Embed Size (px)
Citation preview
UPJ ObstructionUPJ Obstruction
Zarine BalsaraZarine Balsara
HMS IVHMS IV
September 17, 2007September 17, 2007
CC: Left flank pain
HPI: 32 yoM
who presented to the BIDMC Emergency Department with acute, colicky left flank pain
with nausea and vomiting. Pain has
actually been long-standing and is exacerbated with large fluid intake.
PMH/PSH: none
Meds: none
ALL: none
Patient presentation
Patient presentation (cont.)
FH: non-contributory
SH: Bar owner; 2-4 alcoholic drinks/day
PE: AVSS in NADsignificant for left-sided palpable abdominal mass
Labs:BUN 15, Cr 1.0U/A: Neg
for LE and nitrite; occ
bacteria
5 RBC/hpf, 2 WBC/hpf

UrolithiasisUrolithiasis
HydronephrosisHydronephrosis
Benign tumor/cyst vs malignant tumor Benign tumor/cyst vs malignant tumor
PyelonephritisPyelonephritis/Renal abscess/Renal abscess
Renal infarctionRenal infarction
HematomaHematoma
Clinical differential diagnosis
UrolithiasisUrolithiasis
HydronephrosisHydronephrosis
Benign tumor/cyst vs malignant tumor Benign tumor/cyst vs malignant tumor
PyelonephritisPyelonephritis/Renal abscess/Renal abscess
Renal infarctionRenal infarction
HematomaHematoma
Clinical differential diagnosis
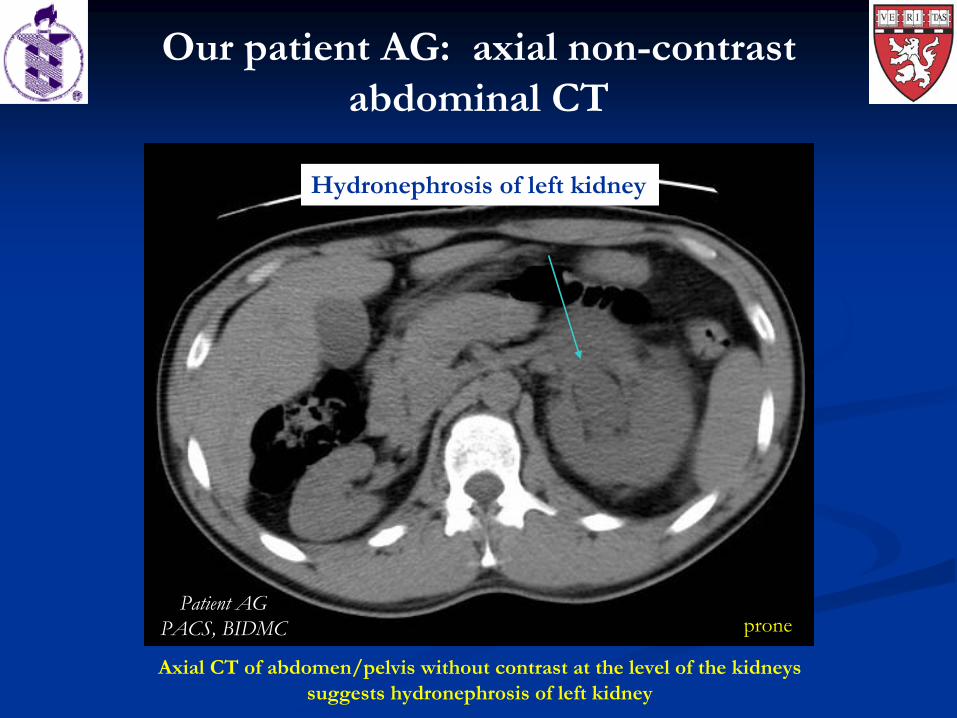
Our patient AG: axial non-contrast abdominal CT
Patient AGPACS, BIDMC
