Embed Size (px)
Citation preview

Trends in Pharmacological Sciences
October 1983
Use of sales statistics for evaluating prescription rationale Sophisticated methodology is now avail- able for the scientific evaluation of drug efficacy and valuable efforts are being made to detect side-effects. Patient com- pliance has recently become a concern for physicians. However, prescribing deci- sions, although subject to major educa- tional efforts to optimize them, have rarely been scrutinized ~5. It has been said that they are shaped by forces unrelated to the pharmacological properties of medications (the 'non-pharmacological basis of therapeutics'). Studies which have been reported on how physicians arrive at therapeutic decisions, accord the most important role to scientific literature. How- ever, these surveys are generally based on weak methodology. A recent study strongly
suggested that drug advertisement could he a decisive factor, even though doctors were not aware of such influences 1.
Our aim was to test whether there is a correlation between prescribing habits and the supply of correct data on drug efficacy to the medical community. The ability of the system to produce optimal prescribing on the basis of available evidence on drugs effects is questioned by this approach.
Our study covered the period 1974-1979. The system under investiga- tion could he regarded as an almost com- pletely closed model, with only two con- nections with the outside: one for input and one for output. The input consisted of data on drug efficacy or on cost/benefit ratio. These data are provided by original reports
of controlled trials, they are generally pub- lished in specialized journals or high stan- dard unoriented journals. We only took into account trials which were designed to test the clinical efficacy of a treatment, i.e. phase HI or phase IV studies. There is a constant pressure in therapy evaluation to shift from clinical end-points, such as event free period or patient subjective improvement, to measurable targets, such as a change in serum cholesterol level, blood pressure or biochemical indicators of inflammatory state. However, health status is not ade- quately defined by biochemistry, nor is a patient's disability necessarily improved because some blood parameter has increased or decreased. Only reports of tri- als whose objectives were to assess a clini-
1983 Ehew~r S¢~m~e Publud~ B V, AmsteMm~ 016.5 - 6147/83/$01 00

SALES
1 0 0 0
INPUT f( t)
f (to) FINDINGS
+1 POSITIVE
- I NEGATIVE
0 NEUTRAL OR DUBIOUS
EXPECTED OUTPUT g(t)
SALES
402
~t
AG TI ME 1
t (o)
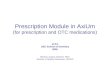
Fig. 1 I f the results o f a study are positive, an increase in the prescribing o f the corresponding drug is expected, i f the results are negative, a decrease is expected. Dubious or neutral results should lead to no change in prescription rate. There is a lag between issue o f the paper and change in sales.
7 5 0 -
5 0 0
2 5 0
+ .... l l l l l , l I I I .
1974 ' 1975 1976 ' 1977 ' 1978 ' 1979 a
~ o
674 t ~ t ~ ~7 1~ 1~
T I P S - O c t o b e r 1 9 8 3
cal benefit were taken into account. 'Out- put' was drug sales, measured in number of packages delivered or, when possible, in the Daffy Defined Dose 2.
Information fluxes inside the system stream in pre-formed paths to the pre- scriber, and the information can be modi- fied at each step. It is quite unusual in France for prescribers to read original reports of controlled trials; they usually only read second-hand summaries or abstracts.
The system, described above, is analog- ous with a'black box'. The investigator of a 'black box' varies a certain input and examines how the system responds by measuring the output. The simplest varia- tion is the unit impulse. Report of a control- led trial behaves as an impulse function: it is unique, and precisely dated (date of issue). It is easy to grade each report, positive results correspond to a positive unit impulse, negative results correspond to a negative unit impulse and dubious results to no impulse at all. The response function is estimated by measuring changes in sales. Were the system efficient, we would easily foresee the behavior of the response func- tion for each type of impulse. The three possibilities are shown in Fig. 1. The sys- tem is assumed to be in steady-state before the observation started. As this is obviously not always true, any discrepancy from the expected behavior should be scrutinized with respect to the consequences of depart- ing from this assumption.
In order to emphasize changes in output, the cusum technique was used to express
Fig. 2. (left) The cumulative sum o f fl-blocker sales are plotted. The annual sales have been transformed into percentage o f 1974 sales be[ore summing. The lower part o f the figure schematically indicates the positive (+), negative ( - ) , or dubious (+1-) results, corresponding arrows or points indicate the dates when the publications were issued.
Fig. 3. (below) The cumulative sum o f anti-platelet drug sales are plotted. (See legend of Fig. 2.)
600
500-
400
300
200
100.
0

