.4 Shunt systems2.1.4.1 ValvesMost frequently used was the Pudenz Schulte valve (101). The Holter (79), Orbis Sigma(63) Hakim (33), Accu-flo (30), Phoenix (26), Pudenz flushing valve (24) and Raimondivalve (20) were less frequently inserted. More than half (211) of these valves had ’medium’ as a specification. The ‘low’ valve wasinserted 89 times. The Orbis Sigma valve (flow limitation) was used in 63 cases. (Table2.1.3 and 2.1.4).
2.1.4.2 Shunt componentsIn 90 cases a one-piece shunt was inserted. The other patients got a combination of sever-al shunt components which are connected to get a complete shunt system. In five patientsan anti siphon device (ASD) was inserted. A reservoir was part of the system in 178patients. The mean number of shunt connections was 1.9, with a mean of 1.3 in theyoungest group, 2.4 in the middle group and 2.2 in the oldest group.
The mean ventricular catheter length was 6.7 cm, varying from 6.1 cm in group A to7.0 in group C. The mean abdominal catheter length was 29.7 cm: 33.2 cm in group A,33.5 cm in group B and 26.5 cm in group C.
2.1.5 Pre-operative external ventricular drainage (EVD)A hundred and eleven patients underwent EVD before internal shunt insertion. Reasonsfor this EVD were an increase in intracranial pressure (43), often in combination withhemorrhage (26), infection (11) and/or the need for pressure recording (11).
2.1.6 Cerebrospinal fluid analysis Pre-operative ventricular CSF analysis (protein, leucocytes, erythrocytes) was done in 80patients. All these patients had an EVD. In addition to this, 59 patients had their CSF ana-lyzed during the operation. There was a certain overlap between patients in these groups,
6
so for statistical analysis we decided to include only the most recently obtained CSF val-ues of protein, leucocytes and erythrocytes. For example, for a patient whose CSF wasanalyzed prior as well as during the shunt operation, we included the values obtained dur-ing the shunt operation.
7
Table 2.1.3 Valve types per age group
valve type group A group B group C total
PS medical 52 9 40 101Holter 17 5 57 79Phoenix 1 5 20 26Pudenz flushing valve 6 3 15 24Accu-flo 2 4 24 30Orbis Sigma 28 3 32 63Hakim 7 3 23 33Raimondi 11 5 4 20Sophy 0 0 7 7Delta 0 0 1 1Hakim Medos (np)b 1 1 7 9Hakim Medos (p)c 0 0 1 1
total 125 39 230 394a
a An El Shafei procedure was performed in six cases. In this procedure no valve is used.bnp=non-programmablecp=programmable
Table 2.1.4 Valve specification per age group
valve group A group B group C total
low pressure 65 7 17 89medium pressure 30 25 156 211high pressure 1 0 4 5flow 28 3 32 63adjustable 0 0 8 8normal 0 3 10 13low/medium 1 0 1 2level II 0 1 0 1unknown 0 0 2 2
total 125 39 230 394a
a An El Shafei procedure was performed in six cases. In this procedure no valve is used.
Results obtained through lumbar puncture were not included in the analysis because lum-bar CSF may have a different composition compared to ventricular CSF.
2.1.7 Statistical analysisFor statistics we used the χ2-test and the Student’s t-test. In both tests, a p-value of 0.05 orless was considered significant. An analysis of variance was done once to look at theinfluence of several factors together on the outcome. With this test, significance wasagain attained with a p-value of 0.05 or less.
2.2 Results
2.2.1 Number of revisions and interval until revisionOf the 400 patients included in this study, 109 (27%) underwent a revision operation. Ofthese patients, 51 needed a second revision and 19 needed a third. Two patients under-went a seventh revision. Overall there were 200 revisions. Therefore the mean revisionrate per patient was 50%.
Looking only at the first revision, the revision rate per patient is 27% (see above). Ingroup A 55 patients (44%) needed a first revision. In group B a first revision was neces-sary for 7 patients (18%) and in group C 47 patients (20%) underwent a first revision.These differences in revision rates we found between the three age groups are significant(χ2; p<0.0001). The mean age of the whole group that underwent revision was 24 years,for the group without revision this was 36 years. Between hospitals, there were no significant differences in the rate of first revisions perpatient with, all age groups considered, a minimum of 6% to a maximum of 28%.
The mean number of days until the first revision was 230 (min. 2 days, max. 5 years).For group A this was 262 days (min. 2 days, max. 5 years), for group B 205 days (min. 30days, max. 3 years) and for group C 195 days (min. 3 days, max. 3 years).
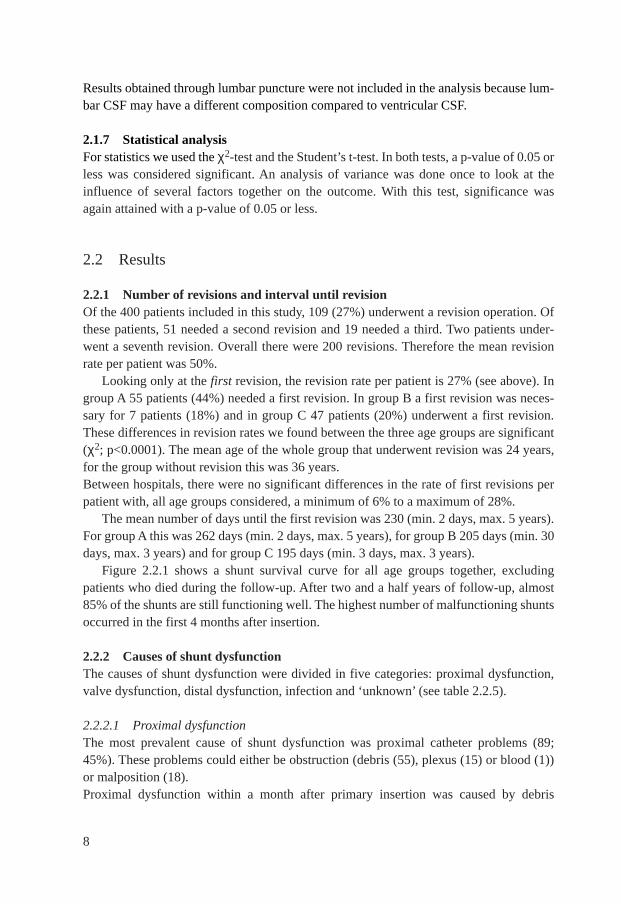
Figure 2.2.1 shows a shunt survival curve for all age groups together, excludingpatients who died during the follow-up. After two and a half years of follow-up, almost85% of the shunts are still functioning well. The highest number of malfunctioning shuntsoccurred in the first 4 months after insertion.
2.2.2 Causes of shunt dysfunctionThe causes of shunt dysfunction were divided in five categories: proximal dysfunction,valve dysfunction, distal dysfunction, infection and ‘unknown’ (see table 2.2.5).
2.2.2.1 Proximal dysfunctionThe most prevalent cause of shunt dysfunction was proximal catheter problems (89;45%). These problems could either be obstruction (debris (55), plexus (15) or blood (1))or malposition (18). Proximal dysfunction within a month after primary insertion was caused by debris
8
obstructing the catheter or, by malposition. Obstruction later on was due to plexus in-growth or, again, debris. In 2.2.6.2 the correlation between proximal shunt obstructionand ventricular catheter length will be analyzed further.
2.2.2.2 Valve dysfunctionIn 35 (17,5%) cases it was the valve which caused shunt malfunction, but in 18 of thesecases the exact valve problem remained unknown. Ten revisions were performed becauseof valve obstruction. In the other seven patients the valves were patent, but they had thewrong resistance: four valves had a resistance too low which caused overdrainage, threevalves had a resistance too high causing underdrainage.
2.2.2.3 Distal dysfunctionDistal catheter dysfunction occurred less frequently (31; 15,5%). Usually there was amalposition (19) of the abdominal catheter. Obstruction was found in five cases, a cyst inone case and in six cases the cause of the distal dysfunction remained unknown.
2.2.2.4 Infection2.2.2.4.1 Definition of infection Infection was diagnosed according to the CSF shuntinfection criteria based on clinical and laboratory findings as discussed by Walters et
9
Figure 2.2.1 Shunt survival curve, excluding patients who died during follow-up.
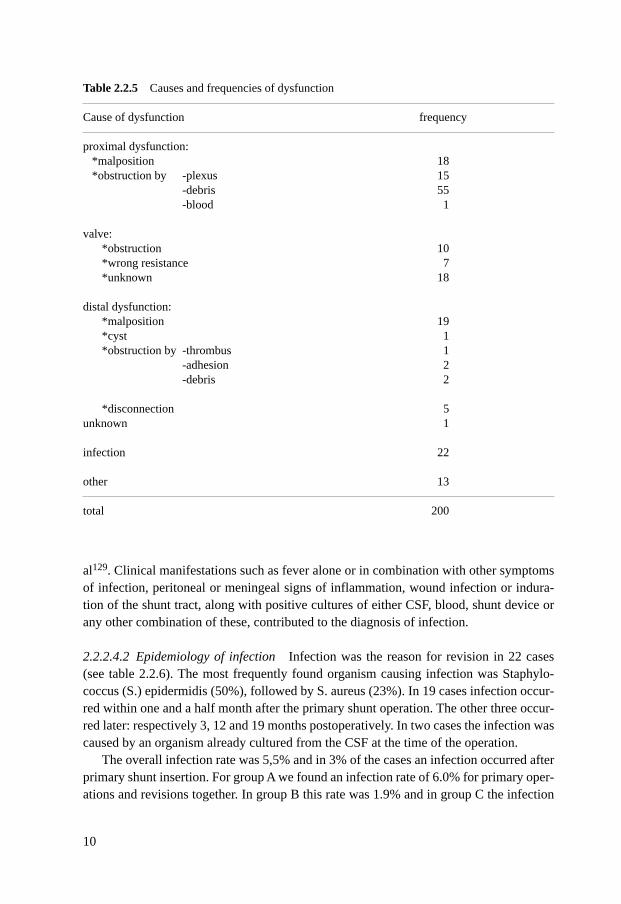
al129. Clinical manifestations such as fever alone or in combination with other symptomsof infection, peritoneal or meningeal signs of inflammation, wound infection or indura-tion of the shunt tract, along with positive cultures of either CSF, blood, shunt device orany other combination of these, contributed to the diagnosis of infection.
2.2.2.4.2 Epidemiology of infection Infection was the reason for revision in 22 cases(see table 2.2.6). The most frequently found organism causing infection was Staphylo-coccus (S.) epidermidis (50%), followed by S. aureus (23%). In 19 cases infection occur-red within one and a half month after the primary shunt operation. The other three occur-red later: respectively 3, 12 and 19 months postoperatively. In two cases the infection wascaused by an organism already cultured from the CSF at the time of the operation.
The overall infection rate was 5,5% and in 3% of the cases an infection occurred afterprimary shunt insertion. For group A we found an infection rate of 6.0% for primary oper-ations and revisions together. In group B this rate was 1.9% and in group C the infection
10
Table 2.2.5 Causes and frequencies of dysfunction
Cause of dysfunction frequency
proximal dysfunction:*malposition 18*obstruction by -plexus 15
-debris 55-blood 1
valve: *obstruction 10*wrong resistance 7*unknown 18
distal dysfunction:*malposition 19*cyst 1*obstruction by -thrombus 1
-adhesion 2-debris 2
*disconnection 5unknown 1
infection 22
other 13
total 200
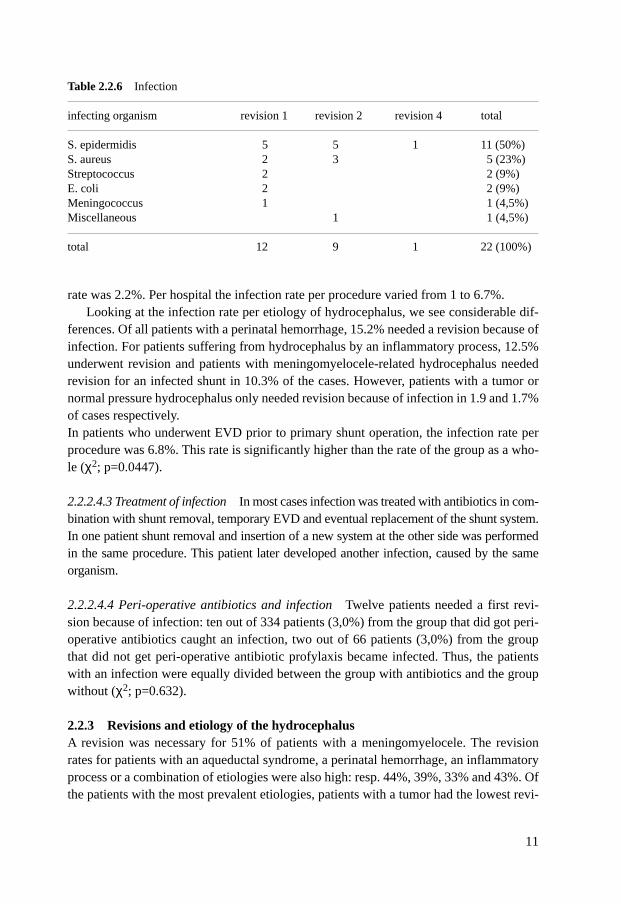
rate was 2.2%. Per hospital the infection rate per procedure varied from 1 to 6.7%. Looking at the infection rate per etiology of hydrocephalus, we see considerable dif-
ferences. Of all patients with a perinatal hemorrhage, 15.2% needed a revision because ofinfection. For patients suffering from hydrocephalus by an inflammatory process, 12.5%underwent revision and patients with meningomyelocele-related hydrocephalus neededrevision for an infected shunt in 10.3% of the cases. However, patients with a tumor ornormal pressure hydrocephalus only needed revision because of infection in 1.9 and 1.7%of cases respectively. In patients who underwent EVD prior to primary shunt operation, the infection rate perprocedure was 6.8%. This rate is significantly higher than the rate of the group as a who-le (χ2; p=0.0447).
2.2.2.4.3 Treatment of infection In most cases infection was treated with antibiotics in com-bination with shunt removal, temporary EVD and eventual replacement of the shunt system.In one patient shunt removal and insertion of a new system at the other side was performedin the same procedure. This patient later developed another infection, caused by the sameorganism.
2.2.2.4.4 Peri-operative antibiotics and infection Twelve patients needed a first revi-sion because of infection: ten out of 334 patients (3,0%) from the group that did got peri-operative antibiotics caught an infection, two out of 66 patients (3,0%) from the groupthat did not get peri-operative antibiotic profylaxis became infected. Thus, the patientswith an infection were equally divided between the group with antibiotics and the groupwithout (χ2; p=0.632).
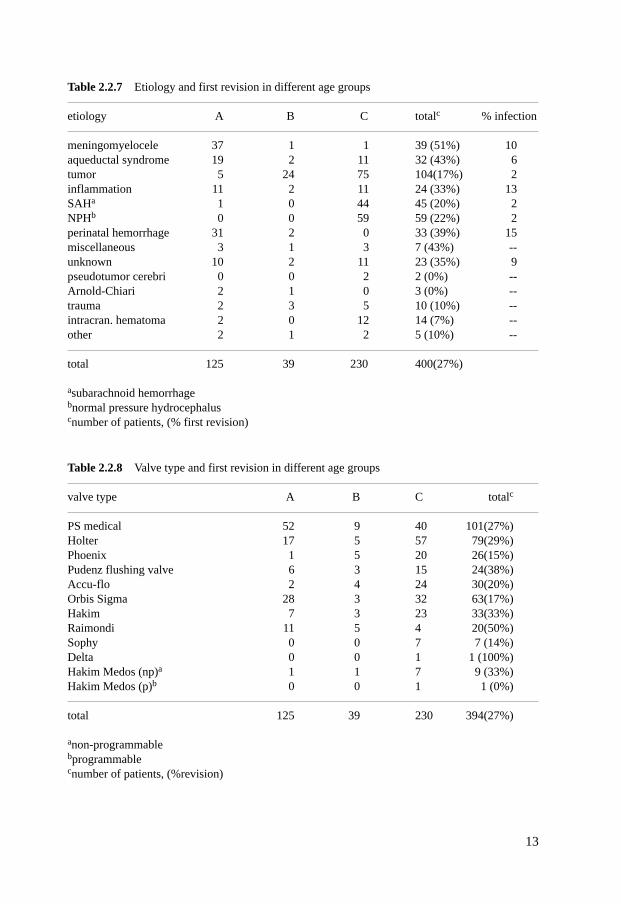
2.2.3 Revisions and etiology of the hydrocephalusA revision was necessary for 51% of patients with a meningomyelocele. The revisionrates for patients with an aqueductal syndrome, a perinatal hemorrhage, an inflammatoryprocess or a combination of etiologies were also high: resp. 44%, 39%, 33% and 43%. Ofthe patients with the most prevalent etiologies, patients with a tumor had the lowest revi-
11
Table 2.2.6 Infection
infecting organism revision 1 revision 2 revision 4 total
S. epidermidis 5 5 1 11 (50%)S. aureus 2 3 5 (23%)Streptococcus 2 2 (9%)E. coli 2 2 (9%)Meningococcus 1 1 (4,5%)Miscellaneous 1 1 (4,5%)
total 12 9 1 22 (100%)
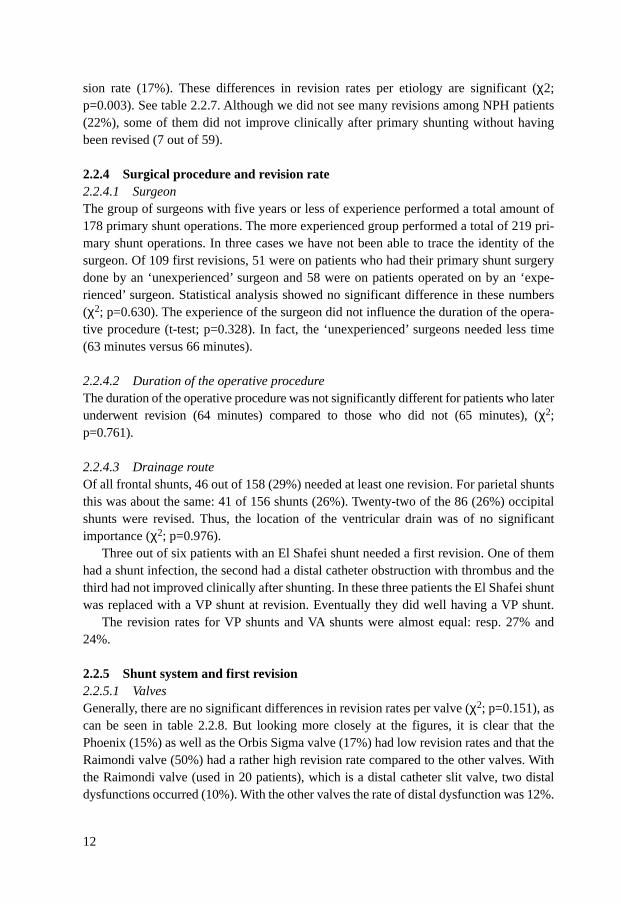
sion rate (17%). These differences in revision rates per etiology are significant (χ2;p=0.003). See table 2.2.7. Although we did not see many revisions among NPH patients(22%), some of them did not improve clinically after primary shunting without havingbeen revised (7 out of 59).
2.2.4 Surgical procedure and revision rate2.2.4.1 SurgeonThe group of surgeons with five years or less of experience performed a total amount of178 primary shunt operations. The more experienced group performed a total of 219 pri-mary shunt operations. In three cases we have not been able to trace the identity of thesurgeon. Of 109 first revisions, 51 were on patients who had their primary shunt surgerydone by an ‘unexperienced’ surgeon and 58 were on patients operated on by an ‘expe-rienced’ surgeon. Statistical analysis showed no significant difference in these numbers(χ2; p=0.630). The experience of the surgeon did not influence the duration of the opera-tive procedure (t-test; p=0.328). In fact, the ‘unexperienced’ surgeons needed less time(63 minutes versus 66 minutes).
2.2.4.2 Duration of the operative procedureThe duration of the operative procedure was not significantly different for patients who laterunderwent revision (64 minutes) compared to those who did not (65 minutes), (χ2;p=0.761).
2.2.4.3 Drainage routeOf all frontal shunts, 46 out of 158 (29%) needed at least one revision. For parietal shuntsthis was about the same: 41 of 156 shunts (26%). Twenty-two of the 86 (26%) occipitalshunts were revised. Thus, the location of the ventricular drain was of no significantimportance (χ2; p=0.976).
Three out of six patients with an El Shafei shunt needed a first revision. One of themhad a shunt infection, the second had a distal catheter obstruction with thrombus and thethird had not improved clinically after shunting. In these three patients the El Shafei shuntwas replaced with a VP shunt at revision. Eventually they did well having a VP shunt.
The revision rates for VP shunts and VA shunts were almost equal: resp. 27% and24%.
2.2.5 Shunt system and first revision2.2.5.1 ValvesGenerally, there are no significant differences in revision rates per valve (χ2; p=0.151), ascan be seen in table 2.2.8. But looking more closely at the figures, it is clear that thePhoenix (15%) as well as the Orbis Sigma valve (17%) had low revision rates and that theRaimondi valve (50%) had a rather high revision rate compared to the other valves. Withthe Raimondi valve (used in 20 patients), which is a distal catheter slit valve, two distaldysfunctions occurred (10%). With the other valves the rate of distal dysfunction was 12%.
12
13
Table 2.2.7 Etiology and first revision in different age groups
etiology A B C totalc % infection
meningomyelocele 37 1 1 39 (51%) 10aqueductal syndrome 19 2 11 32 (43%) 6tumor 5 24 75 104(17%) 2inflammation 11 2 11 24 (33%) 13SAHa 1 0 44 45 (20%) 2NPHb 0 0 59 59 (22%) 2perinatal hemorrhage 31 2 0 33 (39%) 15miscellaneous 3 1 3 7 (43%) --unknown 10 2 11 23 (35%) 9pseudotumor cerebri 0 0 2 2 (0%) --Arnold-Chiari 2 1 0 3 (0%) --trauma 2 3 5 10 (10%) --intracran. hematoma 2 0 12 14 (7%) --other 2 1 2 5 (10%) --
total 125 39 230 400(27%)
asubarachnoid hemorrhagebnormal pressure hydrocephaluscnumber of patients, (% first revision)
Table 2.2.8 Valve type and first revision in different age groups
valve type A B C totalc
PS medical 52 9 40 101(27%)Holter 17 5 57 79(29%)Phoenix 1 5 20 26(15%)Pudenz flushing valve 6 3 15 24(38%)Accu-flo 2 4 24 30(20%)Orbis Sigma 28 3 32 63(17%) Hakim 7 3 23 33(33%)Raimondi 11 5 4 20(50%)Sophy 0 0 7 7 (14%)Delta 0 0 1 1 (100%)Hakim Medos (np)a 1 1 7 9 (33%)Hakim Medos (p)b 0 0 1 1 (0%)
total 125 39 230 394(27%)
anon-programmablebprogrammablecnumber of patients, (%revision)
Because the mechanism of the Orbis Sigma valve (flow limitation) is based on a differentprinciple than the mechanism of the other valves (differential pressure), we compared theOrbis Sigma valve alone with the other valves together for the occurrence of shunt dys-function in each age group. Table 2.2.9 shows the mean number of revisions per sub-group.
An analysis of variance on the influence of the main factors age and valve type onshunt dysfunction showed a significant effect of these main factors together (analysis ofvariance; p<0.0001). There is also a significant effect of age alone, as well as valve typealone. The Orbis Sigma valve causes significantly less shunt dysfunction (analysis of var-iance; p=0.008) than the other valves. The youngest age group needs significantly morerevisions (analysis of variance; p<0.0001), see also paragraph 2.2.1.As shown in table 2.2.9, the Orbis Sigma valve has positive effects mainly in age groupsA and B. In group C the mean number of revisions for the Orbis Sigma valve and theother valve types is almost the same (respectively 0.19 and 0.20). In group C we paid spe-cial attention to NPH patients. In these patients, the Orbis Sigma valve did not cause sig-nificantly less shunt dysfunction than the other valve types, although the mean number ofrevisions was lower with the Orbis Sigma valve (0.17 versus 0.23; t-test, p=0.589).
For the group as a whole, valve specification (table 2.2.10) was of significant impor-tance for revision rate (χ2; p=0.003). Focussing on the three most frequently used valves,we found the following results: there was no significant difference between low pressurevalves and medium pressure valves (t-test; p=0.483), but shunt systems in which theOrbis Sigma valve had been incorporated, necessitated significantly less revisions thanshunt systems in which the low or medium pressure valve had been used (t-test; resp.p=0.001 and p=0.026).
2.2.5.2 Shunt componentsThe number of shunt connections is of no significant importance for the revision rate (χ2;p=0.749). The mean number of connections in the group that underwent revision was 2.0,in the other group it was 1.9.
The ventricular catheter length was significantly shorter (χ2; p=0.035) in the groupthat needed revision (6.4±1.7 cm) than in the group that did not (6.8±1.6 cm). Per agegroup, we looked at the relation between ventricular catheter length and the occurrence ofobstruction of the proximal catheter. In group A the ventricular catheter length in thegroup with proximal obstruction was 5.2 cm, whereas the ventricular catheter length inthe group without obstruction was 6.2 cm. This difference was almost significant (t-test;p=0.073). In group B the ventricular catheter length in the groups with and without revi-sion was respectively 6.0 and 6.4 cm. This difference was not significant (t-test;p=0.642). The ventricular catheter length in group C for patients with and withoutobstruction was resp. 6.0 and 7.0 cm. The difference in length was almost significant (t-test; p=0.092). In all age groups together, the difference is significant: (t-test; p=0.003).There was no difference in the abdominal catheter lengh between the groups with andwithout revision (χ2; p=0.108). In the children under one year of age we paid extra atten-
14
tion to the correlation between revision rate and abdominal catheter length. But again,there was no significant difference between the groups with and without revision.
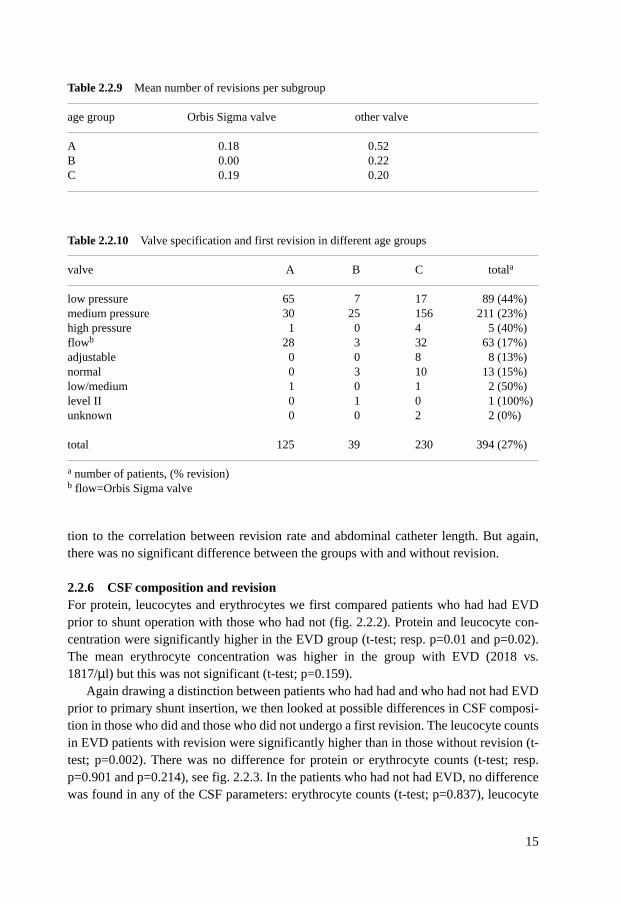
2.2.6 CSF composition and revisionFor protein, leucocytes and erythrocytes we first compared patients who had had EVDprior to shunt operation with those who had not (fig. 2.2.2). Protein and leucocyte con-centration were significantly higher in the EVD group (t-test; resp. p=0.01 and p=0.02).The mean erythrocyte concentration was higher in the group with EVD (2018 vs.1817/µl) but this was not significant (t-test; p=0.159).
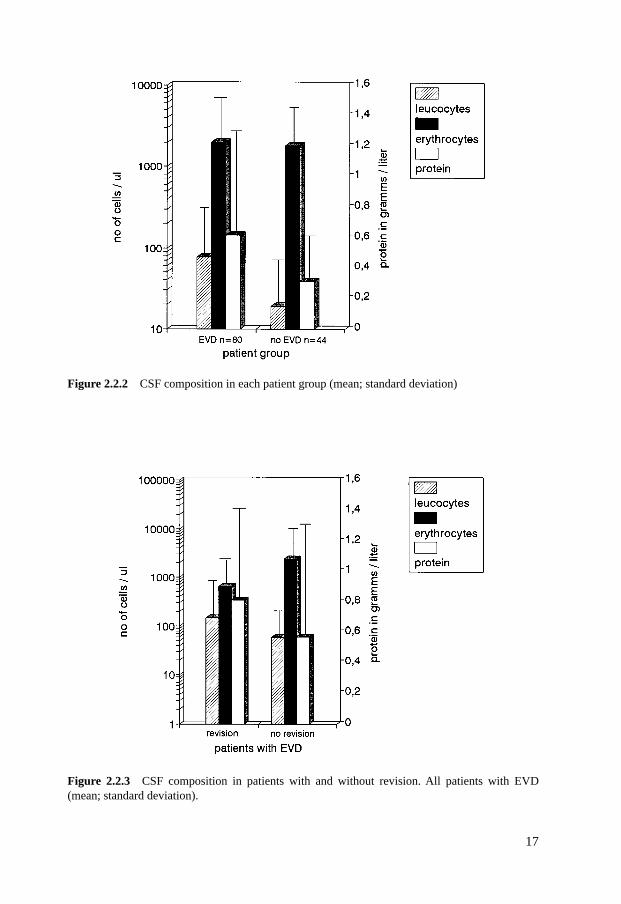
Again drawing a distinction between patients who had had and who had not had EVDprior to primary shunt insertion, we then looked at possible differences in CSF composi-tion in those who did and those who did not undergo a first revision. The leucocyte countsin EVD patients with revision were significantly higher than in those without revision (t-test; p=0.002). There was no difference for protein or erythrocyte counts (t-test; resp.p=0.901 and p=0.214), see fig. 2.2.3. In the patients who had not had EVD, no differencewas found in any of the CSF parameters: erythrocyte counts (t-test; p=0.837), leucocyte
15
Table 2.2.9 Mean number of revisions per subgroup
age group Orbis Sigma valve other valve
A 0.18 0.52B 0.00 0.22C 0.19 0.20
Table 2.2.10 Valve specification and first revision in different age groups
valve A B C totala
low pressure 65 7 17 89 (44%)medium pressure 30 25 156 211 (23%)high pressure 1 0 4 5 (40%)flowb 28 3 32 63 (17%)adjustable 0 0 8 8 (13%)normal 0 3 10 13 (15%)low/medium 1 0 1 2 (50%)level II 0 1 0 1 (100%)unknown 0 0 2 2 (0%)
total 125 39 230 394 (27%)
a number of patients, (% revision)b flow=Orbis Sigma valve