Axial CT of abdomen/pelvis without contrast at the level of the kidneys suggests hydronephrosis
of left kidney
prone
Hydronephrosis
of left kidney
Hydronephrosis
of left kidney
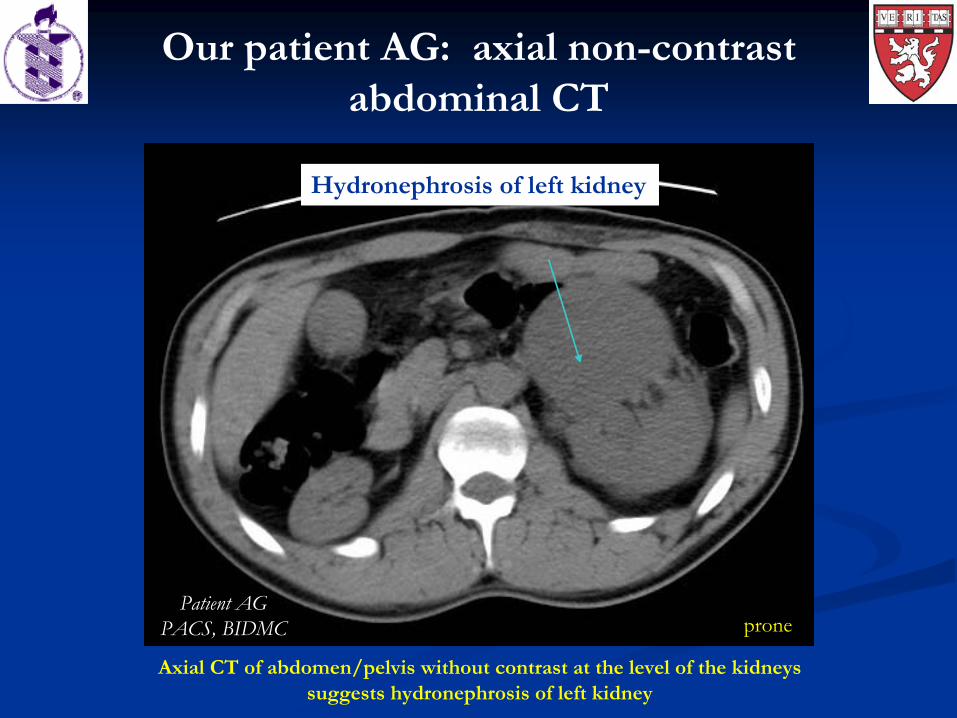
Our patient AG: axial non-contrast abdominal CT
Patient AGPACS, BIDMC prone
Axial CT of abdomen/pelvis without contrast at the level of the kidneys suggests hydronephrosis
of left kidney
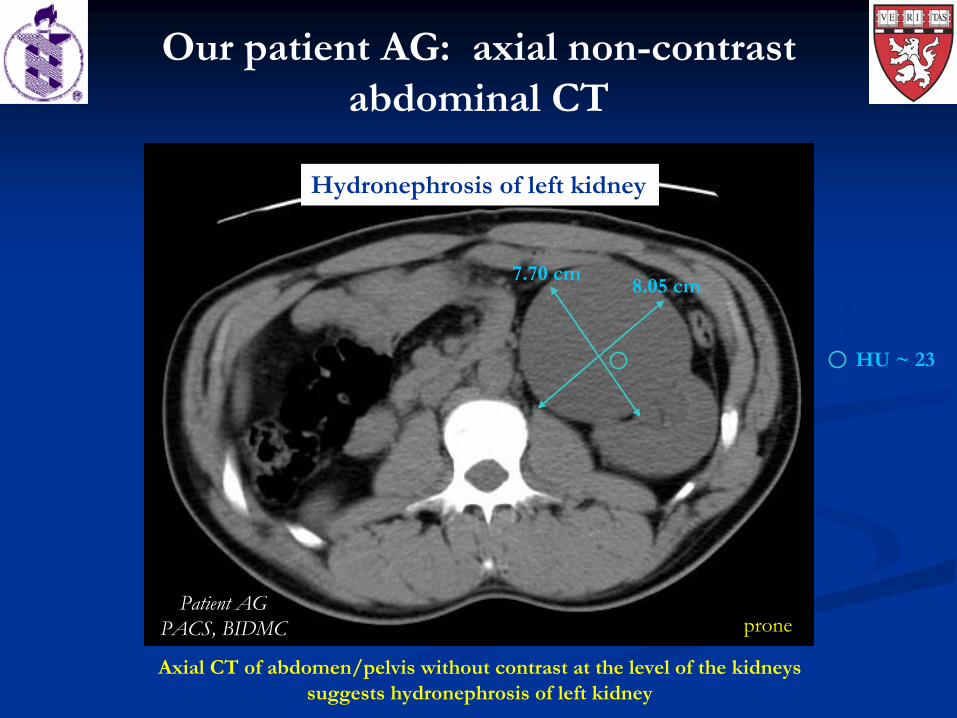
8.05 cm7.70 cm
HU ~ 23
Hydronephrosis
of left kidney
Our patient AG: axial non-contrast abdominal CT
Patient AGPACS, BIDMC prone
Axial CT of abdomen/pelvis without contrast at the level of the kidneys suggests hydronephrosis
of left kidney
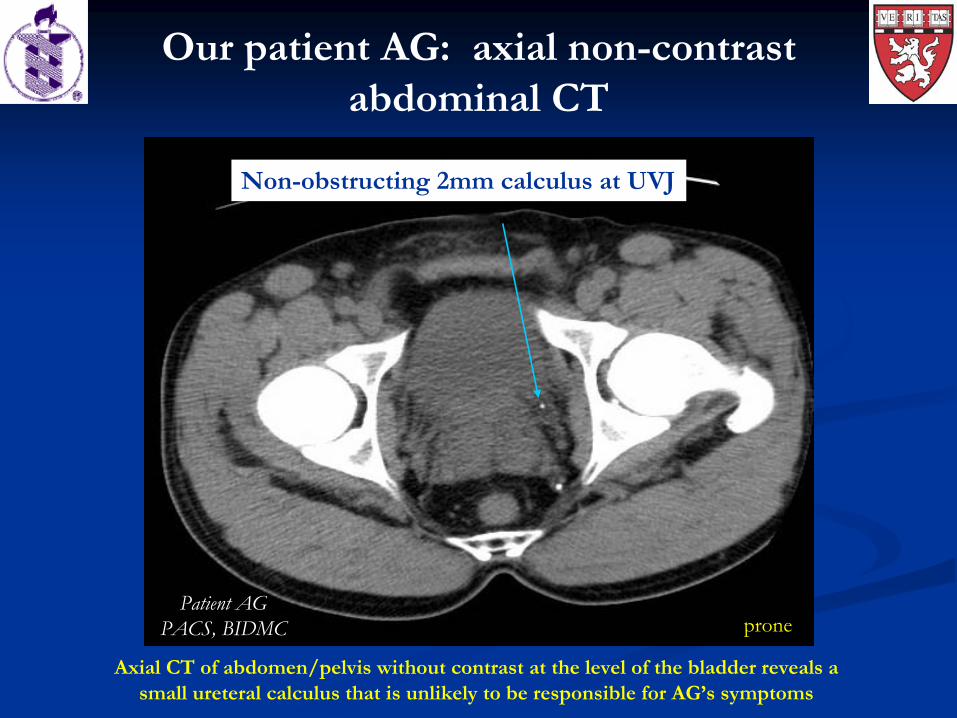
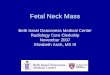
Non-obstructing 2mm calculus at UVJ
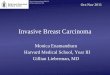
Our patient AG: axial non-contrast abdominal CT
Patient AGPACS, BIDMC prone
Axial CT of abdomen/pelvis without contrast at the level of the bladder reveals a small ureteral
calculus that is unlikely to be responsible for AG’s symptoms
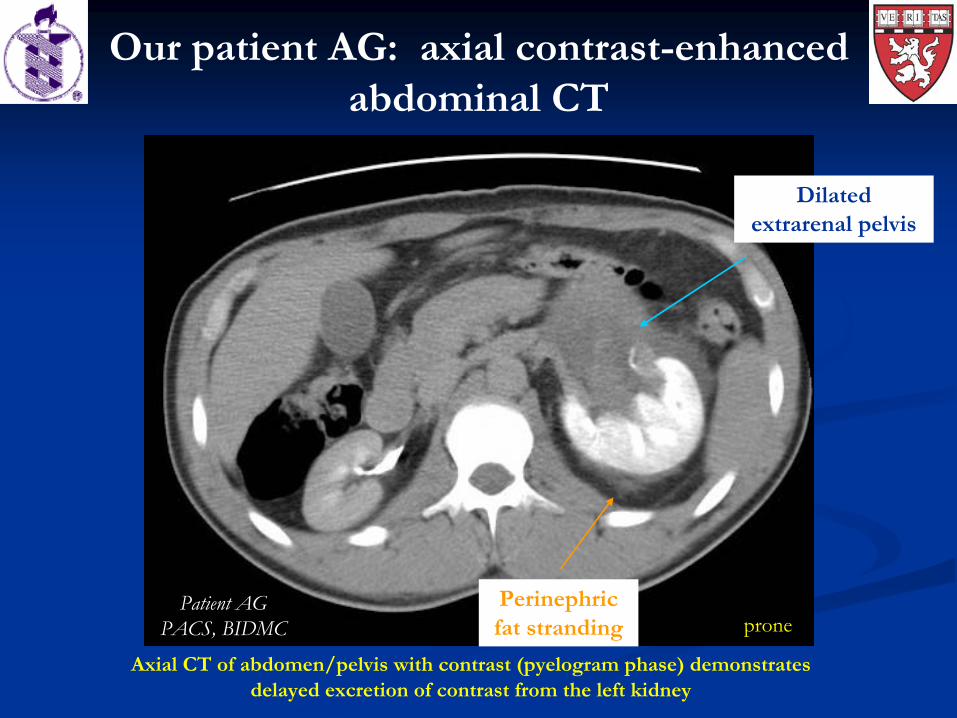
Axial CT of abdomen/pelvis with contrast (pyelogram
phase) demonstrates delayed excretion of contrast from the left kidney
Perinephric
fat stranding
Dilated extrarenal
pelvis
Patient AGPACS, BIDMC prone
