Embed Size (px)
Citation preview
University of ZurichZurich Open Repository and Archive
Winterthurerstr. 190
CH-8057 Zurich
http://www.zora.uzh.ch
Year: 2008
Ophthalmic diagnostic & therapeutic guidelines for theveterinary practitioner. Part 1
Spiess, B M
Spiess, B M (2008). Ophthalmic diagnostic & therapeutic guidelines for the veterinary practitioner. Part 1.VETMED, 21(3):7-9.Postprint available at:http://www.zora.uzh.ch
Posted at the Zurich Open Repository and Archive, University of Zurich.http://www.zora.uzh.ch
Originally published at:VETMED 2008, 21(3):7-9.
Spiess, B M (2008). Ophthalmic diagnostic & therapeutic guidelines for the veterinary practitioner. Part 1.VETMED, 21(3):7-9.Postprint available at:http://www.zora.uzh.ch
Posted at the Zurich Open Repository and Archive, University of Zurich.http://www.zora.uzh.ch
Originally published at:VETMED 2008, 21(3):7-9.
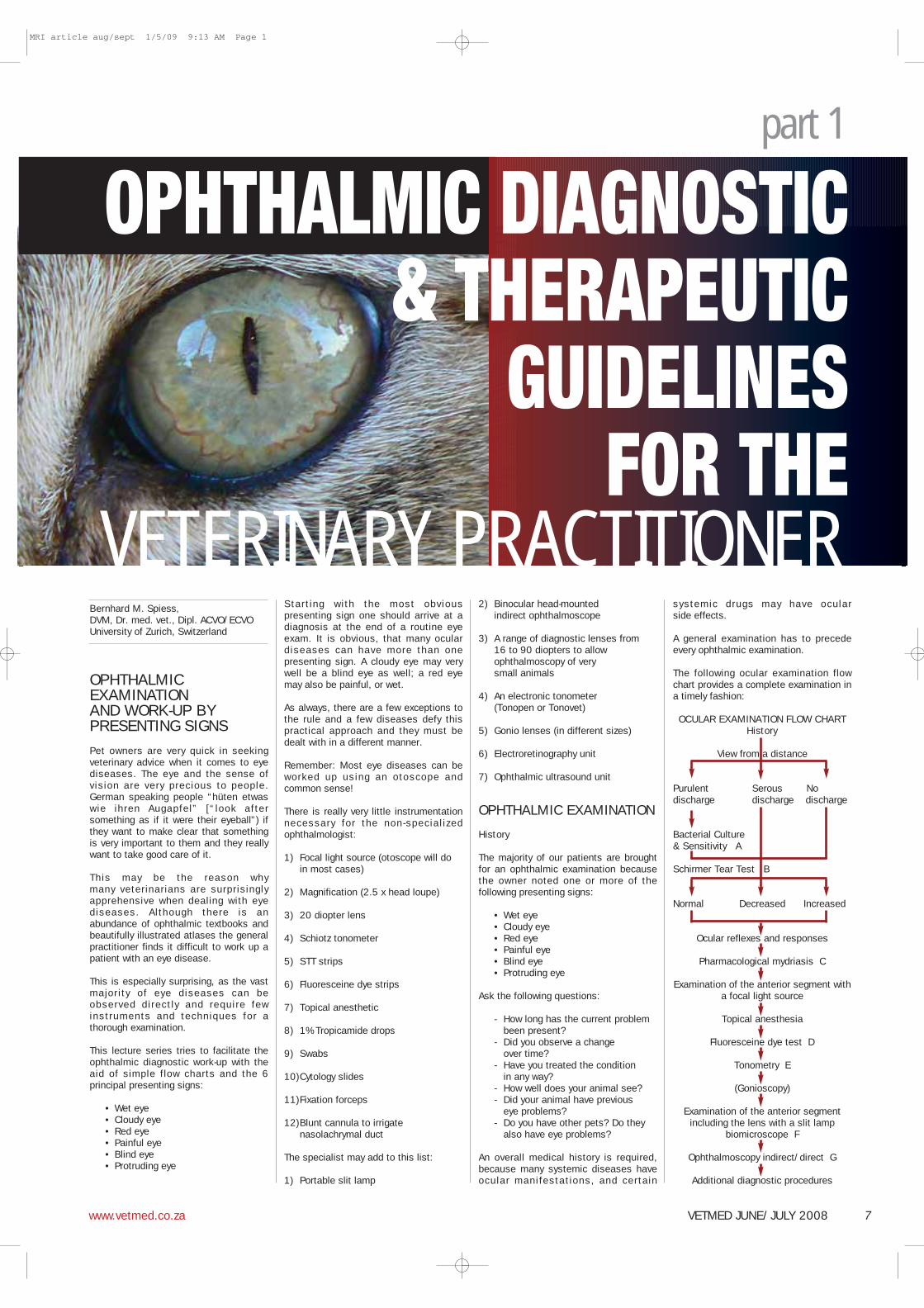
Bernhard M. Spiess,DVM, Dr. med. vet., Dipl. ACVO/ECVOUniversity of Zurich, Switzerland
OPHTHALMICEXAMINATIONAND WORK-UP BYPRESENTING SIGNS
Pet owners are very quick in seekingveterinary advice when it comes to eyediseases. The eye and the sense ofvision are very precious to people.German speaking people “hüten etwaswie ihren Augapfel” [“look aftersomething as if it were their eyeball”) ifthey want to make clear that somethingis very important to them and they reallywant to take good care of it.
This may be the reason whymany veterinarians are surprisinglyapprehensive when dealing with eyediseases. Although there is anabundance of ophthalmic textbooks andbeautifully illustrated atlases the generalpractitioner finds it difficult to work up apatient with an eye disease.
This is especially surprising, as the vastmajority of eye diseases can beobserved directly and require fewinstruments and techniques for athorough examination.
This lecture series tries to facilitate theophthalmic diagnostic work-up with theaid of simple flow charts and the 6principal presenting signs:
• Wet eye• Cloudy eye• Red eye• Painful eye• Blind eye• Protruding eye