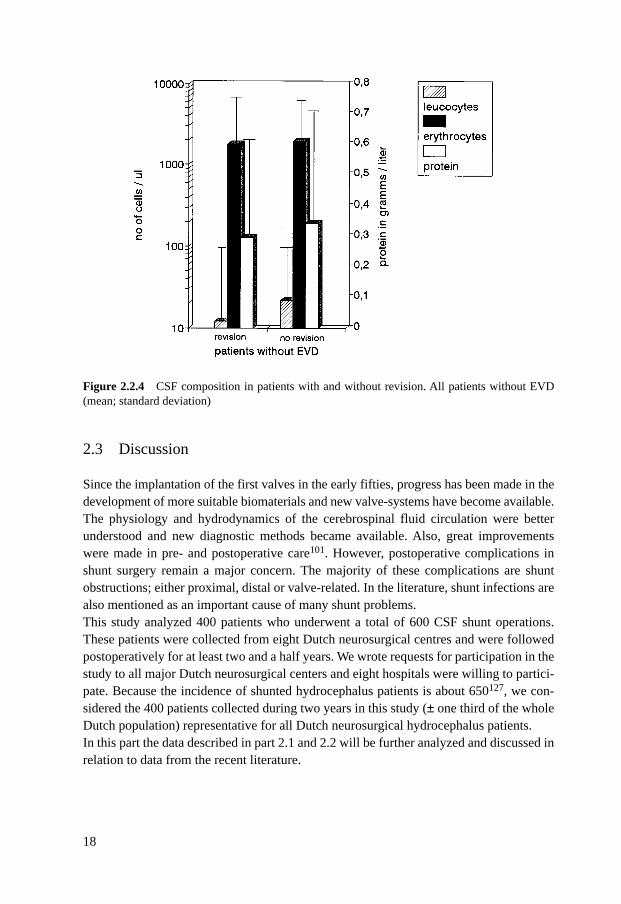
counts (t-test; p=0.082) and protein concentration (t-test; p=0.460). See fig. 2.2.4.To look very closely at the influence of erythrocyte concentration on revision rate, we
compared patients with the lowest erythrocyte levels (<500/µl) with those with the high-est erythrocyte levels (>3000/µl). Again, no difference in revision rate could be detected(t-test; p=0.353)
2.2.7 MorbidityPostoperative morbidity was defined as ‘added morbidity’ after operation. Nine patients(2,3%) showed morbidity after their primary shunt operation. In one patient a treatmentother than the shunt insertion itself was the cause of this morbidity. This patient had avenous leg thrombosis. In another patient a pre-existing tumor caused morbidity.Symptoms resulting from a subdural hematoma occurred in two cases. Symptoms afterpostoperative hemorrhage also occurred twice. Postoperative seizures, transient hemiple-gia and transient CSF hypotension were also mentioned in single cases as morbiditysymptoms. Eventually the morbidity was persistent in only four cases (1%) after primary shunt inser-tion: one as a result of a subdural hematoma, one because of tumor, one because of post-operative hemorrhage and in one case seizures were the cause of morbidity.In five cases a postoperative radiologic diagnosis of subdural hygroma or hematoma wasmade, without any clinical signs.
2.2.8 MortalityIn the follow-up period, 68 out of 400 patients died: ten of them were in group A, ninewere in group B and the other 49 were in group C. The most important cause of death wasa pre-existing tumor (26); pulmonary (9) and cardial (7) problems were also important.The mortality of two patients was shunt related. One appeared to have a subdural hemat-oma, the other died of a shunt infection (aspergillus) which caused obstruction of theshunt system.After revision another nine patients died. Again, tumor was the most frequent cause ofdeath: three patients. Another three patients died of unknown causes and two succumbedafter pulmonary problems. Only one death could be explained by shunt dysfunction. Theproximal catheter was found to be obstructed by debris.
The overall shunt related mortality was 0.5%.
16
17
Figure 2.2.2 CSF composition in each patient group (mean; standard deviation)
Figure 2.2.3 CSF composition in patients with and without revision. All patients with EVD(mean; standard deviation).
2.3 Discussion
Since the implantation of the first valves in the early fifties, progress has been made in thedevelopment of more suitable biomaterials and new valve-systems have become available.The physiology and hydrodynamics of the cerebrospinal fluid circulation were betterunderstood and new diagnostic methods became available. Also, great improvementswere made in pre- and postoperative care101. However, postoperative complications inshunt surgery remain a major concern. The majority of these complications are shuntobstructions; either proximal, distal or valve-related. In the literature, shunt infections arealso mentioned as an important cause of many shunt problems. This study analyzed 400 patients who underwent a total of 600 CSF shunt operations.These patients were collected from eight Dutch neurosurgical centres and were followedpostoperatively for at least two and a half years. We wrote requests for participation in thestudy to all major Dutch neurosurgical centers and eight hospitals were willing to partici-pate. Because the incidence of shunted hydrocephalus patients is about 650127, we con-sidered the 400 patients collected during two years in this study (± one third of the wholeDutch population) representative for all Dutch neurosurgical hydrocephalus patients.In this part the data described in part 2.1 and 2.2 will be further analyzed and discussed inrelation to data from the recent literature.
18
Figure 2.2.4 CSF composition in patients with and without revision. All patients without EVD(mean; standard deviation)
2.3.1 Shunt revision rate per patientThe study-population consisted of 400 patients who underwent 200 revision operationsduring the follow-up period. Therefore the mean revision rate per patient was 50%.The rate of first revisions per patient was 27%. There were no major differences in revi-sion rates between Dutch hospitals. In 1994 Lund-Johansen79 et al. studied a population of adult patients only and found66% revisions per patient (follow up time varied from 1 to 9 years).In 1994 Kast et al71
reported 78% revisions per patient in a sightly younger population (2 months to 26 yearsold) than our study-population. A study performed in the children’s hospitals in Torontoand Paris109 showed an even higher revision rate of 120%.
The overall revision rate per patient we found is rather low compared to the otherstudies71,109,79. This difference cannot be explained by differences in age or etiology ofthe patient population. Our Dutch population consisted of children as well as adults.Adults apparently need less revisions than infants (see 2.3.5). Even with this mixed pop-ulation we observed less revisions than Lund-Johansen et al.79 reported in an adult popu-lation. A possible explanation for the low revision rate in the study could be that duringthe last decades, improvements in overall medical management of shunt patients haveprobably enabled Dutch neurosurgeons to reach a relatively high standard in CSF shuntsurgery.
2.3.2 Causes of shunt dysfunction2.3.2.1 Proximal dysfunctionThe most frequent cause of shunt malfunction was a dysfunction of the ventricular cathe-ter. This was found in 45% of the revisions. Dysfunction in the first postoperative monthwas either because of a catheter malposition or an obstruction by debris. Dysfunctionmore than six months after the first operation was more commonly caused by obstructionthrough plexus ingrowth or, again, debris.
In a 1993 review27, percentages of 39 to 47 were reported; later studies found revisionrates in the same range41,71,88,98,110. These studies also report that ventricular dysfunctionshortly after the operation is usually caused by debris. Ingrowth of choroid plexus was afrequent cause of proximal dysfunction later on.
2.3.2.2 Valve dysfunctionIn the 200 revisions encountered in this study, valve obstruction was the cause of mal-functioning in ten cases (5%). In only 7 cases (3,5%), problems were caused by over orunderdrainage in the presence of an otherwise patent valve. One of the patients died of asubdural hematoma probably caused by overdrainage
In the literature27,31,41,109, over or underdrainage is the cause of shunt dysfunction in7 to 12% of cases. According to Sainte-Rose109, overdrainage may be directly or indirectlyrelated to more than 40% of the shunt failures. He not only mentioned subdural hematomas,craniostenosis, slit ventricles and orthostatic hypotension as complications due to over-drainage, but also shunt obstruction. Regarding valve obstruction, Sainte-Rose et al.110
19
reported on two series of patients, one treated with shunts incorporating the Orbis Sigmavalve, the other with shunts incorporating standard differential pressure valves. Theyfound a valve obstruction rate of 18,3% for the Orbis Sigma valve, compared to 9,7% forthe standard differential pressure valve (see also 2.3.6.1). In spite of this high obstructionrate for the Orbis Sigma valve, the overall mechanical complication rate was actuallylower for the Orbis Sigma valve compared to differential pressure valves. A valveobstruction rate of 1% over a 2-year period was found by Kast et al.71.
In our study, and also in previous studies, the actual rate of valve problems seemsrather low. The catheter is probably more important than the valve in determining the rateof shunt dysfunction. However, Sainte-Rose’s statement that the indirect complications(shunt obstruction) of, for example, overdrainage are considerable, cannot be rejected byour study in which we only included direct (obvious) complications.
In paragraph 2.3.6.1 the different valve types will be discussed further.
2.3.2.3 Distal dysfunctionOur study shows a distal dysfunction rate of 16%. Most of these cases (9,5%) consisted ofa malposition of the abdominal catheter, usually caused by initial placement of the cathe-ter in the preperitoneal fat layer instead of the abdominal cavity or by migration of thedistal catheter. We did not see migrations to unexpected locations like the colon, the tho-racic cavity, etcetera.
Previous studies showed that 14 to 33% of shunt malfunction was caused by distaldysfunction41,71,88,98,110. In the literature, migration of the distal catheter to unexpectedlocations such as the colon118, the thoracic cavity30, the scrotum73, the anus92, the blad-der89, the pulmonary artery93 and the stomach66 have been described.
2.3.2.4 Infection2.3.2.4.1 Infection and epidemiology In 22 cases, infection was the reason for a revi-sion operation. The overall infection rate was 5,5% and in 3% of the cases an infectionoccurred after primary shunt insertion. Half of the infections in our study were caused byStaphylococcus epidermidis, followed by S. aureus in 22% of the infection cases. Animportant finding was that the infection rate in patients who underwent EVD beforeshunting was significantly higher than the overall rate. But even after EVD the infectionrate remained relatively low (6,8%). This slight increase in infection rate is indeed rele-vant in a study like this, with a large population of 400 patients. Most cases of infectionoccurred shortly after operation: 19 of our patients showed signs and symptoms of infec-tion within one and a half month after operation. Two patients in our study had a shuntinfection caused by an organism which could later be cultured from CSF obtained duringthe previous shunt operation. Fifteen out of 22 cases (68%) were found in the youngestage group.
In the literature, infection rates of 3 to 29% are reported with a mean of 5 to8%27,41,63,71,88,98,128. Most infections are caused by S. epidermidis, followed by S. aure-us27,42,63,128. The reason for S. epidermidis to become such a frequent cause of shunt
20
infection, is its property to form a mucoid glycocalyx which protects itself against antimi-crobial drugs and host immune responses27. The glycocalyx also induces increased adhe-sion of the bacteria to shunt material42. Furthermore, host leucocyte immune function isimpaired in the presence of shunt material27. Although higher infection rates after EVDhave been described before94, other studies42 showed no difference in infection rates forpatients with previous EVD compared to patients without. Most studies show that infec-tions usually occur within 2 months after shunt insertion42,44,71. Because of this shortinterval it is assumed that in these cases contamination took place during shunt opera-tion44,58. The literature on age and shunt insertion and infection shows that, in general,infection rates are higher in younger children27,29,41,42,98,128. Sometimes the underlyingetiology of the hydrocephalus is mentioned as being important for the susceptibility toinfection: in case of a perinatal hemorrhage, the chance of an infection is high98. A pos-sible explanation for this high rate might be that perinatal hemorrhage most frequentlyoccurs in preterm infants. In these preterm infants the immune system is still immature27.Thus, age is probably more important than etiology. The high susceptibility to infection inyounger children has been explained in several ways. As mentioned above, the immunesystem in babies, especially preterm babies, is still immature. Probably even more impor-tant is the bacterial skinflora. In babies there is a quantitative as well as a qualitative dif-ference in bacterial skin flora compared to adults. Pople et al.99 showed that the higherbacterial density in the skin of newborn was a risk factor for infection. Furthermore,strains of coagulase negative staphylococci with a high degree of bacterial adherence aremore often found in newborn than in older children99. Another explanation proposed byDuhaime et al.44 was the higher temperature and humidity in the operating room duringpediatric neurosurgery.
The data we found on infection are in concordance with reports from the literature.But it is clear that the Dutch infection rates are rather low compared to the rates found inother studies. A possible explanation could be that Dutch standards of asepsis during sur-gery are high. Also, in the last decade materials and skills have improved, which alsomight contribute to low infection rates
2.3.2.4.2 Treatment of infection All cases of infection except one in our Dutch studywere treated according to the ‘gold standard’ as described by Gardner et al.58. This con-sists of: removal of the shunt, EVD if necessary, administration of antibiotics and replace-ment by a new shunt system only after recovery. This treatment was sufficient in all cas-es. The one patient who was not treated according to this standard developed anotherinfection caused by the same organism later on (see 2.2.2.4.3).
In a retrospective study on 38 patients with a shunt infection Morisette et al.94 found acure rate of 94% after treatment with intravenous antibiotics and shunt replacement, eith-er with or without EVD. For other modalities of treatment like medical support, intrave-nous antibiotics alone and intravenous antibiotics with shunt revision (no replacement!)the cure rates were respectively 0%, 25% and 0%. All patients who only received a sup-portive treatment died. Those who received antibiotics together with a shunt revision
21
always developed a recurrent infection. Morisette et al. also concluded that careful selec-tion of antibiotics in combination with shunt removal (with eventual replacement), eitherwith or without EVD is the proper way to treat shunt infections. Walters et al.129 support-ed this view: they reported that the best treatment for shunt infection consisted of antibi-otics, shunt removal and delayed shunt replacement. Replacement during the same oper-ation in which the infected system was removed gave results that were worse. They notedthat EVD treatment of infections resulted in a higher mortality and morbidity but theycould explain this by the severity of the underlying problem. In the literature it has beendescribed1, that in the instance of a shunt infection caused by an organism which is foundin meningitis in the ’normal’ population there is no absolute indication for shunt removal:this conclusion was based on successful treatments of H. Influenza, meningococcus andgonococcus infections with antibiotics alone. However, if the CSF had not become sterilewithin 72 hours, the shunt system was still removed. An alternative way of treating shuntinfections, a third ventriculostomy68 , has been suggested by Jones et al. They reportedfour successfully treated cases of recurrent infections by third ventriculostomy and intra-venous and/or intraventricular antibiotics.
Comparing the literature and our own experience in the treatment of shunt infection,the ‘gold’ standard appears to be the most suitable method to treat shunt infection. Thecure rate is high and complications of infection are low. Other ways of treatment27,68,94
are possible in some cases, but they are not necessarily better. The increasing popularityof third ventriculostomy might change this situation.
2.3.2.4.3 Prevention of infection Our study showed that peri-operative antibiotics hadno significant effect on infection rates. The relative number of infections in patients withor without infection was the same. Other preventive measures like planning the operationearly in the morning and other suggestions done by Choux29 were not part of the proce-dure in a systematical way in the participating centres and their impact could not be stud-ied hence.
From a metanalysis63 of studies of the past few years it can be concluded that antibio-tic prophylaxis is only useful when the baseline infection rate is higher than 5%. Choux29
by following a strict operative protocol could reduce the infection rate from 7,8 to 0,3%.Some of the precautions constituted planning the operations early in the morning, reduc-ing the duration of the operating to a minimum and unpacking the shunt material immedi-ately before implantation. This study also agreed that the surgeon’s concern with theinfection problem already influences the incidence of infection. Pople et al.99 mentionedsuch precautions as washing the patient with two separate chlorhexidine shampoos 2 to24 hours pre-operatively, isolation of wound edges with antiseptic drapes and the chang-ing of gloves just before the actual implantation of shunt material. They also stated therate of infection will already decline by greater alertness of the surgeon. Another study44
concluded that airborne bacteria from personnel present in the operating room are animportant cause of shunt infections, even more important than endogenous bacteria. Thisstudy has several suggestions to reduce this surgeon-related contamination, varying from
22
washing or covering the surgeon’s face and increasing the distance between surgeon andwound, to installing a transparant mechanical barrier between surgeon and patient.Another precaution mentioned in the literature is impregnating the shunt catheter withantibiotics. A recent report18 showed that catheters impregnated with antibiotics (rifam-pin/clindamycin) protected against infection in the immediate postoperative period. In astudy112 performed by Schierholz et al. in 1997, a shunt impregnated with broad-spec-trum antibiotics was tested. This study also showed that shunt impregnation with antibio-tics could reduce the incidence and amount of bacterial colonization on the surface ofshunt catheters.
With the Dutch low infection rates, radical methods of prevention may not be neces-sary. If we do want to reduce the infection rate even more, measures for prevention shouldbe aimed at the youngest patients who run the highest risk of infection. The impregnationmethod18,112 as well as a strict peri-operative protocol might be useful in reducing infec-tion rates in high risk patients.
2.3.3 Revisions in the various age groupsOur results clearly show a relation between age and the need for a first revision operation.In the group under one year of age the first revision rate was 44%, versus 20% in olderage groups. Looking at the occurrence of obstruction, which is the most prevalent causeof dysfunction in the three age groups, a relatively high rate of obstruction is found in theyoungest group.
Previous studies have also reported age as an important factor determining shunt dys-function27,29,31,41,42,71,98,99. Another hypothesis was put forward by Liptak78. An erectposition changes the ventricular pressure and the cerebrospinal fluid flow through theventriculoperitoneal shunt system. The increase in movement and time spent in the anerect position by children over one year of age may prevent obstruction of catheters andvalves by means of the increase in CSF drainage. Although Liptak’s hypothesis is interesting, it is probably not the only explanation for therelatively high rate of dysfunction in the youngest group. The etiology of the hydrocepha-lus may be a more important factor41,98, and shall be dealt with separately (see 2.3.4).
2.3.4 Revisions related to underlying etiology of hydrocephalusWe found a significant influence of the etiology of hydrocephalus on shunt revision: the-re was a predisposition to shunt dysfunction in meningomyelocele, aqueductsyndrome,infection and perinatal hemorrhage.
These findings are concomitant with the data from the literature showing the etiologyof hydrocephalus to be of great influence on the later occurrence of shunt dysfunc-tion41,98. In a 14-year retrospective study98 of shunt operations a clear, almost significant,trend was seen regarding etiology and the need for a revision operation. Posthemorrhagichydrocephalus and hydrocephalus caused by meningomyelocele in particular have beenreported as being relevant to a high rate of shunt obstructions41,98. In posthemorrhagichydrocephalus there might be sedimentation of blood cells on the shunt valve. This sedi-
23
mentation can impair valve closure or cause obstruction26. Another possibility is thatplatelets mediate blood cell adhesion to the shunt material26. In meningomyelocele aswell as aqueductal syndrome and infection, a weak physical condition might lead to ahigher frequency of shunt dysfunction overall76,91.
In spite of the many different explanations that have been given, the exact reason whyetiology is so important in shunt dysfunction remains unknown.
2.3.5 Operative procedure and incidence of shunt revision2.3.5.1 SurgeonIn our Dutch study there was no relation between the experience of the surgeon and theincidence of revisions. Also, there was no difference in the duration of the surgical proce-dure between ‘experienced’ and ‘unexperienced’ surgeons.
In the literature, there are divergent views regarding the experience of the neurosur-geon41,79,98. According to Piatt et al.98 , the experience of the surgeon was of no signifi-cant importance for the rate of revisions. Di Rocco et al.41 could not detect any differencein the percentage of shunt dysfunction after operations performed by residents comparedto those performed by staff surgeons either. But a Norwegian study79 showed that inexpe-rienced surgeons performed significantly more inadequate operations, leading to a higherrevision rate.
2.3.5.2 Duration of the surgical procedureAs reported by others27,41,79,98 this study showed that the time spent in the operatingroom did not affect the revision rate.
2.3.5.3 Drainage routeThere was no difference in revision rates between frontal and parietal shunts. Neithercould we detect a difference in revision rates between VP and VA shunts.
But in a study in which they analyzed the functioning duration of frontal and parietalshunts in a population of 114 children, Albright et al.2 found that frontal shunts func-tioned for a significantly longer period than parietal shunts, even if in both groups ven-tricular catheters were implanted in a correct position. But according to Bierbrauer etal.19, parieto-occipital shunts survived longer than frontal shunts. In accordance with ourstudy, Piatt et al.98 found no difference between frontal and parietal shunts.
In the literature it is widely known that the number of dysfunctions of ventriculoperit-oneal and ventriculoatrial shunts is roughly the same27,88.
2.3.6 Shunt system versus revision 2.3.6.1 ValvesOur study indicates a high rate of dysfunction for a distal slit valve (Raimondi valve;50%). Significantly less revisions were seen in shunts with the Orbis Sigma valve (17%).In this study we found a high revision rate of 44% for the low pressure valve; the differ-ence in revision rates for low and medium pressure valves (23%) was not significant. It
24
was significant for the Orbis Sigma valve (17%) compared to the differential pressurevalves, as discussed before in 2.2.5.1.
Recent studies reported an increased risk for distal catheter obstruction with the use ofdistal slit valves in the peritoneal catheter31,109,110. These slit valves apparently constitut-ed a canal into which the omentum could grow and cause obstruction at the distal end ofthe catheter. Some studies17,110 reported a lower incidence of revisions for the OrbisSigma valve compared to differential pressure valves11,110. Sainte-Rose et al.110 showedthat shunts with Orbis Sigma valves survived longer than shunts with differential pressurevalves. A higher number and larger proportion of proximal obstructions occurred with thestandard differential pressure valves. Also, the proportion of slit ventricles was signifi-cantly lower using the Orbis Sigma valve. They did find, however, a higher rate of valveobstruction with the Orbis Sigma valve than with the differential pressure valves (18,3versus 9,7%). The high obstruction rate could be explained by the valve architecture: theOrbis Sigma valve is a high resistance system with a narrow orifice that might be easilyoccluded. Aschoff et al.9 reported that, although there are some encouraging results withthe Orbis Sigma valve in pediatric patients, the results in adult patients are disappointing.They stated that the considerable decrease in overdrainage problems with the OrbisSigma valve may be outweighed by the increased rate of shunt insufficiency with this val-ve. In another report12 Aschoff et al. also mentioned the high chance of valve blockadewith the Orbis Sigma valve. Not much has been reported about the designation of the valve (low, medium or highpressure or flow-limiting) with repect to the revision rate. But it is widely known that lowpressure valves are generally used in the youngest age group, which is characterized by adifferent etiology of hydrocephalus and other age-related problems than the other groups.The etiologies themselves tend to cause more revisions in the youngest group. Also, it hasbeen reported before98 that valve dysfunction is more prevalent in children under twoyears of age. In a recent study, Boon et al.20 reported a better outcome for NPH patientswho were treated with low-pressure valves compared to NPH patients treated with medi-um-pressure valves. Most outcome parameters (gait, disability, reduction in ventricularsize) showed trends in favor of the low-pressure valve, but only the dementia scale wassignificant. This outcome scale does not involve the occurrence of shunt complications; itis meant to be an indicator of the quality of life. We did not include any measurements ofthe quality of life in our study.
The advice given before 31,109,110 to use open-ended distal catheters without valvesseems to be justified by our results. However, the high rate of dysfunction with theRaimondi valve (which is a distal slit valve) cannot be explained by a more frequentoccurrence of distal shunt obstruction with this valve. In fact, in our material the rate ofdistal dysfunction is actually lower with the Raimondi valve than with the other valves.The difference is mainly caused by a relatively high frequency of obstruction by debris. We observed that Orbis Sigma valves not only function better in pediatric patients thandifferential pressure valves, but also that these valves function just as well as the differen-tial pressure valves in adult patients. Especially in NPH patients both valve types func-
25
tioned equally well. This is in contrast with previous reports11, which stated that the OrbisSigma valve would only give satisfactory results in children. A possible explanation forthe good results in NPH patients might be that in these patients the CSF flow through theshunt is lower than the flow in the other patients with other etiologies69. In 1987,Kadowaki et al.69 showed that the maximum CSF flow in one NPH patient was 0.12ml/min, whereas the maximum flow in patients with other etiologies was often higher.The limited drainage capacity of the Orbis Sigma valve is probably just sufficient for the-se patients. The fact that our results show the same success rate for both valve types inolder patients as well is more difficult to explain. Apparently, even in these patients, thelow flow through the Orbis Sigma valve is enough to get a satisfactory clinical result. In contrast to previous findings11,110 we did not see a high rate of valve obstruction withthe Orbis Sigma valve.
2.3.6.2 Shunt componentsOur results show that the number of shunt connections was of no significant importancefor the occurrence of a shunt revision. A short ventricular catheter did constitute a riskfactor for a later shunt revision. The risk was mainly determined by the higher chances ofventricular catheter obstruction with a shorter ventricular catheter. The length of theabdominal catheter was not important for the incidence of revisions. This was alsoapplied to the group under one year of age.
From the literature, opposite views are known concerning the influence of the numberof shunt components on the frequency of shunt revisions41,79,98,109. Piatt et al. reportedthat complex shunts (multi-component) had survived significantly shorter than simpleshunts98 (single-component) and Di Rocco et al.41 stated that shunts in which surgeonshad added an extra component ran a higher risk of failure. Sainte-Rose109 also warnedthat the number of shunt connections was important for the chance of dysfunction. On theother hand, a Norwegian study79 was published which showed no difference in the num-ber of shunt connections in patients who needed a revision compared to patients who didnot. According to several studies, the length of the abdominal catheter has no influence onthe rate of distal shunt dysfunction109,110,116. One study found a shorter abdominal cathe-ter to be related to a higher rate of revisions110. This was explained by the need for length-ening the catheter.
The fact that we did not find any influence of the number of shunt connections onrevision rate might show that with the currently used materials the number of shunt con-nections is not as important as it used to be. Another explanation is that surgeons try tolimit the number of connections because of previous reports of higher revision rates withmulti-component shunts. The mean number of connections in this Dutch study was only1.9, which is rather low.
A possible explanation for the higher revision rate with shorter ventricular cathetersmay be the shrinkage of the ventricles after implantation of a functioning shunt. When theexcess of cerebrospinal fluid has been drained, the ventricles shrink and as a result theventricular catheter may retract into the brain parenchyma. The shorter the ventricular
26

catheter, the greater the chance of ‘pseudo-retraction’. The view held by some surgeons that in younger children the abdominal catheter
shouldn’t be too long is rejected by our study. We couldn’t detect any influence of thelength of the abdominal catheter on revision rates. The conclusion may be that an abdom-inal catheter length of up to 60 cm does not increase the risk of complications in youngerchildren.
2.3.7 Cerebrospinal fluid composition versus revision operationsBecause it has been assumed for years that CSF concentrations of protein and cells wereimportant factors in shunt malfunctioning, we paid special attention to the relationbetween these concentrations and revision rates.
Our study showed no correlation between CSF protein concentration and the occur-rence of shunt dysfunction. It should be remarked that the maximal protein concentrationwas 3.5 g/l. We also didn’t find any significant difference in erythrocyte concentrationsbetween patients who needed a revision operation and patients who did not. Shunts wereinserted in a single patient with a cell count above 20.000 cells/µl without the need for arevision later on. Since the beginning of shunt surgery it has been assumed that a highCSF protein may induce shunt dysfunction because55,114 a high concentration of proteinwould cause a high viscosity, which is proportional to the resistance a liquid will encoun-ter during flow. Current literature however, expresses a different view26,27,129. High pro-tein concentrations hardly affect viscosity. In fact, a high protein concentration is shownto lower the surface tension of a fluid which would facilitate valve opening26. It has beendescribed129 in vivo that a CSF erythrocyte count of more than 1000 per µl would increasethe chance of shunt dysfunction (and revision). Sainte Rose et al110. already mentionedthat a shunt operation in which a ventricular catheter was placed in a ventricle full ofblood clots was doomed to failure.
The lack of influence of protein concentration on shunt dysfunction we found corre-sponds with results from other studies. In erythrocyte counts, however, the reports fromthe literature and our own results differ. We do not have a satisfactory explanation for thiscontrast between literature and our own clinical results. Because our study only includeda few patients with extremely high erythrocyte counts (90% of the patients had countsbelow 5000 cells/µl), there is a possibility that we have observed too few patients with(extremely) high counts to show a correlation between these high counts and an increasedshunt failure rate.
2.3.8 MorbidityAs mentioned before we defined morbidity as “added morbidity” after the operation. Thisdefinition makes the morbidity found in our Dutch study very low. After primary shuntoperations the morbidity rate was 2,3%. After revision the rate was comparable: 1,5%. Inonly four cases the morbidity resulted in a permanent disability. Morbidity in these caseswas caused by a subdural hematoma, postoperative seizures and postoperative hemor-rhage. In one case the morbidity was caused by a pre-exisisting tumor.
27

