Embed Size (px)
Citation preview
ORIGINAL ARTICLE
Validation of a Persian version of the Fibromyalgia ImpactQuestionnaire (FIQ-P)
Ali Bidari • Morteza Hassanzadeh •
Mohamad-Farzam Mohabat • Elham Talachian •
Effat Merghati Khoei
Received: 18 July 2013 / Accepted: 11 October 2013 / Published online: 29 October 2013
� Springer-Verlag Berlin Heidelberg 2013
Abstract The aim of this study is to translate, adapt, and
validate a Persian version of the Fibromyalgia (FM) Impact
Questionnaire (FIQ-P). The FIQ-P was adapted following the
translation and back-translation approach; then, it was
administered to thirty females with FM. Participants also
completed two other validated questionnaires, the Medical
Outcome Survey Short Form-36 (SF-36) and the Beck
Depression Inventory (BDI). Internal consistency within the
FIQ-P items and its test–retest reliability were assessed with
Cronbach’s alpha and Spearman’s correlation coefficient,
respectively. Construct validity was analyzed by Spearman’s
r when correlating the FIQ-P to other questionnaires. The
translated version was concordant. Adaptation affected two
sub-items of physical function. Participants’ mean
age ± standard deviation was 40.4 ± 9.0 years. Internal
consistency proved good with a = 0.80. Test–retest coeffi-
cient ranged from 0.50 for the item ‘‘work days missed’’ to 0.79
for all FIQ-P items. Fair and statistically significant (P \ 0.01)
correlations were found between the FIQ-P items and two
other questionnaires, SF-36 (r = -0.57) and BDI (r = 0.53).
We concluded that the FIQ-P is a valid and reliable instrument
for measuring health status of Persian-speaking FM patients.
Keywords Fibromyalgia Impact Questionnaire �Validation studies � Persian � Iran
Introduction
Fibromyalgia (FM) is a common clinical entity that affects
2–3 % of population and is characterized by widespread
body pain as the pivot symptom, as well as other somatic
complaints including fatigue, anxiety, non-restorative
sleep, and cognitive problems [1–7].
The FM syndrome is of major interest for exerting sig-
nificant impact on general health status and activity of
daily living in affected patients [8]. Clinical tools to mea-
sure the consequences of FM in personal and social life of
patients are critical for clinical, epidemiological, and out-
come studies and are useful for following the response to
treatment interventions [9].
For FM syndrome, there are several outcome measure
questionnaires, validated in English language, which are
employed to assess different aspects of overall health and
function of the patients [10]. The Arthritis Impact Mea-
surement Scale (AIMS) [11], the Health Assessment
Questionnaire (HAQ) [12], the Medical Outcome Survey
Short Form-36 (SF-36) [13], and the Fibromyalgia Impact
Questionnaire (FIQ) [14] are among many widely accepted
instruments [15].
A. Bidari
Department of Rheumatology, Iran University of Medical
Sciences, Tehran, Iran
M. Hassanzadeh
Department of Internal Medicine, Iran University of Medical
Sciences, Tehran, Iran
M.-F. Mohabat
Medical Laser Research Center, Iranian Center for Medical
Laser (ICML), Academic Center for Education, Culture and
Research (ACECR), Tehran, Iran
E. Talachian
Division of Pediatric Gastroenterology, Iran University of
Medical Sciences, Tehran, Iran
E. M. Khoei (&)
Brain and Spinal Cord Injury Research Center (BASIR), Iranian
National Center of Addiction Studies (INCAS), Tehran
University of Medical Sciences, Buiding No. 486, Ghazvin
Square, South Karegar Street, Tehran, Iran
e-mail: [email protected]
123
Rheumatol Int (2014) 34:181–189
DOI 10.1007/s00296-013-2883-0

As a protean clinical condition, FM is modulated by
many environmental, genetic, and epidemiological factors
[16], mandating field research in different geographical and
cultural settings. Correspondingly, translation and valida-
tion of standardized questionnaires is essential for the best
evidence-based practice in various societies.
The FIQ, as the most widely used outcome measure tool
for FM, was first developed by Burckhardt et al. [14]. It has
been translated into many languages, and the Arabic [17],
Dutch [18], French [19], German [20], Italian [21], Japa-
nese [22], Spanish [23], Swedish [24], Korean [25], and
Turkish [26] versions proved to have psychometric prop-
erties, validity, and reliability that are comparable to the
original version.
In order to join this international development, we
designed this study to make a Persian version of the FIQ
(FIQ-P) and to evaluate its validity and reliability for being
used in a Persian-speaking population.
