Embed Size (px)
Citation preview
1
Executive Summary
Double Fatalities Investigation Report
June 8, 2011
USW Local 6500
Investigation
Jason Chenier and Jordan Fram died because of on-going and documented neglect of
safety standards by the owner of the Frood/Stobie Mine complex, the international
mining company Vale.
After an incident of this kind, in accordance with previous practice there would have
been a joint investigation by union and management representatives from the
Frood/Stobie JHSC (Joint Health and Safety Committee).
But Vale insisted on restrictions on what the joint committee could investigate,
demanded exclusive control of all documents and communication, and required
non-disclosure of all information and findings acquired in the investigation process.
In effect, Vale demanded that it would control the determination of the cause of the
fatalities, as well as the conclusions and recommendations drawn from the
investigation and findings (pg. 20/USW Report)
Because of Vale’s restrictions, the Health and Safety Chair of USW Local 6500, Mike
Bond, announced on June 23rd, 2011 that USW Local 6500 would initiate its own
investigation into the deaths of Jordan Fram and Jason Chenier.
Throughout the Union’s investigation, Vale officials refused to be interviewed by
members of the USW Team; dozens of USW members cooperated fully in
management’s investigation, attended interviews and answered their questions
fully.
Over the course of eight months, the USW Team examined evidence, conducted
interviews, performed research and considered all aspects affecting the fatality and
the mining processes that impacted upon the tragic events of June 2011.
The USW Local 6500 Report was submitted to the Ontario Ministry of Labour on
February 28, 2012.
Cause of Death
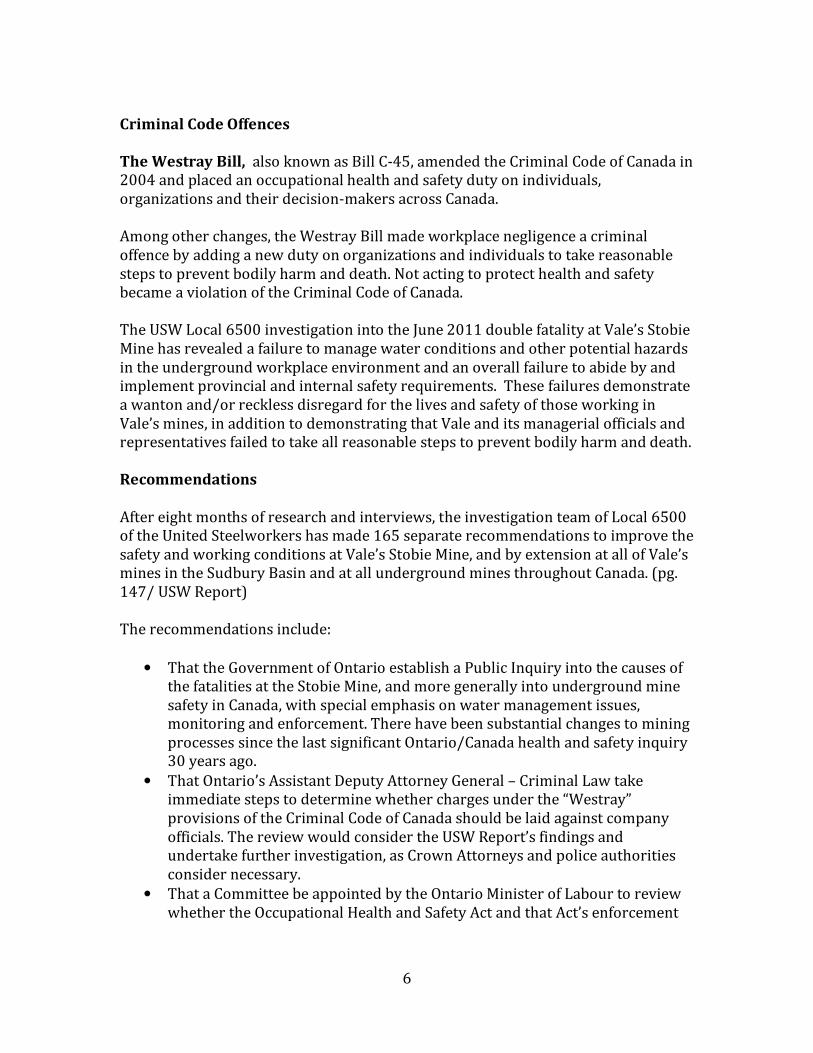
Jordan Fram and Jason Chenier died on the evening of June 8th, 2011, when an
uncontrolled torrent of wet ore material or run of muck burst out of the #7 ore pass,
and buried them. Ore passes allow miners to move ore from upper levels of the
mine down to lower levels, where it is eventually transported to the surface. The #7
2
ore pass carries ore from the 2600 foot level of the mine past the 3000 foot level of
the mine where the June 2011 deaths occurred.