In the literature a higher percentage is reported27, but this is probably due to the definitionused. Previous studies included morbidity caused by the pre-existing etiology of thehydrocephalus. In our study we would then observe a considerable morbidity rate ofpatients with a tumor especially. Generally, it may be concluded that a CSF shunt procedure harbours little risks in termsof morbidity.
2.3.9 MortalityAfter primary shunt operation 68 out of 400 patients died, which implies a mortality rateof 17%. Shunt-related mortality alone shows a different picture. Only two patients died ofa shunt complication (0.5%) after primary insertion. One of them had an infection, theother died after a subdural hematoma, probably caused by overdrainage. The majority ofdeaths were caused by progressive tumor growth. Another nine patients died after revi-sion. Only one of those deaths was caused by a shunt complication. The proximal cathe-ter appeared to be obstructed by debris.
Older studies27 report very high shunt-related mortality rates. Some studies found arate of 60%. Currently, a mortality rate of about 12% is usually found27. Another currentstudy109 showed a shunt-related mortality rate of 1%. It has been reported27 though, thatin general more people die of the disease causing hydrocephalus, than of the shunt treat-ment.
The mortality rate we found, shunt-related and non-shunt-related together (17%),looked substantially higher than the rates reported in the literature27. The difference canbe explained reasonably by the population studied: in most former studies only patientswith a non-neoplastic cause of the hydrocephalus were included. When we exclude neo-plastic cause in our study, we find a mortality rate of 11% (shunt-related plus non-shuntrelated) which is similar to previous studies. As written above, older studies27 mentionedvery high shunt-related mortality rates compared to our 0.5%. This difference is hard toexplain. Probably several factors act together. In other studies, infections were an impor-tant cause of death. We found a low infection rate. Also, in our study only 45 patientsreceived a ventriculo atrial shunt. A probable cause of death in this type of shunt is pul-monary embolism. We did not observe this complication, whereas the older studies27
reported it as a major cause of death. Overall, it can be concluded that in Dutch hospitals very few patients die of shunt-relatedcauses.
28
2.4 Conclusions
2.4.1 Summary of previous conclusionsFrom this study it is clear that the revision rate after shunt operation in Dutch neurosurgi-cal centers is low compared to other studies. Proximal dysfunction is the most frequentreason for shunt revision. Valves cause shunt problems in a minority of cases: only 35cases (17,5%) overall. Similar for distal shunt problems. If distal problems occur at all,they are usually caused by an initial malplacement of the abdominal catheter in the pre-peritoneal fat layer, or migration later on.
The infection rate after primary shunt insertion in the Netherlands is rather low (over-all 5,5% and 3% after primary insertions). External ventricular drainage increases thechance of infection. Young age is a risk factor for infection. If infection occurs, it willmostly be in the first postoperative months. In Dutch hospitals, CSF shunt infection istreated according to the ‘gold standard’ by Gardner et al.58. This method of treatment isvery efficient. Complications of infection are rare and the cure rate is high.
Overall, age is the most important determinant of shunt dysfunction. This can beexplained by the occurrence of risk-increasing etiologies in the youngest age group, theweaker general condition of, especially, preterm infants and also the immaturity of theimmune system of these infants.
The experience of the surgeon does not influence the time spent in the operating roomor the need for a later shunt revision. There is no preferential drainage route for CSFshunts: VA and VP shunts show equal rates of complications, and there is no difference incomplications between frontal, parietal and occipital drainage routes.
In the youngest age groups, the Orbis Sigma valve causes less complications than dif-ferential pressure valves. In the adult group, there is no difference in the number of com-plications between the Orbis Sigma valve and the differential pressure valves. In shuntsystems incorporating the Raimondi valve, the revision rate is high. This cannot beexplained by an increased rate of distal dysfunction.
A short ventricular catheter predisposes to shunt obstruction. A possible mechanism forthis might be ‘pseudoretraction’. After the excess of cerebrospinal fluid has been drainedto the abdominal cavity, the ventricles shrink and the ventricular catheter may retract intothe brain parenchyma. A long abdominal catheter poses no problems in any of the agegroups. There is no need to refrain from using long abdominal catheters in infants underone year of age. In fact, putting in a longer abdominal catheter might prevent a later revi-sion to lengthen the shunt.
Neither moderately elevated CSF protein nor a high erythrocyte count caused addi-tional problems in CSF shunting in our study. Shunts functioned successfully in patientswith a CSF protein concentration as high as 3.5 g/l or, exceptionally, CSF with erythro-cyte counts above 20.000 cells/µl.
Morbidity, defined as ‘added’ morbidity after shunting, and shunt-related mortalityare very low in this study. A reasonable conclusion here can be that CSF shunt operationsin the Netherlands harbour little adverse consequences for the patient.
29
2.5 Future directions
Although Dutch CSF shunt surgery has low morbidity and mortality rates, there are stillmany complications. Recommendations for the future resulting from this study could bethe following:
1. As the Orbis Sigma valve has been shown to cause significantly less shunt dysfunc-tion in young patients than differential pressure valves, we would recommend toincorporate this valve in all CSF shunt systems in children under 15 years of age.
2. Our results justify a prospective randomized trial to compare the Orbis Sigma valvewith differential pressure valves in a selected group of adult patients. These patientsshould be patients with an expected low shunt flow rate, for example NPH patients.
3. To further decrease the infection rate, preventive measures should be aimed speciallyat the youngest age groups, in which the infection rate is highest. In these high-riskpatients, shunt impregnation with antibiotics as well as a strict peri-operative protocolmight be useful.
4. In 1998 Rekate106 stated: ‘The best shunt is no shunt’. Further use and improvementof endoscopic techniques such as the use of laser125 may decrease the need for shuntsin the future.
5. Our study did not include the quality of life in the evaluation of shunt functioning. AsAschoff et al.15 mentioned, the patient’s quality of life is more important than thenumber of shunt revisions. Patients requiring several shunt revisions, may actuallyhave an excellent quality of life. We therefore recommend future studies in which thequality of life should be evaluated.
30
Chapter 3 Cerebrospinal fluid dynamics and hydrocephalus shunts
Introduction
To understand the mechanism of shunt functioning and shunt dysfunctioning, it is neces-sary to know the normal CSF dynamics and CSF composition and also to know the vary-ing physical properties of the different shunt systems. In addition, an overview of the cur-rent knowledge of interactions between shunts and CSF and the causes of shunt dysfunc-tions might be valuable. Therefore, this chapter will give background information on CSFhydrodynamics and shunt physiology.
3.1 Cerebrospinal fluid dynamics
3.1.1 CSF flow and productionUnder normal physiological circumstances, CSF is largely produced in the choroid plex-us (50-80%)76. In addition, there is extrachoroidal production of which the actual extentand location is unknown. The assumption that the spinal subarachnoid space was respon-sible for the extrachoroidal CSF production was rejected by Marmarou in 197384 andSahar in 1972108. The ventricular wall has been reported to produce as much as 30% ofthe extrachoroidal CSF76. Choroidal CSF is secreted into the ventricles and exits thefourth ventricle through the midline foramen of Magendie and the lateral foramina ofLuschka into the cisterna magna and juxta brain stem cisterns. Some of the CSF flowsdorsally by the intracranial subarachnoid spaces and cisterns toward the convexities ofthe brain3. Here it is absorbed through the arachnoid granulations into the venous system.The rest of the CSF descends around the spinal cord and is absorbed into the extensivevenous network surrounding the spinal cord76.
The CSF is secreted continuously at a normal rate of around 0.34 ml/min. In 1966,Rubin107 found a rate of 0.37 ml/min; In 1968 Cutler32 reported a rate of 0.35 ml/min. Hefound a reduced production of 0.30 ml/min in hydrocephalus patients. On the other hand,in patients with a plexus papilloma, rates of 1.05 to 1.43 have been reported84,90. The cur-rent hypothesis for the mechanism of CSF secretion is based on the assumption that theosmotic gradient which attracts the bulk water of secreted CSF, is caused by active Na+
transport toward the ventricle by the Na+/K+-ATPase of the choroid epithelial cell60.Similarly, a Na+K+/2Cl- cotransporter is directed to the ventricle. Na+ in the cell is pro-
31
vided by an Na+/H+ exchange system, H+ and HCO3- are obtained by the action of car-
bonic anhydrase on H20 and CO2. HCO3- is exchanged for Cl-. There are several factors
influencing CSF formation rate60. A high CSF osmolarity is known to increase the CSFformation rate. On the other hand, a high plasma osmolarity decreases the CSF formationrate. The pH is also mentioned as having an influence on CSF production. A metabolic orrespiratory alkalosis reduces CSF production, whereas a metabolic or respiratory acidosishardly influences the formation rate. Another factor is the cerebral perfusion pressure,being the difference between arterial blood pressure and intracranial pressure. Animalexperiments showed that raising intracranial pressure did not reduce CSF formation rateas long as the cerebral perfusion pressure was maintained above a certain level. Loweringarterial blood pressure reduced CSF production. Raising CSF pressure lowered the CSFformation rate. Studies in hydrocephalus patients showed that CSF production decreasedwith 0.003 ml/min per mm CSF pressure elevation. Several drugs have been reported toinfluence CSF formation rate. Acetazolamide and ouabain inhibit CSF production byinhibition of carbonic anhydrase and the Na+/K+-ATPase, respectively. Also, dexametha-son (by inhibiting the Na+/K+-ATPase) and the diuretics furosemide and chlorthiazide (byinhibiting the Na+K+/2Cl- cotransporter) reduce CSF formation. Spironolacton and chol-era toxin stimulate CSF production. Of the hormones, the atriopeptins (Atrial NatriureticFactor, ANF) diminish CSF production. Hypothermia is known to reduce CSF formationas much as 11% per degree centigrade between 31o and 41oC60.
3.1.2 CSF absorptionThe most important sites of CSF absorption are the arachnoid granulations on the cerebralconvexities3 as well as the villi in the spinal subarachnoid space. Other possible sites havebeen reported by McComb in 198386. In a review he described several reports of lym-phatic drainage of CSF and also some reports on CSF absorption by the choroid plexus.Earlier, alternative absorption sites where reported by DiChiro et al in 197240 and byBradbury in 198021 . DiChiro described CSF drainage through the olfactory nerve path-way; Bradbury and Cole showed drainage to cervical lymph nodes through the optic ner-ve sheath. The resistance to absorption is low, so that a normal individual can absorb CSFat a rate three to four times the normal rate of CSF formation. The colloid-osmotic pres-sure existing between the virtually protein-free CSF and plasma may be an important fac-tor affecting absorption. Another factor is the CSF hydrostatic pressure. The rate ofabsorption increases linearly with CSF pressure76. The exact mechanism of absorption isunknown. Possible mechanisms could be that lining cells of the arachnoid granulationscontain vesicles that move material across the cell by pinocytosis or existing76 intracellu-
lar channels and possibly passages or tubules that may move material through the cell .
3.1.3 CSF composition As described above, CSF is not just a protein-free plasma filtrate76. CSF has a lowerpotassium and calcium concentration than plasma, whereas sodium and chloride concen-trations are higher (see table 3.1). The blood-brain barrier has a selective permeability to
32
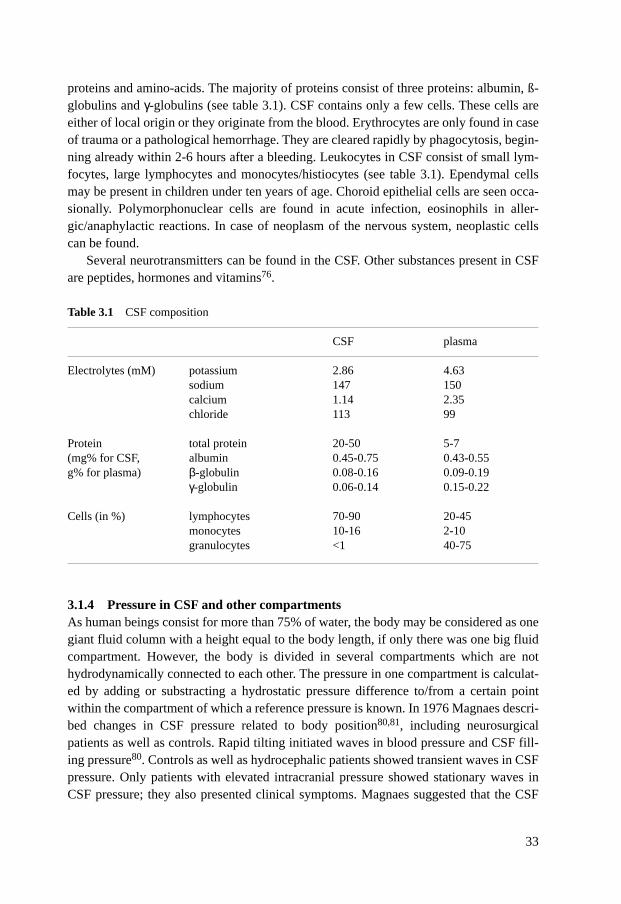
proteins and amino-acids. The majority of proteins consist of three proteins: albumin, ß-globulins and γ-globulins (see table 3.1). CSF contains only a few cells. These cells areeither of local origin or they originate from the blood. Erythrocytes are only found in caseof trauma or a pathological hemorrhage. They are cleared rapidly by phagocytosis, begin-ning already within 2-6 hours after a bleeding. Leukocytes in CSF consist of small lym-focytes, large lymphocytes and monocytes/histiocytes (see table 3.1). Ependymal cellsmay be present in children under ten years of age. Choroid epithelial cells are seen occa-sionally. Polymorphonuclear cells are found in acute infection, eosinophils in aller-gic/anaphylactic reactions. In case of neoplasm of the nervous system, neoplastic cellscan be found.
Several neurotransmitters can be found in the CSF. Other substances present in CSFare peptides, hormones and vitamins76.
3.1.4 Pressure in CSF and other compartmentsAs human beings consist for more than 75% of water, the body may be considered as onegiant fluid column with a height equal to the body length, if only there was one big fluidcompartment. However, the body is divided in several compartments which are nothydrodynamically connected to each other. The pressure in one compartment is calculat-ed by adding or substracting a hydrostatic pressure difference to/from a certain pointwithin the compartment of which a reference pressure is known. In 1976 Magnaes descri-bed changes in CSF pressure related to body position80,81, including neurosurgicalpatients as well as controls. Rapid tilting initiated waves in blood pressure and CSF fill-ing pressure80. Controls as well as hydrocephalic patients showed transient waves in CSFpressure. Only patients with elevated intracranial pressure showed stationary waves inCSF pressure; they also presented clinical symptoms. Magnaes suggested that the CSF
33
Table 3.1 CSF composition
CSF plasma
Electrolytes (mM) potassium 2.86 4.63sodium 147 150calcium 1.14 2.35chloride 113 99
Protein total protein 20-50 5-7(mg% for CSF, albumin 0.45-0.75 0.43-0.55g% for plasma) β-globulin 0.08-0.16 0.09-0.19
γ-globulin 0.06-0.14 0.15-0.22
Cells (in %) lymphocytes 70-90 20-45monocytes 10-16 2-10granulocytes <1 40-75

pressure waves were related to changes in cerebral blood volume, probably reflecting thepostural blood pressure wave and autoregulation. He also looked at the level of the zeroCSF pressure point, which is the point at which the fluid pressure is equal to atmosphericpressure, and the hydrostatic indifferent point (HIP)81. The HIP is the point at which thefluid pressure in a sitting position equals the pressure in a lateral position43. In a sittingposition, the pressure in the caudal part of the neuraxis increases, varying from 320 to 630mm H2O with a mean of 490 mm H2O. Thus, the mean level of zero CSF pressure in a sit-ting position will be 49 cm above the level of lumbal puncture. This corresponds to a zeroCSF pressure point at the level of the first cervical disc, or the base of the neck. In hydro-cephalic patients the HIP, and thereby the zero CSF pressure point, was shifted caudallyafter shunting. The pressure decrease was larger in a sitting position than in a lateral posi-tion. Clinically, this means that the zero pressure point may be a useful variable in controlof CSF shunt function.
The pressure in the right atrium is slightly positive compared to atmospheric pres-sure43. The pressure in the peritoneal cavity depends on the place where it is measured,the abdominal contents, the abdominal wall musculature tone, etcetera43. Overall, perito-neal pressure can be considered basically equal to atmospheric pressure. Intrapleuralpressure is consistently subatmospheric due to the characteristics of the chest wall.
3.2 Pressure, resistance, flow and viscosity in a shunt system
A shunt system is intended for transport of liquid from a high-pressure compartment to alow-pressure compartment. The shunt system is built up from a series of tubes intercon-nected by a valve. The valve is a mechanical resistance device which regulates flow. Todescribe valve functioning, four basic principles of fluid dynamics are important: pres-sure, flow, resistance and viscosity43.
3.2.1 PressurePressure (p) can be defined as the force (F) per unit area (A). This definition is expressedin the following equation:
P = F–A
(1)
The s.i. units of these variables are: P in N/m2, F in N, A in m2. A fluid column with a height h (m) having a density of mass ρ (kg/m3) generates a hydro-static pressure P of:
P = h.ρ.g (2)
where g (m/s2) is the gravity acceleration.
34
3.2.2 FlowThe amount or volume V (m3) of fluid that passes a cross sectional area A (m2) of thetransport system per second is defined as flow, ϕ (m3/s).
3.2.3 ResistanceFlow depends on the difference in pressures (∆P=P2-P1) of the two compartments and theresistance R. The resistance (N/m2.s) can be calculated according to the next equation:
R = P1–P2
ϕ(3)
The pressure difference generates a force on the particles of the fluid, thereby causing aninitial acceleration. This results in velocity of the particles. Moving particles undergo areversely directed force that is caused by friction between the particles among themselvesand also between the particles and the inner wall of the tube or other parts of the transportsystem. Particles near the wall show velocities close to zero, whereas particles at the axishave maximum velocities. The way the velocity is distributed along the cross-section of atube is referred to as the profile of the velocity. A profile may express a laminar or turbu-lent flow pattern. At a turbulent flow, R depends on flow velocity, whereas at laminarflow, R does not depend on flow. Excluding transient moments of high pressure due to,for example, coughing, CSF shunt systems will expose laminar flow. It is possible to cal-culate R with Poiseulle‘s law:
ϕ = π.r4.∆P
(4)8.L.η
where L (m) is the length of a tube with inner radius r (m) and η (in N.s/m) the viscosityof the fluid. Substituting 3 into 4 yields:
R = 8.L.η
(5)π.r4
The flow ϕ strongly depends on the dimensions of the shunt system expressed in radius(fourth law relation), pressure difference (∆P), length (L) and viscosity (η). Viscositydepends on many factors among which is the temperature (see 3.2.4).
3.2.4 ViscosityViscosity is the resistance of a fluid against shear forces. Water has the lowest viscosity inour system. Adding protein to water increases viscosity. Blood e.g., has a rather high vis-cosity. Viscosity is influenced by temperature. If the temperature increases, the viscositydecreases.
35

In shunt physiology, viscosity is relevant in two respects: firstly the temperature depen-dence of viscosity, secondly the influence of viscosity on resistance and flow. InPoiseuille’s law (equation 4), resistance is a linear function of viscosity: if viscosity dou-bles, resistance will double.
3.2.5 SiphoningIn physiologal conditions, cerebrospinal fluid circulation is hardly influenced by bodyposture, because there is only a slight difference in hydrostatic pressure between the sitesof CSF production and absorption into the sagittal sinus33 and the other absorption sites.The positive pressure difference, which is usually about 2-3 mm Hg, facilitates CSFabsorption.
However, in patients treated with ventriculoperitoneal shunts, CSF is drained from theventricles to the abdominal space. The hydrostatic pressure difference between these sitescan be as high as 60-80 cm H2O, depending on body position. This difference may accel-erate drainage of fluid from the site of higher pressure to that of lower pressure. In a supi-ne position the intracranial pressure in patients with CSF shunts is comparable to that inhealthy persons. The normal intracranial pressure in an upright position is -65 mm H2O,indicating that a zero intracranial pressure level exists at 65 mm below the brain vertex.However, as mentioned above, this normal upright intracranial pressure cannot be main-tained by differential pressure shunts because of the extra hydrostatic pressure due to thedifference in height between the endings of the ventricular and the peritoneal catheters56.Problems of overdrainage may occur. E.g., in an infant with a fluid-filled shunt system of30 cm in length, there will be a 30 cm difference in height between the proximal and dis-tal end of the shunt system in the upright position, which corresponds to a pressure differ-ence of 300 mm H2O. This may entirely abolish the effect of low and medium pressurevalves.
To maintain a normal upright intracranial pressure, an anti-siphon device (ASD) canbe used. Another name for this device is a zero pressure device.When upright, it acts as aclosing valve by means of a mobile membrane that moves in response to a difference inpressure across it. CSF flow is allowed to occur as long as there is a positive intracranialpressure above the level of the anti-siphon device. If the intracranial pressure above thelevel of the ASD drops to zero, the membrane will be pushed against the orifice, therebyincreasing the resistance to flow, preventing further siphoning43.
Gruber et al. in 198461 as well as Tokoro in 1994120 found that an ASD was effectivein preventing overdrainage in adults and children. Tokoro showed that an ASD was lesseffective in children than in adults. Gruber reported that the use of an ASD in connectionwith the regular shunt system reduced the number of complaints and shunt dysfunctionsover a period of more than 6 years.
3.2.6 Measuring flow in shunt systemsDuring the past decades, much effort has been spent on measuring fluid flow in shunt sys-tems. Percutaneous thermistors28,59, thermosensitive liquidcrystals (chameleon print)131
36
and clearance of isotopes75,85 have been used to measure flow. All these methods had thedisadvantage that they could only be used for a short period. In 1983, Hara65 presented amodel for measuring flow in shunts which was based on air bubbles induced by electrol-ysis within the shunt system which could be observed by an ultrasonic Doppler technique.This system enabled measurements for longer time periods. Hara described 24-hour flowpatterns in two patients. The flow varied between 0.05 and 0.78 ml/min. In 1987Kadowaki69 ,used the same method and found a flow varying from 0.01 ml/min to 1.93ml/min. Both authors reported circadian rythms in the flow patterns with peaks in themorning and at night during REM sleep phases. This nocturnal increase in intracranialpressure could be related to intracranial vasodilation. Also, shunt flow was influenced bychanges in body position as well as increases in intracranial pressure acting due toincreases in intrathoracal pressure or abdominal pressure.
3.3 Shunt materials
Shunts tend to be in contact with the brain and CSF for prolonged periods of time. Inaddition, a well-functioning shunt system is important to the patient’s well-being. Thebottom line for the material constituting shunts is biocompatibility43. Several factors per-taining to biocompatibility are: cytotoxicity, sensitization, irritation, intracutaneous reac-tivity, genotoxicity and hemocompatibility. Only in the long run, acute or chronic toxicityand carcinogenicity are important. Materials should be chemically highly inert to be usedfor shunts safely.
Only a few materials are currently used in shunt systems. The most frequently usedmaterial is silicone rubber. It is used in catheters, valves and access chambers and anti-siphon devices. Some of the very favorable properties of silicone rubbers are their ther-mal stability, their resistance to oxidation and ozone, their chemical inertia to manychemicals, their low surface energy and their high gas permeability. Stainless steel, syn-thetic ruby, titanium and plastics are other components of shunt systems. These materialsare mainly used in valves or needle stops.
In 1987,Echizenya et al.45 conducted a study on 25 shunts that had been implanted for6 days to 10 years. Four shunts showed surface deposits of calcium phosphate, probablycaused by mechanical stress. In addition, surface wrinkles, microscopic holes and tinyparticles which appeared to be aluminium crystals could be found. Echizenya et al. sug-gested these changes to be caused by degradation of the silicone rubber. The physicalproperties indicated a progressive change with a considerable deterioration after implan-tations of more than 5 years. In 1991, Schoener et al.113 studied explanted catheters andvalves by electron microscopy. In 19 out of 36 systems they observed a foreign-bodyreaction. Dysfunction occurred in 22 out of 36 valves. In a 1994 study by Brydon et al.23
on 43 explanted shunt valves, a dysfunction rate of 77% was found. Valves with metalcomponents had a high tendency to accumulate debris. On the contrary, only a few poly-mer valves showed accumulation of debris. Also, only the polymer valves functioned
37

well after infection, whereas five out of six valves containing metal components per-formed badly. In a recent review38 on shunt complications dealing with tissue reactions,Del Bigio reported that cellular debris or blood can cause dysfunction of valve compo-nents. Moreover, chronic inflammation could contribute to degradation of shunt compo-nents, whereas glial tissue or choroid plexus were found to infiltrate ventricular cathetersdriven by mechanical pressure.
These studies show the need for further investigations on improvement of biocompat-ibility and biodurability of shunt systems. In conservative treatment of shunt infection,success might depend on the material and construction of the valve.
3.4 Valve mechanics and valve types
3.4.1 Valve mechanicsBasically, a valve is a device which opens and permits flow when a certain pressure levelis exceeded8. Below that pressure the valve is closed.
The opening pressure refers to the pressure level at which the valve opens, whereasthe closing pressure is defined as the pressure level when the valve closes during decrea-se of pressure. The mechanical behavior of the material, with emphasis on silicone rub-bers of which parts of the valve can be composed, is the reason for differences betweenopening and closing pressures. Silicone material is easy to deform, has a non-perfect elas-ticity and may have adhesive properties.
The static characteristics of a valve can be presented in a flow-pressure (ϕ-P) curve.Figure 3.1 shows some examples. Fig. 3.1a represents an ideal valve: opening pressureequals closing pressure. Below the opening pressure the valve acts as an infinite highresistance that completely blocks the flow, whereas at the opening pressure any forwarddirected (positive) flow is allowed passage. Fig. 3.1b is typical for a valve performingbadly. The sharp transition at the opening pressure is replaced by a gradual changingcourse which also allows negative directed flows which implies leakage.
The shape of the silicone material tends to adapt slowly to altered flow conditions. Asa result there is a bad reproducability of the flow-pressure relationship when comparingthe curves resulting from a low to a high flow and reverse. This effect of non-reprodu-cability is called “hysteresis”. The dynamic behavior of the elastomere material can bevisualized in pressure-time (P-t) plots at a step function flow input. Before the step func-tion the flow is zero. A flow-controlled circuit forces a predefined flow to settle regardlessof the pressure. At the onset of the flow step function, the pressure starts at zero level andwill gradually increase until the valve opens. The gradual course is due to the complianceof the tubing material and other parts of the valve feeding circuit. Fig. 3.2 shows someexamples of different material behavior. Fig. 3.2a represents a well-functioning valvewith no adhesive behavior and a time-independent curve. The pressure increases towardsthe opening pressure and reaches without too much delay the asymptotic level whichbelongs to the flow value. Fig. 3.2b shows an increase to a high pressure level which is
38
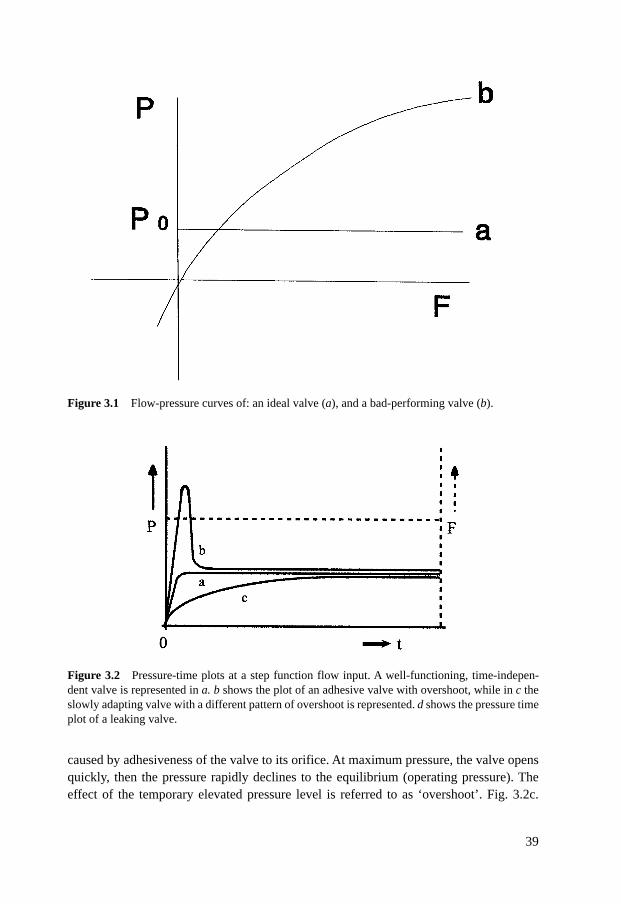
caused by adhesiveness of the valve to its orifice. At maximum pressure, the valve opensquickly, then the pressure rapidly declines to the equilibrium (operating pressure). Theeffect of the temporary elevated pressure level is referred to as ‘overshoot’. Fig. 3.2c.
39
Figure 3.1 Flow-pressure curves of: an ideal valve (a), and a bad-performing valve (b).
Figure 3.2 Pressure-time plots at a step function flow input. A well-functioning, time-indepen-dent valve is represented in a. b shows the plot of an adhesive valve with overshoot, while in c theslowly adapting valve with a different pattern of overshoot is represented. d shows the pressure timeplot of a leaking valve.

shows a very slowly increasing pressure to the equilibrium level. This can be explainedby a leaking valve and the slowly (reversely) adapting shape of the valve mechanism.
3.4.2 Valve types most commonly used in our clinical study
Ball and spring valve
The mechanical principle of this type of valve is a metallic spring exerting force on a ballwhich is located at a conical orifice that can be occluded by the ball43. The ball used to bemade of metal, but currently it is made of industrial corrundum (saphire or ruby). Thehydrodynamic characteristics of this valve depend on tension and deformability of thespring on one hand and of the cone shape and diameter on the other hand. Because sili-cone rubber is not used in this valve, there are no problems like hysteresis and ‘drift’. Thisvalve does incorporate an ‘on/off’ principle, leading to a high flow immediately after theopening of the valve which might bring an increased risk of overdrainage. The spring ballvalve we tested was the Hakim valve (see chapter 4).
Diaphragm valves
The principle of this type is based on a mobile and flexible silicone membrane whichmoves in response to pressure differences, leading to a circular flow pattern43. The hydro-dynamics of this valve depend on elasticity, tension and thickness of the membrane aswell as on shape and size of the orifice in the valve. There is a risk that at excessive pres-sure differences the membrane may collapse. Another problem is the non-linear increasein resistance of the membrane with enlargement of its surface which may lead to over-drainage. Because the valve is made of silicone, basic problems as hysteresis and driftmay arise. We tested three diaphragm valves of this type: PS medical, Pudenz and Accu-flo (seechapter 4).
Complex valves
The complex valve we tested in the laboratory was the Orbis sigma valve (see chapter 4).This valve consist of an extremely delicate mechanism. A tight conical cylinder is insert-ed into a ring which is attached to a pressure-sensitive silicone membrane43. The innerdiameter of the ring is slightly larger than the outer diameter of the conical cylinder. Thedistance between cylinder and ring varies with the pressure, leaving more or less spacefor the passage of CSF. The system is vulnerable and sensitive to increased proximal pres-sure. The membrane is easily damaged, and the ring or cylinder may dislocate. The flowvalve has the smallest outlet of all valves (<0.01mm).
The whole concept is based on the rate of CSF production, which is about 20-25 mlper hour in adults in a normal situation. The small outlet of the Orbis sigma flow-valveonly allows a maximum flow of 25 ml per hour and protects adequately against over-drainage. In 1987, Kadowaki et al.69 reported that during nightly REM fases CSF produc-tion may amount to 60 ml per hour. This may invoke problems of underdrainage when
40
this valve is used. Also, the small outlet of the Orbis Sigma valve is prone to obstruction.Schoener et al. (1992)113 conducted electron microscopic studies on explanted orbisSigma valves and observed disturbances in the shape of the valve as well as evidence oflocal immune reactions around the cylinder. Aschoff also expressed his doubts on thefunctioning of the Orbis Sigma valve11,12 with regard to the small outlet of the valve, aswell as the rigid flow limitation.
Slit valves
These valves consist of a ’slit’ in a silicone layer43. The principle is based on memoryproperties of silicone: after deformation the material will resume its original shape, whichmay take a variable time in the range of seconds to days. There are two types of slit val-ves: proximal and distal slit valves.
The proximal valves consist of either a side slit at the lower catheter-end, or they mayhave one or multiple slits at the upper end. Proximal slit valves we tested were the Holtervalve and Phoenix valve. Distal slit valves consist of a closed silicone catheter with slitsof varying length and number at the distal end. We tested the Raimondi valve as the onlydistal slit valve.
This type of shunt has little resistance to flow because there are no flow-restrainingelements in the system. An increase in resistance of the whole system can be obtained byreducing the inner diameter of the connecting catheters.
3.5 Protein concentration and shunt functioning
In 1969, Rayport and Reiss105 and in 1970 Hakim et al.64 reported that an increase in pro-tein concentration resulted in an equal64 or higher105 flow capacity with Hakim valvesand decreased flow capacities in other valve types. In 1968, Steinke119 also concludedthat an increased protein concentration impaired valve functioning and therefore decreas-ed flow which was confirmed by Schubert et al. in 1979114.
However, in most of the early experiments testing CSF valves, the influence of chang-es in temperature was not tested. Tests were conducted at room temperature (21oC), instead of body temperature (37oC). This lower temperature alone resulted in a consider-able increase in viscosity, a restriction of flow and eventual occlusion of the catheter aswell as the valve. This was reported by Van der Veen in 1972126 and stated again byBrydon et al. in 199524.
In 1973, Jährig and Steiner67 included temperature in their study of the correlationbetween total CSF protein and viscosity and they reported that at a stable temperature the-re was a direct correlation between CSF composition and viscosity. In their studies, theyrelated CSF viscosity to that of distilled water at the same temperature. Using this method,they found that the relative viscosity increased linearly with elevations of CSF protein upto a concentration of 60 g/l. In 1972, Van der Veen126 concluded that for protein concen-trations less than 8.5 g/l, increases in viscosity could not be responsible for shunt mal-
41

functioning. He also tested at a constant temperature. He did mention, however, the pos-sibility of the presence of fibrinogen in high-protein CSF with the risk of clotting andshunt obstruction. In 1990, Aschoff et al.10 tested valves at an albumin concentration of 5g/l and compared these results with a control group tested without addition of protein. Nodifference was found. In 1992, Pudenz et al.102 were not able to detect any differences inhydrostatic properties of valves perfused with an artificial CSF containing 4 g protein/leither. Valve dysfunction occurred, however, with protein solutions of 15 g/l,. Accordingto Pudenz et al. these dysfunctions were caused by obstruction through fibrin particlesand cryoglobulin aggregates. It must be remarked, that normal CSF does not containfibrin particles.
Brydon et al. (199524; 199626) investigated the relation between CSF protein concen-tration and absolute viscosity at 37oC in 126 CSF samples with varying protein concen-trations (50%< 0.5 g protein/l, 80%< 2.0 g/l, 11% > 3 g/l). It turned out that the proteinconcentration hardly influenced CSF viscosity24. When flow of the most viscous CSF(9,5 gramms protein/liter) was compared with flow of the least viscous CSF (<0,45 g pro-tein/liter), it was observed that the flow of CSF with the highest protein concentration wasonly reduced by 7% compared to that of CSF with the lowest protein concentration. Also,they rejected the theoretical possibility of high protein concentration leading to valvesticking. In a subsequent report25, Brydon et al. described the effect of protein concentra-tion on the functioning of shunt valves. A high surface tension tends to disturb the open-ing of a valve in the way a layer of water hinders the lifting of a flat object from a table.The addition of protein to water (or CSF) will decrease the surface tension and facilitatethe opening of the valve. Surface tension also depends on the angle of contact betweenthe surface of a solid substance and a liquid, which per se depends on the degree of hydro-philic and hydrophobic interactions. In the study in which the surface tension in CSF withvarying protein concentrations was measured, it appeared that the surface tension de-creased with rising protein concentrations. Above the concentration of 1 g/l, increasingprotein had no effect on surface tension. In practice, the opening pressure of valves willbe reduced by this decrease in surface tension.
Thus, at body temperature, a high protein concentration of up to 9 g/l only slightlyincreases CSF viscosity and in this way does not impair shunt functioning. On the otherhand, a high protein concentration reduces surface tension and lowers the opening andclosing pressures. This is supported by clinical results: back in 1965 Eckstein46 reportedsuccessful shunt functioning in the presence of a protein concentration as high as 40 g/l.It must be remarked however, that under certain pathological conditions, high total pro-tein levels may be associated with the appearance of fibrinogen in the CSF5,126. Thisfibrinogen can polymerize and form fibrin clots which obstruct the shunt102,126. In thatcircumstance, high protein levels can cause shunt dysfunction.
42