Our patient AG: axial contrast-enhanced abdominal CT
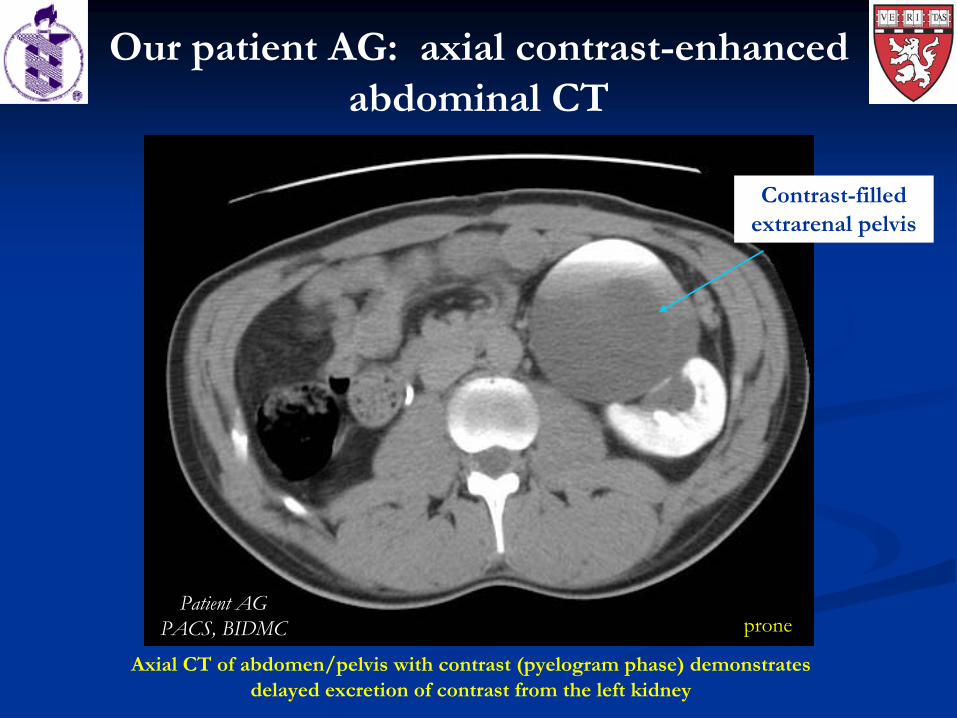
Contrast-filledextrarenal
pelvis
Our patient AG: axial contrast-enhanced abdominal CT
Patient AGPACS, BIDMC prone
Axial CT of abdomen/pelvis with contrast (pyelogram
phase) demonstrates delayed excretion of contrast from the left kidney
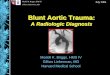
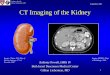
Patient AGPACS, BIDMC
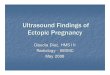
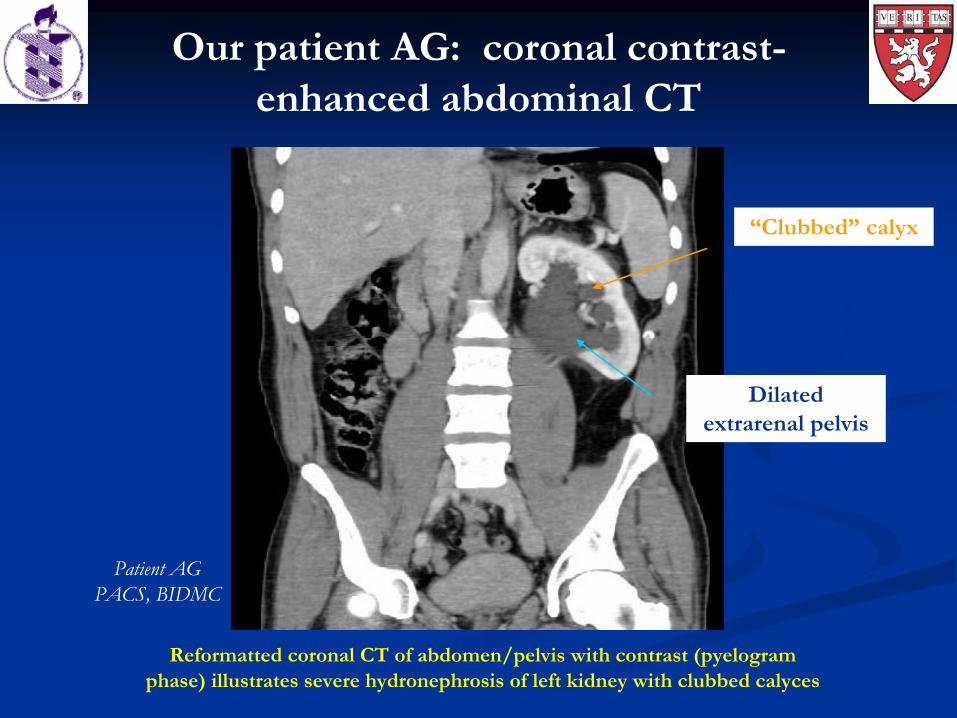
Reformatted coronal CT of abdomen/pelvis with contrast (pyelogram
phase) illustrates severe hydronephrosis
of left kidney with clubbed calyces
Dilated extrarenal
pelvis
Our patient AG: coronal contrast- enhanced abdominal CT
“Clubbed” calyx
Hospital course
Admitted to hospital for pain control and IV hydration
Cystoscopy
and retrograde pyelogram
performedLeft uretero-pelvic junction (UPJ) obstruction
confirmedDouble J left ureteral
stent
placed to relieve
obstruction and reduce hydronephrosis
Successful stent placement confirmed on KUB
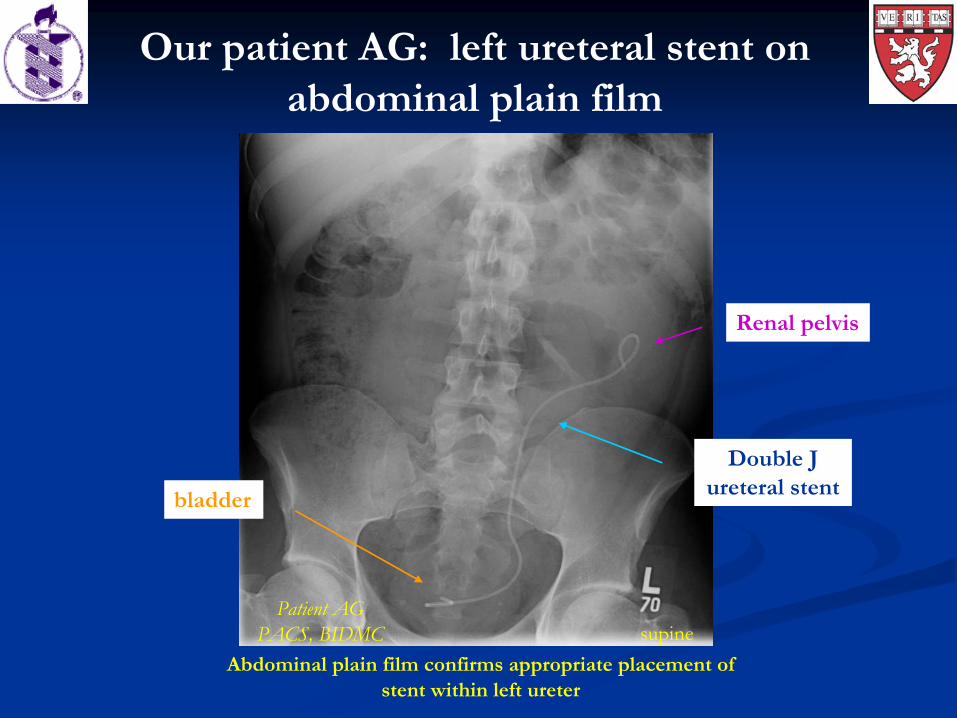
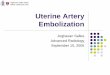
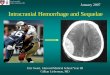
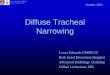
Our patient AG: left ureteral
stent on abdominal plain film
Double J ureteral
stent
Renal pelvis
bladder