The run of muck occurred because wet ore from the 2600 level had “hung up” and
clogged the #7 ore pass at a narrowing of the ore pass above the 3000 foot level.
Fram and Chenier were working there when they died.
Miners, mining companies and health and safety regulators have long recognized
this as one of the most hazardous conditions in underground mining. USW Local
6500 members had complained for weeks about hang-ups in the #7 ore pass; the
issues were not adequately addressed by management (pg. 107/USW report).
When investigators arrived on the scene of the fatalities, they found that the crash
gate, which is used to move material in the #7 ore pass from above the 3,000 level to
levels below, was left in the open position. Jason Chenier had apparently opened the
gate in order to assess the “hang-up” and prepare to blast it loose. While this is an
accepted practice, it has also been recognized as a non-routine hazardous task for
which there were no listed or detailed procedures. It is one of the most hazardous
tasks in underground mining. (pg. 51, 61/USW Report)
Cause of Deaths
The deaths of Jason Chenier and Jordan Fram are directly attributable to the unsafe
accumulation of water in the Stobie Mine and the inadequate procedures in effect to
deal with the consequences of such foreseeable developments.
The Stobie Mine is located underneath and adjacent to three abandoned open-pits,
which collect water predictably and regularly. This is within the knowledge of the
company and its engineers. Water accumulation issues are exacerbated during the
spring runoff. The spring run off occurs every spring.
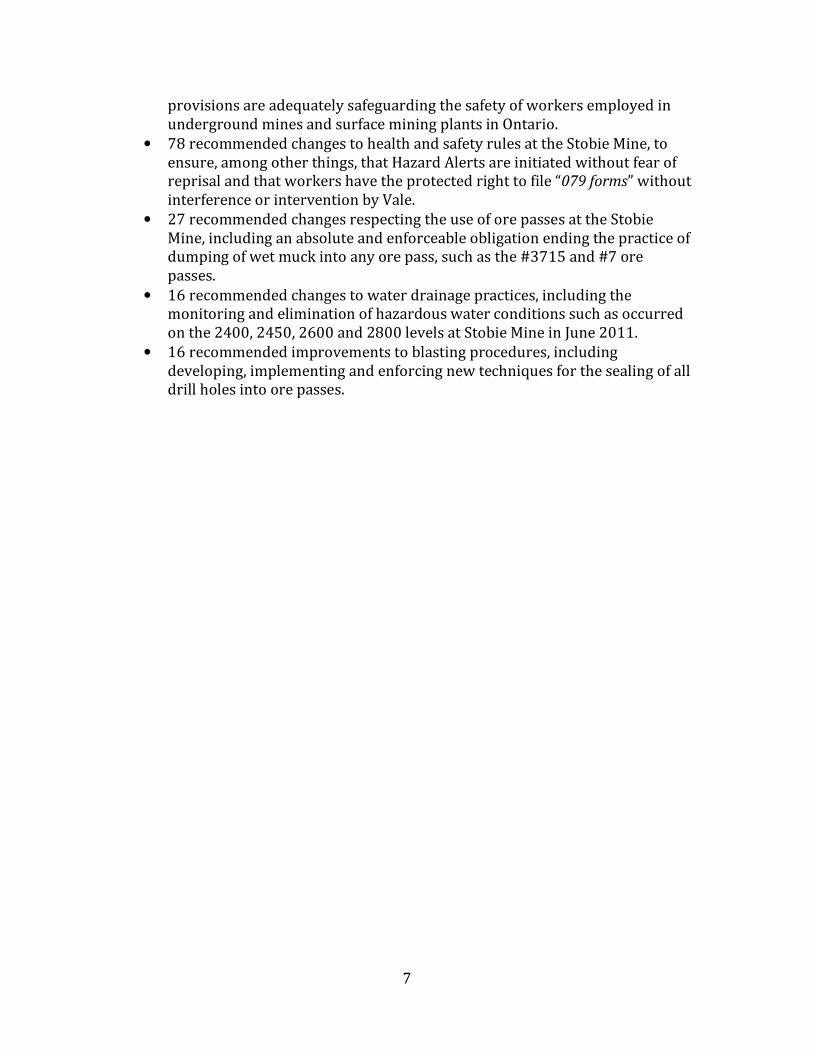
The company pumps and is obliged to safely manage 3 million gallons of water per
day. Shortly after the fatalities in June 2011, excessive water accumulation was
noticed on the 2400, 2450, 2600, 2800 and 3000 levels of the mine. (See photos pg.