Materials and methods
Patient selection
Study subjects were recruited from FM cases attending the
pain clinic at Medical Laser Research center, Iranian
Center for Medical Laser (ICML), Academic Center for
Education, Culture and Research (ACECR), Tehran, Iran.
All enrolled patients were females, aged between 18 and
65 years, who fulfilled the American Colleague of Rheu-
matology (ACR) 1990 classification criteria for FM [27].
Patients were excluded if they were pregnant or physically
handicapped or if there was any associated medical prob-
lem (e.g., inflammatory rheumatic diseases, other painful
conditions, or known malignancy).
Making FIQ-P
Translation
The original FIQ [14] was translated from English into
Persian by a bilingual linguist. Then, a panel composed of
two rheumatologists, two general practitioners, and an
experienced specialist in designing questionnaires, reached
a consensus about the terms used in the translated text; so
the initial Persian draft of the FIQ was generated. After
that, we had our initial Persian version back-translated into
English by another bilingual linguist who had no previous
knowledge about the questionnaire.
Adaptation
We administered the initial Persian version to a pilot group
of patients with FM to evaluate the areas of potential
comprehension difficulty and assess the need for cultural
adaptation. After making some modifications according to
the results of the pilot study, we obtained a definitive
Persian version of FIQ (FIQ-P) (see ‘‘Appendix’’). This
version again back-translated into English by another
blinded bilingual linguist, and then, it was evaluated in
term of concordance with the original FIQ.
Study questionnaires and measures
FIQ [14]
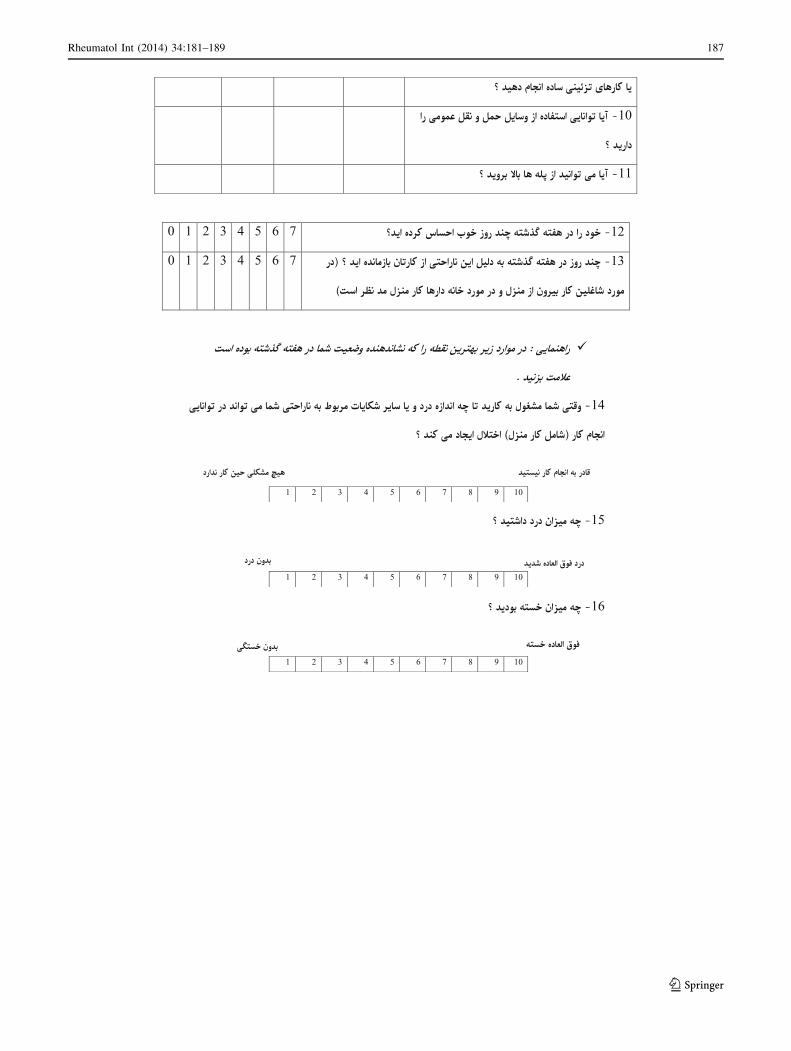
The FIQ is composed of 10 items. The first item contains
questions related to daily activities, each are rated in a 4-point
Likert type scale from 0 (always able to do) to 3 (never able to
do). The scores are summed and divided by the number of
rated items to yield a score between 0 and 3 for physical
functioning. Items 2 and 3 are about the number of days the