Starting with the most obviouspresenting sign one should arrive at adiagnosis at the end of a routine eyeexam. It is obvious, that many oculardiseases can have more than onepresenting sign. A cloudy eye may verywell be a blind eye as well; a red eyemay also be painful, or wet.
As always, there are a few exceptions tothe rule and a few diseases defy thispractical approach and they must bedealt with in a different manner.
Remember: Most eye diseases can beworked up using an otoscope andcommon sense!
There is really very little instrumentationnecessary for the non-special izedophthalmologist:
1) Focal light source (otoscope will do in most cases)
2) Magnification (2.5 x head loupe)
3) 20 diopter lens
4) Schiotz tonometer
5) STT strips
6) Fluoresceine dye strips
7) Topical anesthetic
8) 1% Tropicamide drops
9) Swabs
10)Cytology slides
11)Fixation forceps
12)Blunt cannula to irrigate nasolachrymal duct
The specialist may add to this list:
1) Portable slit lamp
2) Binocular head-mounted indirect ophthalmoscope
3) A range of diagnostic lenses from 16 to 90 diopters to allow ophthalmoscopy of very small animals
4) An electronic tonometer (Tonopen or Tonovet)
5) Gonio lenses (in different sizes)
6) Electroretinography unit
7) Ophthalmic ultrasound unit
OPHTHALMIC EXAMINATION
History
The majority of our patients are broughtfor an ophthalmic examination becausethe owner noted one or more of thefollowing presenting signs:
• Wet eye• Cloudy eye• Red eye• Painful eye• Blind eye• Protruding eye
Ask the following questions:
- How long has the current problem been present?
- Did you observe a change over time?
- Have you treated the condition in any way?
- How well does your animal see?- Did your animal have previous
eye problems?- Do you have other pets? Do they
also have eye problems?
An overall medical history is required,because many systemic diseases haveocular manifestations, and certain
systemic drugs may have ocularside effects.
A general examination has to precedeevery ophthalmic examination.
