Embed Size (px)
Citation preview

Validation of a novel mutation screening strategy for Familial
Hypercholesterolaemia: LIPOchip®, a DNA-array based
system
Jonathan CallawayWessex Regional Genetics Laboratory

Familial Hypercholesterolaemia (FH)
• Autosomal dominant disorder of lipid metabolism
• Heterozygous prevalence in UK population of 1 in 500
• Characterised by:– Raised serum LDL-c (low density lipoprotein cholesterol)– Tendon and skin xanthomata (due to cholesterol deposits)– Premature coronary heart disease
• Early diagnosis is beneficial to patients since treatment with lipid-lowering therapy (e.g. statins) can result in a near-normal life expectancy by lowering the risk of coronary heart disease
• Homozygous FH exists but is rare– Prevalence of 1 in a million– Symptoms more severe: appear in childhood and often lead to early
death from coronary heart disease

Genes implicated in FH
• FH is a genetically heterogeneous disorder
• Mutations which cosegregate with the disease have been found in at least three genes:
– LDLR (low density lipoprotein receptor)
• Over 1000 mutations spread throughout gene• Exonic deletions and duplications (5-10% FH cases)
– APOB (apolipoprotein B)
• 9 mutations– PCSK9 (proprotein convertase subtilisin/kexin type 9)
• 6 mutations
• Most mutations identified are in LDLR (~79%) with lower proportion in APOB (~5.5%) and PCSK9 (~1.5%)

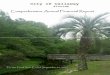
LDL-receptor pathway
LDL-receptor pathway maintains intracellular cholesterol homeostasis
Cholesterol synthesis
LDL-c
LDLR
ApoB-100 protein
Lipid core of cholesterol esters
? PCSK9
LDLR synthesis

Current FH testing strategy
• FH20 Elucigene ARMS kit (Tepnel Diagnostics)– Identifies 20 most common mutations in UK
population– Sensitivity of only 40%
• NICE guidelines recommend DNA testing be used to confirm a diagnosis of FH (March 2009)
• Need for an increase in testing sensitivity

LIPOchip® • A DNA array-based system designed by Progenika
• Used as the primary testing strategy for FH in Spain
• Detection of 251 common FH point mutations– 242 LDLR, 3 APOB, 6 PCSK9
• Copy number variation detection in LDLR
• Currently targeted towards Spanish population within which the manufacturers claim a sensitivity of 80%
• 4 FH20 mutations are not detected by Spanish version– FS206, K290RfsX20, Q363X, C656R
• British version is under development– June 2010 availability– Sensitivity of 80-85%– Probe sets for the 4 missing FH20 mutations

LIPOchip®: DNA-array technology1. Multiplex PCR amplification2. Product fragmentation3. Labelling with biotin4. Hybridization and washing
- Using Tecan 4800 HS Pro station - Addition of Cy3-streptavidin (fluorochrome)
5. Results analysis- Using Agilent scanner and customised software
Laser
Light
Cy3-streptavidin
Biotin
Fragmented PCR product

A scanned LIPOchip® slide
• 2 pairs of oligonucleotides per mutation:– Each pair consists of a WT probe and a mutant probe– Signal intensity ratios calculated for WT / (WT+Mut)
• Controls for hybridization process and for measuring background signal noise
• Copy number variation detection controls

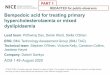
Graphical display of results generated by LIPOchip® software
Normal
Homozygous mutant
Heterozygous WT/mutant

Validation Strategy• 48 LIPOchip® slides were provided by Progenika to validate the
technology
• Maximum of 12 samples per run - in order to perform copy number detection two of these must be normal male & female controls
• Samples selected for validation:– 10 normal controls– 6 FH20 positive controls– 22 FH20 negative patients
• Criteria for selection of FH20 negative patients:– ‘Definite FH’ on referral card; or– High cholesterol level (over 8 mmol/L) plus either
(i) Family history of high cholesterol; or(ii) Family history of cardiovascular disease

Results from Validation• Normal controls:
– 9/10 slides passed quality control– No point mutations were detected
• FH20 positive controls:– 6/6 mutations correctly called by LIPOchip®
• FH20 negative patients:– 2 pathogenic LDLR missense mutations:
• c.1796T>C (p.Leu599Ser)• c.1618G>A (p.Ala540Thr)
– 1 unclassified LDLR variant:• c.2177C>T (p.Thr726Ile)…likely non-pathogenic by in-silico
analysis– Mutations were confirmed by direct sequencing

Problem 1: The M064 probe set
• c.91G>T (p.Glu31X)• ‘No Call’ result was frequently
obtained:– 7/9 normal controls– 3/6 positive controls– 20/22 FH20 negative patients
• Signal intensity values extended beyond the normal distribution parameters although they were still distinct from the mutation range
• Progenika are aware of this problem and hope to resolve it in the forthcoming British version
Normal

Problem 2: Copy number variation detection
7/9 normal controls appeared to have a deletion of the LDLR promoter and exon 1
Normal LDLR gene dosage Apparent deletion of promoter + exon 1

Problem 2: Copy number variation detection
Also, poor quality dosage data was often generated…
These issues raised the question as to whether LIPOchip® could be used in our laboratory for reliable copy number variation detection

Traditional Full Screen
• Testing strategy– Combination of dHPLC and direct sequencing
of LDLR gene– MLPA for dosage analysis of LDLR gene
(MRC-Holland kit P062-C1)
• Samples: – 10 normals from the validation– 22 FH20 negative patients tested using
LIPOchip®

Results from Traditional Full Screen
• The 2 pathogenic LDLR mutations and the unclassified LDLR variant identified by LIPOchip® were confirmed
• 2 further pathogenic LDLR mutations and an additional unclassified variant were detected:– c.1061A>T (p.Asp354Val)– c.1067delA (p.Ala356ValfsX14)– c.2479G>A (p.Val827Ile)…undecided pathogenicity by in-silico
analysis
• MLPA did not detect any deletions or duplications in the LDLR promoter or exonic regions of patients or controls

Possible Stratified Testing Approach for FH
FH20 – 40% sensitivity
Full screen with dHPLC and sequencing plus MLPA – 99.9% sensitivity
Full screen with dHPLC and sequencing
?
LIPOchip® - possibly 80-85% sensitivity (currently need to use MLPA in addition)

Implementation of LIPOchip®?
Sensitivity : Cost Ratio
Full screen LIPOchip®

Conclusions• LIPOchip® can be reliably used to detect common FH
point mutations with an increase in testing sensitivity
• Currently MLPA is required as a necessary complement to LIPOchip® testing
• Some mutations detected by LIPOchip® require further investigation regarding their pathogenicity using in-silico analysis
• Additional validation work is needed on the British version of LIPOchip®, when available
• Costing is an issue for LIPOchip® and will influence the decision on whether or not to use the technology in a diagnostic setting

Acknowledgements
• Wessex Regional Genetics Laboratory:– Oliver Wood– Esta Cross– Alison Skinner– Dr John Harvey
• Progenika:– Dr Xabier Abad Lloret– Maximiliano Crosetti





![Assessment report · lipoprotein (a) [Lp(a)] in patients with homozygous familial hypercholesterolaemia (HoFH) and in patients with severe heterozygous familial hypercholesterolaemia](https://img.pdfslide.net/doc/110x75/5e32b9f8d3afcb53c94a2775/assessment-report-lipoprotein-a-lpa-in-patients-with-homozygous-familial-hypercholesterolaemia.jpg)