patient felt well (0–7) or was unable to work (including
housework) because of FM symptoms over the last week
(0–7), respectively. Item 2 is scored inversely, so that a higher
score means greater impairment (i.e., 0 days = 7, 1 day = 6,
2 days = 5, etc.); but item 3 is scored directly (i.e.,
0 days = 0, 1 day = 1, 2 days = 2, etc.). Item 4 through 10
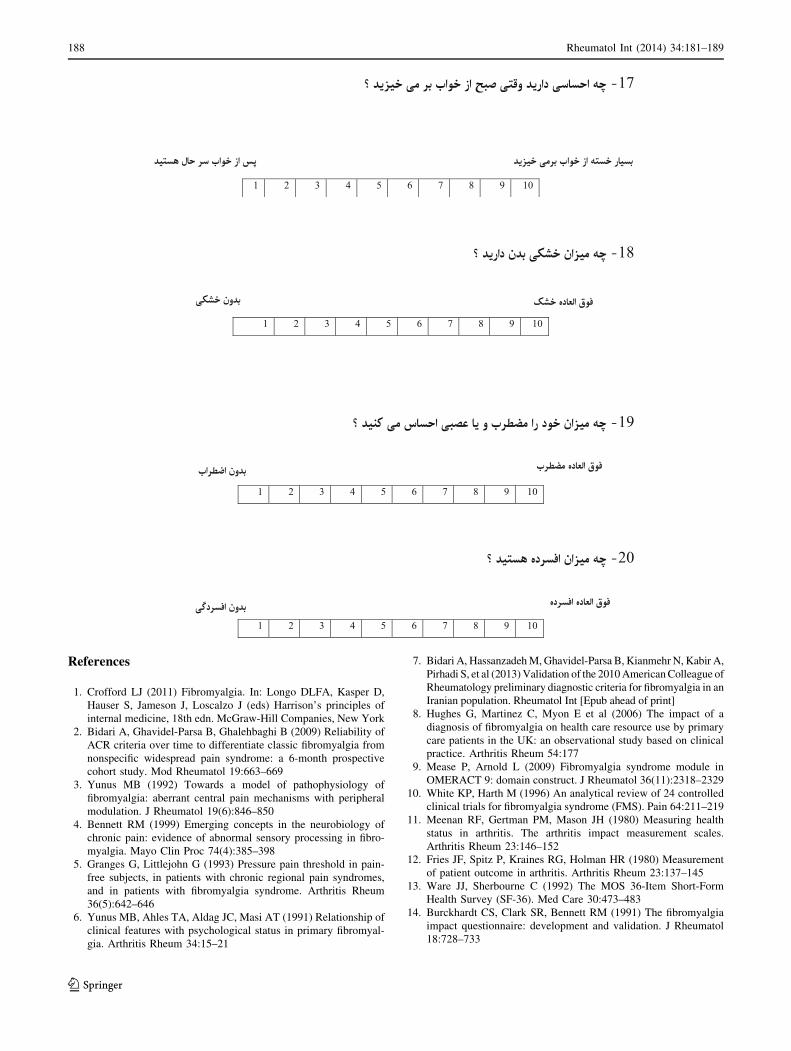
contain 100 mm visual analogue scales on which the patients
rate their pain, fatigue, stiffness, morning tiredness, difficulty
to do job, anxiety, and depression. After initial scoring is
obtained, each of the resulting scores is standardized on a
0–10 scale, with higher scores indicating more impairment.
SF-36 questionnaire [13]
As a health-related quality of life questionnaire, the SF-36
consists of 36 questions categorized in 8 domains: general
health, mental health, role physical, role emotional, phys-
ical function, social function, bodily pain, and vitality.
Each domain may reach a standardized score between 0
and 100, with higher scores indicating better status. It also
contains one more question about change in health during
the past year, rated in a Likert format scale. In this study,
we used the validated Persian version of the SF-36 [28].
We hypothesized that individuals with higher SF-36 score
would have lower levels of fibromyalgia impairment and
lower FIQ scores.
Beck Depression Inventory (BDI) [29]
This is a self-reported questionnaire that measures patient’s
level of depression. The obtained score ranges from 0 to
63. We used the Persian version of the BDI validated
elsewhere [30]. Individuals with higher BDI score were
hypothesized to take higher FIQ score owing to more
impairment by fibromyalgia.
182 Rheumatol Int (2014) 34:181–189
123

Tender point examination
An expert rheumatologist (AB) performed a dolorimetry
examination on each patient. Any of the 18 standard body
points, defined by the ACR 1990 criteria [27], were
examined by a dolorimeter with gradual increasing the
pressure at rate of about 1 kg/cm2/s. If pain was elicited
with pressures less than 4 kg/cm2, the point was considered
to be tender.