Abdominal plain film confirms appropriate placement of stent within left ureter
supinePatient AG
PACS, BIDMC
Hospital course
Admitted to hospital for pain control and IV hydration
Cystoscopy
and retrograde pyelogram
performedLeft uretero-pelvic junction (UPJ) obstruction confirmedDouble J left ureteral
stent placed to relieve
obstruction and reduce hydronephrosis
Successful stent placement confirmed on KUB
MAG3 scan performed to evaluate differential renal function
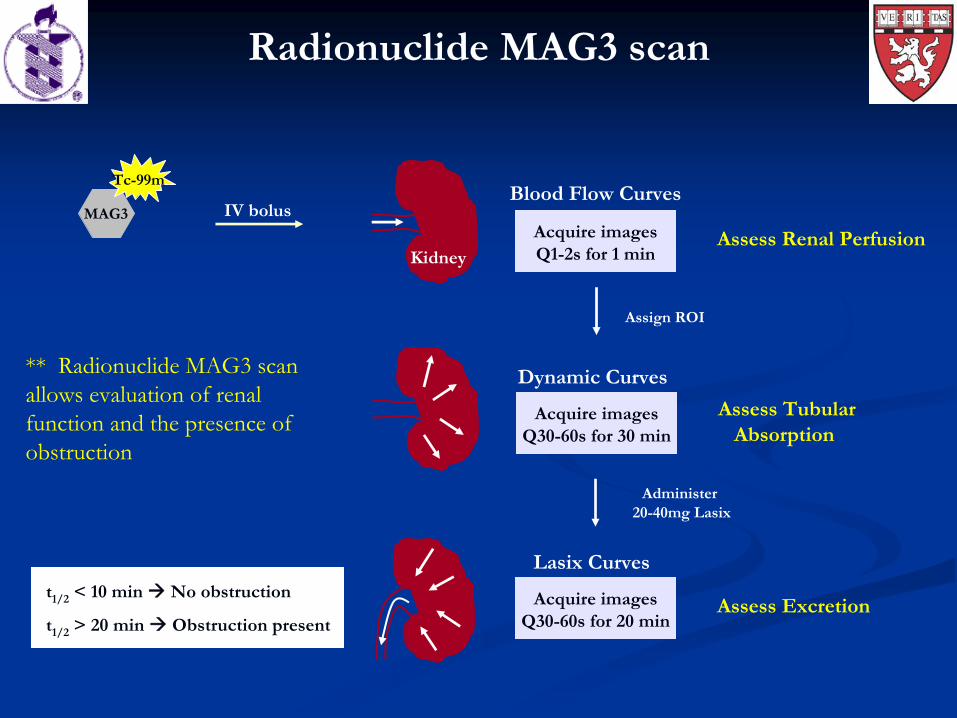
Radionuclide MAG3 scan
Tc-99m
MAG3 IV bolusAcquire images Q1-2s for 1 min
Blood Flow Curves
KidneyAssess Renal Perfusion
t1/2
< 10 min No obstruction
t1/2
> 20 min Obstruction present
Acquire images Q30-60s for 30 min
Dynamic Curves
Assess Tubular Absorption
Assign ROI
Acquire images Q30-60s for 20 min
Lasix
Curves
Assess Excretion
Administer 20-40mg Lasix
** Radionuclide MAG3 scan allows evaluation of renal function and the presence of obstruction

Our patient AG: radionuclide MAG3 scan, flow curves
L RL R
MAG3 scan (Flow phase)
L R
** Flow curves demonstrate comparable renal arterial blood flow to both kidneys
Patient AGImages courtesy of
Dr. Kevin Donohoe
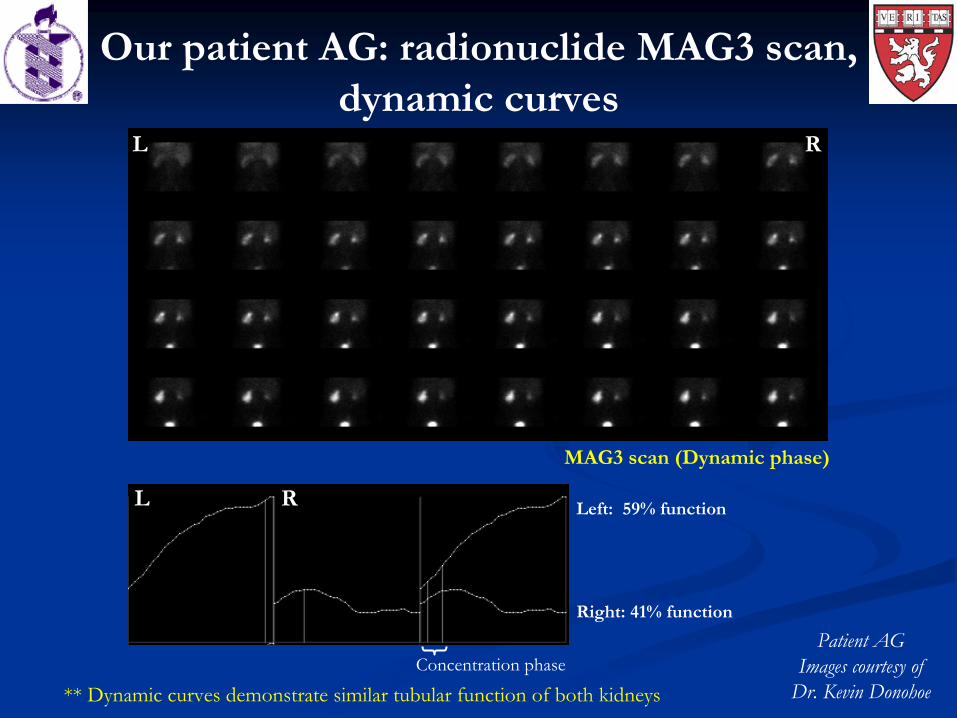
MAG3 scan (Dynamic phase)
L R Left: 59% function
Concentration phase
Right: 41% function
L R