The following ocular examination flowchart provides a complete examination ina timely fashion:
OCULAR EXAMINATION FLOW CHARTHistory
View from a distance
Purulent Serous Nodischarge discharge discharge
Bacterial Culture & Sensitivity A
Schirmer Tear Test B
Normal Decreased Increased
Ocular reflexes and responses
Pharmacological mydriasis C
Examination of the anterior segment witha focal light source
Topical anesthesia
Fluoresceine dye test D
Tonometry E
(Gonioscopy)
Examination of the anterior segmentincluding the lens with a slit lamp
biomicroscope F
Ophthalmoscopy indirect/direct G
Additional diagnostic procedures
VETERINARY PRACTITIONER
part 1
OPHTHALMIC DIAGNOSTIC& THERAPEUTIC
GUIDELINESFOR THE
VETMED JUNE/JULY 2008www.vetmed.co.za 7
MRI article aug/sept 1/5/09 9:13 AM Page 1
A: Sampling the eye for bacterial cultureand sensitivity testing has to be doneprior to the instillation of topical anesthesia or mydriatics because these drops contain preservatives which may inhibit bacterial growth in vitro. This does not apply for preservative-free single dose units.
B: The STT has to be performed before any manipulation of the eye and priorto instillation of drops of any kind.
C: Applying tropicamide at this point safes a lot of time. During the 15 to 20 minutes it usually takes for the pupils to dilate, the next steps of examination can be taken.
D: The fluoresceine dye test is done before tonometry, because in the presence of a corneal erosion or ulcer one may choose not to measure IOP with a Schiotz tonometer.
E: Tonometry* can be performed at thispoint. Usually, the pupil is not dilatedenough at this time to possible alter (increase) IOP.
F: The pupil should be dilated enough atthis point to allow examination of theentire lens and the fundus.
G: Indirect (and direct) ophthalmoscopy concludes the ocular examination
One hardly misses any important diagnosis if one follows these rules:
1. Perform tonometry in any red eye!
2. Stain any painful eye with fluoresceine!
3. Do a STT on any eye with chronic purulent discharge!
*Tonometry
There are three basic methods todetermine IOP. Although digitaltonometry (comparative palpation ofthe globes) may give an impressionabout the tension of the globes, forexact measurements a tonometer has tobe used.
Schiotz TonometryThe Schiotz tonometer has greatadvantages, as it is cheap, robust andrelatively easy to use in most dogs andcats. The eyes have to be anesthetizedwith oxybuprocaine or tetracaine. Theanimal’s head has to be positioned toallow perpendicular placement of theinstrument on the cornea. The unitsindicated by the instrument have to beconverted into mm Hg using aconversion table.
The basic weight of 5.5 gr is usuallyused. If the instrument indicates lessthan 3 scale units, an additional weight(7.5 gr or 10 gr) has to be added.Decentration of the footplate is toleratedas long as the plunger rests on thecornea. The curvature of the footplatefits the human cornea and isapproximately correct for canine andfeline corneas as well.
In small eyes with a steeper curvature,IOP is over-estimated, whereas in largeeyes with flatter corneas IOP is under-estimated. Normal IOP in dogs and catsis between 6 scale units (14.6 mmHg)and 3 scale units (24.4 mm Hg.
Applanation tonometry The new electronic applanationtonometers (Tonopen) al lowmeasurements of IOP in a variety ofanimals including horses, becausethey function independent of the positionof the instrument or the eye. They alsorequire topical anesthesia. The corneais f lattened (applanation) over adefined small area and the forcenecessary for the applanation isconverted in mm Hg. The tip of thetonometer is touching the center of thecornea several times, until an acousticsignal indicates that the instruments hascalculated an average IOP.
Rebound tonometryA recent development is the reboundtonometer (Tonovet) in which a small pinis launched to contact the cornea. Thetip rebounds in relation to the IOP. Thisinstrument is extremely well tolerated byall animals and doesn’t require topicalanesthesia. It has been calibrated forhumans, dogs (and cats), and horses.