Study protocol
All eligible patients were received sufficient information
about objectives of the study, and those who completed a
written consent form were recruited.
At first visit, demographic data were obtained from all
enrolled subjects; they completed the FIQ-P as well as
other study questionnaires and underwent dolorimetry
examination. After 7 days, patients came back to the same
clinic for a second visit and completed another FIQ-P as
the retest measure. During the week, no new therapeutic
intervention was introduced.
Statistical analysis
Data were analyzed using the software SPSS version 20.0.
Descriptive statistics were calculated, and results were
expressed, where applicable, as proportions and mean with
standard deviation (SD). The internal consistency for items of
the FIQ-P was measured with Cronbach’s alpha coefficient.
The construct validity was computed by the Spearman’s
correlation coefficient (r) between the FIQ-P and the other
questionnaires. Test–retest reliability was calculated again by
using the Spearman’s coefficient. All statistical tests were
two tailed, and statistical significance was set at P \ 0.05.
Results
Demographics
The study sample consisted of 30 patients fulfilling the
ACR 1990 criteria for FM. The mean age (±SD) of par-
ticipants was 40.4 (±9.0) years, all of them were females.
Of the total of 30 enrolled subjects, 21 (70 %) were mar-
ried, 20 (66 %) were housekeeper, and education level of
24 (80 %) was diploma or higher. Table 1 summarizes
demographic characteristics of the study patients.
Results of cultural adaptation
After administering the initial Persian version of FIQ to a
pilot group of FM patients, some issues were noted and we
changed two sub-items of physical functioning for cultural
adaptation:
1. The ninth item, ‘‘Do yard work?’’, was coded by only
34 % of pilot FM patients, because people in Tehran
usually live in apartments; so we changed it to a more
applicable question in the definitive FIQ-P (see ‘‘Appen-
dix’’) which was back-translated as ‘‘Undertake flower
pot arrangements or simple decorative activities?’’.
2. The tenth item, ‘‘Drive a car?’’, was left blank by 83 %,
since the number of Iranian women (especially house-
keepers) who drive cars is less than Western countries.
Instead, using public transportation or transporting
services by women are more common in Iran. Thus, we
replaced the tenth item with another relevant question in
the final FIQ-P (see ‘‘Appendix’’) that was back-
translated as ‘‘Ability to use public transportation?’’.
Analysis of translation of final FIQ-P indicated it is
satisfactory and concordant for most of the questions, and
the translators considered none of the back-translated
questions as vague or doubtful. When comparing the ori-
ginal FIQ and the back-translation of FIQ-P, only two
differences were found, both stem from the cultural adap-
tations in sub-items 9 and 10.
Reliability and internal consistency of the FIQ-P
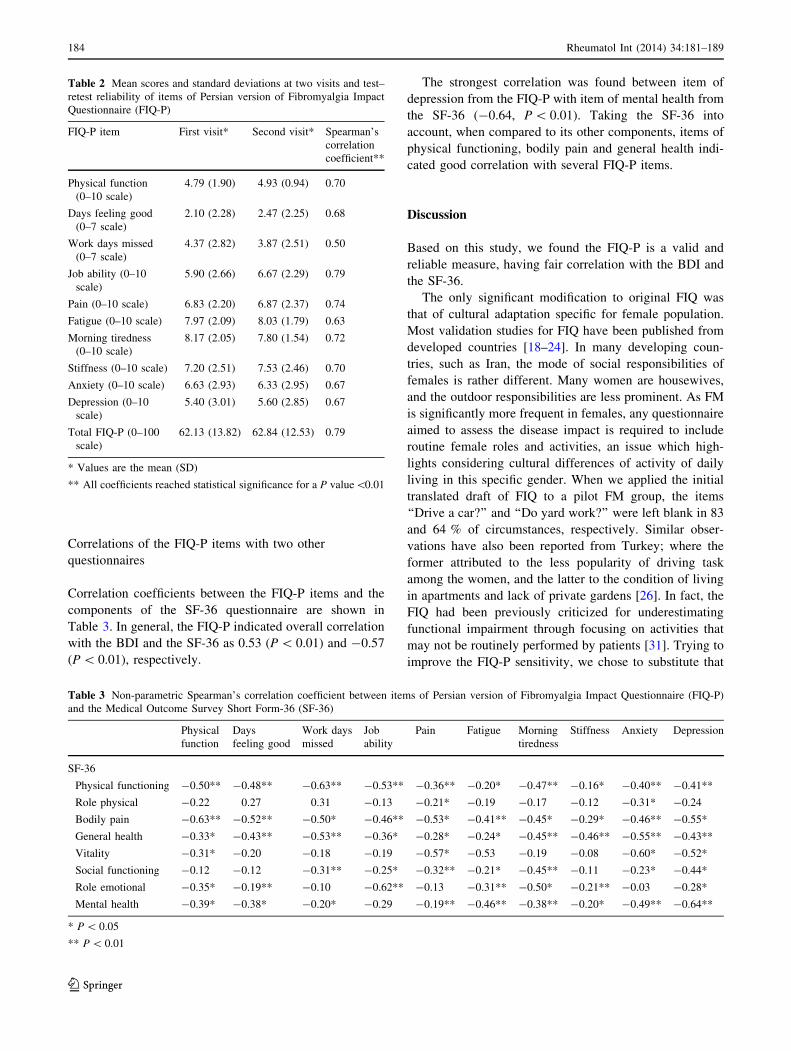
The mean (±SD) of FIQ-P items at baseline and at the
second visit, as well as results of test–retest analysis is
presented in Table 2. Analysis of reliability indicated
correlation coefficients between the test and retest varying
from 0.50 for work days missed to 0.79 for Job ability and
total FIQ-P items (Table 2). Furthermore, an a coefficient
of 0.80 was obtained for internal consistency of the total
items of the FIQ-P.