40-42/USW Report).
When too much water saturates the ore, this creates sticky muck, a mixture that can
plug an ore pass. Since this is one of the most hazardous conditions in underground
mining, constant control of water is essential to maintain safety in the mine. A run of
muck is like an avalanche of wet rocks, wet gravel and wet sand.
The flow of water combined with mining material creates a mixture of mineralized
material, sand-fill and water. Stobie Mine’s technical service group stipulates that it
is acceptable to have sand and silt make up 30% of the ore material. A ratio in
excess of 30% has to be handled differently.

3
Six (6) weeks after the June 2011 tragedy, the ore was found to contain 50% sand
and silt and 13% moisture. (pg. 47/USW Report)
Safety Requirements:
Ore Pass Design, Operation, and Maintenance are critical to the safe transfer of
material in a mine. It is important that the original design takes into account the
type and consistency of material that will go through a pass. This would include a
sizing device to restrict the size of material being dumped, a cavity monitoring
system, crash gate operation procedures, prohibitions against the introduction of
water into an ore pass, procedures to maintain ore pass dimensions, safe crash gate
operation, and safe procedures for clearing “hang ups” in ore passes. (pg. 29/USW
Report)
Drain holes are one of the principal strategies to control and redirect excess water
in an underground mine such as Stobie. At the time of the incident, drain holes at the
2400, 2600 and 2800 levels were known to have been plugged by rock, sand fill and
debris. Water at the 2400 level was approximately 5 feet above the top of the drain
holes. Water at the 2600 level was about 4 feet above the top of the drain holes. This
caused water to flow into the top of #3715 ore passes, mixing with the ore and
creating sticky muck. (pg. 35-38/USW Report)
Blast holes are drilled into an ore pass to allow miners to blast or breakup a
blockage. Safety procedures require that the blast holes must be sealed and grouted
after use. The blast holes at the 2600 level broke through into the #7 ore pass since
they are below the level of the accumulated water. The blast holes provided a path
for water to enter the #7 ore pass. The blast holes drilled at the 2800 level were also
below the level where water had accumulated, providing another way for water to
enter the #7 ore pass. (pg. 52/USW Report)
Guardrails: Jason Chenier erected double guardrails at the 2450 and 2600 levels
to prevent the dumping of any more ore into the #7 ore-pass. This, in effect, was a
shut down signal for this production area. Jason Chenier wrote in an e-mail in the
days before he died that the Company “should not be dumping or blasting this ore
pass until the water situation is under control.” For reasons that require further
forensic investigation by appropriate authorities, and which the USW Investigation
Team was unable to ascertain because of non co-operation by Vale management
officials, the double guardrails were removed under management’s directions and
re-installed up to 3 times over the course of 2 days. It appears that this was done to
allow miners to continue to dump wet ore into the #7 ore pass. The company has
provided no explanation for the removal of the double guard rails which Jason
Chenier , a supervisor at the time of his death, had erected as a safety measure. (pg.