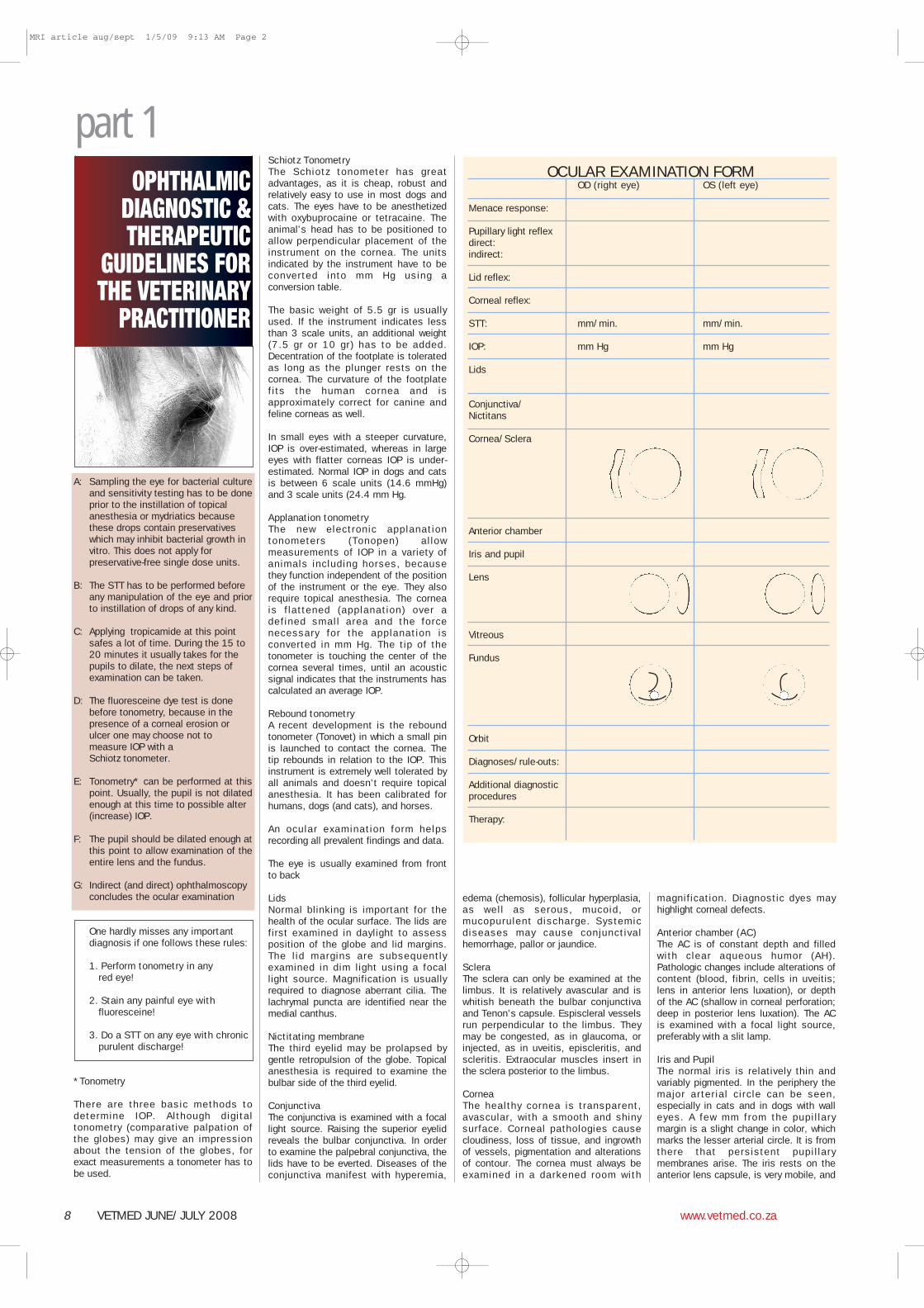
An ocular examination form helpsrecording all prevalent findings and data.
The eye is usually examined from frontto back
LidsNormal blinking is important for thehealth of the ocular surface. The lids arefirst examined in daylight to assessposition of the globe and lid margins.The l id margins are subsequentlyexamined in dim light using a focallight source. Magnification is usuallyrequired to diagnose aberrant cilia. Thelachrymal puncta are identified near themedial canthus.
Nictitating membraneThe third eyelid may be prolapsed bygentle retropulsion of the globe. Topicalanesthesia is required to examine thebulbar side of the third eyelid.
ConjunctivaThe conjunctiva is examined with a focallight source. Raising the superior eyelidreveals the bulbar conjunctiva. In orderto examine the palpebral conjunctiva, thelids have to be everted. Diseases of theconjunctiva manifest with hyperemia,
edema (chemosis), follicular hyperplasia,as well as serous, mucoid, ormucopurulent discharge. Systemicdiseases may cause conjunctivalhemorrhage, pallor or jaundice.