Table 1 Demographic characteristics of 30 study females with
fibromyalgia
Age (years)* 40.4 ± 9.0
Marriage status**
Married 21 (70)
Single 3 (10)
Widow 6 (20)
Educations**
Under diploma 6 (20)
Diploma 16 (53.3)
Higher diploma 8 (26.6)
Work status**
Housekeeper 20 (66.6)
Working outdoor 10 (33.3)
* Value is the mean ± SD
** Values are the no. (%)
Rheumatol Int (2014) 34:181–189 183
123
Correlations of the FIQ-P items with two other
questionnaires
Correlation coefficients between the FIQ-P items and the
components of the SF-36 questionnaire are shown in
Table 3. In general, the FIQ-P indicated overall correlation
with the BDI and the SF-36 as 0.53 (P \ 0.01) and -0.57
(P \ 0.01), respectively.
The strongest correlation was found between item of
depression from the FIQ-P with item of mental health from
the SF-36 (-0.64, P \ 0.01). Taking the SF-36 into
account, when compared to its other components, items of
physical functioning, bodily pain and general health indi-
cated good correlation with several FIQ-P items.
Discussion
Based on this study, we found the FIQ-P is a valid and
reliable measure, having fair correlation with the BDI and
the SF-36.
The only significant modification to original FIQ was
that of cultural adaptation specific for female population.
Most validation studies for FIQ have been published from
developed countries [18–24]. In many developing coun-
tries, such as Iran, the mode of social responsibilities of
females is rather different. Many women are housewives,
and the outdoor responsibilities are less prominent. As FM
is significantly more frequent in females, any questionnaire
aimed to assess the disease impact is required to include
routine female roles and activities, an issue which high-
lights considering cultural differences of activity of daily
living in this specific gender. When we applied the initial
translated draft of FIQ to a pilot FM group, the items
‘‘Drive a car?’’ and ‘‘Do yard work?’’ were left blank in 83
and 64 % of circumstances, respectively. Similar obser-
vations have also been reported from Turkey; where the
former attributed to the less popularity of driving task
among the women, and the latter to the condition of living
in apartments and lack of private gardens [26]. In fact, the
FIQ had been previously criticized for underestimating
functional impairment through focusing on activities that
may not be routinely performed by patients [31]. Trying to
improve the FIQ-P sensitivity, we chose to substitute that
Table 2 Mean scores and standard deviations at two visits and test–
retest reliability of items of Persian version of Fibromyalgia Impact
Questionnaire (FIQ-P)
FIQ-P item First visit* Second visit* Spearman’s
correlation
coefficient**
Physical function
(0–10 scale)
4.79 (1.90) 4.93 (0.94) 0.70
Days feeling good
(0–7 scale)
2.10 (2.28) 2.47 (2.25) 0.68
Work days missed
(0–7 scale)
4.37 (2.82) 3.87 (2.51) 0.50
Job ability (0–10
scale)
5.90 (2.66) 6.67 (2.29) 0.79
Pain (0–10 scale) 6.83 (2.20) 6.87 (2.37) 0.74
Fatigue (0–10 scale) 7.97 (2.09) 8.03 (1.79) 0.63
Morning tiredness
(0–10 scale)
8.17 (2.05) 7.80 (1.54) 0.72