3.6 Blood and shunt functioning
Several authors110,129 have pointed to the adverse effect of high numbers of erythrocyteson shunt functioning in vivo. In 1984, Walters et al129 reported that an erythrocyte countof more than 1000/µl would increase the risks of shunt dysfunction. In 1993, Sainte Roseet al110 stated that placing a ventricular catheter in a ventricle full of blood was ‘doomedto failure’. The negative effects of an increased erythrocyte count on shunt functioning invivo is probably not to be attributed to an increase in viscosity. In 1973, Jährig andSteiner67 reported that erythrocyte or leucocyte counts of up to 50.000/µl only influencedviscosity in the third decimal. The only report on in vitro testing26 of shunt systems withCSF containing varying erythrocyte counts was by Brydon et al. in 1996. He perfusedvalves with blood suspensions containing 10.000 to 50.000 erythrocytes/µl. Perfusion ofHakim and PS medical valves with CSF containing 10.000 erythrocytes/µl did not showany impairments in valve functioning. At higher concentrations, opening as well as clos-ing pressure increased, as did the difference between opening and closing pressure. Also,in some cases, the valve’s closing time increased from 5 to 15 minutes. This was explai-ned by erythrocyte sedimentation which might have affected the closing of the valve.Obstruction may also occur because of adhesions mediated by platelets.
43
Chapter 4 Laboratory study on hydrocephalus shunt valves
4.1 Valve testing in a laboratory setting
In an experimental setting we perfused the valves with saline and compared our resultswith the valve specifications as given by the manufacturer. Afterwards we focussed on thevalve’s behavior in the presence of CSF contamination with protein or blood. As men-tioned before in chapter 3, changes in CSF composition for protein and/or erythrocytesmay induce dysfunctioning of the valve. In our experimental setting we tested the pres-sure-flow characteristics of the eight most frequently used valve types of our clinical stu-dy.
In vivo there are large variations in CSF dynamics. Differences in pressure and floware not only found between individuals, but also within one person. This can be explainedby dynamical variations in heart and bloodvessels, respiration, contraction of muscles andstatical influences due to changes in body position. To study the effect of these dynamicvariations on valve functioning, these variations should be mimicked in an experimentalsetting.
4.1.1 Methods and materials4.1.1.1 Tested valvesIn the laboratory we tested the eight valves that were most frequently implanted in ourclinical study (see chapter 2).
The Hakim valve is a dual-spring ball valve that consists of a ruby ball held against acone-shaped seat (stainless steal) by a spring. The chassis is made of titanium (fig.4.1.1A).
The PS medical flow-control valve (contoured) is manufactured with a polypropylenebase invested in a smooth flexible silicone elastomer housing with a flat bottom and con-sists of a molded silicone elastomere membrane (fig 4.1.1B).
The Holter valve consists of two silicone slit valves with internal springs to preventinvagination of the slits. The valves are enclosed into stainless steel bodies separated by asilicone pumping chamber (fig. 4.1.1C).
The Phoenix Cruciform slit valve consists of two unidirectional silicone slit-valves,located at opposite ends of a silicone body. Each slit-valve is enclosed in a stainless steelhousing assembly (fig 4.1.1D).
The Accu-flo valve (burr hole design) consists of a flexible and ribbed silicone mem-
44
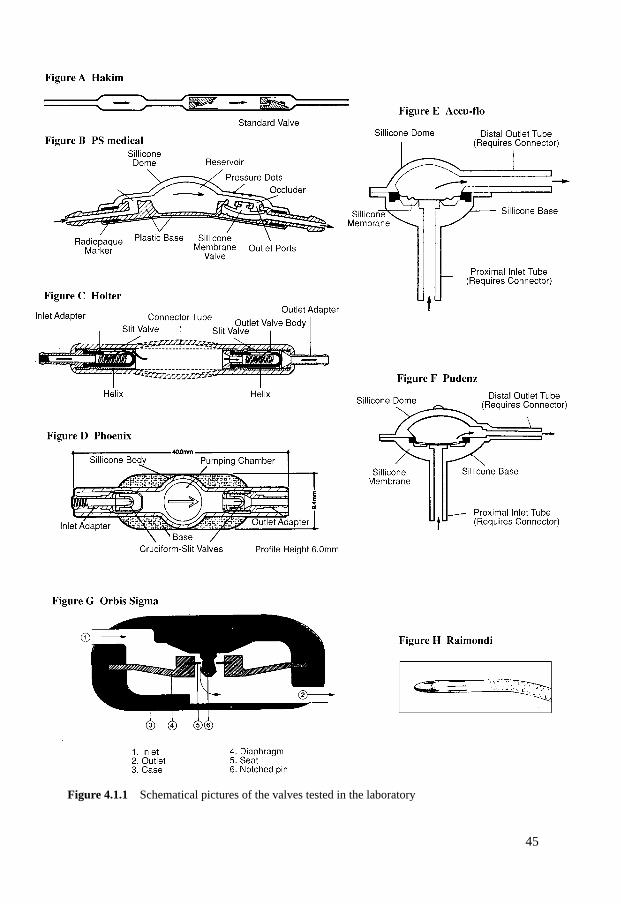
45
Figure 4.1.1 Schematical pictures of the valves tested in the laboratory
brane enclosed in a silicone base and covered with a silicone dome (fig. 4.1.1E).The Pudenz flushing valve (burr hole design) consists of a spherically-shaped silicone
elastomer device carrying a single silicone membrane diaphragm valve (fig. 4.1.1F).The Orbis Sigma valve consists of a flexible silicone diaphragm containing a synthet-
ic ruby ring seat that moves along a synthetic ruby flow-control pin dependent on diffe-rential pressure. The synthetic ruby pin is contoured in such a way that the openingaround the pin decreases as the diaphragm descends with increasing pressure. Thisincreases the resistance and limits the flow. The valve housing is of polysulphone encasedin silastic (fig. 4.1.1G).
The Raimondi peritoneal catheter consists of a silicone elastomer peritoneal catheterwith a distal-tip-slit valve. The slit-valve consists of four individual slits placed in thecatheter wall (fig. 4.1.1H).
4.1.1.2 Pump-driven versus pressure-driven test rigsIn an experimental laboratory set-up, hydrodynamic properties of valves can be measuredin different ways: a defined flow can be supplied and the flow resistance can be recorded(pump-driven system), or the pressure is defined and given and the resultant flow isrecorded (pressure-driven system)11.
A constant-flow test rig leads to an increasing pressure at the level of the valve.Because of the lack of compressibility of the fluid in the rigid shunt system, the transferfrom flow to pressure increase will be fast. With a continuous flow, the pressure willincrease in time until the opening pressure is reached and the valve opens. After openingof the valve, the pressure will increase a little more to an equilibrium (operating pres-sure). In a constant-flow system, the opening pressure will always be reached and eventu-ally be exceeded. The measurements can be related to the physiological generation ofCSF. Disadvantages of this constant-flow system are its sensitivity to artefacts (air bub-bles), especially at opening pressure, and the difficulty of testing the system in a pulsatileway (Aschoff, 199511).
In a pressure-driven test system, there are basically two possibilities: the pressure dif-ference is either too low and flow will not be initiated, or the pressure difference risesabove the opening pressure and flow is induced. The advantage of a pressure-regulatedsystem is the absence of artefacts (air bubbles are easily cleaned up by the system). A dis-advantage is the impossibility of registering the opening pressure. Also, a forced flow inthis sytem is not feasible11.
We chose a pump-driven system because this system is comparable to the physiologi-cal situation. The CSF production rate amounts to 20-25 ml.
4.1.1.3 Conditions for in vitro testing of shunt valvesThe system used in testing valves should possess the basic principles to determine valvecharacteristics, namely:a. The flow-pressure relationship
46