ScleraThe sclera can only be examined at thelimbus. It is relatively avascular and iswhitish beneath the bulbar conjunctivaand Tenon’s capsule. Espiscleral vesselsrun perpendicular to the limbus. Theymay be congested, as in glaucoma, orinjected, as in uveitis, episcleritis, andscleritis. Extraocular muscles insert inthe sclera posterior to the limbus.
CorneaThe healthy cornea is transparent,avascular, with a smooth and shinysurface. Corneal pathologies causecloudiness, loss of tissue, and ingrowthof vessels, pigmentation and alterationsof contour. The cornea must always beexamined in a darkened room with
magnification. Diagnostic dyes mayhighlight corneal defects.
Anterior chamber (AC)The AC is of constant depth and filledwith clear aqueous humor (AH).Pathologic changes include alterations ofcontent (blood, fibrin, cells in uveitis;lens in anterior lens luxation), or depthof the AC (shallow in corneal perforation;deep in posterior lens luxation). The ACis examined with a focal light source,preferably with a slit lamp.
Iris and PupilThe normal iris is relatively thin andvariably pigmented. In the periphery themajor arterial circle can be seen,especially in cats and in dogs with walleyes. A few mm from the pupil larymargin is a slight change in color, whichmarks the lesser arterial circle. It is fromthere that persistent pupil larymembranes arise. The iris rests on theanterior lens capsule, is very mobile, and
OPHTHALMICDIAGNOSTIC &THERAPEUTIC
GUIDELINES FORTHE VETERINARY
PRACTITIONER
OCULAR EXAMINATION FORMOD (right eye) OS (left eye)
Menace response:
Pupillary light reflexdirect:indirect:
Lid reflex:
Corneal reflex:
STT: mm/min. mm/min.
IOP: mm Hg mm Hg
Lids
Conjunctiva/Nictitans
Cornea/Sclera
Anterior chamber
Iris and pupil
Lens
Vitreous
Fundus
Orbit
Diagnoses/rule-outs:
Additional diagnostic procedures
Therapy:
8 VETMED JUNE/JULY 2008 www.vetmed.co.za
part 1
MRI article aug/sept 1/5/09 9:13 AM Page 2
the pupil di lates and constricts inresponse to light. The shape of the pupilis species-dependent. Pathologicalterations include abnormal shape, sizeand motility of the pupil, as well analtered color, location and texture ofthe iris.
LensThe lens can only be examined with thepupil dilated. View from a distancethrough a direct ophthalmoscope anyopacity of the lens (or the cornea) isseen as a black defect. With a slitlamp, opacities of the lens can belocalized and the position of the lens canbe assessed.
Vitreous With focal l ight sources andophthalmoscopes the healthy vitreous isabsolutely clear and transparent. Anyopacity, hemorrhage, floaters or otherinclusion suggest inflammation of theposterior segment.
FundusTo examine the fundus, an indirect ordirect ophthalmoscope is necessary. Fora good overview of the fundus, theindirect ophthalmoscope is best suited.It is best performed with a binocularophthalmoscope, but a bright focal lightsource and a 20-diopter lens are oftensufficient with some practice.
Additional diagnostic procedures include
• Cytology
• Examination/catheterization of the nasolacrimal duct
• Gonioscopy
• Electroretinography
• Ultrasonography
• CT scans, MRI
With the exception of corneal andconjunctival cytology and nasolachrymalflush, these diagnostic proceduresusually require referral to a specialist.
CytologyBrush cytology is easily performed andusually yields a large number of cells forinterpretation without causing unduedamage to the ocular surface.
Examination of the nasolacrimal ductAfter identification of the lachrymalpuncta, fluoresceine dye is applied andis al lowed to drain through thenasolachrymal duct. Dye exiting from thenostril after a few minutes proves theduct to be patent. Failure of the dye toexit the nostril, on the other hand, doesnot prove that the duct is blocked.Cannulation and irrigation of the ductmay demonstrate patency or blockage ofthe duct or one of the ductules.