Stiffness (0–10 scale) 7.20 (2.51) 7.53 (2.46) 0.70
Anxiety (0–10 scale) 6.63 (2.93) 6.33 (2.95) 0.67
Depression (0–10
scale)
5.40 (3.01) 5.60 (2.85) 0.67
Total FIQ-P (0–100
scale)
62.13 (13.82) 62.84 (12.53) 0.79
* Values are the mean (SD)
** All coefficients reached statistical significance for a P value\0.01
Table 3 Non-parametric Spearman’s correlation coefficient between items of Persian version of Fibromyalgia Impact Questionnaire (FIQ-P)
and the Medical Outcome Survey Short Form-36 (SF-36)
Physical
function
Days
feeling good
Work days
missed
Job
ability
Pain Fatigue Morning
tiredness
Stiffness Anxiety Depression
SF-36
Physical functioning -0.50** -0.48** -0.63** -0.53** -0.36** -0.20* -0.47** -0.16* -0.40** -0.41**
Role physical -0.22 0.27 0.31 -0.13 -0.21* -0.19 -0.17 -0.12 -0.31* -0.24
Bodily pain -0.63** -0.52** -0.50* -0.46** -0.53* -0.41** -0.45* -0.29* -0.46** -0.55*
General health -0.33* -0.43** -0.53** -0.36* -0.28* -0.24* -0.45** -0.46** -0.55** -0.43**
Vitality -0.31* -0.20 -0.18 -0.19 -0.57* -0.53 -0.19 -0.08 -0.60* -0.52*
Social functioning -0.12 -0.12 -0.31** -0.25* -0.32** -0.21* -0.45** -0.11 -0.23* -0.44*
Role emotional -0.35* -0.19** -0.10 -0.62** -0.13 -0.31** -0.50* -0.21** -0.03 -0.28*
Mental health -0.39* -0.38* -0.20* -0.29 -0.19** -0.46** -0.38** -0.20* -0.49** -0.64**
* P \ 0.05
** P \ 0.01
184 Rheumatol Int (2014) 34:181–189
123

items with ‘‘Ability to use public transportation?’’ and
‘‘Undertake flower pot arrangements or simple decorative
activities?’’, more common social tasks among Iranian
women.
We found FIQ-P as a reliable tool over time, with
overall test–retest reliability of 0.79 when we administered
the questionnaire to sample cases 1 week apart (ranging
from 0.50 for ‘‘work days missed’’ to 0.79 for ‘‘job abil-
ity’’). The reliability of the original FIQ in English had
been ranged from 0.56 on the pain score to 0.95 for
physical function [32]. The internal consistency of the FIQ-
P also proved good with Cronbach a of 0.80 for all items.
Although higher alphas have been reported from developed
countries [18–24], studies from developing eastern coun-
tries found values of 0.80 or less [17, 25, 26]. In the ori-
ginal version of the FIQ, however, the internal consistency
had not been evaluated [32].
We did not recruit men with FM. No study has been
specifically analyzed the validity of FIQ in this sex group.
Taking this limitation into account, we are not able to
extrapolate the results of this validation study to the men.
The setting of our study was in an urban population. Fur-
ther studies are required to validate the questionnaire in
rural setting, where different social tasks are expected.
Finally, we used a minimum number of cases needed for a
validation study. Including more cases is recommended to
improve the power of future studies.
In summary, we introduced the first translated version of
FIQ into Persian language. The FIQ-P showed reliable and
valid performance in our selected FM Iranian patients and
could be of use for future follow-up and outcome studies in
Persian-speaking population.
Conflict of interest None.