Our patient AG: radionuclide MAG3 scan, dynamic curves
** Dynamic curves demonstrate similar tubular function of both kidneys
Patient AGImages courtesy of
Dr. Kevin Donohoe
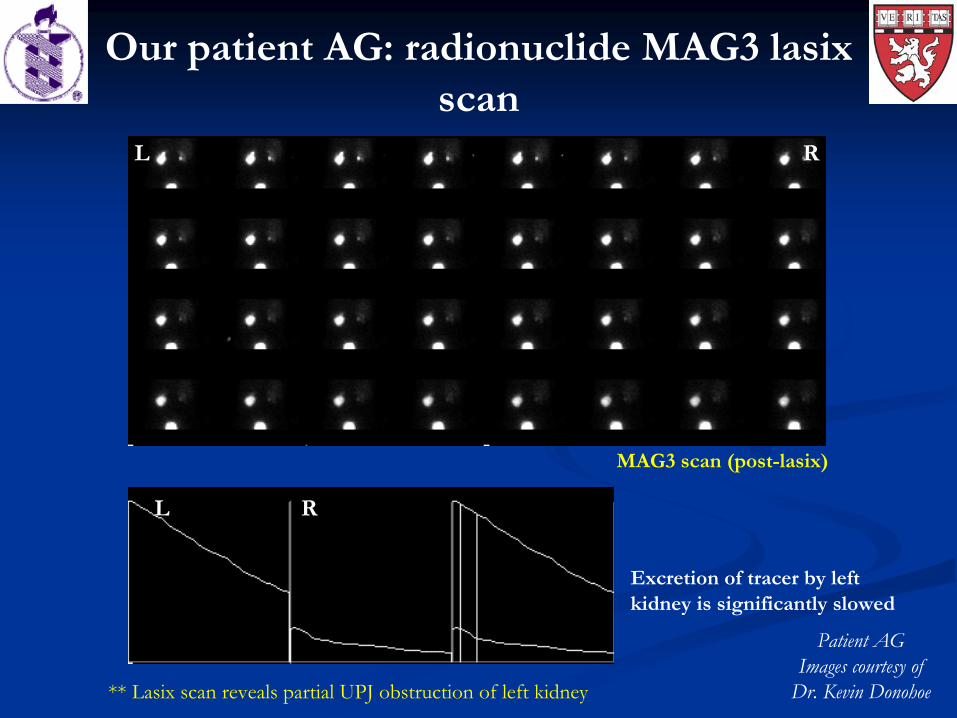
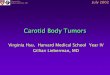
MAG3 scan (post-lasix)
L R
L R
Excretion of tracer by left kidney is significantly slowed
Our patient AG: radionuclide MAG3 lasix scan
** Lasix
scan reveals partial UPJ obstruction of left kidney
Patient AGImages courtesy of
Dr. Kevin Donohoe
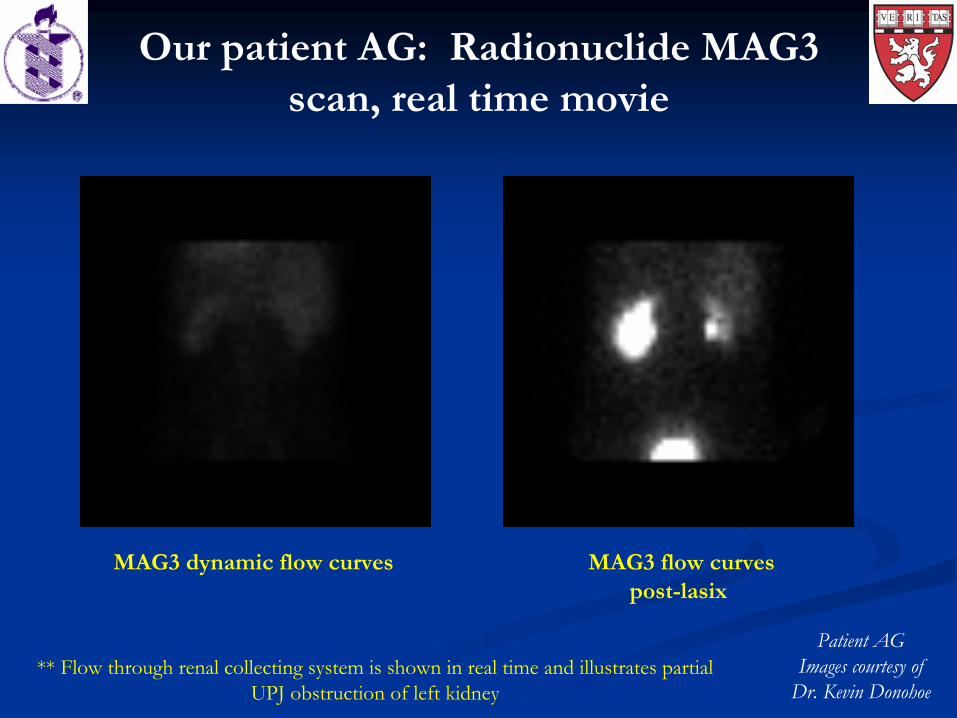
Our patient AG: Radionuclide MAG3 scan, real time movie
MAG3 dynamic flow curves MAG3 flow curvespost-lasix
Patient AGImages courtesy of
Dr. Kevin Donohoe** Flow through renal collecting system is shown in real time and illustrates partial
UPJ obstruction of left kidney
Patient follow-up
Patient continued to have left flank pain despite ureteral
stent placement
He underwent elective dismembered pyeloplasty of left kidney 3 weeks later
Patient’s pain was relieved following pyeloplasty
Follow-up IVP 7 months later showed resolution of obstruction despite a persistently dilated left renal pelvis
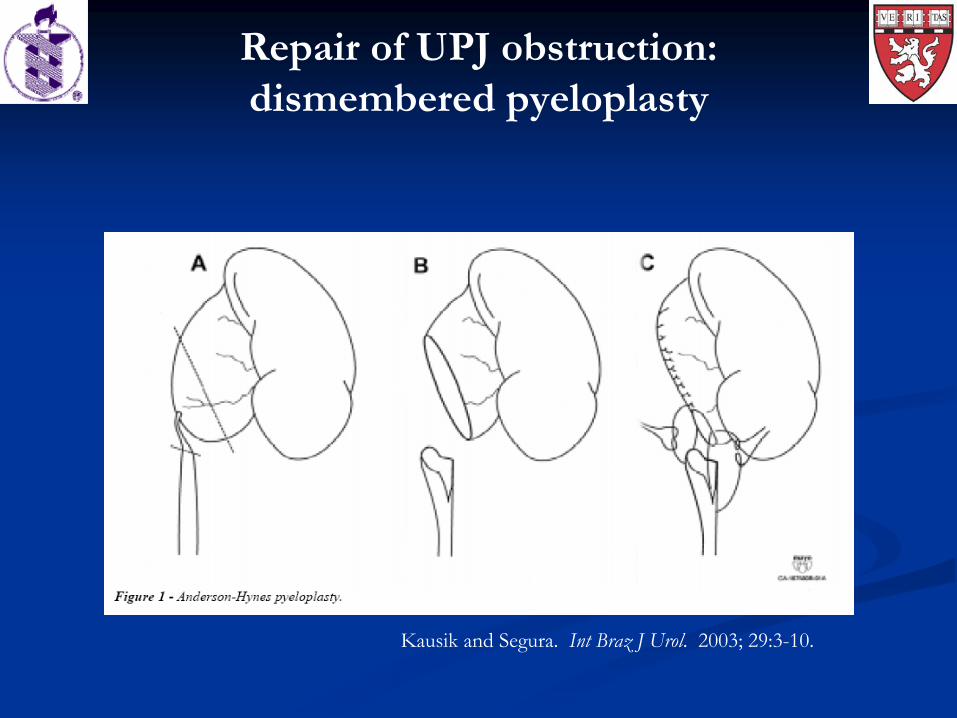
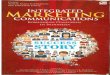
Repair of UPJ obstruction: dismembered pyeloplasty
Kausik
and Segura. Int
Braz
J Urol. 2003; 29:3-10.