b. At a constant flow, changes in pressure express the reaction of the valve to perfusionwith a different test solution
c. The effect of pressure modulation on pressure at a constant flow.d. The changes in pressure after step-by-step elevation and arrest of flow. This shows the
valve characteristics during opening and closing.
Therefore, we postulated seven conditions to satisfactorily test shunt valves. 1. It must be possible to record pressure-flow relationships using a 0.9% NaCl solution,
with a flow range from 10 to 50 ml/h. 2. The flow should persist for at least 4 hours to study the short-term stability of the sys-
tem.3. Halfway the 4-hour flow period, large physiological pressure differences should be
simulated to mimic the situation in vivo.4. To judge stability and hydrodynamic valve properties, the test series must be repeated
with varying compositions of the test solution at a flow velocity of 25 ml/h. The pro-tein concentration of the test solution will be between 0 and 10 g/l; the maximumerythrocyte count will be 10.000 erythrocytes/µl.
5. The tests should proceed automatically following a fixed protocol.6. The temperature of the test solution should be maintained at 37oC.7. It should be possible to measure the flow directly in front of the valve, which allows
the assessment of the time to reach a steady-state situation at a new flow velocity.
4.1.1.4 Test rig set-upFigure 4.1.2 shows the essential elements of the test rig. The system consists of a pumpwhich is subsequently connected with the valve through a serial resistance. The valve isplaced at a predefined level within a water bath. At the valve inlet, a pressure gaugerecords the inlet pressure (P2) of the valve. The oulet opening of the efferent tube will beat the same height as the valve to avoid the need for correcting hydrostatic pressure differ-ences. The pressure over the valve will then be equal to P2. A second pressure gauge hasbeen placed proximal of the serial resistance. This gauge measures the pressure P1.
The instantaneous flow can be calculated by using equation 3 (see chapter 3):
ϕ = P1 - P2
R
The derived flow ϕ also reflects the dynamic flow variations induced by the pressuremodulator. Three identical systems were incorporated for testing simultaneously.
The temperature in the water bath is controlled by a system containing a thermal sen-sor connected to a Hewlett Packard type 78205B temperature module and a heating ele-ment. To maintain a homogeneous temperature in the waterbath, the water is stirred by anelectrically driven device. A separate temperature transducer monitors the temperature ofthe water bath.
47
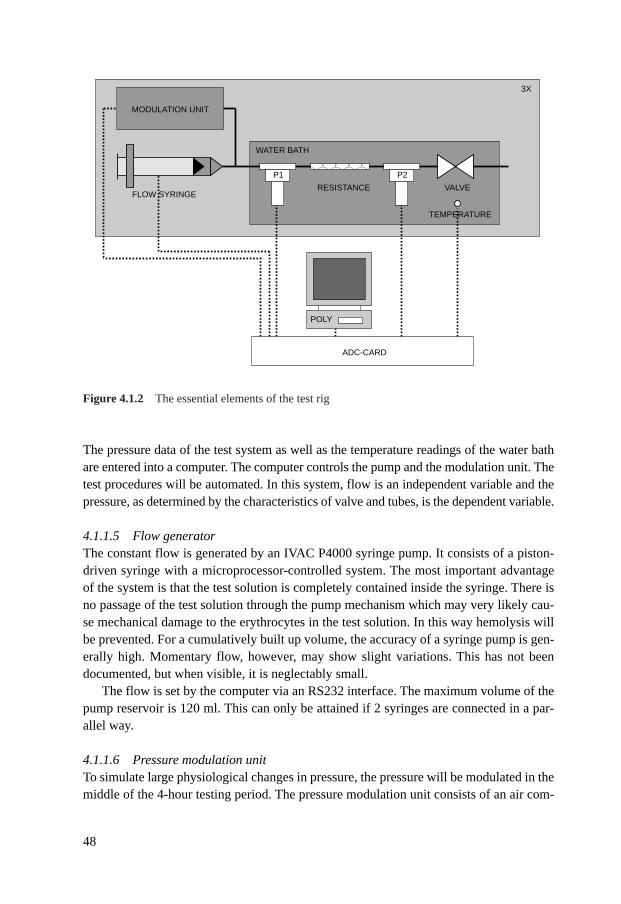
The pressure data of the test system as well as the temperature readings of the water bathare entered into a computer. The computer controls the pump and the modulation unit. Thetest procedures will be automated. In this system, flow is an independent variable and thepressure, as determined by the characteristics of valve and tubes, is the dependent variable.
4.1.1.5 Flow generatorThe constant flow is generated by an IVAC P4000 syringe pump. It consists of a piston-driven syringe with a microprocessor-controlled system. The most important advantageof the system is that the test solution is completely contained inside the syringe. There isno passage of the test solution through the pump mechanism which may very likely cau-se mechanical damage to the erythrocytes in the test solution. In this way hemolysis willbe prevented. For a cumulatively built up volume, the accuracy of a syringe pump is gen-erally high. Momentary flow, however, may show slight variations. This has not beendocumented, but when visible, it is neglectably small.
The flow is set by the computer via an RS232 interface. The maximum volume of thepump reservoir is 120 ml. This can only be attained if 2 syringes are connected in a par-allel way.
4.1.1.6 Pressure modulation unitTo simulate large physiological changes in pressure, the pressure will be modulated in themiddle of the 4-hour testing period. The pressure modulation unit consists of an air com-
48
MODULATION UNIT
FLOW SYRINGE
WATER BATH
3X
RESISTANCE VALVE
TEMPERATURE
��P1 P2
ADC-CARD
POLY
Figure 4.1.2 The essential elements of the test rig
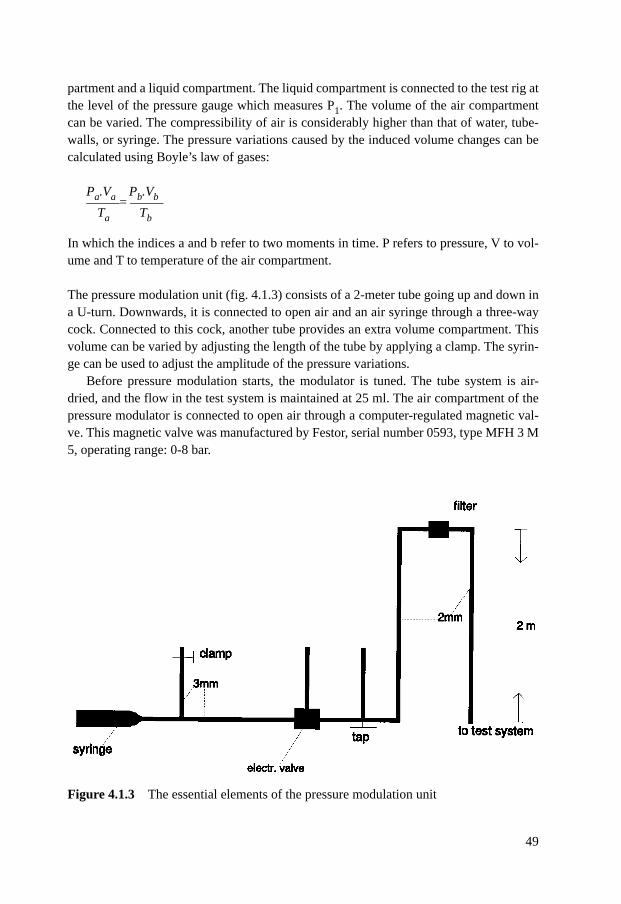
partment and a liquid compartment. The liquid compartment is connected to the test rig atthe level of the pressure gauge which measures P1. The volume of the air compartmentcan be varied. The compressibility of air is considerably higher than that of water, tube-walls, or syringe. The pressure variations caused by the induced volume changes can becalculated using Boyle’s law of gases:
Pa.Va Pb.Vb_____= _____Ta Tb
In which the indices a and b refer to two moments in time. P refers to pressure, V to vol-ume and T to temperature of the air compartment.
The pressure modulation unit (fig. 4.1.3) consists of a 2-meter tube going up and down ina U-turn. Downwards, it is connected to open air and an air syringe through a three-waycock. Connected to this cock, another tube provides an extra volume compartment. Thisvolume can be varied by adjusting the length of the tube by applying a clamp. The syrin-ge can be used to adjust the amplitude of the pressure variations.
Before pressure modulation starts, the modulator is tuned. The tube system is air-dried, and the flow in the test system is maintained at 25 ml. The air compartment of thepressure modulator is connected to open air through a computer-regulated magnetic val-ve. This magnetic valve was manufactured by Festor, serial number 0593, type MFH 3 M5, operating range: 0-8 bar.
49
Figure 4.1.3 The essential elements of the pressure modulation unit
The pressure P1 results from the height of the fluid column in the ascending part of themodulator tube. After stabilisation of P1 the connection to open air will be blocked. Theinitial pressure within the system is equal to the atmospheric pressure. In addition, themodulation syringe is switched on. The piston of the 20 ml syringe makes cyclic move-ments, driven by an engine (Crouzet Synchro engine; Rapor 25/4; speed 375 rpm). Thefrequency of modulation is 1 Hz or 60 rpm. The amplitude of the piston in the syringedetermines the cyclic volume changes which are adjustable between 7 and 17 ml. Thetotal volume is derived from the volume of the piston in minimum position and the lengthof the tube up to the liquid surface. The total volume can be adjusted until the modulationpressure is in the desired working range. Often the adjustment is not necessary. The mod-ulation depth depends on the starting position of the modulation syringe. The startingposition is not defined in the protocol.
The modulation depth has to exceed the opening and closing pressures of the valve.This will cause the valve to open and close during a modulation cycle. When the pressurebecomes too low (undermodulation) the valve will not open. The pressure range is withina liquid column of 2 meters in height’s which should be sufficient for all valves. The left-over air column is kept high to prevent liquid overflow into the descending arm of the U-turn (overmodulation). A filter (Millex HA) is placed in the U-turn to avoid overmodula-tion. Establishing absolute modulation pressures is of no use, since the transfer functionof the system to the valve inlet is unknown. The modulation depth will therefore be deter-mined by the pressure recorded at the level of the valve inlet (P2).
4.1.1.7 Pressure measurementsEach unit of the test rig is equipped with two pressure gauges. The pressure gauges arecalibrated with the software. Throughout the experiments, two types of pressure gauges(Gould Statham P2310 and the Staham Spectramed P23 XL) have been used.
The range of these gauges is 0-300 x 1.36 cm H2O. The pressure underwent a 12-bitanalogue to digital conversion. The resolution of one digital step is smaller than 0.1 cmH2O. The pressure transducers are connected with 78205 HP pressure modules, placed ina 78901 main frame. The linearity of the pressure gauges is within 1%. The measured noise is within 1 mm Hg(0.14 cm H2O). The time response to step-by-step changes is smaller than 80 ms.
4.1.1.8 Flow resistance devicesThe test rig harbours resistance devices constructed from standard lumbar needles(Spinocan; 26G x 3.5 and 25G x 3.5). The devices are placed in between the pressuregauges (P1 and P2). The resistance device is calibrated using a tube with a low resistanceinstead of the valve. Calibration is performed by recording of the pressure difference P1-P2 in a steady state situation. According to equation 3 (3.1.2.3) the resistance is calculat-ed as the quotient of P1-P2 and the predefined flow velocity. During the tests the calculat-ed resistance is applied in the computation of the instantaneous flow.
50
4.1.1.9 Prevention of air bubblesAir bubbles may greatly affect the mechanical properties of the valve. Once these air bub-bles are formed, they hardly resolve. Every liquid contains solved air. The solvability ofair in water decreases with temperature. It is linearly related with pressure according toHenry’s law. Starting from an air-saturated solution, elevation of temperature and reduc-tion of pressure lead to formation of air bubbles.
A portion of the test solution is outside the waterbath in an environment with a tem-perature of about 15 oC below 37oC. The heating of 1 liter of air-saturated water by 10oCreleases an amount of 0.6 ml air. Since the test fluid is contained in a closed system, noenvironmental air can dissolve into it. The test solutions are prepared at 37 oC. This imp-lies that the outside part of the test fluid at a 15 oC temperature decrement becomes under-saturated since penetration of air is blocked, and reheating it to 37oC, the fluid may, reacha normal level of air-saturation, whereas the probability of formation of air bubblesremains neglectably low. Other measures are extra turns in the fluid-transporting tubes inthe water bath. This increases the transportation time of the fluid. As a consequence, the-re is more time for adaptation of temperature and the chance of adherence to the tube wallby existing air bubbles is increased. Air bubbles will remain at the top of the U-turn befo-re they may interfere with the valve mechanism. In addition, the system is inspected (vis-ually) for the presence of air bubbles before and during testing.
4.1.1.10 Composition of test solutionsThree different test solutions were used: saline, saline containing protein and saline con-taining red blood cells. The protein solutions have concentrations of respectively 0.5; 2.0;5.0 and 10.0 g/l. Twenty percent albumin from human venous plasma (central laboratoryof the Dutch Red Cross, Amsterdam, the Netherlands) was used to prepare the solutions.Caprylate and amandelate were used to stabilize the solution.
The red blood cell counts were respectively 1000; 2000; 5000 and 10.000 cells/µl. Toprepare the solutions, an erythrocyte suspension (obtained from the blood bank service ofthe North Netherlands) was added to citrate phosphate dextrose adenide (CPDA) plasmato get a solution with an erythrocyte count of 10.000 cells/µl. This solution was dilutedwith saline to get the desired test solutions. The solutions contained per 800 erythrocytes,40 thrombocytes and 1 leucocyte.
4.1.1.11 Recording protocolThree valves are tested simultaneously. Before testing, the valves are stored in saline for24 hours. The manufacturer’s specifications of the valves are entered into a computer pro-gram, resistances are calibrated and the modulation unit is adjusted. Every session inclu-des several stages. At every stage the flow and/or the test solution will be changed (table4.1.1). Before changing, the valve is perfused with saline at a flow of 20 ml/h.
51
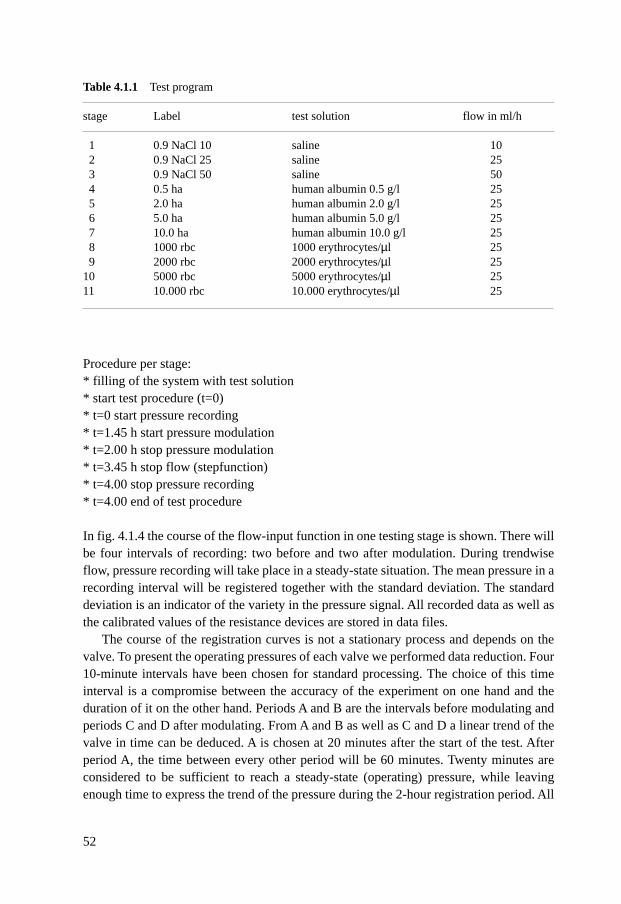
Procedure per stage:* filling of the system with test solution* start test procedure (t=0)* t=0 start pressure recording* t=1.45 h start pressure modulation* t=2.00 h stop pressure modulation* t=3.45 h stop flow (stepfunction)* t=4.00 stop pressure recording* t=4.00 end of test procedure
In fig. 4.1.4 the course of the flow-input function in one testing stage is shown. There willbe four intervals of recording: two before and two after modulation. During trendwiseflow, pressure recording will take place in a steady-state situation. The mean pressure in arecording interval will be registered together with the standard deviation. The standarddeviation is an indicator of the variety in the pressure signal. All recorded data as well asthe calibrated values of the resistance devices are stored in data files.
The course of the registration curves is not a stationary process and depends on thevalve. To present the operating pressures of each valve we performed data reduction. Four10-minute intervals have been chosen for standard processing. The choice of this timeinterval is a compromise between the accuracy of the experiment on one hand and theduration of it on the other hand. Periods A and B are the intervals before modulating andperiods C and D after modulating. From A and B as well as C and D a linear trend of thevalve in time can be deduced. A is chosen at 20 minutes after the start of the test. Afterperiod A, the time between every other period will be 60 minutes. Twenty minutes areconsidered to be sufficient to reach a steady-state (operating) pressure, while leavingenough time to express the trend of the pressure during the 2-hour registration period. All
52
Table 4.1.1 Test program
stage Label test solution flow in ml/h
1 0.9 NaCl 10 saline 102 0.9 NaCl 25 saline 253 0.9 NaCl 50 saline 504 0.5 ha human albumin 0.5 g/l 255 2.0 ha human albumin 2.0 g/l 256 5.0 ha human albumin 5.0 g/l 257 10.0 ha human albumin 10.0 g/l 258 1000 rbc 1000 erythrocytes/µl 259 2000 rbc 2000 erythrocytes/µl 25
10 5000 rbc 5000 erythrocytes/µl 2511 10.000 rbc 10.000 erythrocytes/µl 25
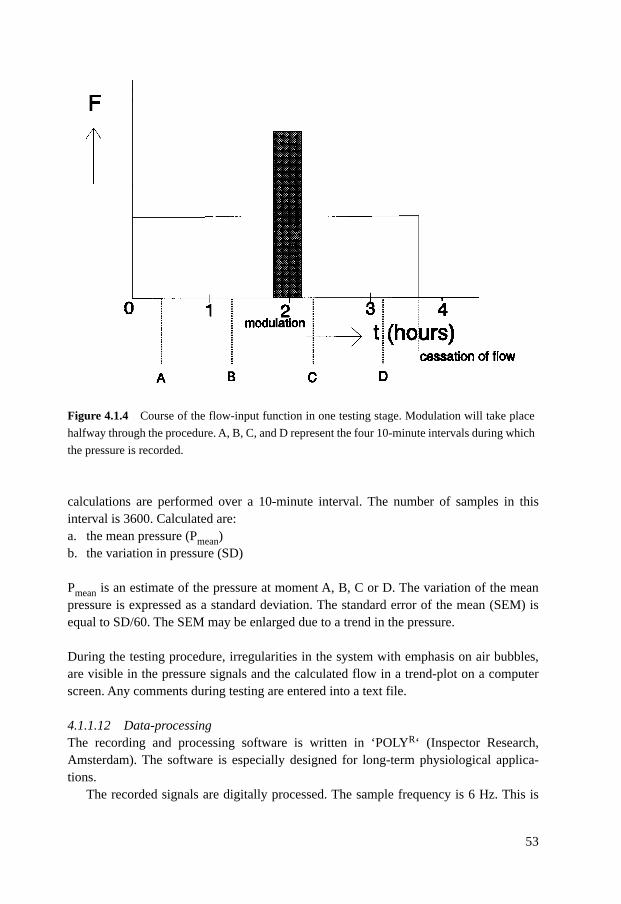
calculations are performed over a 10-minute interval. The number of samples in thisinterval is 3600. Calculated are:a. the mean pressure (Pmean)b. the variation in pressure (SD)
Pmean is an estimate of the pressure at moment A, B, C or D. The variation of the meanpressure is expressed as a standard deviation. The standard error of the mean (SEM) isequal to SD/60. The SEM may be enlarged due to a trend in the pressure.
During the testing procedure, irregularities in the system with emphasis on air bubbles,are visible in the pressure signals and the calculated flow in a trend-plot on a computerscreen. Any comments during testing are entered into a text file.
4.1.1.12 Data-processingThe recording and processing software is written in ‘POLYR‘ (Inspector Research,Amsterdam). The software is especially designed for long-term physiological applica-tions.
The recorded signals are digitally processed. The sample frequency is 6 Hz. This is
53
Figure 4.1.4 Course of the flow-input function in one testing stage. Modulation will take place
halfway through the procedure. A, B, C, and D represent the four 10-minute intervals during which
the pressure is recorded.
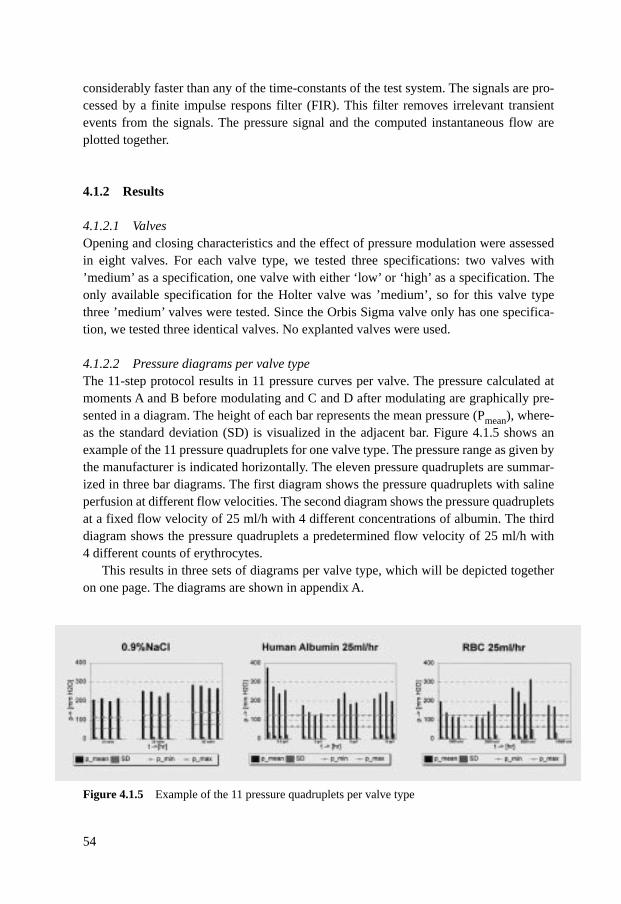
considerably faster than any of the time-constants of the test system. The signals are pro-cessed by a finite impulse respons filter (FIR). This filter removes irrelevant transientevents from the signals. The pressure signal and the computed instantaneous flow areplotted together.
4.1.2 Results
4.1.2.1 ValvesOpening and closing characteristics and the effect of pressure modulation were assessedin eight valves. For each valve type, we tested three specifications: two valves with’medium’ as a specification, one valve with either ‘low’ or ‘high’ as a specification. Theonly available specification for the Holter valve was ’medium’, so for this valve typethree ’medium’ valves were tested. Since the Orbis Sigma valve only has one specifica-tion, we tested three identical valves. No explanted valves were used.
4.1.2.2 Pressure diagrams per valve typeThe 11-step protocol results in 11 pressure curves per valve. The pressure calculated atmoments A and B before modulating and C and D after modulating are graphically pre-sented in a diagram. The height of each bar represents the mean pressure (Pmean), where-as the standard deviation (SD) is visualized in the adjacent bar. Figure 4.1.5 shows anexample of the 11 pressure quadruplets for one valve type. The pressure range as given bythe manufacturer is indicated horizontally. The eleven pressure quadruplets are summar-ized in three bar diagrams. The first diagram shows the pressure quadruplets with salineperfusion at different flow velocities. The second diagram shows the pressure quadrupletsat a fixed flow velocity of 25 ml/h with 4 different concentrations of albumin. The thirddiagram shows the pressure quadruplets a predetermined flow velocity of 25 ml/h with4 different counts of erythrocytes.
This results in three sets of diagrams per valve type, which will be depicted togetheron one page. The diagrams are shown in appendix A.
54
Figure 4.1.5 Example of the 11 pressure quadruplets per valve type
4.1.2.3 Results per valve
Pudenz flushing valve (appendix A, page 75)Two out of the three Pudenz flushing valves had operating pressures (=pressure at equi-librium after valve opening) at a 25 ml/h saline perfusion that were considerably higherthan the maximum pressure stated by the manufacturer. Protein perfusion did not changethe operating pressure for any of the valves. However, two out of the three valves mal-functioned at erythrocyte counts of 10.000 cells/µl, probably because of partial or totalvalve obstruction. The remaining valve showed a very high pressure after modulation:373 mm H2O.
It must be remarked that the testing of valve 35 at an erythrocyte count of 10.000 cel-ls/µl only lasted 2 hours because of total valve obstruction. With the 0.5 g/l albumin perfu-sion through valve 36, the pump stopped after modulation because of technical problems.
Phoenix valve (appendix A, page 76)For the Phoenix valve no. V39 (medium pressure) the manufacturer only provided onevalue (opening pressure) and no pressure range at different flow rates.
Two out of three Phoenix valves had operating pressures with saline perfusion at 25ml/h that were much higher than the pressure stated by the manufacturer. Adding proteinto the test solution showed similar results, although an effect of modulation (pressureincrease) at a higher concentration was seen. An erythrocyte count of 2000 cells/µl andhigher increased the operating pressure furthermore. For all three valves, the pressure atpoint D with a perfusion of 10.000 cells/µl is extremely high (resp. 4087, 585 and 842mm H2O). For the low pressure Phoenix valve, the pressure is already extremely high at2000 cells/µl.
Raimondi valve (appendix A, page 77) At 25 ml/h saline perfusion, the operating pressure of all three valves was within the pres-sure specifications of the manufacturer. The operating pressure increased slightly in twovalves after protein perfusion with at least 2 g/l protein. The remaining valve showed aconsiderable increase in pressure at this protein concentration. Erythrocyte perfusion with10.000 cells/µl increased the operating pressure of all valves. One valve already showedan increased operating pressure at 5000 cells/µl.
It must be remarked that for valve 43 the pressure at B is not valid due to temporarypump failure.
Orbis Sigma valve (appendix A, page 78)The manufacturer intentionally constructed a valve with an S-shaped pressure-flow cur-ve. The pressure values are read from this curve at flow rates of 10, 25 and 50 ml. Thehigh pressure values at 25 and 50 ml/h are obtained from the rising part of the curve. Thepressure values obtained are 65 mm H2O at a flow rate of 10 ml/h, 365 mm H2O at 25ml/h and 435 mm H2O at 50 ml/h.
55
Summarizing the results of the three valves, we can state that at flow rates of 25 and 50ml/h with saline perfusion, the Orbis Sigma valve functions at an operating pressurewhich approaches the one given by the manufacturer. Perfusion with protein solutionsdoes not change this. At a flow rate of 10 ml/h, and at a flow rate of 50 ml/h (less clear),the operating pressure at saline perfusion considerably exceeds the pressure specificationof the manufacturer. An erythrocyte count of 10.000 cells/µl causes malfunctioning intwo out of three Orbis Sigma valves, probably because of obstruction. The third valveshows a considerably increased operating pressure at all erythrocyte counts.
Holter valve (appendix A, page 79)The manufacturer of the Holter valve only provided a pressure range at a flow of 8.6 ml/hwhich covers pressures of 41-75 mm H2O. We applied this range for all tests as the manu-facturer’s range.
At a 25 ml/h saline perfusion, all three valves show an operating pressure far exceed-ing the maximum pressure as given by the manufacturer. This is also true for perfusionrates of 10 ml and 50 ml/h. Adding protein does not alter this picture, although in one ofthe valves the operating pressure at higher protein solutions decreases to the range as giv-en by the manufacturer. With erythrocyte perfusion, one valve broke down (V20) for unk-nown reasons. The second valve showed no change in operating pressures, whereas thelast valve showed an increased pressure.
Accu-flo valve (appendix A, page 80)A 25 ml/h saline perfusion, two out of three valves had operating pressures within the ran-ge given by the manufacturer. The remaining valve had an increased operating pressure.Protein perfusion had a different effect on each valve. One valve showed a small increasein operating pressure, the second showed no change at all, and the third showed an incre-ased operating pressure at the two lowest protein concentrations which decreased again tonormal at higher concentrations. Erythrocyte perfusion also had varying effects on thethree valves. One valve showed no change, another showed an increased operating pres-sure at all erythrocyte counts with a peak at 2000 and 5000 cells/µl, another broke downwhen the erythrocyte count of 10.000 cells/µl was reached.
PS medical valve (appendix A, page 81)At a saline perfusion of 25 ml/h all three valves were within or approached the range asprovided by the manufacturer. Protein perfusion had no effect at all on two out of threevalves. In the remaining valve a 2 g/l albumin solution caused an increase in operatingpressure at point D. At erythrocyte counts of 5000 cells/µl or more, all valves showedconsiderably elevated operating pressures. One of the valves already started to have anincreased operating pressure at 2000 cells/µl.Additional remarks: the test procedure at 5 g/l albumin with valve 6 and 4 was arrestedtoo early. This resulted in three pressure values instead of four. For valve 41 the test pro-cedure at an erythrocyte count of 1000/µl was also arrested too early. Again, this resultedin three pressure values instead of four.
56
Hakim valve (appendix A, page 82)At a saline perfusion rate of 25 ml/h, two out of three valves had operating pressureswithin the range, whereas the pressure values of one valve were somewhat below the ran-ge. Testing with protein solutions reduced the operating pressure in one valve, whereas inthe other two valves the operating pressure increased (in one of the valves there is a con-siderable increase at 5 g/l). During perfusion with erythrocyte solutions one valve showeda small increase in operating pressure, the other two a decrease starting at 5000 cells/µl. The data for the 10 ml/h saline perfusion through valve 27 at A were incorrectly recorded.The obtained values were not representative. The test procedure for valve 28 during the10 g/l albumin perfusion was arrested too early. This explains the low value at D.
4.1.2.4 Dynamical propertiesThe functional quality of a valve is primarily determined by its opening and closing char-acteristics. These characteristics reflect a dynamic action and therefore can be deducedfrom the time-response functions of the pressure. In the tests, the behavior of opening andclosing is encountered at the start of the step-function of the flow, around the modulationtests and after flow cessation. The dynamical characteristics can be distinguished in a fewtypes and are presented in figures. These figures will be shown in tables. The tables arearanged like the graphic plots of the pressure values. The results from three valves of onetype are summarized in three tables on one page. Each table is subdivided in three groups,referring to the experiments with saline, albumin solutions and blood cell suspensions. Afurther description is given below. 1. At the start of one test (t=0), the flow will increase step-by-step to the desired value.
As the test system has its own volume and compliance between the pump and the val-ve, the pressure at the valve inlet will gradually increase. This shows the openingcharacteristics of the valve in a pressure curve (fig 4.1.6). Three types are distin-guished: normal opening, overshoot or undershoot. dP is the difference between theinitial maximum and the steady-state pressure (Pe) In case of overshoot the relationdP/Pe will be higher than zero, whereas in case of a normally opening valve this quo-tient will be equal to zero. In case of undershoot, the pressure will gradually increaseto the eventual steady-state pressure (Pe), which is the same as the operating pressure.The undershoot is expressed in the time to reach the operating pressure.
2. At the end of the recording procedure the flow is reduced step-by-step to 0 ml.Pressure recording will continue for another 15 minutes (fig 4.1.6). The quotient ofthe pressure at the end of registration and the pressure immediately before decreasingflow will be calculated and expressed in a percentage (Pr/Pc in %). Zero percent cor-responds to a remaining pressure of 0. A good drainage system shows a remainingpressure (the pressure at the end of registration) after flow cessation that is below theoperating pressure. Thus, the remaining pressure does not necessarily have to be zero.The main concern is the flow restriction through the valve resistance. In some record-ings (usually red blood cell suspensions) the remaining pressure was not availablebecause of valve complications (obstruction).
57
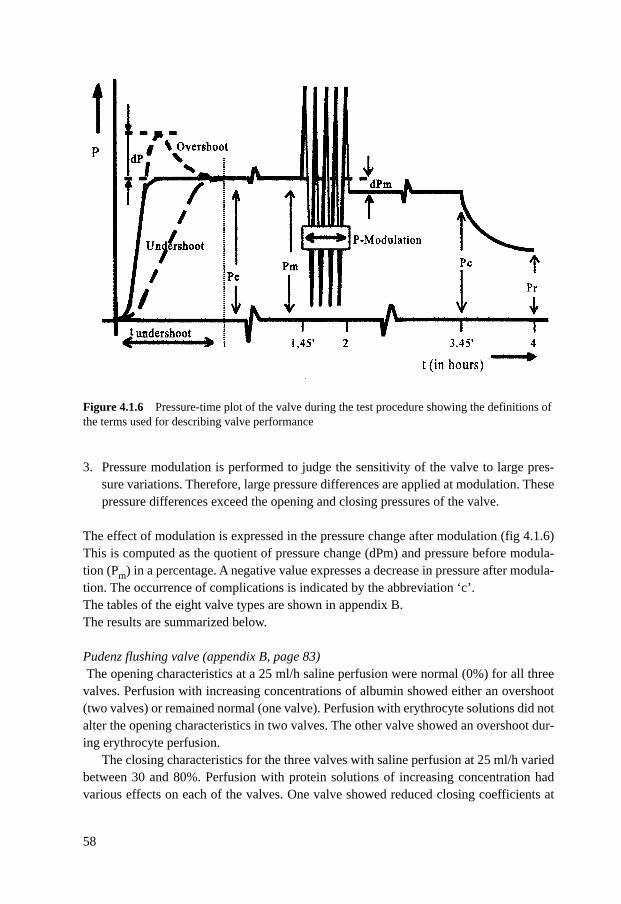
3. Pressure modulation is performed to judge the sensitivity of the valve to large pres-sure variations. Therefore, large pressure differences are applied at modulation. Thesepressure differences exceed the opening and closing pressures of the valve.
The effect of modulation is expressed in the pressure change after modulation (fig 4.1.6)This is computed as the quotient of pressure change (dPm) and pressure before modula-tion (Pm) in a percentage. A negative value expresses a decrease in pressure after modula-tion. The occurrence of complications is indicated by the abbreviation ‘c’.The tables of the eight valve types are shown in appendix B. The results are summarized below.
Pudenz flushing valve (appendix B, page 83)The opening characteristics at a 25 ml/h saline perfusion were normal (0%) for all three
valves. Perfusion with increasing concentrations of albumin showed either an overshoot(two valves) or remained normal (one valve). Perfusion with erythrocyte solutions did notalter the opening characteristics in two valves. The other valve showed an overshoot dur-ing erythrocyte perfusion.
The closing characteristics for the three valves with saline perfusion at 25 ml/h variedbetween 30 and 80%. Perfusion with protein solutions of increasing concentration hadvarious effects on each of the valves. One valve showed reduced closing coefficients at
58
Figure 4.1.6 Pressure-time plot of the valve during the test procedure showing the definitions ofthe terms used for describing valve performance
the lower albumin concentrations, whereas at the highest albumin concentrations thepressure decreased to zero. A second valve showed no changes in closing coefficients. Inthe last valve the closing coefficients remained around 80%. At erythrocyte perfusion,measurements with erythrocyte counts above 2000 cells/µl failed in two valves, probablydue to valve obstruction. The remaining valve showed no changes in closing characteris-tics.
The effect of modulation during saline perfusion at 25 ml/h varied between 0 and -27%.Protein perfusion did not really alter the operating pressure after modulation. It must beremarked that the test for valve 36 with a protein concentration of 0.5 g/l failed becausethe pump stopped during the test procedure. Erythrocyte perfusion didn’t show any sig-nificant effect of modulation on the operating pressure either. In two valves the test failedat a count of 10.000 cells/µl.
Phoenix valve (appendix B, page 84)The opening characteristics of two of the valves at a 25 ml/h saline perfusion were normal(0%). The remaining valve showed an undershoot of 13 minutes. Protein perfusion didnot have any effect on the opening characteristics in one valve. The other two valvesshowed an overshoot at 2, 5 and/or 10 g albumin/l. Erythrocyte perfusion did not have asignificant effect on the opening characteristics.
The closing characteristics at saline perfusion varied from 0 to 30 %. It was not pos-sible to determine the closing characteristics in all three valves at erythrocyte counts of2000 cells/µl or more.
The effect of modulation with a 25 ml/h saline perfusion varied between -33 and -150%.Protein concentration caused an overall slight increase in pressure after modulation com-pared to saline perfusion. The effect of erythrocyte perfusion varied considerably fromvalve to valve and within each valve, but it can be stated that erythrocyte perfusion, espe-cially with high cell counts, caused an increase in pressure after modulation compared toperfusion with saline.
Raimondi valve (appendix B, page 85)At a 25 ml/h saline perfusion, the opening characteristics varied from 66 to 138 %.Protein perfusion caused considerable variation in opening characteristics between thevalves and in the same valve. In valve 43 there was temporary malfunctioning of thepump at an albumin concentration of 10 g/l. This measurement was not valid.
All valves closed properly at a 25 ml/h saline perfusion. With protein perfusion therewas a small increase in closing coefficients at higher protein concentrations. With erythro-cyte counts of more than 2000 cells/µl, the measurements could not be performed in twoout of three valves. The remaining valve failed at 5000 cells/µl.
There was no effect of modulation with saline perfusion. Protein perfusion causedeither a decrease or no difference in pressure after modulation. Erythrocyte perfusionsgenerally caused no differences in pressure after modulation compared to saline perfu-sion.
59
Orbis Sigma valve (appendix B, page 86)The opening characteristics with saline perfusion were normal (0%) for all three valves.Protein perfusion did not cause any change in opening characteristics in two valves,whereas the remaining valve showed an overshoot of about 30% with all protein concen-trations. Erythrocyte perfusion had little effect on the opening characteristics.
The closing characteristics varied between 60 and 90% with saline perfusion at25 ml/h. Protein pefusion lowered the closing coefficients in two valves, whereas in theremaining valve no changes occurred. The effects of erythrocyte perfusion on closingcharacteristics could not be determined, possibly because of valve obstruction.
The effect of modulation during saline perfusion at 25 ml/h varied from 0 to -4 %.Protein concentration did not change this effect considerably. In two of the valves, theeffect of erythrocyte perfusion could not be determined at cell counts of more than 2000cells/µl, possibly because of obstruction. In the other valve there was no obvious effect ofcells on pressure after modulation.
Holter valve (appendix B, page 87)Saline perfusion at 25 ml/h showed normal opening characteristics of 0% in all three val-ves. Protein perfusion did not alter these characteristics. Erythrocyte perfusion did nothave a considerable effect at concentrations up to 5000 cells/µl. At 10.000 cells/µl therewere complications in one valve.
The closing characteristics with saline perfusion at 25 ml/h varied from 40 to 60 %. Invalve 21 there were technical problems during testing with a 25ml/h saline perfusion,therefore no results were available. Protein perfusion caused a slight decrease in closingcoefficients in all valves. Erythrocyte perfusion caused complications in one valve at cellcounts of 1000/µl and more. The other two valves showed no changes.
The effect of modulation varied between 0 and -16% with saline perfusion at 25 ml/h.Protein perfusion did not have a significant effect. Erythrocyte perfusion did not reallyaffect the pressure after modulation either.
Accu-flo valve (appendix B, page 88)The opening characteristics at a 25 ml/h saline perfusion varied between 0 and 14%.Protein perfusion did not change these characteristics in two valves. The remaining valveshowed an increase at 2 and 10 g albumin/l. Erythrocyte perfusion did not have any effectin two valves. The remaining valve showed complications at a perfusion with 10.000 cells/µl.
The closing characteristics at saline perfusion at 25 ml/h varied from 25 to 60%.Overall, protein perfusion caused a slight decrease in closing coefficients. Erythrocyteperfusion had varying effects: one valve totally failed and did not develop any pressure,the second showed an increase in closing coefficients, and the third showed a decrease.
The effect of modulation with saline perfusion varied between 0 and -25 %. Proteinperfusion had no effect on pressure after modulation. In two valves, erythrocytes did notaffect pressure after modulation. The remaining valve, as mentioned above, hardly devel-oped any pressure.
60
PS medical valve (appendix B, page 89)The opening characteristics of this valve varied from normal (0%) to a maximum over-shoot of 50 % at a 25 ml/hour saline perfusion. Protein perfusion caused an increase inopening characteristics in all valves. It must be mentioned that in valves 4 and 6 the testsat an albumin concentration of 5 g/l were arrested too early. Erythrocyte perfusion did notreally change the opening characteristics.
The closing characteristics with saline perfusion at 25 ml/h were respectively 0, 40and 90 %. Protein perfusion, overall, slightly decreased the closing coefficients. Witherythrocyte perfusion at counts of more than 2000 cells/µl, the closing characteristicscould not be determined due to complications (obstruction).
There was no effect of modulation in all three valves with saline perfusion. Proteinperfusion did not really affect this. Erythrocyte perfusion hardly had any effect. Onlyonce the effect of modulation was 266 % at a count of 10.000 cells/µl.
Hakim valve (appendix B, page 90)The opening characteristics at saline perfusion varied from normal (0%) to a maximumovershoot of 50%. Protein perfusion did not have a considerable effect. Erythrocyte perfu-sion did not really have any effect on the opening characteristics either. Only once theopening characteristics could not be determined at an erythrocyte count of 10.000 cells/µl.
The closing characteristics with saline perfusion at 25 ml/h were resp. 0, 10 and 60%.In general, protein perfusion did not change these characteristics significantly. Erythro-cyte perfusion caused an increase in closing pressure at all cell counts.
The effect of modulation with saline perfusion at 25 ml/h varied between 0 and 50%.Protein perfusion had varying effects on pressure after modulation, but these effects weresmall. No effect of modulation could be determined during erythrocyte perfusion in twovalves. It must be mentioned, however, that in one of these valves the effects were notmeasurable at 2000 and 5000 cells/µl. In the third valve the effect of modulation variedwith each cell count.
Summary of dynamical characteristicsFrom a general point of view it can be stated that the protein as well as the erythrocyte testfluids had varying effects on the opening characteristics. Only rarely did high erythrocytecounts cause alterations in opening coefficients. Most frequently, alterations were foundwith the Pudenz flushing valve. Another, singular, alteration in opening characteristicswas seen with the Orbis Sigma and Accu-flo valve .Closing characteristics showed a different picture. Again, protein solutions had unpredict-able effects on pressure characteristics, but plain alterations were never found. However,(partial) obstruction after erythrocyte perfusion occurred in two or three valves of the fol-lowing types: Pudenz flushing, Phoenix, Raimondi, Orbis Sigma, and PS medical. In theHolter and Accu-flo valves, (partial) obstruction only occurred in one valve. Problems during perfusion with erythrocyte solutions after modulation occurred once forthe Pudenz flushing valve, the Orbis Sigma valve, and the Accuflo valve.
61
4.2 Discussion
The eight most frequently inserted hydrocephalus shunt valves in eight Dutch neurosurgi-cal centres were tested in a laboratory setting. Aims of the study were firstly to test if the-se valves performed according to the manufacturer’s specifications and secondly if thevalve’s hydrodynamic characteristics changed after adding protein or erythrocytes to thetest solution. The protein and erythrocyte test solutions were used to mimic the changes incerebrospinal fluid composition in some clinical circumstances.
As the cerebrospinal fluid production in hydrocephalus patients is more or less contin-uous, a pump-driven test rig was chosen. The rig was equipped with test facilities for stat-ic conditions as well as dynamic pressure variations in order to cover a wide spectrum ofphysiological conditions in man. A standardized test protocol was embedded in the soft-ware of the computer-controlled test rig. Temperature of the test solution was maintainedat 37oC. The study aimed to test the short-term performance of the valves during 4-hourtest periods.
4.2.1 Summary of the test resultsBefore starting the discussion, an overview of the test results per valve type will be given.The test results per valve are summarized in table 4.2.1. In this summary the valve’s per-formance is given in a 3-scale division in the categories ‘good (g)’, ’moderate (m)’ and‘bad (b)’.
The results with saline perfusion are used to compare the performance of the valvewith the manufacturer‘s specification, whereas the results of the performance of the valvewith protein as well as red blood cells are to be related to those with saline. For saline perfusion the score “good” indicates that generally the operating pressures didnot exceed a deviation of 100% of the values specified by the manufacturer, whereas thescore ”moderate” indicates deviations up to 200%. The score “bad” indicates operatingpressure deviations of more than 200% from the manufacturer’s specifications. For pro-tein and erythrocyte perfusion the score “good” indicates generally no clear and consis-tent change in operating pressure compared to the results obtained during saline perfusion(deviations of up to 100%), whereas the score ”moderate” is used when generally moreobvious deviations occurred (up to 200%). The score “bad” indicates generally deviationsof more than 200% compared to saline perfusion or signs of total or partial obstruction.
The dynamic behavior of the valve is expressed during opening and closing. The qual-ities of the valves are scored in terms of over- and undershoot (opening characteristics)and the course of the pressure after cessation of flow (closing characteristics). Overshootexpresses the ’sticky’ behavior of the valve causing opening difficulties whereas under-shoot represents problems like a leaking valve. When the valves generally had normalopening characteristics we scored them “good”, whereas ”moderate” indicates regulardeviations. The score “bad” is used when normal opening almost never occurred. Thescore “good” for effect of modulation means generally no obvious changes in operatingpressure after modulation, whereas the score ”moderate” is used when regular changes in
62
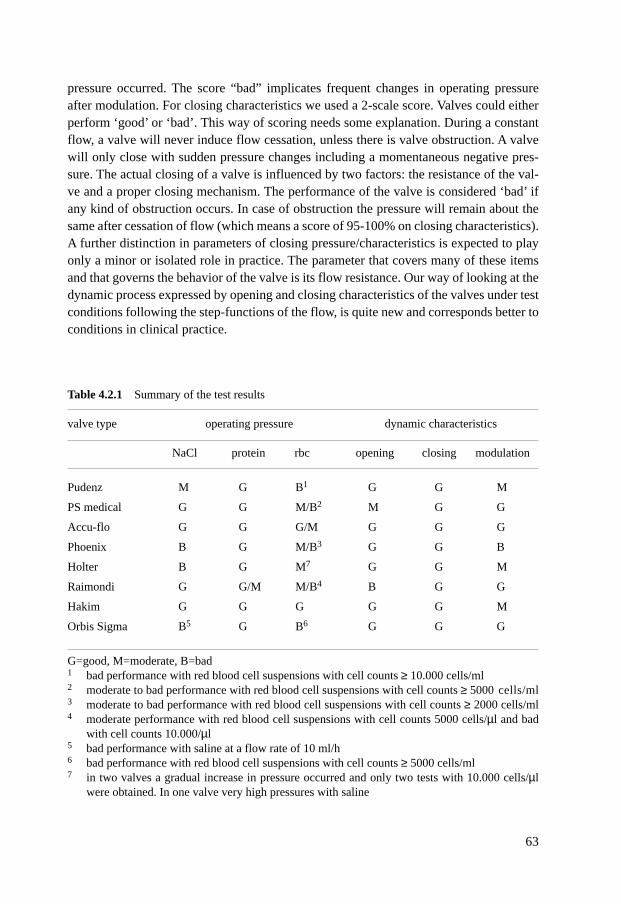
pressure occurred. The score “bad” implicates frequent changes in operating pressureafter modulation. For closing characteristics we used a 2-scale score. Valves could eitherperform ‘good’ or ‘bad’. This way of scoring needs some explanation. During a constantflow, a valve will never induce flow cessation, unless there is valve obstruction. A valvewill only close with sudden pressure changes including a momentaneous negative pres-sure. The actual closing of a valve is influenced by two factors: the resistance of the val-ve and a proper closing mechanism. The performance of the valve is considered ‘bad’ ifany kind of obstruction occurs. In case of obstruction the pressure will remain about thesame after cessation of flow (which means a score of 95-100% on closing characteristics).A further distinction in parameters of closing pressure/characteristics is expected to playonly a minor or isolated role in practice. The parameter that covers many of these itemsand that governs the behavior of the valve is its flow resistance. Our way of looking at thedynamic process expressed by opening and closing characteristics of the valves under testconditions following the step-functions of the flow, is quite new and corresponds better toconditions in clinical practice.
63
Table 4.2.1 Summary of the test results
valve type operating pressure dynamic characteristics
NaCl protein rbc opening closing modulation
Pudenz M G B1 G G M
PS medical G G M/B2 M G G
Accu-flo G G G/M G G G
Phoenix B G M/B3 G G B
Holter B G M7 G G M
Raimondi G G/M M/B4 B G G
Hakim G G G G G M
Orbis Sigma B5 G B6 G G G
G=good, M=moderate, B=bad 1 bad performance with red blood cell suspensions with cell counts ≥ 10.000 cells/ml2 moderate to bad performance with red blood cell suspensions with cell counts ≥ 5000 cells/ml3 moderate to bad performance with red blood cell suspensions with cell counts ≥ 2000 cells/ml4 moderate performance with red blood cell suspensions with cell counts 5000 cells/µl and bad
with cell counts 10.000/µl5 bad performance with saline at a flow rate of 10 ml/h6 bad performance with red blood cell suspensions with cell counts ≥ 5000 cells/ml7 in two valves a gradual increase in pressure occurred and only two tests with 10.000 cells/µl
were obtained. In one valve very high pressures with saline
4.2.2 Performance (saline) compared to the manufacturer‘s specificationsAs far as operating pressures in saline are concerned, about half of the valves performedin reasonable agreement with the manufacturer‘s specifications. Only the Orbis Sigmavalve, the Phoenix valve and the Holter valve did not perform satisfactorily.All three val-ves showed operating pressures that were much higher than the specified pressures asgiven by the manufacturer.
Aschof conducted several studies9,10,11,13,14,15 in which he tested the pressure-flowcharacteristics of hydrocephalus valves. The percentage of new valves in these studiesthat met the official specifications varied from 23 to 38%. One fifth of the valves deviat-ed 100 to 1460% from the manufacturer’s specifications. From these studies it was appar-ent that the Hakim valves performed best in their laboratory situation. Holter, Heyer-Schulte, Phoenix and Orbis Sigma valves did not meet the specifications as given by themanufacturer. In a study115 done by Schulte, the Orbis Sigma valves were perfused for 1year with ultra- filtered water, during which several pressure-flow tests were done. Theresults varied widely from valve to valve, so no consistent performance was observed.Leonhardt et al.77 used a computer-aided test rig for CSF shunts. They tested Codman-Medos, Hakim and Heyer Schulte valves. None of these valves performed according tothe manufacturer’s specification. Trost123,124 tested 13 new and 19 explanted valves in aflow-driven test rig and reported that only diaphragm valves and some ball and springvalves performed in the pressure range as given by the manufacturer. The performance ofslit valves varied widely from good to dramatic. Trost did not study the Orbis Sigma val-ve.
Whereas Aschoff tested the valves in a pump-driven as well as a pressure-driven testrig, we tested them in a pump-driven rig, like Trost did. Our laboratory results confirmTrost’s findings on the performance of valves compared to the specifications as given bythe manufacturer. Strikingly, two of the valves that performed badly in our study were slitvalves. Aschoff repeatedly mentioned the tendency of slit valves to deviate from themanufacturer’s specification10,13,15. Although he tested them in pressure-driven rigs, it isprobably legitimate to compare his results with ours. Our pump-driven test rig enabled usto measure the operating pressure of the valve during a steady-state situation, whereasAschoff measured the pressure to maintain the flow through an open valve. We both com-pared the obtained pressures with the pressure range as given by the manufacturer.
An explanation for the impaired performance of slit valves can be that shunt systemsin which a slit valve is incorporated do not contain plain flow-restraining elements, whichmight cause overdrainage. In addition, the mechanism of this valve is based on the mem-ory property of silicone: the material will resume its original shape, which may take a var-iable time in the range of seconds to days. For the Orbis Sigma valve, our findings are again confirmed by Aschoff10,13,15 andSchulte115. The extremely delicate mechanism of the Orbis Sigma valve is sensitive toincreased proximal pressure. The membrane could be easily damaged, and the ring or cyl-inder might dislocate. The small outlet of the valve is prone to obstruction. Schulte con-cluded that the very sophisticated micro-mechanical construction of the Orbis Sigma val-
64
ve leads to an only average accuracy. The construction is so delicate, that even minorinfluences might cause valve dysfunction.
4.2.3 Effect of protein on valve performanceAs mentioned in 3.5, in the early years of shunt testing protein was reported to impair
valve functioning64,105,114,119 by increasing the viscosity of the test solution and therebydecreasing flow. This was contradicted by the results of Van Veen126 and Brydon et al.24 ,who proved that the increase in viscosity was mainly caused by a decrease in temperaturewhereas the increase in viscosity of the high protein solutions was negligible. Tests in theearly years were performed at room temperature instead of body temperature. Also, thetheoretical possibility of valve sticking was rejected by Brydon et al. Aschoff10 tested theprotein sensitivity of shunt valves and concluded that the performance of most valves washardly influenced by protein concentrations of up to 5 g/l. This was confirmed by Pudenzet al.102 when they tested solutions of 4 g protein/l.
Our results support the current views from the literature: protein concentrations up to10 g/l did not impair valve functioning.
4.2.4 Effect of red blood cells on valve functioningTo evaluate the valve’s performance during erythrocyte perfusion, we compared the oper-ating pressures recorded at erythrocyte perfusion with those recorded at saline perfusion.In general, most of the valves (6 out of 8) tested in our study performed badly or moder-ately at erythrocyte counts of more than 5000 cells/µl. The calculated standard deviationof the operating pressure increased at higher pressures, which indicates an increase inpressure fluctuation. Only the Hakim valve performed well up to the maximum erythro-cyte count of 10.000 cells/µl. The Orbis Sigma valve performed worst. This valve alreadyshowed partial obstruction at the lowest erythrocyte counts.
It was stated in 1984 by Walters et al.129 and in 1993 by Sainte-Rose110 that higherythrocyte counts increased the risk of shunt malfunctioning considerably. As early as in1973 it was reported67
that this effect could not be explained by changes in viscosity. Brydon26 tested shunt sys-tems in vitro with test solutions containing varying erythrocyte counts. He concluded thatHakim and PS valves performed well during perfusion with test solutions containing upto 10.000 erythrocytes/µl. At higher erythrocyte counts, opening as well as closing pres-sure increased, as did valve closing time. Brydon suggested erythrocyte sedimentationand platelet adhesion to be responsible for these effects. Brydon conducted the only invitro study on the effect of erythrocytes on valve functioning. In addition, Aschoff in sev-eral studies mentions the susceptibility of the Orbis Sigma valve to obstruction by debris,blood clots, etc.11,12.
Our study is the second in vitro study on the effects of red blood cells on valve func-tioning. The main differences compared to Brydon’s study26 are that we were able to testmore valve types and that we tested new valves instead of explanted valves that mightalready have debris deposits on them. Brydon only tested six new PS medical valves
65
(three low- and three medium-pressure valves) and six explanted Hakim valves (threelow- and three medium pressure valves). Furthermore, Brydon used a roller pump insteadof the syringe pump we used. This roller pump might cause mechanical damage in erythro-cytes which may cause artefacts. In concordance with Brydon, we found that the Hakimvalve functions well with test solutions containing up to 10.000 erythrocytes/µl. In con-trast to Brydon’s study, the PS valve performed badly at erythrocyte counts above5000/µl. In addition, our study proves the high susceptibility of the Orbis Sigma valvecompared to other valves to red blood cells (obstruction), which was already suggested byothers11,12,110,129. The high susceptibility may be explained by the above mentioned smalloutlet of the valve.
4.2.5 Opening characteristicsMost valves show no deviations in opening characeristics. Only the Raimondi valve andoccasionally the PS valve showed an overshoot.
Not much data exist in the literature concerning opening characteristics of valves in apump-driven test rig. Most studies were performed in a pressure-driven rig, which ena-bles straight-forward recording of opening and closing pressures. Aschoff 9,10,11,12,13 test-ed with pump-driven as well as pressure-driven rigs. In his pump-driven rigs, flow rateswere varied from 1 to 200 ml/h in ascending and descending steps. In addition to this con-stant flow, Aschoff performed subtests with a 5 mm Hg pulsatile superimposition(80/min) on this constant flow. This pulsatile superimposition considerably increased theflow rate in all the valves around the opening and closing points. It had no effect when thevalves were completely opened or closed. It must be remarked, however, that these testsare based on variations in pressure, which might presumably alter opening- and closingcharacteristics. The Hakim valve was most sensitive to pressure superimpositions, where-as the Heyer Schulte was less sensitive and the Orbis Sigma least. Aschoff did not test theRaimondi valve in a pump-driven setting.
It is hard to compare our results with Aschoff’s results. In addition, there is again thedifference between testing in a pressure-driven test rig and testing in a pump-driven rig.The Raimondi valve (distal slit valve) had the worst opening characteristics. The over-shoot we reported can be explained by the ’sticky’ behavior of the valve. The PS valve(diaphragm valve) showed moderate opening characteristics. Whereas the dynamics ofthis valve depend on elasticity, tension and thickness of the membrane as well as on theshape and size of the orifice of the valve, there is only one explanation for the overshootseen in the PS valve. However, a well-known problem with diaphragm valves is theirnon-linear increase in resistance of the membrane with enlargement of its surface whichmay lead to overdrainage. It is possible that in the PS valve this problem is more apparentthan in other diaphragm valves ( Pudenz, Accu-flo).
4.2.6 Closing characteristicsFrom table 4.1 it is concluded that none of the valves had a plain ‘bad’ score on closingcharacteristics. However, there were large differences in values and course of the remain-
66