Rheumatol Int (2014) 34:181–189 185
123
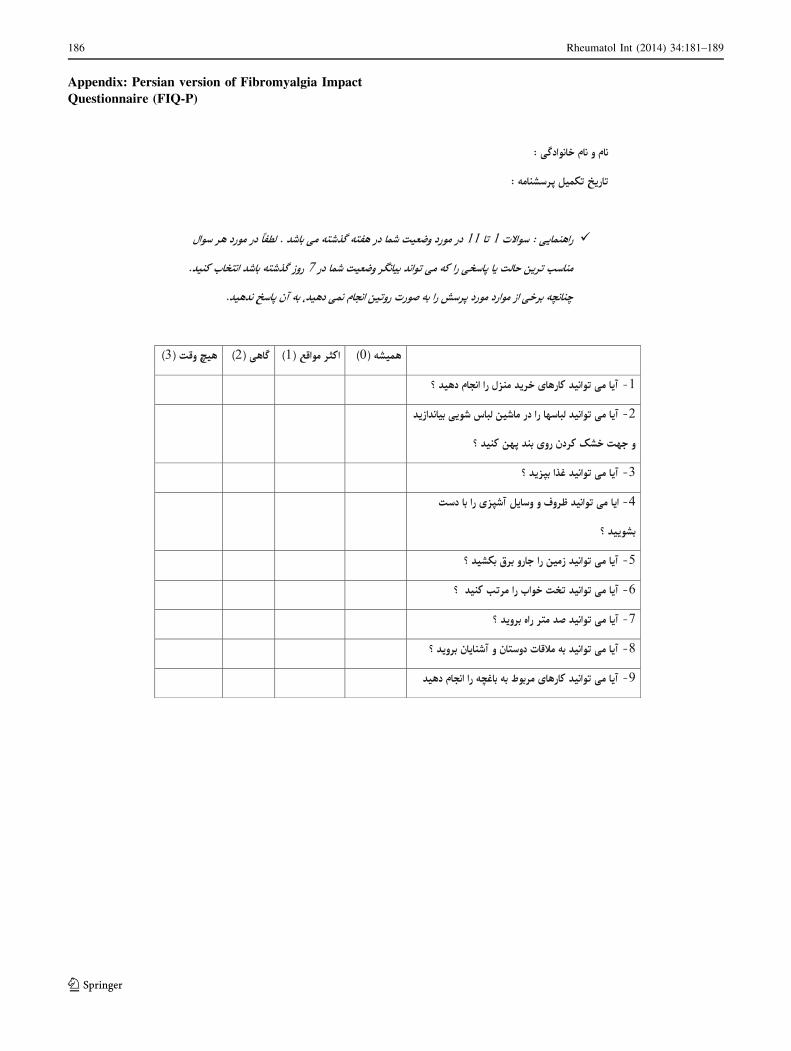
Appendix: Persian version of Fibromyalgia Impact
Questionnaire (FIQ-P)
186 Rheumatol Int (2014) 34:181–189
123
Rheumatol Int (2014) 34:181–189 187
123
References
1. Crofford LJ (2011) Fibromyalgia. In: Longo DLFA, Kasper D,
Hauser S, Jameson J, Loscalzo J (eds) Harrison’s principles of
internal medicine, 18th edn. McGraw-Hill Companies, New York
2. Bidari A, Ghavidel-Parsa B, Ghalehbaghi B (2009) Reliability of
ACR criteria over time to differentiate classic fibromyalgia from
nonspecific widespread pain syndrome: a 6-month prospective
cohort study. Mod Rheumatol 19:663–669
3. Yunus MB (1992) Towards a model of pathophysiology of
fibromyalgia: aberrant central pain mechanisms with peripheral
modulation. J Rheumatol 19(6):846–850
4. Bennett RM (1999) Emerging concepts in the neurobiology of
chronic pain: evidence of abnormal sensory processing in fibro-
myalgia. Mayo Clin Proc 74(4):385–398
5. Granges G, Littlejohn G (1993) Pressure pain threshold in pain-
free subjects, in patients with chronic regional pain syndromes,
and in patients with fibromyalgia syndrome. Arthritis Rheum
36(5):642–646
6. Yunus MB, Ahles TA, Aldag JC, Masi AT (1991) Relationship of
clinical features with psychological status in primary fibromyal-
gia. Arthritis Rheum 34:15–21
7. Bidari A, Hassanzadeh M, Ghavidel-Parsa B, Kianmehr N, Kabir A,
Pirhadi S, et al (2013) Validation of the 2010 American Colleague of
Rheumatology preliminary diagnostic criteria for fibromyalgia in an
Iranian population. Rheumatol Int [Epub ahead of print]
8. Hughes G, Martinez C, Myon E et al (2006) The impact of a
diagnosis of fibromyalgia on health care resource use by primary
care patients in the UK: an observational study based on clinical
practice. Arthritis Rheum 54:177
9. Mease P, Arnold L (2009) Fibromyalgia syndrome module in
OMERACT 9: domain construct. J Rheumatol 36(11):2318–2329
10. White KP, Harth M (1996) An analytical review of 24 controlled
clinical trials for fibromyalgia syndrome (FMS). Pain 64:211–219
11. Meenan RF, Gertman PM, Mason JH (1980) Measuring health
status in arthritis. The arthritis impact measurement scales.