83/USW Report)
Crash Gate Station: The design of the by-pass station at the 3000 level put Jason
Chenier and Jordan Fram in immediate harm’s way from a run of muck incident. The
4
company had installed no cameras to allow them to view and operate the crash gate
from a safe distance. The crash gate at the station was not designed to close
automatically. This means that if a miner needed to leave the area quickly, the crash
gate would remain open, and material would continue to flow. Miners also had no
way of leaving; there was no second exit. (Pg. 90/USW Report)
This danger involving the type of location where Jason Chenier and Jordan Fram
were apparently undertaking a hazardous task was noted in the Inquest Report into
the 1995 death of Stobie miner Clifford Bastien.
The USW Report notes that this is a violation of mining regulations. (pg. 90/USW
Report)
Health and Safety Requirements:
Clifford Bastien Inquest: Following the death of Clifford Bastien in a similar run of
muck accident in 1995 at Stobie Mine, a coroner’s jury made 33 recommendations.
Six of these addressed the issue of reducing the threat of another fatal run of muck
accident.
The fact is that there have been at least six (6) other run of muck incidents at the
Stobie Mine in the period 2005 to 2011, the six years before the deaths of Jason
Chenier and Jordan Fram. (pg. 69&74/USW Report)
All Mine Standards: The All Mine Standards, the Ontario Occupational Health and
Safety Act and Regulation 854 of the OHSA, establish the legal requirements for
workplace health and safety in mines. The company failed to meet these
requirements by allowing excess water to accumulate and by failing to provide a
training package that addressed the safe operation of the crash gate at the #7 ore
pass. (Pg. 122/USW Report)
Management failed to follow the legal requirements of OHSA when a worker refused
to work because of unsafe conditions. Workers who were told to blast suspended
material hung-up in the #3715 ore pass were NOT told other workers had refused
to do such work. (Pg. 125/USW Report)
All miners working at Stobie were given a two-day training program. Only one
bullet point in the two PowerPoint presentations dealt with the danger of run of
muck incidents. (Pg. 112/USW Report)
079 Form: When an unsafe working condition is reported, company procedures
require the completion of what is known as a “079 form.” After the lengthy
2010/2011 labour dispute, workers and the Joint Health and Safety Committee have
been denied the right to initiate 079 forms and know that their health and safety
concern/complaint would be filed and addressed by management. The filing of such
a complaint is now done at the “discretion” of the supervisor. In addition, when
5
interviewed during the Local 6500 investigation, many miners reported that they
were and are discouraged from reporting hazards. Miners recounted that when they
did report hazards, this was not logged on 079 forms. Miners reported having fears
of retaliation for raising health and safety concerns. This reflects a “culture issue”
that requires further investigation and positive steps to redress. (Pg. 57/USW
Report)
SafeProduction: Vale’s safety program is known as SafeProduction. It purports to
ensure that management is accountable for preventing injuries, and that employee
involvement is essential. Unlike the 079 form processes, there is no process under
SafeProduction to ensure a hazard is communicated to others. (Pg. 105/USW
Report)
Hazard Alerts communiqués are issued as a warning of hazards that have been
identified. There were no Hazard Alert warnings issued in relation to the water
conditions that developed at the time of the June 2011 double fatality. Management
has provided no explanation for this failure. (Pg. 100/USW Report)
After the June 2011 tragedy, a USW Local 6500 Worker Representative requested
the issuance of a Hazard Alert, but his request was denied by Vale (Pg. 59/USW
Report).
Joint Health and Safety Committee: In the months immediately before the June
2011 double fatality, the worker representatives on the JHSC raised concerns about
stuck drain holes, hang-ups, sticky muck and the excessive accumulation of water.