ing pressure after flow cessation which can be explained by the difference in valve resis-tance. The remaining pressure is proportionally related to valve resistance which is clear-ly shown by the results of the Orbis Sigma valve. This valve has the smallest outlet of allvalves. In contrast, The Phoenix and the Raimondi valves have a low resistance, causing‘leaking’ which will lead to a remaining pressure of zero relatively fast. When obstructionoccured during erythrocyte perfusion recording of the closing characteristics was not pos-sible.
As mentioned above, most of the previously mentioned studies were performed usinga pressure-driven test rig, which enables recording of opening and closing pressures.Only Aschoff 9,10,11,13 also used a pump-driven rig with a pulsatile flow. Nevertheless, hefound a considerable increase in closing pressure in all valves when pulsatile pressurewas applied in addition to a constant flow rate. In a bench test of 372 valves, in a pres-sure-driven test rig, Aschoff et al9,13,14,15 found that only 30% of the conventional valves(Hakim, Orbis Sigma, Heyer Schulte, Phoenix high and medium pressure, Holter) hadeither high closing pressures or a flat pressure-flow graph which may lead to minimallysubnormal or even physiological intracranial pressure in an erect position. All the othervalves, especially the distal slit valves (low and medium range), diaphragm valves (lowpressure) and ball in cone valves (low) had low closing pressures and/or steep pressureflow graphs, harbouring the risk of overdrainage. However, the Orbis Sigma as well asthe proximal slit valves with the same flat pressure flow graphs were mentioned to showa wide variability in closing pressures and flow characteristics. Schulte51 reported thesame wide variability in properties of the Orbis Sigma valve.
There is another difference between the pump-driven test rig in our study and thepressure-driven rig in Aschoff’s study9,13,14,15. Aschoff only recorded a closing pressure,whereas we examined the step response after flow cessation from which the quotient ofremaining pressure and operating pressure is calculated. This difference might play a rolein the partially conflicting results. Aschoff reported the Raimondi valve to be prone tooverdrainage, whereas we could report good closing characteristics. Also, the Phoenixvalve performed well in our study, whereas Aschoff reported this valve and other proxi-mal slit valves to show inconsistent closing pressures. On the other hand, our results con-firm Aschoff’s remark about the Orbis Sigma valve. The closing characteristics of thisvalve show a wide variability in both studies. Again, the extremely sophisticated micro-mechanism of construction of the Orbis Sigma valve might be responsible for this. Evenminor external influences might disturb the closing of this valve.
4.2.7 Effect of modulationAbout half the valves are not affected by considerable pressure changes. Only the perfor-mance of the Phoenix valve was considerably affected by modulation.
Compared to data from the literature, we applied considerably higher amplitudes dur-ing modulation. Aschoff et al.9,10,12,13,14 placed their valves in a pressure chamber andapplied external pressure on the valves to mimic the clinical situation in which a patientmight lie on the valve-side. The Orbis Sigma as well as the Heyer Schulte valve showed
67

dramatic deviations even on physiological subcutaneous pressure ranges of 20 mm Hg. Inaddition, all anti-siphon devices were found to be pressure-sensitive. The Hakim andHolter Hausner were stable, even under high pressure conditions. Schulte115 also report-ed the sensitivity of the Orbis Sigma valve to external pressure. As mentioned in 4.2.5 and4.2.6, Aschoff also applied pulsatile pressure of a flow amplitude during constant flow.Here he reported no effect when the valve was fully opened or closed, but a considerablyincreased flow around the opening and closing points.
Caution has to be taken when results obtained in a flow-driven rig have to be com-pared to results obtained in a pressure-driven rig. However, the fact that Aschoff did notfind any effect of pulsatile pressure-impositions on flow in a pump-driven test rig in situ-ations where the valve was completely opened or closed, supports our findings. Aschoffdid not report about the Phoenix valve, which was not very stable in our study. ThePhoenix valve is a proximal slit valve. As mentioned before, the mechanism of construc-tion of slit valves is based on the memory properties of silicone. There is no flow-restrain-ing element in shunts incorporating a slit valve. No plain explanation can be given for thesensitivity of the Phoenix valve to modulation. It is possible, however, that the architec-ture, mainly based on mechanical properties of silicone material is not able to adaptquickly to pressure fluctuations. In that case, it is surprising that the other slit valves didnot show any changes in operating pressure after pressure fluctuation. Strikingly, theOrbis Sigma valve functioned well after pressure modulation. Apparently, the mechanismis not so delicate that it cannot stand any of the applied large fluctuations in pressure atall.
4.2.8 Concluding remarksAschoff9,10,12,13 and Brydon26 stated that in all valve assessment procedures, both flow-and pressure-dependent valve assessment should be included. In this way, valve openingand closing pressures are measured by the pressure-driven test rig whereas the pulsatileCSF flow can be mimicked in a pump-driven system. We used a constant flow test rig,which might not adequately imitate normal, dynamic, CSF flow, although the pump in thetest rig actually produced a flow in a slight sinus-wave pattern. The syringe pump waschosen because this type of pump does not cause mechanical damage to erythrocytes. Inaddition, the modulation that was applied during testing quite well imitates the dynamicchanges in CSF flow. The fact that opening and closing pressures could not be recorded,is not a shortcoming of this study. We preferred recording the dynamic process of openingand closing instead of recording only one pressure value at the opening or closing of thevalve. Therefore, this study reports on a more practical directed description of openingand closing characteristics in which not only presssures play a role. This is a quite newapproach in shunt testing.
This study only recorded the short-term performance of the valves. Other studies byAschoff9,10,12 Schulte115 and Trost123,124 included measurements which were done overperiods of weeks to, occasionally, a year. These longer periods might give information onlong-term valve functioning, although we think that for comments on long-term function-
68
ing the valves should be tested much longer than a year. This was also stated by Aschoffhimself15. Therefore, the short-term testing as conducted in our study is enough to judgethe performance of the valve compared to the manufacturer’s specifications as well as itsopening and closing characteristics and performance after pressure modulation. Trostalready stated that the least that can be expected from a new valve, is to perform withinthe designated range as given by the manufacturer.
A last comment on the study could be that isolated valves were tested instead of com-plete shunt systems. We deliberately made this choice to get a better comparison with themanufacturer’s specifications. Other advantages are, that direct comparison between thevalves independent of catheters is possible and artefacts are minimized. The disadvantag-es of testing isolated valves are clear: the testing conditions are more distant from thephysiological situation and therefore the obtained values are more difficult to transpose topractice. Registration of siphoning is not possible. Aschoff9,10,11,12,13,14, Schulte115 andTrost123,124 performed studies in which they did applied the pressure of a vertical fluidcolumn on the valve and found overdrainage in nearly all valves. Only the Orbis Sigmaseemed to be able to maintain a reasonably constant flow, although this valve might actu-ally show underdrainage in CSF peak flow situations. In addition, the Orbis Sigma hasbeen reported to be prone to obstruction and sensitive to mechanical stress.
4.3 Conclusions
The conclusions are summarized below.
* About half of the valves performed in reasonable agreement with the manufacturer’sspecifications. Two out of three slit valves performed badly, as did the Orbis Sigmavalve.
* Protein up to a concentration of 10 g/l does not affect valve performance.
* Valve malfunctioning frequently occurred at erythrocyte counts higher than 5000cells/µl. The Orbis Sigma valve was most sensitive to erythrocytes, whereas only theHakim valve was able to perform well at erythrocyte counts up to 10.000 cells/µl.
* Most valves showed normal opening characteristics. Only the Raimondi valve, andsometimes the PS medical valve, showed a tendency for overshoot.
* All the valves showed good closing characteristics with saline perfusion.
* Overall, pressure modulation did not considerably affect valve performance. Only thePhoenix valve very frequently showed an alteration in performance after pressurechanges.
69

Chapter 5 General discussion
In this part a comparison between the clinical and the laboratory study will be made. Inaddition, we will attempt to explain the differences and give future directions
5.1 Comparison between clinical and laboratory results
First of all, it should be remarked that it is hard to compare results obtained in the laborato-ry, a non-physiological situation where several parameters are fixed, and results obtained inpractice, where many different, uncontrollable, parameters play a role in shunt functioning.
In the clinical situation, only a minor part of the number of shunt dysfunctions wascaused by valve problems. On the other hand, the laboratory results indicate that abouthalf of the valves did not perform according to the manufacturer’s specifications. In addi-tion to that, all valves except the Hakim valve were sensitive to eryhtrocyte counts above5000 cells/µl. Particularly the Orbis Sigma valve showed a tendency to obstruction witherythrocyte perfusion in the laboratory situation. Our laboratory results do not impose acontra-indication for shunt insertion in CSF containing high protein levels. We were notable to test the influence of high erythrocyte counts on shunt functioning in the clinicalsituation. Ninety percent of the patients had erythrocyte counts below 5000 cells/µl.Apparently, neurosurgeons decide not to insert shunts if the patient’s CSF contains a higherythrocyte count. Shunts incorporating the Orbis Sigma valve actually showed less dys-function in children under one year of age, whereas in older age groups there was no dif-ference between the valves. In the clinical setting, it was in fact the Raimondi valve thatshowed the highest revision rate.
The best explanation for this discrepancy between the laboratory and clinical results isprobably the already mentioned difference between testing in vitro in a laboratory situa-tion and the actual situation in vivo. Aschoff7,13 stated that whereas approximately 80%of the valves showed overdrainage both during testing and in a clinical situation, the clin-ical results of shunting are usually sufficient. Either the patients may be only partiallyshunt- dependent, or people in general are able to adapt to unphysiological low intracra-nial pressure in an upright position. Aschoff particularly stresses the enormous adaptabil-ity of the patients. In poor countries shunting usually takes place through an open ventric-uloperitoneal tube without a valve7. In fact, these systems may be the most frequentlyimplanted worldwide. Although this system does not incorporate an anti-reflux design,
70

and the flow rates are excessive, until now only subtle clinical differences from valve-incorporating shunts have been proven7. The Poisseuille equation shows that the internaldiameter of the silicone tubes is very important in determining the total shunt resistance:the equation includes the internal diameter in the fourth exponent. Actually, about 80 % ofthe total shunt resistance is determined by the tubes, whereas the resistance of the valve isonly a minor part of the total resistance. Less important are length and viscosity.Therefore, reducing the diameter of the tubes may be a reasonable option for reducingoverdrainage in CSF shunting in the clinical situation. Aschoff7,8 suggested to reduce theinternal diameter from the current 1.3-1.1 mm to 0.8-0.9 mm. According to him thiswould be an acceptable compromise between a more effective flow-control and the nec-essary obstruction-reserve. The question could be, mainly after reviewing the clinical study: ‘Does a shunt systemactually need a valve to function properly in a patient?’ If we would not set our standardsof shunt functioning too high, the answer could be no. However, according toAschoff7,8,13 there is a residual 20% of the patients which does need high-tech valveswith an exact function and a perfect compensation of postural pressure changes.Furthermore, for all patients we should strive for the optimal CSF shunting system, evensmall advantages of valve-use are valuable if they improve the patient‘s quality of life. Inthe clinical situation, the best option would be a shunt system with a smaller internal tubediameter including a programmable valve or a hydrostatic valve, or alternatively, anOrbis Sigma-like valve with a slightly increased outlet diameter which would not be asprone to obstruction as the current valve. Our study shows that an exception should bemade in the youngest age group. In this group we showed that significantly less revisionswere necessary in cases were the Orbis Sigma valve was used.
5.2 Future recommendations
Although CSF shunt surgery has improved greatly over time, it is still a treatment thatharbours many complications.Aschoff 7,8,13 posed several criteria for a satisfactorily functioning shunt system:
* a shunt should maintain the intracranial pressure within the physiological range, inde-pendent on body position or temporary increases in abdominal pressure. It should alsobe able to withstand CSF containing protein or debris
* a shunt should be highly biocompatible, durable and insensitive to external pressure
Our clinical study confirmed other studies, by showing that proximal catheter obstructionis the most frequent cause of shunt malfunctioning. In addition, we reported a correlationbetween a short ventricular catheter length and obstruction. A recommendation for thefuture could be to use ventricular catheters with a minimal length of 6 to 7 cm, dependingon the age of the patient.
71

In The Shunt Book43 Drake and Sainte-Rose stated that today no other materials couldreplace silicone elastomers in their wide medical applications. Silicone has been found tobe an inert material, with minimal reaction of the biologic system to its presence. In arecent report Kalousdian et al.70 reviewed all the articles that reported immunologicalreactions in patients with silicone CSF shunt systems. Over a period of 30 years, theyonly found five journal articles that described possible immunological reactions on CSFshunts. The evidence presented did not support the occurrence of immune-mediatedsystemic reactions to implanted silicone elastomer CSF shunts. In support of theAmerican Medical Association, they stated in 19933, that since each molecular speciesmay have differing potential for biological mobility and activity, it is mandatory to evalu-ate each product for safety and to avoid inappropriate extrapolations among differingchemical entities. Therefore, the controversies that have surrounded silicone gel-filledbreast implants are not relevant to the safety of silicone elastomer shunts. However, mul-tiple clinical problems still exist due to certain applications of silicone products. Theproblems are related to its surface properties62: in the blood, thrombi will form around sil-icone implants, which may dislodge and cause symptoms around the implants. In addi-tion, scar formation may occur, and in the eyes, where transparencies are needed as in theintraocular lens implant, the scar interfaces with the visual image transmissions.Schoener113 conducted a study on 36 explanted shunts and reported that 61 % of theshunts showed defects which led to tissue migration into shunt lumens or to tissue adher-ence to the tube surface. In every case of tube obstruction, he found calcification anddestruction of the silicone elastomer tubing. Brydon23,24 reported that more than 80 % ofexplanted valves containing metallic parts in their construction had internally accumulat-ed debris, whereas only 25 % of non-metallic valves showed accumulation of debris.According to Habal62, some of these internal problems relate to the hydrophobic nature ofthe silicone surface. In certain clinical applications, these problems have been resolved inpart by adsorbing a wetting agent, such as povidone, to the surface. Such obviation hasgained wide clinical application in surface coating of the intraocular lens. Habal statesthat ‘In search of an ideal implantable material, silicone, the most applicable, is still farfrom being called the ideal implant. Perhaps with the changes of its surface properties,such as introducing wetting agents to its surface, a new dimension in clinical applicationswill open the horizons of silicone in the 1980’s’. However, 14 years after this statement,shunt obstruction is still the most frequently found complication after shunt surgery,which indicates the importance of biocompatibility of the shunt materials. Furtherresearch will be necessary to improve the biodurability and biocompatibility of CSFshunt systems.
As mentioned above, a way to reduce overdrainage could be to use tubes with a redu-ced internal diameter together with a conventional valve, or to use an Orbis Sigma valvewith a slightly larger outlet, which is not as sensitive to obstruction as the current OrbisSigma valve.In the youngest age group, we would like to recommend the use of the Orbis Sigma val-ve. This valve gave significantly less complications in children under one year of age.
72

Although the shunt infection rate is rather low in the Netherlands compared to othercountries, it would still be useful to aim preventive measures at high-risk patients, whocan mainly be found in the youngest age group. Shunt impregnation with antibiotics maybe a useful method here.
In the clinical chapter we quoted Rekate106 who stated :’The best shunt is no shunt’.Indeed, further improvement and use of the endoscopic techniques will decrease the needfor shunts in the future. However, in the near future, shunts will still be widely used in thetreatment of hydrocephalus.
In the clinical chapter we already mentioned the importance of the quality of life inthe evaluation of shunt functioning. If the patient’s quality of life is excellent, in spite ofseveral shunt revisions, the evaluation of shunt surgery should be positive in stead of neg-ative, which it would have been in the current studies. Future studies should include thepatient’s quality of life as an important parameter in the evaluation of shunt functioning.
73