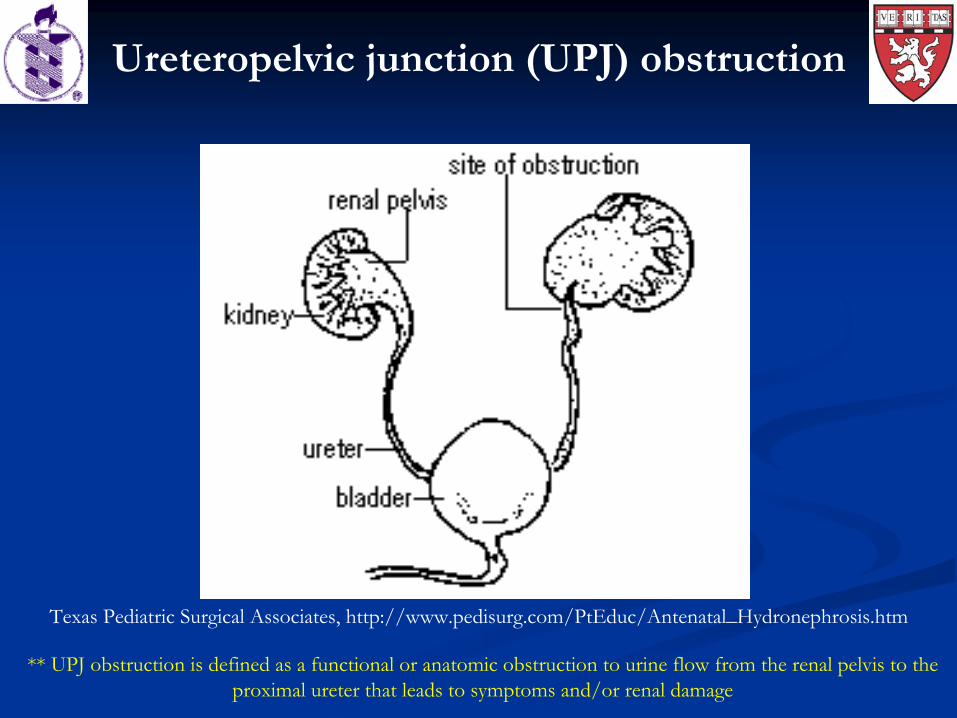
Ureteropelvic
junction (UPJ) obstruction
Texas Pediatric Surgical Associates, http://www.pedisurg.com/PtEduc/Antenatal_Hydronephrosis.htm
** UPJ obstruction is defined as a functional or anatomic obstruction to urine flow from the renal pelvis to the proximal ureter
that leads to symptoms and/or renal damage
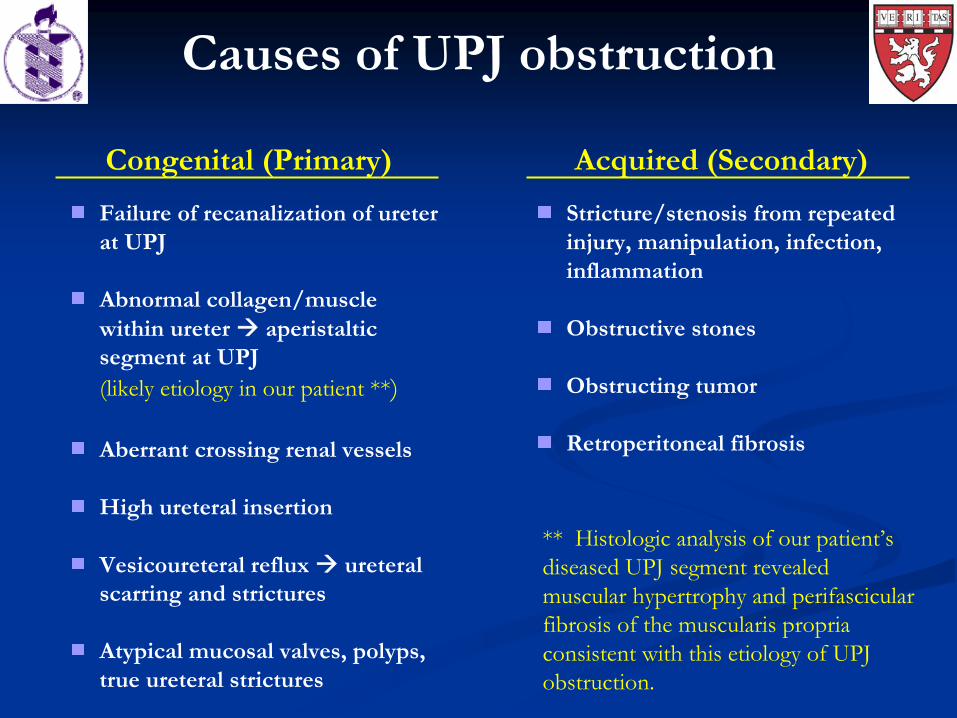
Congenital (Primary) Acquired (Secondary)
Causes of UPJ obstruction
Failure of recanalization
of ureter
at UPJ
Abnormal collagen/muscle within ureter aperistalticsegment at UPJ (likely etiology in our patient **)
Aberrant crossing renal vessels
High ureteral
insertion
Vesicoureteral
reflux ureteralscarring and strictures
Atypical mucosal valves, polyps, true ureteral
strictures
Stricture/stenosis
from repeated injury, manipulation, infection, inflammation
Obstructive stones
Obstructing tumor
Retroperitoneal fibrosis
** Histologic
analysis of our patient’s diseased UPJ segment revealed muscular hypertrophy and perifascicular
fibrosis of the muscularis
propria
consistent with this etiology of UPJ obstruction.