The company failed to address these concerns prior to the deaths of Jason Chenier
and Jordan Fram. (Pg. 114/USW Report)
Supervisors Log Book: The Supervisor Log Book was not being used as is intended
by applicable mining regulations. On June 6, 2011, Supervisor Jason Chenier tried to
enter his concerns about the danger of a run of muck incident in the safety section of
the Supervisor’s log book. There was no room, because the safety section was filled
with previously reported safety concerns. Chenier was forced to send two e-mails to
management instead. (Pg. 106, USW Report)
Wet-Dry Measurements: Given the excessive water accumulation on the levels
immediately above the 3000 level, wet and dry measurements were required to be
taken at both the #7 ore pass and #3715 ore pass. A wet measurement would
quantify the amount of water in the ore mixture, show if there was water
accumulation in the ore passes, and alert supervisors and management to the
possibility of a run of muck incident. The wet and dry measurements are supposed
to be recorded and communicated.
No such wet measurements were found in the daily shift log for the year previous to
the fatalities. No explanation for this omission has been provided by Vale. (Pg.
35/USW Report)
6
Criminal Code Offences
The Westray Bill, also known as Bill C-45, amended the Criminal Code of Canada in
2004 and placed an occupational health and safety duty on individuals,
organizations and their decision-makers across Canada.
Among other changes, the Westray Bill made workplace negligence a criminal
offence by adding a new duty on organizations and individuals to take reasonable
steps to prevent bodily harm and death. Not acting to protect health and safety
became a violation of the Criminal Code of Canada.
The USW Local 6500 investigation into the June 2011 double fatality at Vale’s Stobie
Mine has revealed a failure to manage water conditions and other potential hazards
in the underground workplace environment and an overall failure to abide by and
implement provincial and internal safety requirements. These failures demonstrate
a wanton and/or reckless disregard for the lives and safety of those working in
Vale’s mines, in addition to demonstrating that Vale and its managerial officials and
representatives failed to take all reasonable steps to prevent bodily harm and death.
Recommendations
After eight months of research and interviews, the investigation team of Local 6500
of the United Steelworkers has made 165 separate recommendations to improve the
safety and working conditions at Vale’s Stobie Mine, and by extension at all of Vale’s
mines in the Sudbury Basin and at all underground mines throughout Canada. (pg.
147/ USW Report)
The recommendations include:
• That the Government of Ontario establish a Public Inquiry into the causes of
the fatalities at the Stobie Mine, and more generally into underground mine
safety in Canada, with special emphasis on water management issues,
monitoring and enforcement. There have been substantial changes to mining
processes since the last significant Ontario/Canada health and safety inquiry
30 years ago.
• That Ontario’s Assistant Deputy Attorney General – Criminal Law take
immediate steps to determine whether charges under the “Westray”
provisions of the Criminal Code of Canada should be laid against company
officials. The review would consider the USW Report’s findings and
undertake further investigation, as Crown Attorneys and police authorities
consider necessary.
• That a Committee be appointed by the Ontario Minister of Labour to review
whether the Occupational Health and Safety Act and that Act’s enforcement
7
provisions are adequately safeguarding the safety of workers employed in
underground mines and surface mining plants in Ontario.
• 78 recommended changes to health and safety rules at the Stobie Mine, to
ensure, among other things, that Hazard Alerts are initiated without fear of
reprisal and that workers have the protected right to file “079 forms” without
interference or intervention by Vale.
• 27 recommended changes respecting the use of ore passes at the Stobie
Mine, including an absolute and enforceable obligation ending the practice of
dumping of wet muck into any ore pass, such as the #3715 and #7 ore
passes.
• 16 recommended changes to water drainage practices, including the
monitoring and elimination of hazardous water conditions such as occurred
on the 2400, 2450, 2600 and 2800 levels at Stobie Mine in June 2011.
• 16 recommended improvements to blasting procedures, including
developing, implementing and enforcing new techniques for the sealing of all
drill holes into ore passes.









![[XLS] and Construction... · Web view36 6500 30 3000 9 36 6500 62 4500 42 6500 37 3000 19 17 36 6500 42 6000 19 17 41 6500 36 3000 14 11 31 6500 33 6000 10 8 33 6500 31 3000 10 8](https://img.pdfslide.net/doc/110x75/5aaaff237f8b9a8f498b52b0/xls-and-constructionweb-view36-6500-30-3000-9-36-6500-62-4500-42-6500-37-3000.jpg)






