Arthritis Rheum 23:146–152
12. Fries JF, Spitz P, Kraines RG, Holman HR (1980) Measurement
of patient outcome in arthritis. Arthritis Rheum 23:137–145
13. Ware JJ, Sherbourne C (1992) The MOS 36-Item Short-Form
Health Survey (SF-36). Med Care 30:473–483
14. Burckhardt CS, Clark SR, Bennett RM (1991) The fibromyalgia
impact questionnaire: development and validation. J Rheumatol
18:728–733
188 Rheumatol Int (2014) 34:181–189
123
15. Hawley DJ, Wolfe F (1991) Pain, disability, and pain/disability
relationships in seven rheumatic disorders: a study of 1,522
patients. J Rheumatol 18:1552–1557
16. Wolfe F, Ross K, Anderson J, Russell IJ (1995) Aspects of
fibromyalgia in the general population: sex, pain threshold, and
fibromyalgia symptoms. J Rheumatol 22:151–156
17. El-Naby MA, Hefny MA, Fahim AE, Awadalla MA et al (2013)
Validation of an adapted Arabic version of fibromyalgia syn-
drome impact questionnaire. Rheumatol Int 33(10):2561–2567
18. Zijlstra TR, Taal E, van de Laar MA, Rasker JJ (2007) Validation
of a Dutch translation of the fibromyalgia impact questionnaire.
Rheumatology (Oxford) 46:131–134
19. Perrot S, Dumont D, Guillemin F, Pouchot J, Coste J (2003)
Quality of life in women with fibromyalgia syndrome: validation
of the QIF, the French version of the fibromyalgia impact ques-
tionnaire. J Rheumatol 30:1054–1059
20. Offenbaecher M, Waltz M, Schoeps P (2000) Validation of a
German version of the Fibromyalgia Impact Questionnaire (FIQ-
G). J Rheumatol 27:1984–1988
21. Sarzi-Puttini P, Atzeni F, Fiorini T, Panni B, Randisi G, Turiel M,
Carrabba M (2003) Validation of an Italian version of the
Fibromyalgia Impact Questionnaire (FIQ-I). Clin Exp Rheumatol
21:459–464
22. Osada K, Oka H, Isomura T, Nakamura I, Tominaga K, Takah-
ashi S, Kojima A, Nishioka K (2011) Development of the Japa-
nese version of the Fibromyalgia Impact Questionnaire (JFIQ):
psychometric assessments of reliability and validity. Int J Rheum
Dis 14(1):74–80
23. Rivera J, Gonzalez T (2004) The Fibromyalgia Impact Ques-
tionnaire. A validated Spanish version to assess the health status
in women with fibromyalgia. Clin Exp Rheumatol 22:554–560
24. Hedin PJ, Hamne M, Burckhardt CS, Engstrom-Laurent A (1995)
The Fibromyalgia Impact Questionnaire, a Swedish translation of
a new tool for evaluation of the fibromyalgia patient. Scand J
Rheumatol 24:69–75
25. Kim YA, Lee SS, Park K (2002) Validation of a Korean version
of the fibromyalgia impact questionnaire. J Korean Med Sci
17:220–224
26. Sarmer S, Ergin S, Yavuzer G (2000) The validity and reliability
of the Turkish version of the Fibromyalgia Impact Questionnaire.
Rheumatol Int 20:9–12
27. Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C,
Goldenberg DL et al (1990) The American College of Rheuma-
tology 1990 criteria for the classification of fibromyalgia. Report
of the Multicenter Criteria Committee. Arthritis Rheum 33(2):
160–172
28. Motamed N, Ayatollahi AR, Zare N, Sadeghi-Hassanabadi A
(2005) Validity and reliability of the Persian translation of the
SF-36 version 2 questionnaire. East Mediterr Health J 11(3):
349–357
29. Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J (1961) An
inventory for measuring depression. Arch Gen Psychiatry
4:53–63
30. Ghassemzadeh H, Mojtabai R, Karamghadiri N, Ebrahimkhani N
(2005) Psychometric properties of a Persian-language version of
the Beck Depression Inventory, second edition: BDI-II-PER-
SIAN. Depress Anxiety 21(4):185–192
31. Wolfe F, Hawley DJ, Goldenberg DL, Russell IJ, Buskila D,
Neumann L (2000) The assessment of functional impairment in
fibromyalgia (FM): Rasch analyses of 5 functional scales and the
development of the FM Health Assessment Questionnaire.
J Rheumatol 27(8):1989–1999
32. Bennett R (2005) The Fibromyalgia Impact Questionnaire (FIQ):
a review of its development, current version, operating charac-
teristics and uses. Clin Exp Rheumatol 23(Suppl. 39):S154–S162
Rheumatol Int (2014) 34:181–189 189
123

























![[FIQ UNCP] Plan.curricular.2013](https://img.pdfslide.net/doc/110x75/55cf978c550346d03392414a/fiq-uncp-plancurricular2013.jpg)