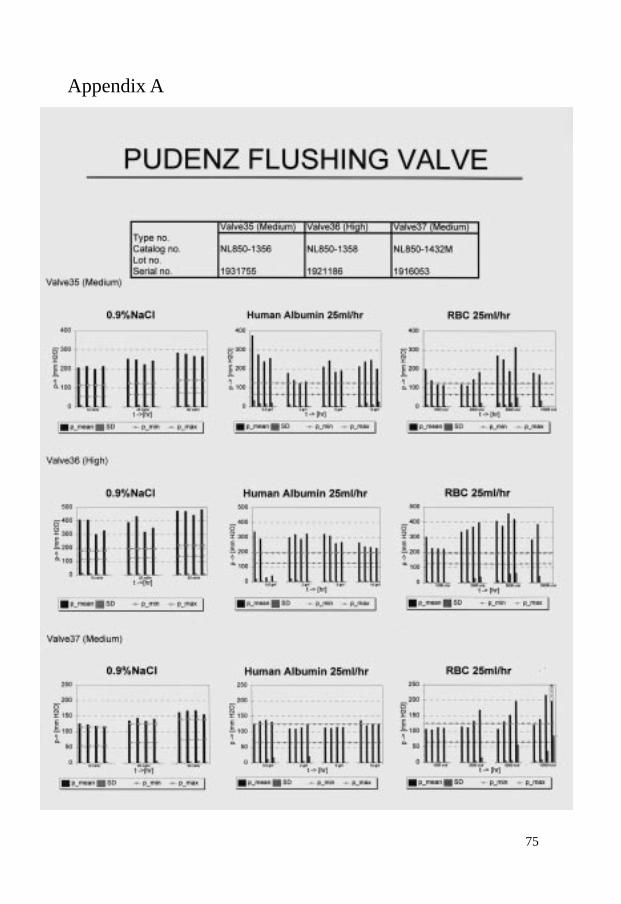
Appendix A
75
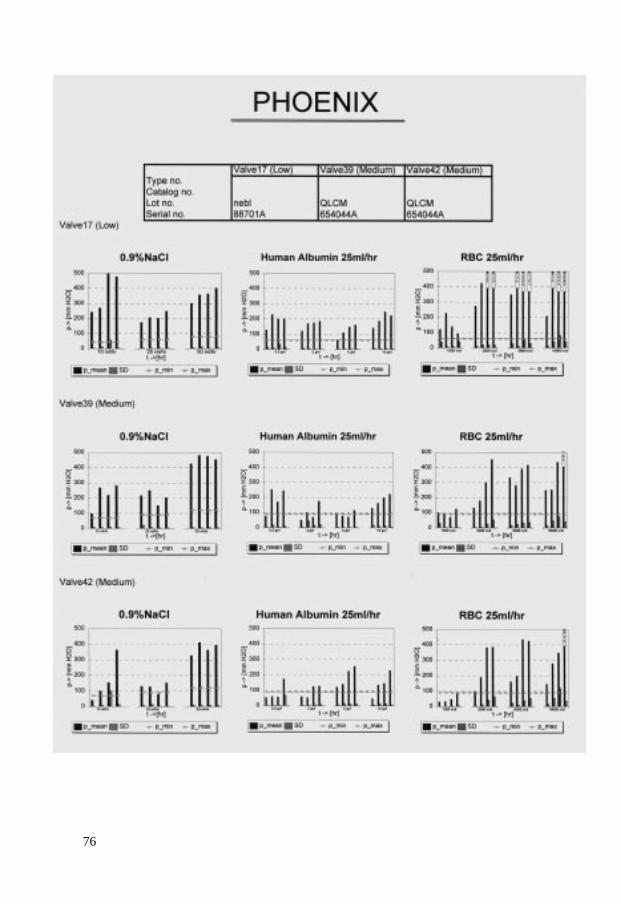
76
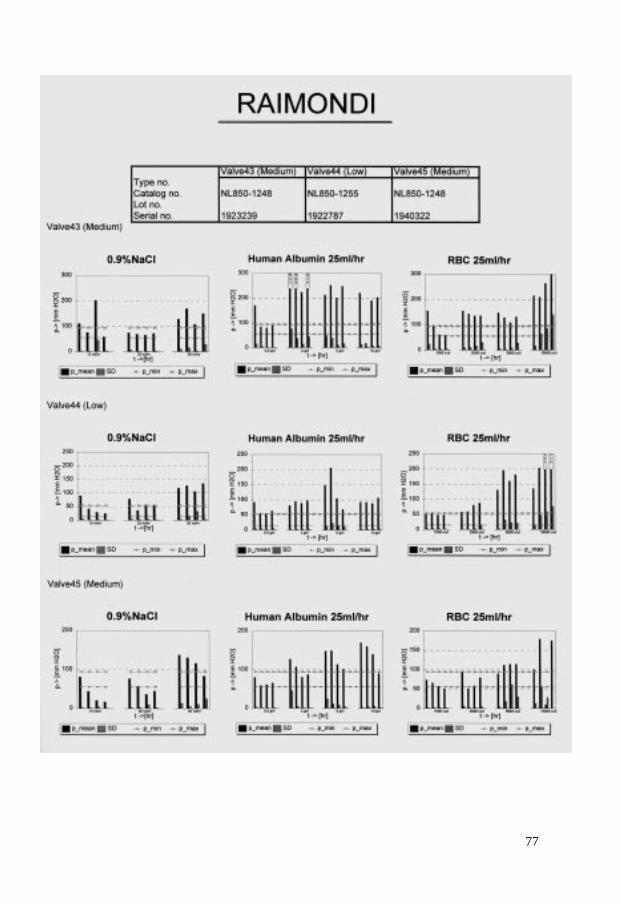
77
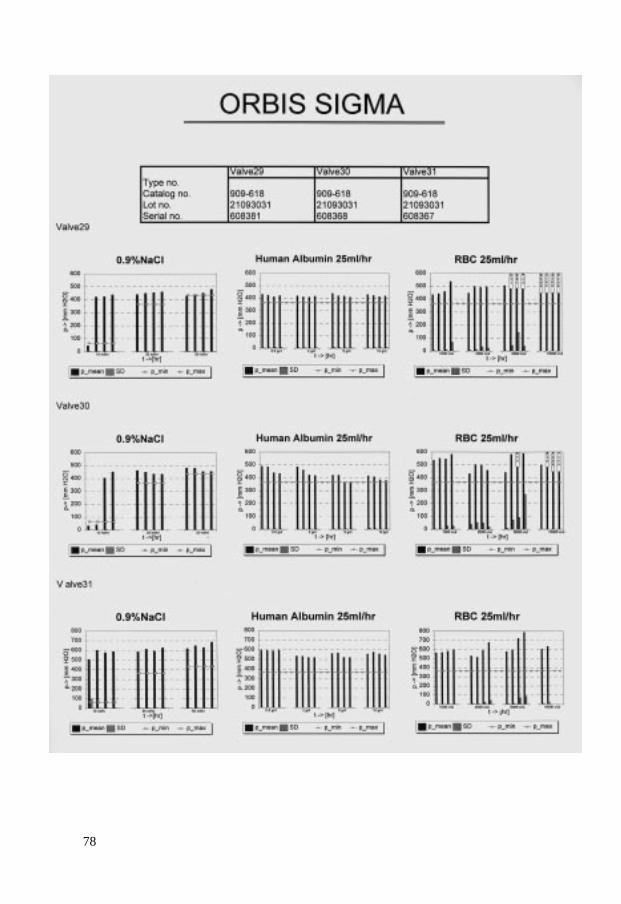
78
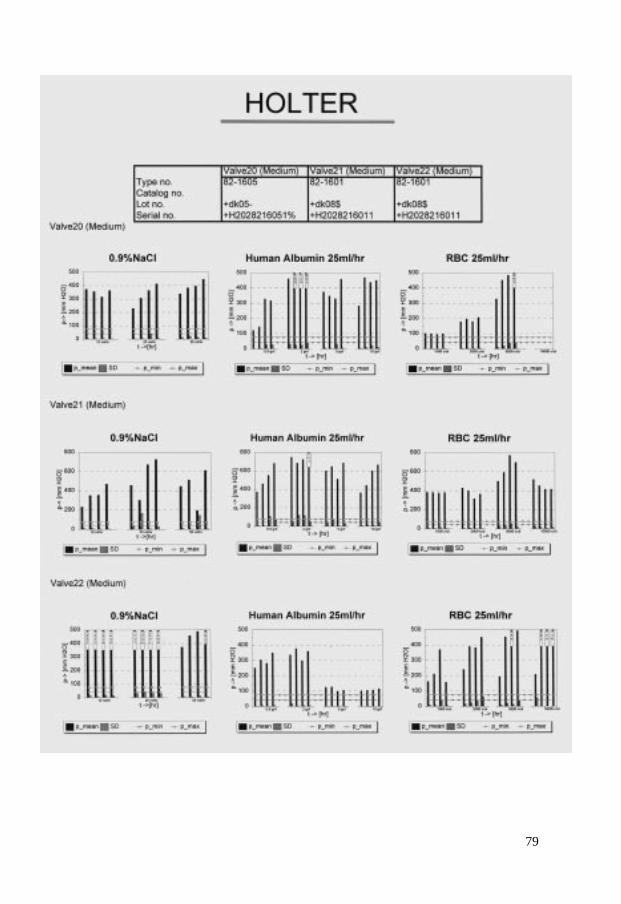
79
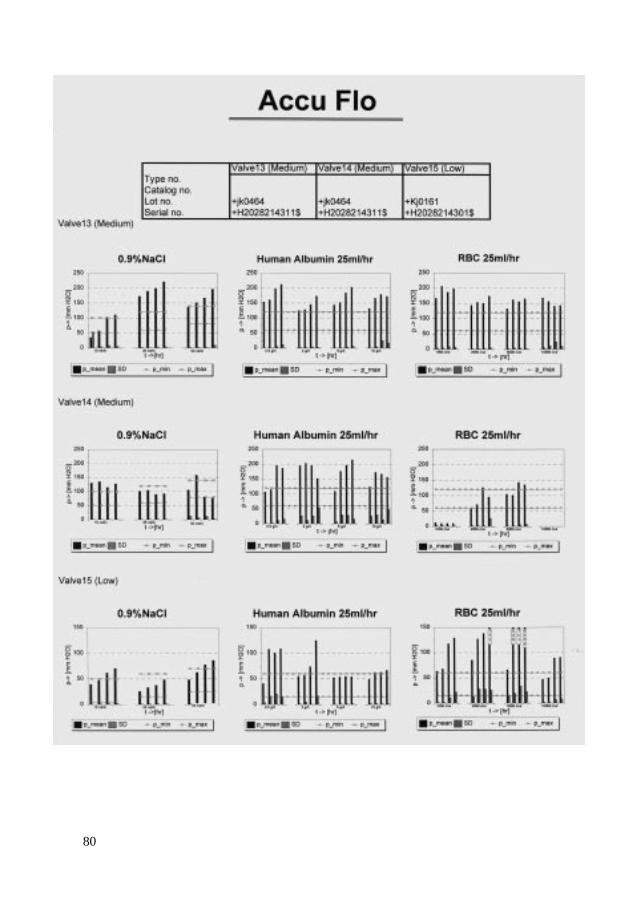
80
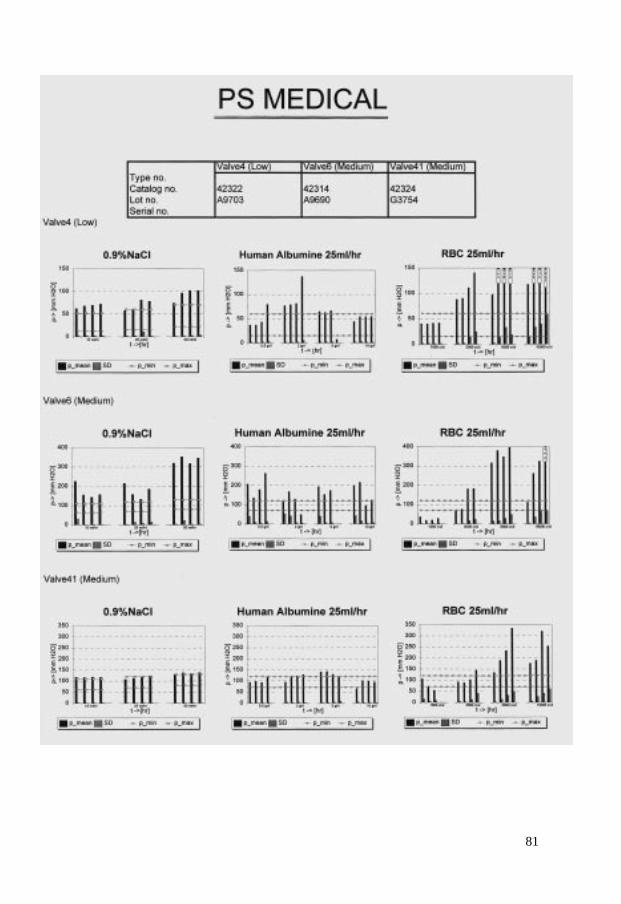
81
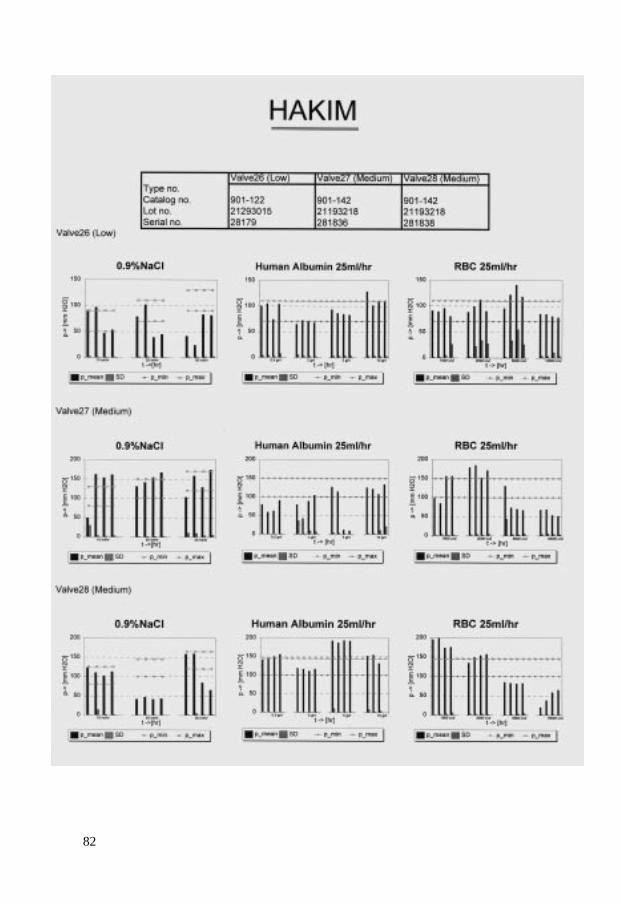
82
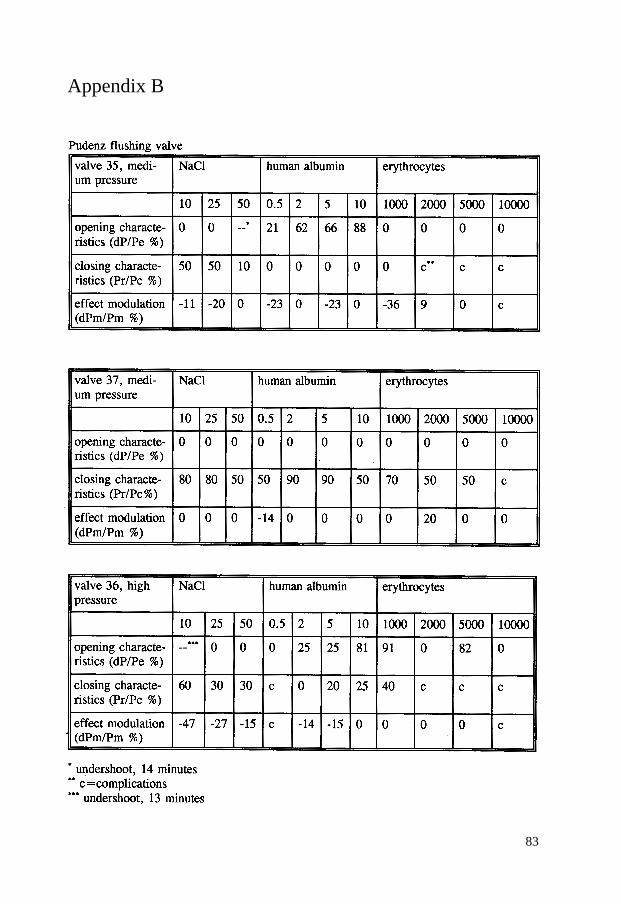
Appendix B
83
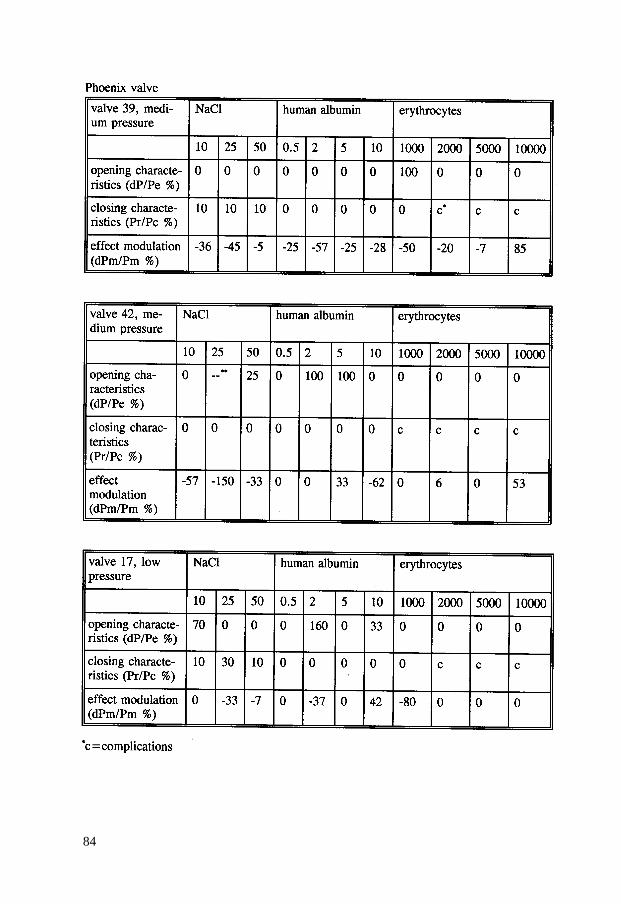
84
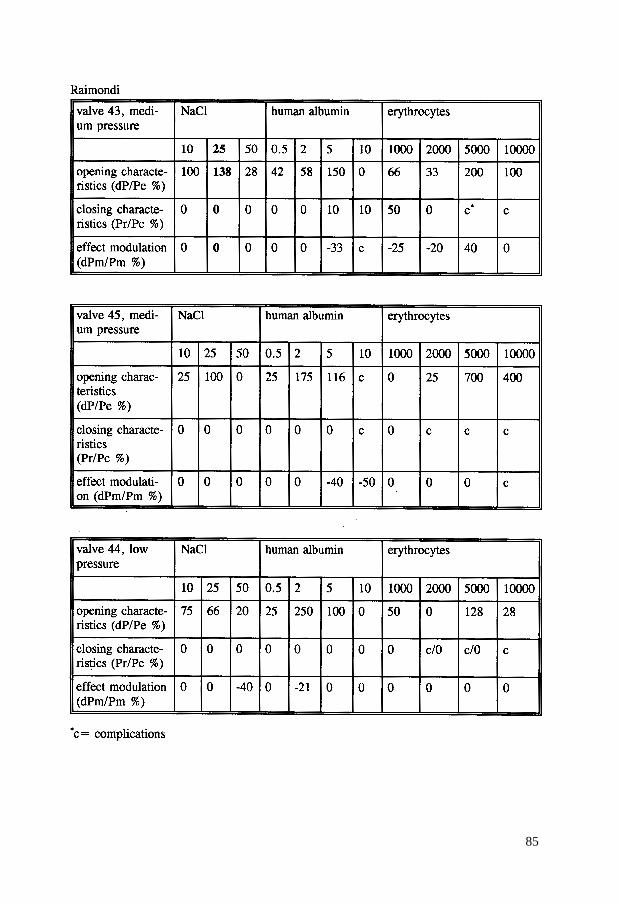
85
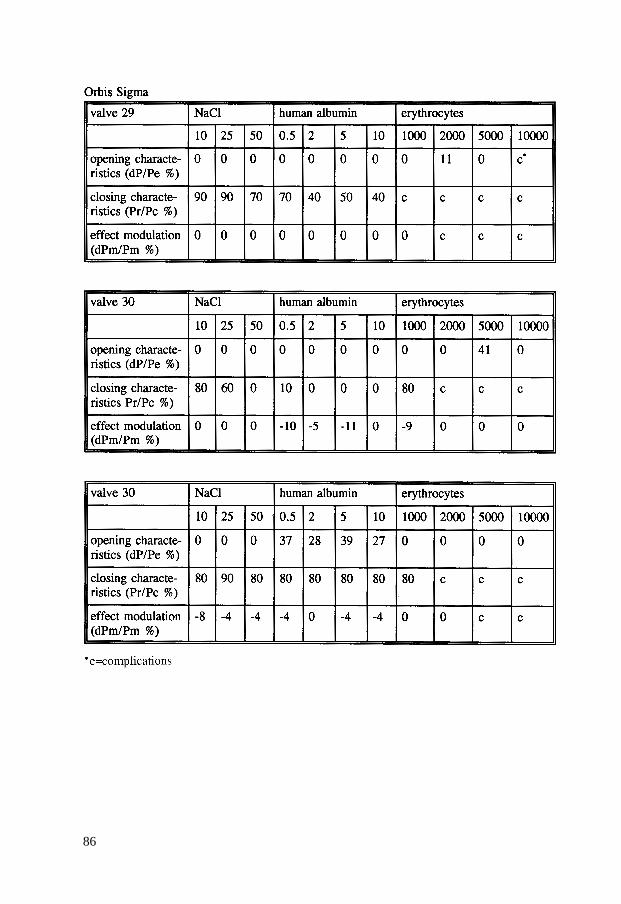
86
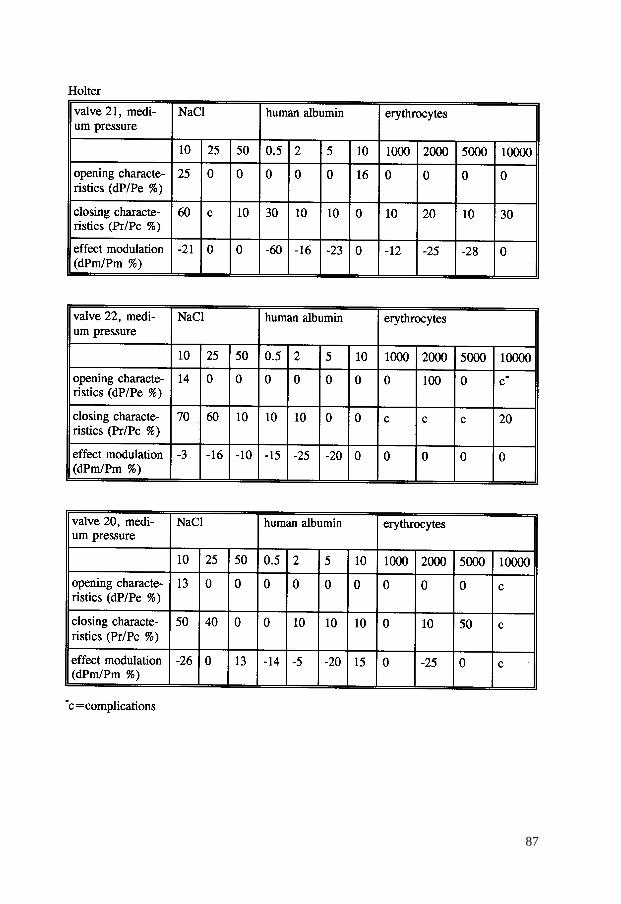
87
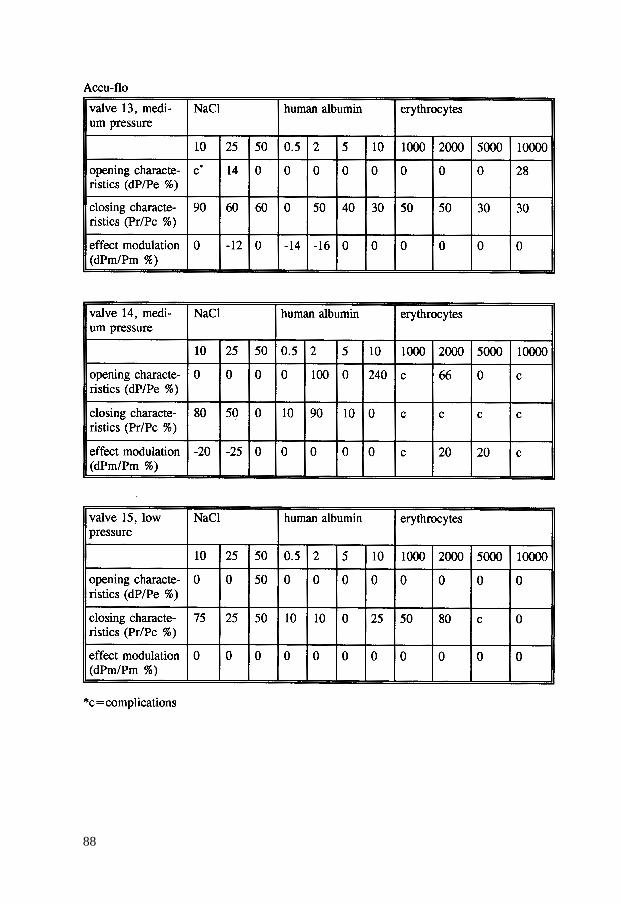
88
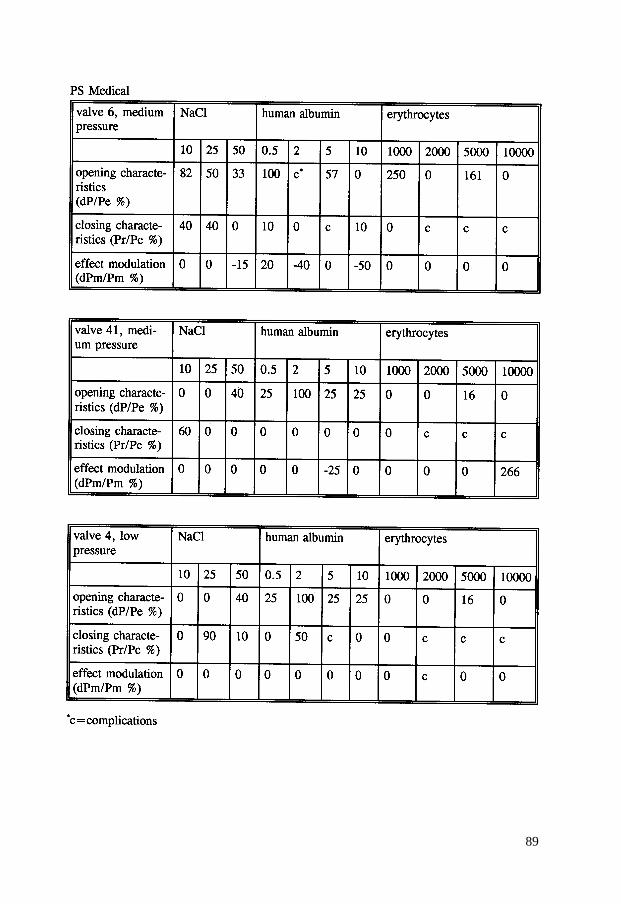
89
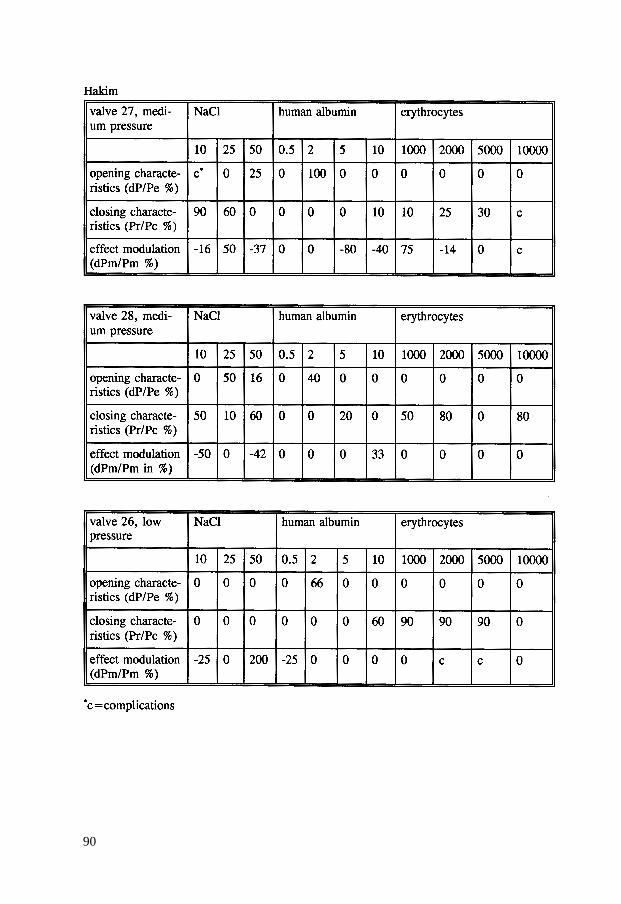
90
Summary
Introduction
This thesis is about the treatment of hydrocephalus and the problems that come with it.Hydrocephalus is characterized by an abundance of cerebrospinal fluid (CSF) in the cere-bral ventricles. In general, hydrocephalus is accompanied by a surplus of pressure withinthe skull, which causes quickened skull growth in infants and might result in neurologicaldisorders. Since the nineteen fifties, hydrocephalus treatment has largely consisted ofimplantation of a shunt system which drains the superfluous fluid. The shunt system con-sists of drains in between which a valve is placed. The shunt connects the ventricles, inwhich the pressure is too high, with a compartment in which the pressure is low. In clini-cal practice, the abdominal cavity or the right atrium is used for the drainage of superflu-ous fluid. The valve is responsible for a fluid flow in one direction (away from the skull),preventing blood for example to flow back. Moreover, the valve regulates the pressurelevel within the skull by opening at high pressure and closing again after the pressure hasbeen normalized.
Chapter 1
In this chapter, the research set-up is described and the history of the surgical treatment ofhydrocephalus patients is briefly reported. In the Netherlands, about 650 new shunt sys-tems are implanted each year and about 500 shunt operations are performed after compli-cations of previously implanted systems. Thus, hydrocephalus surgery is an importantpart of the neurosurgical practice. Nevertheless, at the end of the nineteen eighties, thereseemed to be little communication between neurosurgeons about the different shunt sys-tems used, operation techniques and complications. Moreover, the implications of devia-tions in CSF composition such as high protein concentration or increase in erythrocytecounts, remained unclear. In the pre-1990 literature, there were contradicting reports on theinfluence of protein, and no research had ever been done on the effects of erythrocytes onthe functioning of hydrocephalus shunts. Therefore, it seemed important to examine theuse of hydrocephalus shunts in the Netherlands. A combined set-up was chosen of clini-cal research on one hand and laboratory experiments on the other. An inventory was made of the shunt systems used in the Netherlands and their complica-
91

tions. Also, it was examined whether increase in protein concentration or erythrocytecount in a laboratory setting altered the hydrodynamic characteristics of the different val-ves. Results after perfusion with saline were compared with the manufacturer’s specifica-tions and served as a point of reference. Subsequently, these data were compared with theclinical results to see if the differences between the valve types and the influence of pro-tein and blood concentration correlated to clinical practice.In the second part of the first chapter, a general overview is given of the surgical treat-ment of hydrocephalus in the last century. Of great importance to the development ofshunt systems was the discovery of silicone elastomer in 1945, which was originally usedas sealing material for airplane engines. Since then, over a hundred different valves havebeen manufactured, with occasional variations in their matching drains. In spite of thesedevelopments, complications keep occurring after implantation of shunt systems.
Chapter 2
In this chapter, the clinical study is described. From eight Dutch neurosurgical centers,400 patients were followed after primary shunt operation during a period of between 21/2 and 5 years. Patients were divided into three different age groups: 0 - 1, 1-15 and over16 years of age. Complications during the follow-up period were registered and analyzed.Results were compared with data from the recent literature. During follow-up, 200 revi-sion operations were performed, which is a low amount compared to numbers indicatedin the recent literature. The nature of the problems occurring after shunt implantation wascomparable with complications indicated in previous studies, where obstruction of theventricular catheter was the most frequent cause of shunt dysfunction. Infections occur-red relatively rarely and morbidity (2.3%) and mortality (0.5%) rates after primary shuntimplantation were low. In the youngest age group, a lower revision rate was found afterimplantation of the Orbis Sigma valve compared to the group of patients who wereimplanted with one of the other valves. In about one third of the patients, the compositionof the ventricular CSF was examined just before or during the operation. After data anal-ysis, it turned out that no relation existed between protein concentrations or amounts oferythrocytes and revision rates.
Chapter 3
In this chapter, some background information is given on CSF dynamics and valve archi-tecture, which is important for a better insight in shunt function and dysfunction. The CSFis produced more or less continually, mainly in the choroid plexus, and is absorbed intothe venous system. When the balance of production and resorption is disturbed, hydro-cephalus occurs. By implanting a shunt, the CSF flow is regulated. Four basic physiolog-ical principles are important: pressure, flow, resistance and viscosity. Pressure changes in
92

different body compartments have influence on the CSF flow through the shunt. The cur-rently used valves differ from each other in architecture and materials. For example, bal-ls connected to springs are used, next to mobile membranes and slits in the contact sur-face as a mechanism to arrest fluid or allow it passage. Each valve type therefore has dif-ferent hydrodynamic characteristics.
Chapter 4
In this chapter, the set-up and the results of the laboratory study are discribed. In thelaboratory, the eight most frequently used valves from the clinical study were subjected toa test program. To that purpose, a test rig was developed, taking into consideration certainfactors important in vivo. The testing enabled a continual supply of perfusion fluid andalso large pressure changes could be induced. The valves were perfused with saline at dif-ferent flow rates. In this way reference points were obtained, which were then comparedwith the manufacturer’s specifications. Subsequently, the valves were perfused with pro-tein concentrations of up to 10g/L and solutions with an increasing amount of erythrocy-tes up to 10.000/µL. The pressure rates measured after protein and erythrocyte perfusionwere compared with the reference points obtained after perfusion with saline. Also, thedifferences in pressure pattern during opening and closing of the different valve typeswere looked at and potential alterations after induced pressure changes were analyzed.From the laboratory results, it became apparent that about half of the valves performed inreasonable agreement with the manufacturer’s specifications. In the other valves, theobtained pressure rates were considerably higher than those given by the manufacturer.An increase in protein concentration of up to 10g/L did not cause any alterations in theaggregation in the system. In two valves, a deviation in pressure rates could be observedregularly during the opening of the valve, whereas four valves showed regular functionchanges after artificially induced pressure variations. The valves closed adequately dur-ing perfusion with saline.
Chapter 5
In this chapter, the relationship between the results of the laboratory study and the resultsobtained in clinical practice is further analyzed. Also, the possibilities of future improve-ment in hydrocephalus treatment are discussed. It is important to note that the clinical sit-uation can never be entirely imitated in the laboratory. In the clinical study it becameapparent that dysfunction due to valve obstruction occurred only in 10 cases (5%) andover or underdrainage in an unobstructed valve occurred in 7 cases (3.3%). It can be con-cluded that the valve itself is not the greatest source of problems in the clinical situation.It appeared in the laboratory study that relatively high protein concentrations are of noinfluence on valve functioning but the presence of erythrocytes (from 5000/µL) can be of
93

influence. Protein concentrations of up to 3.5g/L did not appear to cause any complica-tions in the clinical study. Higher concentrations were not observed there. From the factthat 90% of the patients examined had less than 5000 erythrocytes per µL in their CSF, itcan be concluded that Dutch neurosurgeons are rather reticent in implanting shunts athigher erythrocyte counts. These results were hard to compare with the results of thelaboratory study because in the latter instance alterations in valve functioning occuredmainly at cell concentrations of 5000/µL onwards. After it had appeared that the results ofabout half of the valves deviated clearly from the manufacturer’s specifications, the ques-tion arose whether it is important that a valve has a clearly defined, physiologically deter-mined working range. Given the regularly observed high pressure rates it could be pos-sible that people are only partially shunt-dependent or that the possibilities of adaptiationto non-physiological circumstances are larger than thought. The silicone elastomer, pro-cessed in drains and valves, could induce interaction with surrounding substances, whichcould cause obstruction or weakening of the material. As a shunt is often a life-longimplant, improvement of biocompatibility and durability of used materials might contrib-ute to a decrease in the number of complications and a lengthening of life duration. Evenbetter it would be to find a way of treating hydrocephalus without having to implant mate-rials alien to the body. Through the increase of neuro-endoscopical experience andimprovement of belonging appliances, it will become more and more possible to treathydrocephalus without shunt implantation in future.
94
Samenvatting
Inleiding
Dit proefschrift gaat over de behandeling van hydrocefalie en de problemen die zich daar-bij voordoen. Een hydrocefalus kenmerkt zich door een te grote hoeveelheid vocht(liquor) in de hersenkamers, waardoor een zogenaamd “waterhoofd” ontstaat. Over hetalgemeen gaat de hydrocefalie gepaard met een te hoge druk binnen de schedel, die een tesnelle schedelgroei bij kinderen tot ongeveer 1 jaar en neurologische stoornissen totgevolg kan hebben. De behandeling van de hydrocefalus bestaat sinds de jaren ’50 vooreen belangrijk deel uit implantatie van een shuntsysteem dat de overtollige liquor afvoert.Het shuntsysteem is samengesteld uit drains waartussen een klep geplaatst is. De shuntverbindt de hersenkamers waarbinnen een te hoge druk heerst met een compartimentwaarbinnen een lagere druk heerst. In de praktijk wordt de buikholte of het hart gebruiktvoor de afvoer van de overtollige liquor. Het klepje zorgt voor een vloeistofstroom in éénrichting (van de schedel af) waardoor het terugstromen van bijvoorbeeld bloed voorko-men wordt. Voorts regelt de klep het drukniveau binnen de schedel doordat deze opengaat bij een te hoge druk en sluit wanneer de druk genormaliseerd is.
Hoofdstuk 1
In dit hoofdstuk wordt de onderzoeksopzet beschreven en wordt de geschiedenis van dechirurgische behandeling van hydrocefaliepatiënten in het kort weergegeven. In Nederlandworden per jaar ongeveer 650 nieuwe shuntsystemen geïmplanteerd en worden er ongeveer500 operaties aan shunts uitgevoerd na complicaties ten gevolge van eerder geplaatste sys-temen. Hydrocefaliechirurgie vormt dan ook een belangrijk onderdeel van de neuro-chirurgische praktijk. Desalniettemin bleek er eind jaren ’80 tussen de neurochirurgenonderling weinig gecommuniceerd te worden over de verschillende shuntsystemen welkewerden gebruikt, de operatietechniek en de complicaties. Daarnaast bestond er onduide-lijkheid over de implicaties van afwijkingen in samenstelling van de liquor zoals verho-ging van de eiwitconcentratie en toename van het aantal rode bloedcellen. In de literatuurvan voor 1990 waren er elkaar tegensprekende berichten met betrekking tot de invloedvan eiwit, terwijl er geen onderzoek verricht was naar de effecten van rode bloedcellen opde werking van hydrocefaliekleppen. Derhalve leek het van belang het gebruik van
95

hydrocefalieshunts in Nederland nader te onderzoeken. Gekozen werd voor een gecombi-neerde opzet van klinisch onderzoek enerzijds en laboratoriumexperimenten anderzijds.Er vond een inventarisatie van de in Nederland gebruikte shuntsystemen en hun compli-caties plaats. Daarnaast werd nagegaan of verhoging van eiwitconcentratie en het aantal rodebloedcellen in een laboratoriumopstelling leidde tot verandering van de hydrodynami-sche eigenschappen van de verschillende kleppen. De resultaten tijdens perfusie metfysiologisch zout werden vergeleken met de door de fabrikant verstrekte gegevens endienden als referentiewaarde. Vervolgens werden deze gegevens vergeleken met de klini-sche resultaten om te zien of de verschillen tussen de kleppen onderling en de invloed vaneiwit en bloedconcentratie correleerden met de klinische praktijk.In het tweede deel van het eerste hoofdstuk wordt een overzicht gegeven van de chirurgi-sche behandeling van hydrocefalie in de afgelopen eeuw. Van belang voor de ontwikke-ling van shuntsystemen was de ontdekking van silicone-elastomeer (1945) dat oorspron-kelijk gebruikt werd als afdichtmateriaal voor vliegtuigmotoren. In de loop der tijd zijn ermeer dan 100 verschillende kleppen op de markt verschenen met soms ook variaties inbijbehorende drains. Ondanks deze ontwikkelingen blijken er veel complicaties te blijvenoptreden na implantatie van een shuntsysteem.
Hoofdstuk 2
In dit hoofdstuk wordt het klinische onderzoek beschreven. Uit acht nederlandse neuro-chirurgische centra werden 400 patiënten na primaire shuntimplantatie gevolgd geduren-de een periode die varieerde tussen de 2 1/2 en 5 jaar. Patiënten werden naar leeftijdonderverdeeld in drie groepen: 0 - 1, 1 - 15 en ouder dan 16 jaar. De complicaties gedu-rende de follow-up periode werden geregistreerd en geanalyseerd. De resultaten werdenvergeleken met de gegevens uit de recente literatuur. Gedurende de follow-up periodewerden er 200 revisie-operaties uitgevoerd, hetgeen laag is vergeleken met de in de lite-ratuur aangegeven aantallen. De aard van de problematiek na shuntimplantaties was goedvergelijkbaar met de in eerdere studies aangegeven complicaties, waarbij obstructie vande ventriculaire catheter de meest frequente oorzaak van problemen was. Infecties kwa-men relatief weinig voor en de morbiditeit (2,3%) en de mortaliteit (0.5%) na primaireshuntimplantatie waren laag. In de jongste leeftijdsgroep werd na implantatie van eenOrbis Sigma klep een lager revisiepercentage gevonden, vergeleken met de groep patiën-ten die één van de andere kleppen geïmplanteerd kregen. Bij ongeveer 1/3 van de patiën-ten werd vlak voor of tijdens de operatie de samenstelling van de ventriculaire liquoronderzocht. Uit analyse van de gegevens bleek er geen relatie te bestaan tussen hogereconcentraties eiwit of een hoger aantal rode bloedcellen in de liquor en het revisiepercen-tage.
96
Hoofdstuk 3
In dit hoofdstuk wordt enige achtergrondinformatie gegeven met betrekking tot liquordy-namiek en kleparchitectuur, hetgeen van belang is om een beter inzicht te krijgen in func-tie en disfunctie van shunts. De liquor wordt min of meer continu geproduceerd, voorna-melijk in de plexus choroideus, waarna opname volgt in het veneuze systeem. Wanneer hetevenwicht van productie en resorptie verstoord raakt, ontstaat een hydrocefalie. Door hetimplanteren van een shunt wordt de liquorstroom gereguleerd. Vier fysiologische basis-principes spelen een rol: druk, flow, weerstand en viscositeit. Drukveranderingen in deverschillende lichaamscompartimenten hebben invloed op de vloeistofstroom door deshunt. De in omloop zijnde kleppen verschillen qua architectuur en gebruikte materialen.Er wordt o.a. gebruik gemaakt van balletjes verbonden met een veertje, een beweegbaremembraan en sleufjes in het contact-oppervlak als mechanisme om vloeistof tegen te hou-den of door te laten. Ieder kleptype heeft dan ook andere hydrodynamische eigenschappen.
Hoofdstuk 4
In dit hoofdstuk worden opzet en resultaten van het laboratoriumonderzoek beschreven.In het laboratorium werden de acht in het klinische onderzoek meest gebruikte kleppenaan een testprogramma onderworpen. Daartoe werd een testopstelling ontwikkeld waar-bij rekening gehouden werd met een aantal factoren die in vivo van belang zijn. Deopstelling voorzag in de mogelijkheid van een continue aanbod van perfusievloeistof enhet was tevens mogelijk grote drukschommelingen te induceren. De kleppen werdengeperfundeerd met fysiologisch zout met verschillende flowsnelheden. Op deze wijzewerden referentiewaarden verkregen welke werden vergeleken met de door de fabrikantvan de kleppen opgegeven waarden. Vervolgens vond perfusie plaats met eiwitoplossin-gen in concentratie oplopend tot 10g/L en oplossingen met een oplopende hoeveelheidrode bloedcellen tot maximaal 10.000/µL. De gemeten druk na toevoegen van eiwit enrode bloedcellen werd vergeleken met de verkregen referentiewaarden na perfusie metfysiologisch zout. Daarnaast werd er ook gekeken naar verschillen in drukpatroon tijdenshet openen en sluiten van de diverse kleppen en ook eventuele veranderingen na geïndu-ceerde drukschommelingen werden geanalyseerd. Uit het onderzoek bleek dat de referen-tiewaarden van ongeveer de helft van de kleppen redelijk overeenkwamen met defabriekspecificaties. Bij de andere kleppen was de gemeten druk duidelijk hoger dan dedoor de fabriek opgegeven waarden. Verhoging van de eiwitconcentratie tot 10g/L resul-teerde niet in een verandering van eigenschappen van de kleppen. Er van uitgaande datverhoging van de viscositeit de eigenschappen van kleppen verandert, is het resultaatcongruent met deze vooronderstelling, omdat toename van de eiwitconcentraties slechtsleidt tot een geringe toename van de viscositeit. Bij de meeste kleppen traden wel veran-deringen op bij perfusie met hogere concentraties rode bloedcellen. Deze veranderingenwerden verklaard door partiële en soms ook totale obstructie van de klep die veroorzaakt
97