GonioscopyWith a diagnostic contact lens (goniolens) the width of the drainage angle andthe structure of the pectinate ligamentcan be examined. Gonioscopy helps indiagnosing primary versus secondaryglaucoma and gives some indicationregarding prognosis. Gonioscopy isusually performed in the (healthy)fellow eye.
ElectroretinographyElectroretinography (ERG) examines thefunction of the retina. It is usually done
in the presence of opaque media, suchas cloudy cornea or lens. The mostcommon indication for ERG is prior toplanned cataract surgery. It is also usedto distinguish between ocular forms ofbl indness (PRA, SARD, etc.) fromretrobulbar forms of blindness (opticneuritis, central blindness)
UltrasonographyThe eye being a fluid filled sphere at thesurface of the body is exquisitely suitedfor ultrasonography (US). Indications ofB-scan US are the inability to examineintraocular structures because of cornealopacities, anterior chamber opacities,cataracts, and presumed intraocularneoplasia. In addition, US facilitates thediagnosis of orbital diseases. For theexamination of the orbit a 7.5 MHz probeis usually sufficient. US of the globe isdone with a 10 or 12 MHz probe.Ultrasound biomicroscopy is possiblewith >20 MHz probes.
CT scans, MRITomography and resonance imagingare used to diagnose orbital andCNS diseases.
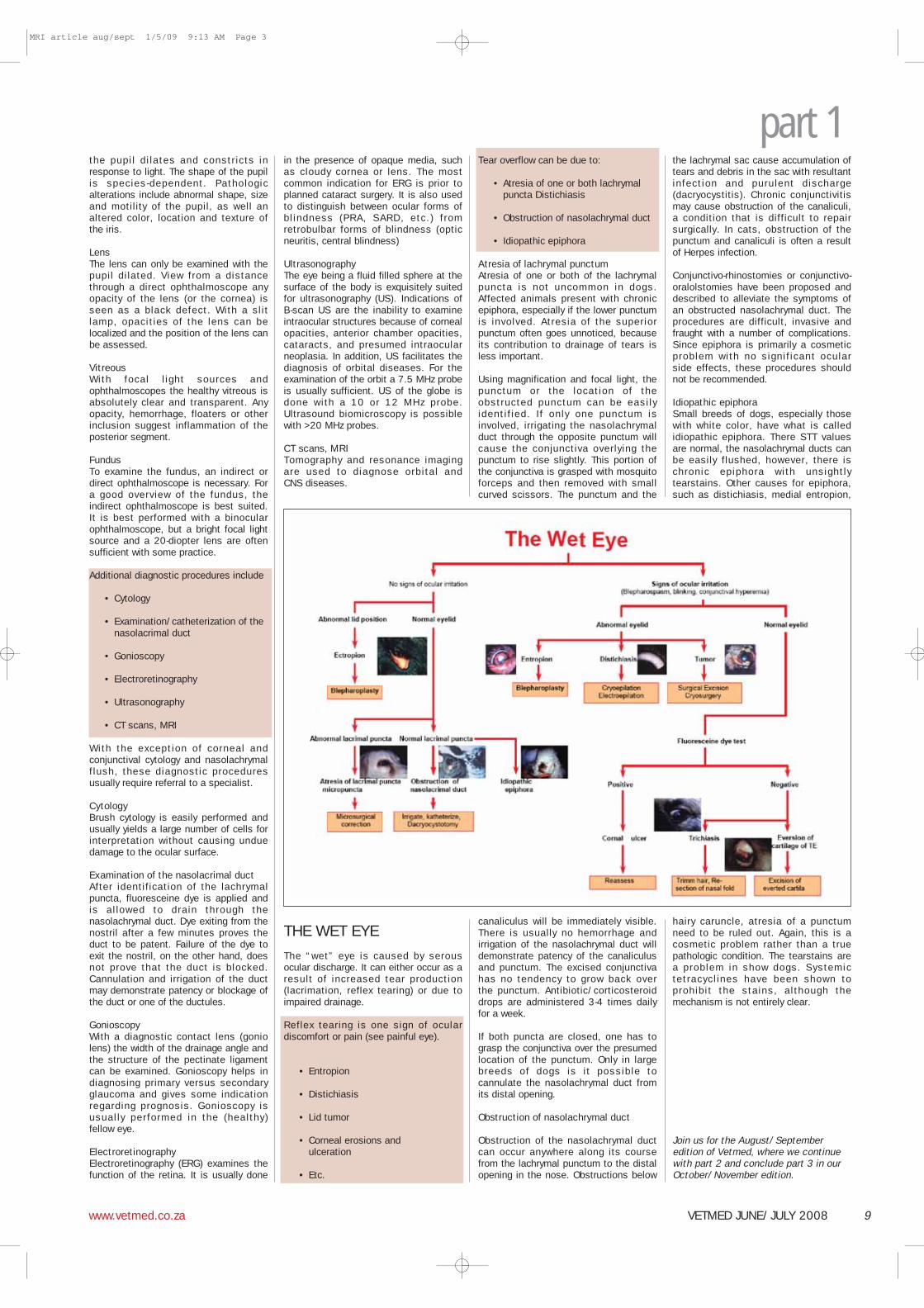
THE WET EYE
The “wet” eye is caused by serousocular discharge. It can either occur as aresult of increased tear production(lacrimation, reflex tearing) or due toimpaired drainage.