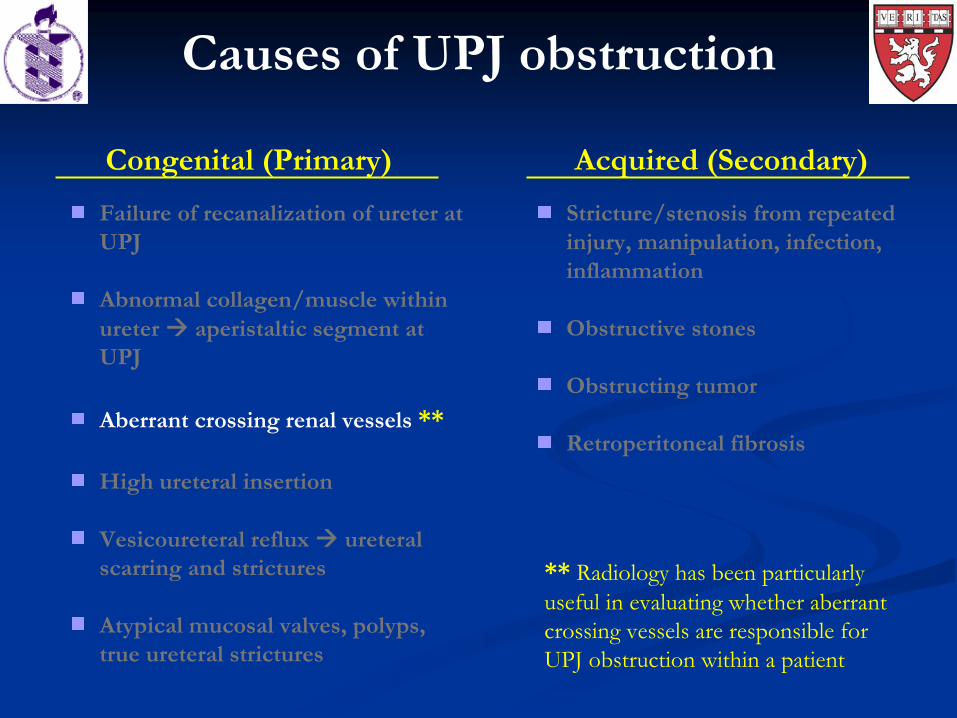
**
Radiology has been particularly useful in evaluating whether aberrant crossing vessels are responsible for UPJ obstruction within a patient
Congenital (Primary) Acquired (Secondary)
Causes of UPJ obstruction
Failure of recanalization
of ureter
at UPJ
Abnormal collagen/muscle within ureter aperistaltic segment at UPJ
Aberrant crossing renal vessels **
High ureteral
insertion
Vesicoureteral
reflux ureteralscarring and strictures
Atypical mucosal valves, polyps, true ureteral
strictures
Stricture/stenosis
from repeated injury, manipulation, infection, inflammation
Obstructive stones
Obstructing tumor
Retroperitoneal fibrosis
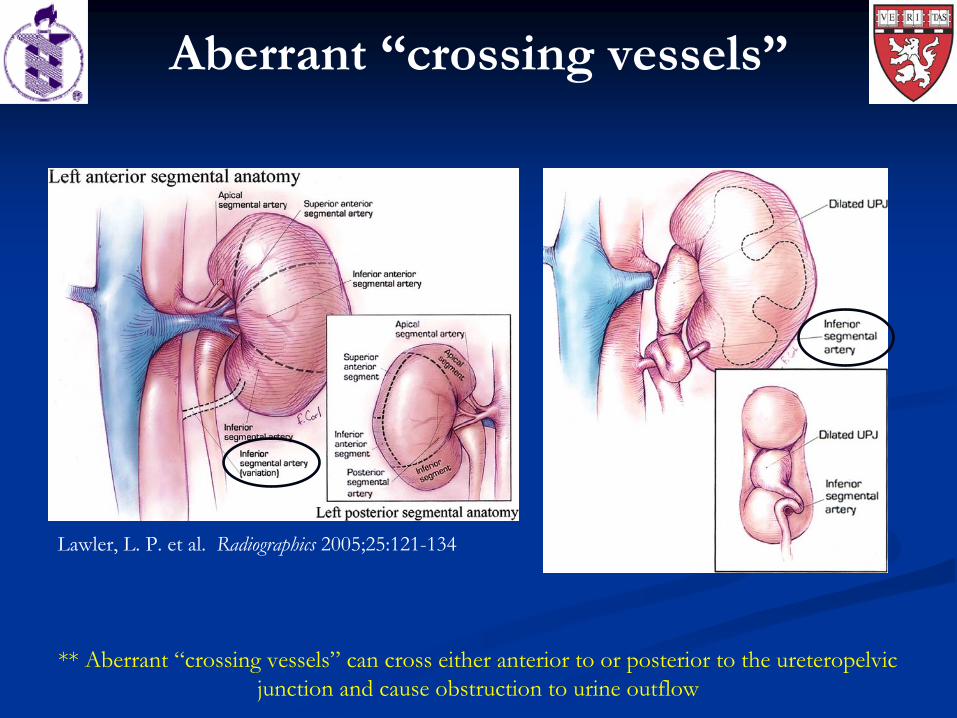
Lawler, L. P. et al. Radiographics
2005;25:121-134
Aberrant “crossing vessels”
** Aberrant “crossing vessels” can cross either anterior to or posterior to the ureteropelvic
junction and cause obstruction to urine outflow
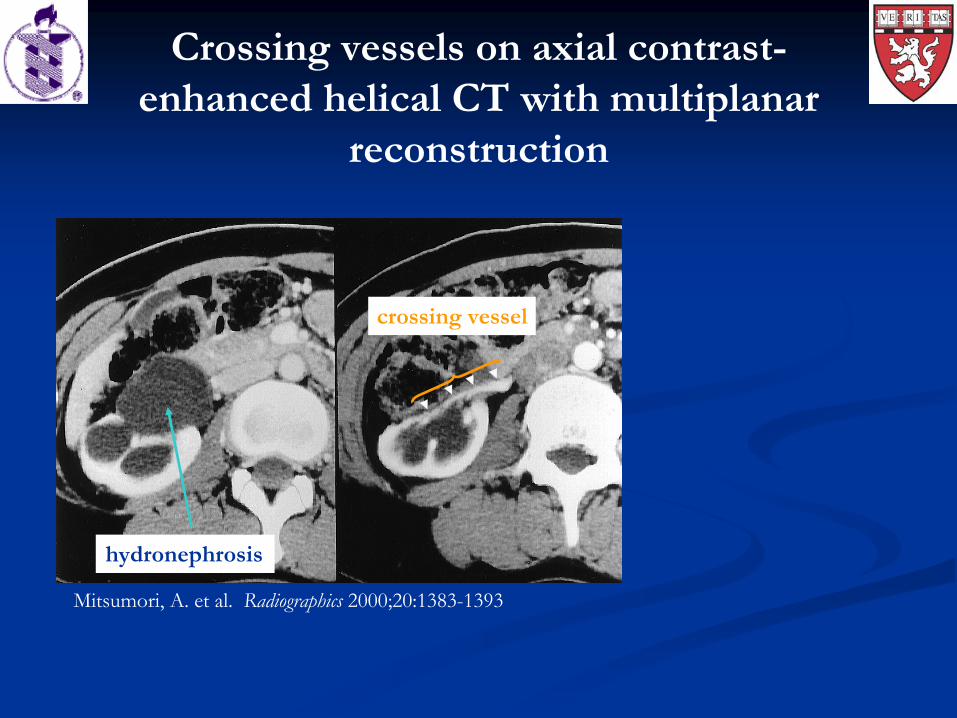
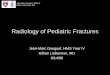
Crossing vessels on axial contrast- enhanced helical CT with multiplanar
reconstruction
Mitsumori, A. et al. Radiographics
2000;20:1383-1393
hydronephrosis
crossing vessel
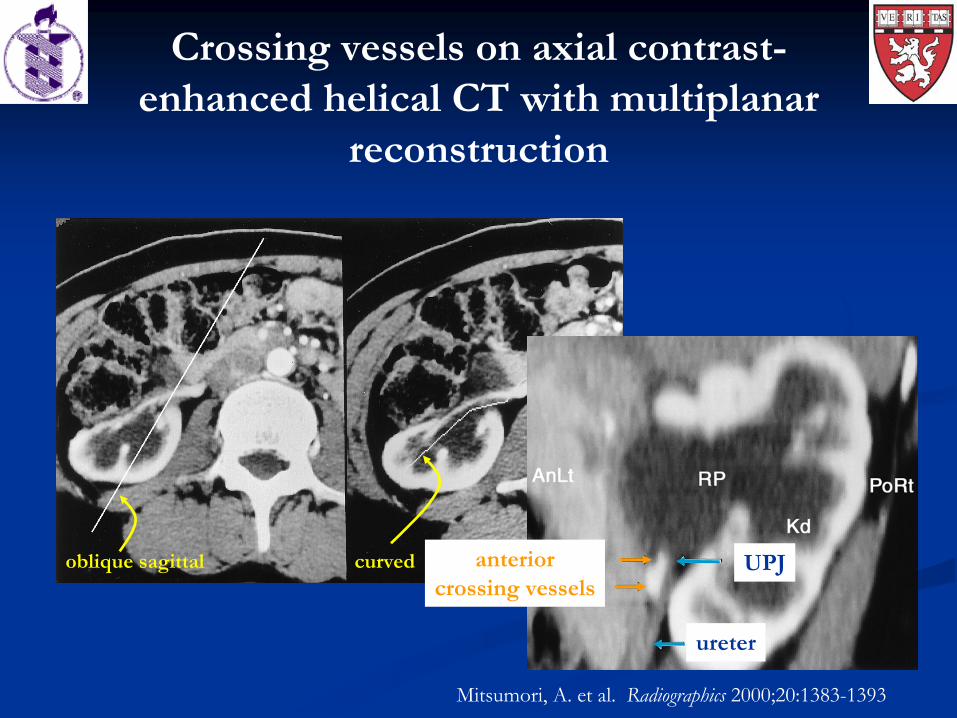
oblique sagittal curved anteriorcrossing vessels
ureter
UPJ
Mitsumori, A. et al. Radiographics
2000;20:1383-1393
Crossing vessels on axial contrast- enhanced helical CT with multiplanar
reconstruction
Complications of UPJ obstruction are varied
Progressive functional impairment of kidneysProgressive functional impairment of kidneys
Poor growth in infantsPoor growth in infants
Urinary stasisUrinary stasis
UTIs/pyelonephritisUTIs/pyelonephritis
StonesStones
HypertensionHypertension
Increased susceptibility to renal pelvis rupture with blunt Increased susceptibility to renal pelvis rupture with blunt
traumatrauma