zou kunnen worden door aggregatie van cellen in het systeem. Bij twee kleppen konregelmatig een afwijkend drukpatroon tijdens het openen van de klep geconstateerd wor-den, terwijl bij vier kleppen regelmatig veranderingen in functie optreden na artificieelgeïnduceerde drukschommelingen. Het sluiten van de kleppen was adequaat te noementijdens perfusie met fysiologisch zout.
Hoofstuk 5
In dit hoofdstuk wordt de relatie tussen de resultaten van het laboratoriumonderzoek ende klinische bevindingen nader geanalyseerd. Daarnaast wordt ingegaan op mogelijkhe-den tot verbetering van de hydrocefaliebehandeling in de toekomst. Het is van belang aante geven dat de klinische situatie in het laboratorium nooit helemaal na te bootsen is. Uithet klinisch onderzoek bleek dat er slechts in tien gevallen (5%) sprake was van disfunc-tie door obstructie van de klep en dat er in zeven gevallen (3,5%) over-of onderdrainagewas bij een doorgankelijke klep. Geconcludeerd kan worden dat de klep niet de grootstebron van problemen was in de klinische situatie. Uit het laboratoriumonderzoek bleek dateen hoge eiwitconcentratie geen invloed heeft op de klepfunctie en dat de aanwezigheidvan rode bloedcellen (vanaf 5000/µL) wel van invloed kan zijn. Eiwitconcentraties tot3,5g/L bleken in het klinisch onderzoek niet tot meer complicaties te leiden. Hogere con-centraties werden in het klinisch onderzoek niet waargenomen. Uit het feit dat 90% vande onderzochte patiënten minder dan 5000 rode bloedcellen perµL in de liquor had, blijktdat de Nederlandse neurochirurgen terughoudend zijn met het implanteren van shunts bijhogere aantallen erythrocyten. Deze resultaten lieten zich niet goed vergelijken met debevindingen van het laboratoriumonderzoek omdat in de laatst genoemde omstandigheidvoornamelijk verandering van klepfunctie optrad vanaf een celaantal van 5000/µL. Toenbleek dat de resultaten van ongeveer de helft van de kleppen duidelijk afweken van defabrieksspecificaties, wierp zich de vraag op in hoeverre het belangrijk is dat een klep eennauwkeurig omschreven, fysiologisch bepaald werkgebied zou moeten hebben. Geziende regelmatig geconstateerde hoge druk zou het mogelijk kunnen zijn dat mensen slechtsgedeeltelijk shunt-afhankelijk zijn of dat de aanpassingsmogelijkheden aan onfysiologi-sche omstandigheden groter zijn dan gedacht. Het silicone-elastomeer, dat in drains enkleppen verwerkt is, kan aanleiding geven tot interaktie met omgevende stoffen waardoorverstopping of verzwakking van het materiaal kan optreden. Omdat een shunt vaak eenlevenslang implantaat is, zal verbetering van de biocompabiliteit en de duurzaamheid vande gebruikte materialen kunnen bijdragen aan een vermindering van het aantal complica-ties en het verlengen van de levensduur. Nog beter lijkt het een behandeling van de hydro-cefalie te bedenken die niet gepaard gaat met implanteren van lichaamsvreemde materia-len. Door toename van de neuro-endoscopische ervaring en verbetering van de bijbeho-rende hulpmiddelen, zal het in de toekomst vaker mogelijk zijn implantatie van een shuntte voorkomen.
98
References
1. Adams RD, Fischer CM, et al. (1965) Symptomatic occult hydrocephalus with “normal” CSFpressure: A treatable syndrome. N Eng J Med 273:117-126
2. Albright AL, Haines SJ, Taylor FH (1988) Function of parietal and frontal shunts in childhoodhydrocephalus. J Neurosurg 69:883-886
3. American Medical Association, Council on Scientific Affairs (1993) Silicone gel breastimplants. JAMA 270: 2602-2606
4. Ames RH (1967) Ventriculoperitoneal shunts in the management of hydrocephalus. JNeurosurg 27: 525-529
5. Anderson M, Matthews KB, Stuart J (1978) Coagulation and fibrinolytic activity of cerebro-spinal fluid. J Clin Path 31: 488-492
6. Aronyk KE (1993) The history and classification of hydrocephalus. Neurosurg Clin America4: 599-610
7. Aschoff A, Benesch C, Krämer P, von Haken M, Klank A, Osterloh M, Fruh K (1992) Gelösteund ungelöste Probleme der Hydrocephalus-Ventiltechnik. Ein Standortbestimmung. 43.Jahrestagungder Deutschen Gesellschaft für Neurochirurgie, Frankfurt/M., May 10-12
8. Aschoff A (1992) Schunt function Technology. Lecture, University of London, Institute ofChild Health, Course Shunting for Hydrocephalus, March 11
9. Aschoff A, Osterloh M, Kunze S (1990) Criteria and methods for testing hydrocephalusvalvesand anti-siphon devices: results of 102 tested examples. Presented at the Joint meeting of theHellenic Neurosurgical Society and der Deutschen Gesellschaft für Neurochirurgie, Athens,Greece. October 14-17
10. Aschoff A, Osterloh M, Kunze S (1990) Long-time tests of 34 hydrocephalus valves.Presented at the 18th Annual Scientific Meeting of the International Society for PediatricNeurosurgery, Paris, France. September 17-19.
11. Aschoff A, Benesch C, Kremer P, von Haken MS, Klank A, Osterloh, M, Fruh K (1995) Thesolved and unsolved problems of hydrocephalus valves: a critical comment. Adv Neurosurg21: 103-114.
12. Aschoff A, Kremer P, Benesch C, Fruh K, Klank A, Kunze S (1995). Overdrainage and shunttechnology. A critical comparison of programmable, hydrostatic and variable-resistance valvesand flow-reducing devices. Child’s Nerv Syst 11: 193-202
13. Aschoff A, Kremer P, Benesch C, Hashemi, B, Leonhardt S, Kunze St (1996) 383 shunt-valvesin bench-test - sufficient or desastrous? XVth Congress of the European Society for PediatricNeurosurgery, Rome, September 21-25
14. Aschoff A, Kremer P, Benesch C, Hashemi B, Leonhardt S, Kunze S (1996) Bench tests on363 shunt valves - are they adequate or a disaster? Child’s Nerv Syst 12: 494
15. Aschoff A, Kremer P (1998) Determining the best cerebrospinal fluid shunt valve design: thepediatric valve design trial. Neurosurgery 42: 949-951
16. Backlund EO, Grepe A, Lunsford D. (1968) Stereotactic reconstruction of the aqueduct ofSylvius. J Neurosurg 28: 215-226
99
17. Barat JL, Decq P, Duplessis E, Gendrault P, Le Guerinel C (1990) Shunting complications inthe treatment of adult hydrocephalus: flow-regulating valves versus diferential-pressure val-ves. December 1990 meeting, Paris
18. Bayston R., Lambert E. (1997) Duration of protective activity of cerebrospinal fluid shuntcatheters impregnated with antimicrobial agents to prevent bacterial catheter-related infection.J Neurosurg 87: 247-251
19. Bierbrauer KS, Storrs BB, McLone DG, Tomita T, Dauser R. (1990-1991) A prospective, ran-domized study of shunt function and infections as a function of shunt placement. PediatrNeurosurg 16: 287-291
20. Boon AJW, Tans JTJ, Delwel EJ, Egeler-Peerdeman SM, Hanlo PW, Wurzer HAL, Avezaat,CJJ, De Jong DA, Gooskens RHJM, Hermans J (1998) Dutch normal-pressure hydrocephalusstudy: randomized comparison of low- and medium-pressure shunts. J Neurosurg 88: 490-495
21. Bradbury MWB, Cole DF (1980) The role of the lymphatic system in drainage of cerebrospi-nal fluid and acqueous humour. J Physiol (Lond) 299: 353-365
22. Brydon HL, Bayston R, Hayward R, Harkness W (1996) Removed shunt valves: reasons forfailure and implications for valve design. Br J Neurosurg. 10 (3): 245-51
23. Brydon HL, Bayston R, Hayward RD, Harkness WFJ (1994) Explanted shunt valves: factorscontributing to their failure. Eur J Pediatr Surg 4, suppl. I: 37-38
24. Brydon HL, Hayward R, Harkness W, Bayston R (1995) Physical properties of cerebrospinalfluid of relevance to shunt function. 1: The effect of protein upon CSF viscosity. Br JNeurosurg 9: 639-644
25. Brydon HL, Hayward R, Harkness W, Bayston R (1995) Physical properties of cerebrospinalfluid of relevance to shunt function. 2: The effect of protein upon CSF surface tension and con-tact angle. Br J Neurosurg 9: 645-651
26. Brydon HL, Bayston R, Hayward R, Harkness W (1996) The effect of protein on the flow-pressure characteristics of shunts. Neurosurgery 38: 498-505
27. Butler AB, McLone DG (1993) Hydrocephalus. Neurosurg Clin N Am 4: 633-65628. Chiba Y, Yuda K (1980) Thermosensitive determination of CSF shunt patency with a pair of
small disc thermistors. J Neurosurg 52: 700-70429. Choux M, Genitori L, Lang D, Lena G (1992) Shunt implantation: reducing the incidence of
shunt infection. J Neurosurg 77: 875-88030. Cooper JR (1978) Migration of ventriculoperitoneal shunt into the chest. J Neurosurg 48: 146-14731. Cozzens JW, Chandler JP (1997) Increased risk of distal ventriculoperitoneal shunt obstruction
associated with slit valves or distal slits in the peritoneal catheter. J Neurosurg 87: 682-68632. Cutler RW, Page L, Galicich J, Watters GV (1968) Formation and absorption of cerebrospinal
fluid in man. Brain 91: 707-72033. Czosnyka Z, Czosnyka M, Richards HK, Pickard JD (1998) Posture-related overdrainage:
comparison of the performance of 10 hydrocephalus shunts in vitro. Neurosurgery 42: 327-33434. Dandy WE (1918) Ventriculostomy following the injection of air into the cerebral ventricles.
Ann Surg 68:5-1135. Dandy WE (1918) Extirpation of the choroid plexus of the lateral ventricles in communicating
hydrocephalus. Ann Surg 68: 569-57936. Dandy WE (1922) An operative procedure for hydrocephalus. Bull Johns Hopkins Hosp 33:
189-19037. Davidoff LE (1929) Treatment of hydrocephalus. Arch Surg 18:1737-176238. Del Bigio MR (1998) Biological reactions to cerebrospinal fluid shunt devices: a review of
cellular pathology. Neurosurgery: 319-326 39. DiChiro G (1964) Movement of the cerebrospinal fluid in human beings. Nature 204: 290-29140. DiChiro G, Stein SC, Harrington T (1972) Spontaneous cerobrospinal fluid rhinorrhea in nor-
mal dogs. J Neuropath Exp Neurol 31: 447-453
100
41. Di Rocco C, Marchese E, Velardi F (1994) A survey of the first complication of newly implant-ed CSF shunt devices for the treatment of nontumoral hydrocephalus. Child’s Nerv Syst 10:321-327
42. Drake JM, Kulkarni AV (1993) Cerebrospinal fluid infections. Neurosurgery Quarterly 3: 283-29443. Drake JM, Sainte-Rose C (1995) The shuntbook. Blackwell Science, inc. Cambridge,
Massachusets. ISBN 0-86542-220-6.44. Duhaime AC, Bonner K, McGowan KL, Schut L, Sutton LN, Plotkin S (1991). Distribution of
bacteria in the operating room environment and its relation to ventricular shunt infections: aprospective study. Child’s Nerv Syst 7: 211-214
45. Echizenya K, Satoh M, Murai H, Ueno H, Abe H, Komai T (1987). Mineralization and biodeg-redation of CSF shunting systems. J Neurosurg 67: 584-591
46. Eckstein HB (1965) The surgical treatment of hydrocephalus with the Holter valve. Turk JPediatr 7: 12-21
47. El Shafei IL (1975) Ventriculo-venous shunt to the proximal segment of an occluded neckvein. A new method for shunting of CSF to the venous circulation. Surg Neurol 3:237-244
48. El Shafei IL (1985) Ventriculovenous shunt against the direction of blood flow: a new appro-ach for shunting the cerebrospinal fluid to the venous circulation. Child’s nerv Syst 1: 200-207
49. El Shafei IL, El Rifaii MA (1987) Ventriculojugular shunt against the direction of blood flow.I. Role of the internal jugular vein as an antisiphon device. Child’s Nerv Syst 3: 282-284
50. El Shafei IL, El Rifaii MA (1987) Ventriculojugular shunt against the direction of blood flow.II. Theoretical and experimental basis for shunting the cerebrospinal fluid against the directionof blood flow. Child’s Nerv Syst 3: 285-291
51. El Shafei IL (1987) Ventriculojugular shunt against the direction of blood flow. III. Operativetechnique and results. Child’s Nerv Syst 3: 342-349
52. El Shafei, IL, Hafez MA (1987) Technical modifications and policy for treatment. Child’sNerv Syst 7: 197-204.
53. Eisenberg HM, McComb JG, Lorenzo AV (1974) Cerebrospinal fluid overproduction andhydrocephalus associated with choroid plexus papilloma. J Neurosurg 40: 381-385
54. Fischer RG Surgery of the congenital anomalies (1951) In: Walker EA, ed. A history of neuro-logical surgery. Baltimore: Williams & Wilkins 334-347
55. Foltz, EL, Shurtleff, DB (1963) Five year comparitive study of hydrocephalus in children withand without operation (113 cases). J Neurosurg 20: 1064-1078
56. Foltz EL, Blanks J, Meyer R (1994) Hydrocephalus: the zero ICP ventricle shunt (ZIPS) tocontrol gravity shunt flow. Child’s Nerv Syst 10: 43-48
57. Fraser J, and Dott NM (1922-23) Hydrocephalus Br J Surg 10:165-19158. Gardner P, Leipzig T, Phillips P (1985) Infections of cerebral nervous system shunts. Med Clin
of North America 69: 297-31459. Go KG, Lakke JPWF, Beks JWF (1968) A harmless method for the assessment of the patency
of ventriculo-atrial shunts in hydrocephalus. Dev Med Child Neurol 10: 100-10660. Go KG (1991) Cerebral pathophysiology - An integral approach with some emphasis on clini-
cal implications. Elsevier Science Publishers B.V., Amsterdam, The Netherlands. ISBN 0-444-81386-1
61. Gruber R, Jenny P, Herzog B (1984) Experiences with the anti-siphon device (ASD) in shunttherapy of pediatric hydrocephalus. J Neurosurg 61: 156-162
62. Habal MB (1984) The biologic basis for the clinical application of the silicones. A correlate totheir biocompatibility. Arch Surg 119(7): 843-848
63. Haines SJ, Walters BC (1994) Antibiotic profylaxis for cerebrospinal fluid shunts: a metanaly-sis. Neurosurgery 34: 87-92
64. Hakim S, Duran de la Roche F, Burton JD (1973) A critical analysis of valve shunts used in thetreatment of hydrocephalus. Develop Med Child Neurol 15: 230-255
101
65. Hara M, Kadowaki C, Konishi Y, Ogashiwa M, Numoto M, Takeuchi K (1983) A new methodfor measuring cerebrospinal fluid flow in shunts. J Neurosurg 58: 557-561
66. Ho KJ (1992) Recurrent meningitis associated with intragastric migration of a ventriculoperit-oneal shunt catheter in a patient with normal-pressure hydrocephalus. South Med J 85: 1145-1148
67. Jährig K, Steiner B (1973) Die Beziehungen von Viskosität und Eiweißgehalt des Liquor cere-brospinalis. Psychiat Neurol med Psychol Leipzig 25: 290-296
68. Jones RFC, Stening WA, Kwok BCT, Sands TM (1993) Third ventriculostomy for shunt infec-tions in children. Neurosurgery 32: 855-860
69. Kadowaki C, Hara M, Numoto M, Takeuchi K (1987) Factors affecting cerebrospinal fluidflow in a shunt. Br J Neurosurg 1: 467-475.
70. Kalousdian S, Karlan MS, Williams MA for the Council on Scientific Affairs, AmericanMedical Association. (1998) Silicone elastomer cerobrospinal fluid shunt systems.Neurosurgery 42: 887-8925.
71. Kast J, Duong D, Nowzari F, Chadduck WM, Schiff SJ (1994) Time-related patterns of ven-tricular shunt failure. Child’s Nerv Syst 10: 524-528
72. Key A, Retzius G (1876) Studien in der Anatomie des Nervensystems und des Bind-gewebes.Stockholm, Samson and Wallin
73. Kobayashi H, Hayashi M, Kawano Y, et al. (1987) Migration of abdominal catheter of ventric-uloperitoneal shunt into the scrotum. Zentralbl Neurochir 48: 232-234
74. Kushner J, Alexander E Jr., and Davis CH (1971) Kyphoscoliosis following lumbar subarach-noid shunts. J Neurosurg 34: 783-791
75. Kurug A, Treves S, Welch K, Merling D (1984) Radionuclide estimation of cerebrospinal fluidshunt flow. J Neurosurg 60: 361-364
76. Leech RW, Brumback RA (1991) Hydrocephalus Current clinical concepts. Mosby year book,inc. St. Louis, MO. ISBN 0-8151-5555-7
77. Leonhardt S, Bluhm V, Steudel WI (1993) Ein computergestützter Prüfstand für Liquor-Drainagesysteme. Biomed Technik 38:188-195
78. Liptak GS, Masiulis BS, McDonald JV (1985) Ventricular shunt survival in children with neu-ral tube defects. Acta Neurochir 74: 113-117
79. Lund-Johansen M, Svendsen F, Wester K (1994) Shunt failures and complications in adults asrelated to shunt type, diagnosis, and the experience of the surgeon. Neurosurgery 35: 839-844
80. Magnaes B (1976) Body position and cerebrospinal fluid pressure. Part 1: Clinical studies onthe effect of rapid postural changes. J Neurosurg 44: 687-697
81. Magnaes B (1976) Body position and cerebrospinal fluid pressure. Part 2: Clinical studies onorthostatic pressure and the hydrostatic indifferent point. J Neurosurg 44: 698-705
82. Matson DD (1949) New operation for treatment of communicating hydrocephalus: report ofcase secondary to generalized meningitis. J Neurosurg 6: 238-247
83. Matson DD (1956) Current treatment of hydrocephalus. New Engl J Med 255:933-93684. Marmarou A (1973) A theoretical model and experimental evaluation of the cerebrospinal fluid
system. Ph.D. thesis, Drexel University, pp 1-14285. Matsumae M, Murakami T, Ueda M, Suzuki Y (1987) Dynamic Changes of cerebrospinal fluid
shunt in patient’s daily life. Shoni no noshinkei 3: 30-3486. McComb JG (1983) Recent research into the nature of cerebrospinal fluid formation and
absorption. J Neurosurg 59: 369-38387. McCullough JC (1990) History of the treatment of hydrocephalus. In: Scott e.a. ed. in
Neurosurgery 3:1-1088. Metzemaekers JDM, Beks JWF, Van Popta JS (1987) Cerebrospinal fluid shunting for hydro-
cephalus: a retrospective analysis. Acta Neurochir (Wien) 88: 75-7889. Mevorach RA, Hulbert WC, Merguerian PA, Rabinowitz R (1992) Perforation and intravesical
102
erosion of a ventriculoperitoneal shunt in a child with an augmentation cytoplasty. J Urol 147:433-434
90. Milhorat TH, Hammock MK, Davis DA, Fenstermacher JD (1976). Choroid plexus papilloma.I. Proof of cerebrospinal fluid overproduction. Child’s Brain 2 : 273-289
91. Mircevski M, Mircevska D, Basevska R, Stankoviƒ B (1991) Congenital central nervous sys-tem malformations associated with hydrocephalus. In Matsumoto S, Tamaki N (eds)Hydrocephalus. Pathogenesis and treatment. Springer, Berlin Heidelberg New York, pp 533-538
92. Miserocchi G, Sironi VA, Ravagnati L (1984) Anal protrusion as a complication of ventriculo-peritoneal shunt. J Neurosurg Sci 28: 43-46
93. Morell RC, Bell WO, Hertz GE, D’Souza V (1994) Migration of a ventriculoperitoneal shuntinto the pulmonary artery. J Neurosurg Anest 6: 132-134
94. Morisette I, Gourdeau M, Francoeur J (1993) CSF shunt infections: A fifteen year experiencewith emphasis on management and outcome. Can J Neurol Sci 20: 118-122
95. Nulsen FE, Spitz EB (1952) Treatment of hydrocephalus by direct shunt from ventricle to jug-ular vein. Surg Forum 399-403
96. Pappenheimer JR, Heiser SR and Jordan EF (1962) Perfusion of the ventricular system inunanesthetized goats. Am. J. Physiol. 203: 763-774
97. Payr E (1908) Drainage der Hirnventrikel mittelst frei transplantirter Blutgefasse; Bermerkun-gen ueber Hydrocephalus. Arch Klin Chir 87: 801-885
98. Piatt JH Jr., Carlson CV (1993) A search for determinants of cerebrospinal fluid shunt surviv-al: retrospective analysis of a 14-year institutional experience. Pediatr Neurosurg 19: 233-242
99. Pople, IK, Bayston R, Hayward RD (1992) Infection of cerebrospinal fluid shunts in infants: astudy of etiological factors. J Neurosurg 77: 29-36
100. Pudenz RH, Russell FE, Hurd AH, Sheldon CH. (1957) Ventriculo-auriculostomy. A techniquefor shunting cerebrospinal fluid into the right auricle. J Neurosurg 14:171-179
101. Pudenz RH (1981) The surgical treatment of hydrocephalus - An historical review. Surg neurol15: 15-26
102. Pudenz RH (1992) CSF-protein study: medical education series pamphlet. Goleta, PS medicalCorporation.
103. Putnam TJ (1943) The surgical treatment of infantile hydrocephalus. Surg Gynecol Obstet76:171-182
104. Quincke H (1891) Ueber Hydrocephalus. Verh Congr inn Med 10:321-339105. Rayport M, Reiss J (1969) Hydrodynamic properties of certain shunt assemblies for the treat-
ment of hydrocephalus. Part 1: Report of a case of communicating hydrocephalus with incre-ased cerebrospinal fluid production treated by duplication of shunting device. Part 2: Pressure-flow characteristics of the Spitz-Holter, Pudenz-Heyer, and Cordis Hakim shunt systems. JNeurosurg 30: 455-467
106. Rekate (personal communication, 1998)107. Rubin RC, Henderson ES, Ommaya AK, Walker MD, Rall DP (1966) The production of cere-
brospinal fluid in man and its modification by acetazolamide. J Neurosurg 25: 430-436 108. Sahar A (1972) Choroidal origin of cerebrospinal fluid. Is J Med Sci 81: 594-6 109. Sainte-Rose C, Piatt jH, Renier D, Pierre-Kahn A, Hirsch jF, Hoffman HJ, Humphreys RP,
Hendrick EB (1991-92) Mechanical complications in shunts. Pediatr Neurosurg 17: 2-9110. Sainte-Rose C (1993) Shunt obstruction: a preventable complication? Pediatr Neurosurg 19:
156-164111. Scarff JE (1963) Treatment of hydrocephalus: an historical and critical review of methods and
results. J Neurol Neurosurg Psychiatr 26:1-26112. Schierholz JM, Pulverer G (1997) Development of a new CSF-shunt with sustained release of
an antimicrobial broad-spectrum combination. Zentralbl.Bakteriol 286: 107-123
103
113. Schoener WF, Verheggen R, Reparon C, Markakis E (1991) Evaluation of shunt failures bycompliance analysis and inspection of shunt valves and shunt materials, using microscopic orscanning electron microscopic techniques. In: Matsumoto, S., Tamaki, N (eds) Hydrocephalus.Pathogenesis and treatment. Springer, Berlin Heidelberg New York, pp 452-472.
114. Schubert W, Prater C (1979) Zum Einfluß von eiweißhaltigem Liquor auf ventrikulo-aurikulä-re Drainagen. Z Exper Chirurg 12: 379-382
115. Schulte C, Aschoff A, Hashemi B, Fruh K, Kunze S (1996) Seven Orbis-Sigma valves in ultralong-term tests. Child’s Nerv Syst 12: 494
116. Scott RM (1990) Preventing and treating shunt complications. In: Scott, R.M. (ed):Hydrocephalus. Baltimore, Williams and Wilkins, p. 115-121
117. Sikkens TB (1957) Traitement de l’hydrocéphalie du nourrison par ventriculo-jugulostomie.Neurochirurgie 3:65-69
118. Snow RB, Lavyne MH, Fraser RAR (1986) Colonic perforation by ventriculoperitonealshunts. Surg Neurol 25: 173-177
119. Steinke JH (1968) Funktionstechnik und Komplicationsursachen bei ventrikulo-atrialenShunts. Z Neurochir 29: 203-215
120. Tokoro K, Chiba Y, Abe H, Tanaka N, Yamataki A, Kanno H (1994). Importance of anti-siphondevices in the treatment of pediatric hydrocephalus. Child’s Nerv Syst 10: 236-238
121. Torack RM (1982) Historical aspects of normal and abnormal brain fluids. II. Hydrocephalus.Arch Neurol 39: 276-279
122. Torkildsen A (1929) A new pallitive operation in cases of inoperable occlusion of the sylvianaqueduct. Acta Chir Scand 82:117-124
123. Trost HA (1991) Testing the hydrocephalus shunt valve: long term bench test results of variousnew and implanted hydrocephalus shunt valves. The need for a model for testing shunt valvesunder physiological conditions. Eur J Pediatr Surg 1 (suppl. 1): 38-40
124. Trost HA (1995) Is there a reasonable differential indication for different hydrocephalus shuntsystems? Child’s Nerv Syst 11 (4): 189-192
125. Vandertop WP, Verdaasdonk RM, Van Swol CFP (1998) Laser-assisted neuroendoscopy usinga neodymium-yttrium aluminium garnet or diode contact laser with pretreated fiber tips. JNeurosurg 88: 82-92
126. Van der Veen PH (1972) Hydrodynamics of Holter ventriculo-atrial shunt systems under vari-ous conditions. Dev Med Child Neurol 14, supp.27: 132-139
127. Voormolen JC, Brand R (1996) Enquete hydrocephalus. Voordracht voor de Themadag van deNederlandse Vereniging van Neurochirurgen, 26 april, Veldhoven.
128. Wallman LJ (1982) Shunting for hydrocephalus: an oral history. Neurosurg 11: 308-313129. Walters BC, Hoffman HJ, Hendrick EB, Humphreys RP (1984) Cerebrospinal fluid shunt
infection. Influences on initial management and outcome. J Neurosurg 20: 1064-1078130. Woolam DHM (1957) The historical significance of cerebrospinal fluid. Med His 1: 91131. Yamasaki S, Osaka K, Hirayama A, (1978) Thermographic determination of cerebrospinal
fluid shunt patency with Chameleon Print. Neurol Surg 6: 253-257
104
Nawoord
Veel mensen hebben bijgedragen aan het tot stand komen van dit proefschrift. Mijn promotoren Jan Jakob Mooij, Jan Beks en Gwan Go dank ik voor hun vlotte correc-ties en goede adviezen. Daarnaast zijn jullie, ieder op een geheel eigen manier, ergbelangrijk geweest voor mijn vorming tot neurochirurg. Mijn referent Louis Journée dank ik voor zijn nauwgezette begeleiding van het laborato-riumonderzoek. Toen we met Joop van de Meer aan het experimenteren waren met eensoort ‘rad van fortuin’ kon ik niet vermoeden dat het onderzoek uiteindelijk deze vormzou krijgen.De twee belangrijkste steunpilaren van dit onderzoek zijn Wim Kaan en Wendy Keldergeweest. Wim, werkzaam bij de Technische Dienst afdeling Ontwikkeling, was echt de“vader” van de testopstelling. Jouw inzet en creativiteit en de hulp van Eric Schenkel hebik zeer gewaardeerd. Wendy, jij hebt mij enorm geholpen bij de verwerking van de onder-zoeksgegevens. Naast zakelijk overleg was het altijd prettig kletsen over het medischbedrijf en jouw aanstaande co-schappen. Je wordt vast een uitstekende dokter.Michiel Staal en Berry Middel, methodoloog verbonden aan het Noordelijk Centrumvoor Gezondheidsvraagstukken, waren de mannen van het eerste uur. Michiel dank ikvoor zijn initiatieven bij het opzetten van deze studie en Berry voor het methodologischstroomlijnen van onze ideeën. Henk Bosveld, methodoloog verbonden aan het Huisartseninstituut, dank ik voor de hulpbij het analyseren van de klinische onderzoeksgegevens. Naast het AZG hebben de volgende neurochirurgische centra geparticipeerd in het klini-sche onderzoek: AMC, AZL, AZN, AZR, AZU, AZVU en Sophia Zwolle (Dick Zeilstra).Ik dank de collega’s van deze centra voor hun hulp. Zonder jullie (belangeloze) inzet, washet multi-centre onderzoek niet mogelijk geweest. Mahé Hilbrands, Liesbeth Broers en Antje Wagenaar hebben mij uitstekend geholpen bijverschillende administratieve zaken. Daarnaast zorgen jullie voor een gezellige sfeer ophet secretariaat bij een kop echte koffie.Naast de nog niet genoemde collega’s, Cees ter Weeme en Eelco Hoving, dank ik allemensen die betrokken zijn bij de behandeling van de neurochirurgische patiënten, vooralvoor de goede sfeer waarin het werk gedaan wordt.Anne Rupert dank ik voor haar correcties van de Engelse taal.Voor het beoordelen van het manuscript ben ik Prof. dr. D.A. Bosch, Prof. dr. J.H.A. DeKeyser en Prof. dr. R.P. Zwierstra zeer erkentelijk.
105
Voor hun inspanningen als paranimf dank ik mijn lieve zus Monique Metzemaekers enmijn goede vriend en collega Maarten Coppes.Mijn ouders dank ik in het bijzonder voor de mogelijkheid die ze mij geboden hebbenmijn geneeskunde studie in België aan te vangen. Lieve Ma, we zullen Pa bij deze gele-genheid enorm missen. Lieve Matthijs, Thomas en Rosalie, nu de ‘promovatie’ achter de rug is, zorgen jullie vastweer voor nieuwe actie.Mijn liefste Jessica, jij bent de motor van ons gezin en van mijn leven.
106

Curriculum Vitae
De schrijver van dit proefschrift werd geboren op 14 november 1957 te Breda. In 1976behaalde hij het Atheneum-B diploma aan het St. Pauluslyceum te Tilburg. In de jaren1977 - 1978 studeerde hij achtereenvolgens economie en rechten aan de KatholiekeHogeschool Tilburg. Van 1978 tot 1981 studeerde hij geneeskunde aan de Rijksuniver-siteit Gent (België), afgesloten met het kandidaatsdiploma. In 1984 werd het arts-examensuccesvol afgelegd aan de Erasmusuniversiteit te Rotterdam. Aansluitend was hij werk-zaam als arts-assistent neurologie in het Dijkzigtziekenhuis te Rotterdam (Prof. Dr. A.Staal). Vanaf 1985 was hij arts-assistent neurochirurgie in het Academisch ZiekenhuisGroningen alwaar in 1992 de opleiding tot neurochirurg kon worden afgerond (opleider:Prof. Dr. J.W.F. Beks). De opleidingsperiode bevatte één stage-jaar neurologie in hetAcademisch Ziekenhuis Groningen (Prof. Dr. H.J.G.H. Oosterhuis) en één jaar algemeneheelkunde in het Rooms Katholiek Ziekenhuis Groningen (Dr. L.J.M. Vos). Sinds 1992 ishij als neurochirurg verbonden aan het Academisch Ziekenhuis Groningen, vanaf 1993 inde functie van Chef de Clinique.
107
Stellingenbehorende bij het proefschrift
Hydrocephalus shuntsa clinical and laboratory study
1. De ideale hydrocefalieshunt bestaat niet.
2. Een ‘hoge’ eiwitconcentratie in de liquor cerebrospinalis (tot 10g/l) is nietvan invloed op het functioneren van een hydrocefalieklep.
3. Hoewel de werking van veel hydrocefaliekleppen al duidelijk verandert bijeen laag aantal erythrocyten, is toch onderzoek van de liquor cerebrospinalismet alleen het blote oog voldoende betrouwbaar om te beoordelen of hetplaatsen van een shunt verantwoord is.
4. Bij prospectief onderzoek naar de chirurgische behandeling van hydrocefalie-patiënten is niet alleen het complicatiepercentage van belang, ook de beoor-deling van de kwaliteit van leven is een belangrijke parameter bij de evaluatievan het behandelingsresultaat.
5. Hoewel het terugdringen van wachtlijsten in de gezondheidszorg een goedezaak is, blijft de stelling: ‘een goede therapie voor de hernia nuclei proposi isde wachtlijst’ nog steeds verdedigbaar.
6. De magnetische resonantie angiografie kan bij veel neurochirurgische patiëntende conventionele angiografie vervangen.
7. Het C-2000 en de C-1000 verschillen numeriek een factor twee en komenovereen in het streven zoveel mogelijk te willen bieden voor zo min moge-lijk geld.
8. De voorkeursbehandeling in de acute fase van patiënten in goede klinische toe-stand na een subarchnoïdale bloeding uit een moeilijk te opereren aneurysmabestaat uit coiling.
9. De kwaliteit van het voetbalspel van FC Groningen heeft al enige tijd geenaanleiding gegeven tot feest in het Oosterparkstadion; deze promotie wel.
10. De prognose van patiënten met een glioblastoma multiforma lijkt vooralsnogniet te verbeteren na gentherapie met een suicide-gen.
Groningen, 30 september 1998Jan D.M. Metzemaekers