Reflex tearing is one sign of oculardiscomfort or pain (see painful eye).
• Entropion
• Distichiasis
• Lid tumor
• Corneal erosions and ulceration
• Etc.
Tear overflow can be due to:
• Atresia of one or both lachrymal puncta Distichiasis
• Obstruction of nasolachrymal duct
• Idiopathic epiphora
Atresia of lachrymal punctumAtresia of one or both of the lachrymalpuncta is not uncommon in dogs.Affected animals present with chronicepiphora, especially if the lower punctumis involved. Atresia of the superiorpunctum often goes unnoticed, becauseits contribution to drainage of tears isless important.
Using magnification and focal light, thepunctum or the location of theobstructed punctum can be easilyidentif ied. If only one punctum isinvolved, irrigating the nasolachrymalduct through the opposite punctum willcause the conjunctiva overlying thepunctum to rise slightly. This portion ofthe conjunctiva is grasped with mosquitoforceps and then removed with smallcurved scissors. The punctum and the
canaliculus will be immediately visible.There is usually no hemorrhage andirrigation of the nasolachrymal duct willdemonstrate patency of the canaliculusand punctum. The excised conjunctivahas no tendency to grow back overthe punctum. Antibiotic/corticosteroiddrops are administered 3-4 times dailyfor a week.
If both puncta are closed, one has tograsp the conjunctiva over the presumedlocation of the punctum. Only in largebreeds of dogs is it possible tocannulate the nasolachrymal duct fromits distal opening.
Obstruction of nasolachrymal duct
Obstruction of the nasolachrymal ductcan occur anywhere along its coursefrom the lachrymal punctum to the distalopening in the nose. Obstructions below
the lachrymal sac cause accumulation oftears and debris in the sac with resultantinfection and purulent discharge(dacryocystitis). Chronic conjunctivitismay cause obstruction of the canaliculi,a condition that is difficult to repairsurgically. In cats, obstruction of thepunctum and canaliculi is often a resultof Herpes infection.
Conjunctivo-rhinostomies or conjunctivo-oralolstomies have been proposed anddescribed to alleviate the symptoms ofan obstructed nasolachrymal duct. Theprocedures are difficult, invasive andfraught with a number of complications.Since epiphora is primarily a cosmeticproblem with no signif icant ocularside effects, these procedures shouldnot be recommended.
Idiopathic epiphoraSmall breeds of dogs, especially thosewith white color, have what is calledidiopathic epiphora. There STT valuesare normal, the nasolachrymal ducts canbe easily flushed, however, there ischronic epiphora with unsightlytearstains. Other causes for epiphora,such as distichiasis, medial entropion,
hairy caruncle, atresia of a punctumneed to be ruled out. Again, this is acosmetic problem rather than a truepathologic condition. The tearstains area problem in show dogs. Systemictetracycl ines have been shown toprohibit the stains, although themechanism is not entirely clear.
Join us for the August/Septemberedition of Vetmed, where we continuewith part 2 and conclude part 3 in ourOctober/November edition.
VETMED JUNE/JULY 2008www.vetmed.co.za 9
part 1
MRI article aug/sept 1/5/09 9:13 AM Page 3