Symptoms of pain, nausea, vomiting, and Symptoms of pain, nausea, vomiting, and hematuriahematuria, ,
especially with large fluid intake especially with large fluid intake DietlDietl’’ss crisiscrisis
Some surgical treatment options for UPJ obstruction
Open dismembered Open dismembered pyeloplastypyeloplasty
Laparoscopic Laparoscopic pyeloplastypyeloplasty
AntegradeAntegrade endopyelotomyendopyelotomy
PercutaneousPercutaneous access to renal calyx with access to renal calyx with antegradeantegrade placement of placement of
nephroscopenephroscope
Endoscopic incision of diseased UPJ segment with cutting Endoscopic incision of diseased UPJ segment with cutting
instrumentinstrument
Retrograde Retrograde endopyelotomyendopyelotomy
UreteroscopeUreteroscope advanced past diseased UPJ segment advanced past diseased UPJ segment
Holmium laser incision of diseased UPJ segmentHolmium laser incision of diseased UPJ segment
Acknowledgments
Dr. Dan AnghelsescuDr. Kevin DonohoeDr. David Graham
Dr. Gillian LiebermanNyca
Bowen
ReferencesGrasso M, Gitlin
JS, and Johnson GB. Ureteropelvic
junction obstruction. eMedicine
from WebMD. Last updated 05-22-06. Retrieved 09-13-07. http://www.emedicine.com/med/topic3074.htm
Kausik
S and Segura JW. Surgical management of ureteropelvic
junction obstruction in adults. Int
Braz
J Urol. 2003; 29:3-10.
Lawler LP, Jarret
TW, Corl
FM, and Fishman EK. Adult ureteropelvic
junction obstruction: insights with three-dimensional multi-detector row CT. Radiographics.
2005; 25:121-134.
Mitsumori
A, Yasui
K, Akaki
S, Togami I, Joja
I, Hashimoto H, Kumon
H, and Hiraki
Y. Radiographics. 2000; 20:1383-1393.
Texas Pediatric Surgical Associates, http://www.pedisurg.com/PtEduc/Antenatal_Hydronephrosis.htm
Weiner J, Yang B, and Gaca
A. Ureteroplevic
Junction Obstruction, Congenital. eMedicine
from WebMD. Last updated 08-03-2007. Retrieved on 09-13-07. http://www.emedicine.com/radio/topic730.htm