T I P S - Oc tober 1 9 8 3
sales graphically as a function of time °. Drugs investigated belonged to four clas- ses: #-adrenergic blocking agents; slow- release or long-acting nitrates; fibrates, i.e. clofibrate and derivatives; and platelet modifying agents, Aspirin was not consi- dered as an anti-platelet agent as other factors govern its sales.
Indications were decided according to the common use of each drug, irrespective of whether they were licensed accordingly. In 1975 more stringent new rules for drug application were issued by the Ministry of Health. However, they were not fully applied until 1979 when the 'Commission d'Autorisation de Mise sur le March6' (Comm/ttee for Drug License) was reor- ganized. Before this, authorization for seb ling a drug was easy to obtain provided that its safety was demonstrated. Diseases, cor- responding drugs and required criteria of efficacy for evaluation are described in Table I. Rare diseases or indications not accepted by the French medical community were not included in the survey. Acute heart failure was not considered as the number of events per year was not high enough to explain the large consumption of long-acting nitrates.
A survey of literature was made through our library's index and 'Mediine ' . More than 500 published reports of controlled tri- Ms were considered. Reports were selected according to four criteria~: (1) the trial was" controlled, i.e. its design included random allocation to control or test drug groups; (2) control group received placebo or, in few instances, reference treatment, the efficacy of which was weft-established; (3) the number of patients recnfited was large enough to give statistically significant results; (4) the end-points permitted clini- cal efficacy evaluation (the list of selected papers and attributed values can be obtained from the authors on request). Table I describes the end-points for each drug class and disease. It is obvious that there is some departure from the fourth rule of selection. In some instances, such as hypertension, it appeared worthwhile to consider lower level end-points in addition. However, reports belonging to this cate- gory have not been mixed with the others when correlation was assessed.
Consumption levels were obtained through IMS reports. A panel of 300 phar- macists provide data which are assumed to be representative of sales of each product in France. These sales were estimated from these data. The error is within _+ 5%.
Sales of/g-blockers correlated well with input of positive results, despite the fact that some early studies yielded negative data (Fig. 2). Therefore, the outcome is in agreement with the expected result. In cow
TABLE I.
Indications Drugs End.points for c "hnical evaluaOon a
Hypertension #-adrenergic antagomsts 1 total mortality; 2 cardio- vascular events (cardmc or cerebral death, su'oke, myocardial infarction ete . . . . ) (3 blood-pressure) b
I a n g i n a p e c t o r i s : n u m b e r s o f
attacks, patient's well-being (2 exercise test perfonmm~)b
1 total mortality; 2 cardio- vascular mortahty; 3 death following cardiac event, 4 myocardial infarction or stroke; 5 transient iscbemic attack
I total mortality; 2 cardiac death 3 functional subjective status; 4 myocardial infarction
I total mortality; 2 cardiac death, 3 functional subjective status; (4 bemodynanuc) b
403
Angina pectoris Long.acting niuates /3-adrenerg~c anugomsts
AtbemscleroUc Fibrates diseases Platelet modifying agents
Coronar x heart Fibrates disease (excluding Platelet modifying agents angina pec~is) ~-adrenergic antagonists
Chronic heart Long-acting nitrates failure
"EnCpomts are numbered according to a decreasing clinical interest. b In some cases, lower level or intermediate end-points have been considen~ in addition to chmcal end-points. However, publications belonging to these categories have been correlated separately with consumption.
10 000
5000
2ooQ
150O
1000
300
200
150
100
...... -~(~
s =®
0. ............ • @
11 S i ,0 .....-"
.... o-'" / .--e- ..... / .8"'''''"
• ......" . ...o""
_- A m .... A =
1974 1975 1976 1977 1978 1979
F~. 4. Long-acting n/trates, the/ogar/thm of the percentage o f annual sales, 1974 being the basis. ISD N = isosorbide-dinitrate; 1 shows products marketed after 1970; 2 shows products marketed before 1971; 3 shows all long-acting nitrates.

404
trast, sales of antiplatelet agents and long- acting nitrates increased tremendously, although only doubtful or negative clinical results were reported during the period studied (Figs 3 and 4). Consumption of dipyridamole in 1979 was three times that during 1974.
Consumption of long-acting nitrates more than doubled. An intriguing issue was observed with sales of isosorbide dinitrate (ISDN). Only one manufacturer had mar- keted this drug. Although it was licensed for many years, consumption was nearly zero until 1975. Thereafter, it rose tremendously. This could not be explained by positive reports, for no controlled trial with ISDN was published prior to 1978. Actually, a report of one trial concerned with ISDN and chronic heart failure was issued in 1978. Surprisingly, the start of
increased sales rate preceded, by two years, the promoting efforts of the firm which did not begin until 1977.
The positive gradient of antiplatelet con- sumption, mainly of dipyridamole, could have been caused by previous positive clin- ical results. Before 1974 only one clinical trial with dipyfidamole had been published which gave a favorable outcome. It con- cerned patients with prosthetic heart valves. However, it would have needed 400 000 French people to be operated for valvular diseases to explain the amount of dipyridamole pills sold in 1979. In addi- tion, doubtful results were published in 1978 concerning the same drug and the same indication.
Overall, sales of fibrates increased from 1974 to 1979. This was a complex phenomenon (Fig. 5). Clofibrate sales in
l I I l I l I l I l I 2 0 0 0 - m
/
ta . . . . . t3 c lo f i b ra te (s ) 1891 z~ a ~ - - - --~ f e n o f i b r a t e E
I 0 0 f i b r a t e s (c lo - f e n o ) t m
I i
i #
i #
/
i i
i i
i E
I i
i i
i 1 0 0 0 - t
931 '~ I
/
/ / "
- 1 0 0 - ~ . . . . . . . A / " - - m
2911
t
1974 1975 1976 1977 1978 1979
Fig. 5. The cumulative sum of clofibrate (and derivatives) sales are plotted. (See legend of Fig. 2.)
T I P S - Oc tober 1983
1979 were half their 1974 value. A possible explanation is the negative findings of CDP and WHO trials. However, a new drug, fenofibrate, was marketed in 1975. Despite the fact that it had not been investigated as thoroughly as the parent drug, it accounted for a three-fold increase in total sales.
Discussion In our study, sales directly reflected the
amount of drugs prescribed, since over the counter products were not included. It must be concluded from these comparisons of availability of reliable clinical efficacy studies and prescription of drugs, that logi- cal behavior was not the rule. Rather, pre- scribing seemed to vary almost indepen- dently of accurate information. However, manufacturers' promotion efforts are not the only force responsible for irrational pre- scribing habits; faculty clinicians and cling cal pharmacologists are not successful in their attempts to teach good practice or, possibly, doctors are not receptive enough. In some instances they clearly failed to teach the scientific evidence, as was the case with isosorbide dinitrate. When made aware of the potential interest of this drug in heart failure by research papers, and of a new and exciting model for treating this disease, doctors transformed hopes into assumptions, then into certitudes. In addi- tion, lack of clinical trial results do not impair the effect of promotion (fenofibrate) and even weak scientific backing can be sufficient to bolster sales (dipyridamole in clinical thrombo-embolism).
The details of the method we used need to be improved. However, it can be pro- posed as a starting-point for future research on doctor education, or as a tool for evalua- tion of medical information systems.
J. P. BOISSEL, S. FERRY AND
P. GALLOIS
H~Spital Neurologique et cardiologique, 59 boulevard Pinel Lyon 3e, BP Lyon Montchat 69394, Lyon Cedex 3, France and HOpital G~n~ral de Macon, 7100 Macon, France.
Reading list 1 Avom, J., Chen, M. and Hartley, R. (1982) Am. J.
Med. 73, 4-8 2 Baksaas, I. (1975) Drug dose statistic. List of
daily defined doses for drugs registered in Nor- way, Oslo, Norks, Medisinaldepot
3 Chalmers, T. C., Smith, H., Blackburg, B., Silverman, B., Schroder, B., Reitman, D. and Ambroz, A. (1981) Control. Clin. Trials 2, 31-49
4 Elmes, P. C. (1976) UlsterMed. J. 45, 56-58 5 Wade, O. L. in Studies in Drug Utilization, pp.
3-15, WHO Regional PublieaUon, European series No. 8, Copenhague
6 Woodward, R. H. and Goldsmith, P. L. (1964) Cumulative Sum Techniques, I.C.I. monograph, Oliver and Boyd





















![Evaluating HIT Standards...interoperable communications. With increased mandates to use standards from HIPAA1 (e.g., ASC X12, National Council for Prescription Drug Programs [NCPDP]),](https://img.pdfslide.net/doc/110x75/5e836071800a4d2b8e6c66d7/evaluating-hit-standards-interoperable-communications-with-increased-mandates.jpg)