-
Validation study of a modern t
, BaNabil Wasif, M.D., F.A.C.S. , Victor J. Pizzitola, M.D. ,
Marina E. Giurescu, M.D. ,
aDepartment of Surgery, bDepar
KEYWORDS:Breast cancer;Nipple discharge;Treatment
algorithm;Validation study
d-
2014 Elsevier Inc. All rights reserved.
complaints. Previous studies have found a breast carcinoma there
is no clear guideline on what differentiates a benign
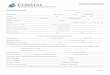
treatment algorithm (Fig. 1) for selectively identifying
pa-tients with nipple discharge who were at higher risk of
ma-lignancy and should undergo excision, whereas the othergroup had
low enough risk to undergo follow-up.14 The
There were no relevant financial relationships or any sources of
support
in the form of grants, equipment, or drugs.
The authors declare no conflicts of interest.
* Corresponding author. Tel.: 11-480-342-2849; fax:
11-480-342-2866.
The American Journal of Surgery (2014) -, --E-mail address:
[email protected] of 9.3% to 21.3% in women with
pathologicnipple discharge,210 but most only included patients
who
etiology from a malignancy based on clinical and radio-graphic
assessment.
For decades, patients with pathologic nipple dischargewere
counseled to undergo a duct excision.3,6,1013 Howev-er, in our
previous study,14 we proposed an evidence-basedNipple discharge is
a frequent presenting symptom,occurring in 3% to 10%1,2 of all
women with breast-related
underwent an operative excision.3,810 While nearly 90%of women
with nipple discharge have benign disease,10graphic findings and
clinical examination for safe clinical follow-up. Most will have
resolution avoiing a surgical procedure.Manuscript received July
23, 2013;
2013
0002-9610/$ - see front matter
2014http://dx.doi.org/10.1016/j.amjsurg.20tment of Radiology, Mayo
Clinic, 5777 E. Mayo Blvd, Phoenix, AZ, USA
AbstractBACKGROUND: Nipple discharge occurs in 2% to 5% of
women. We evaluated the effectiveness of a
previously proposed treatment algorithm for these
patients.METHODS: Patients with pathologic nipple discharge and a
negative mammogram and subareolar
ultrasound were offered follow-up from 2005 to 2011 according to
the algorithm.RESULTS: A total of 192 patients, mean age 56 years,
were studied. Risk of carcinoma among the
entire cohort was 5%. Breast surgeon was consulted for 142 (74%)
patients: 48 (34%) underwent initialsubareolar excision and 94
(66%) were clinically followed. The rate of carcinoma was 17%
(8/48) afterinitial subareolar excision, 0% (0/13) for those
without imaging abnormalities, 23% (8/35) with imag-ing
abnormalities, and 1% (1/94) with clinical follow-up. Of patients
who underwent follow-up, 21% (n5 20) underwent subareolar excision
because of imaging abnormality (n 5 1, 1%) or persistentdischarge
(n 5 19, 20%). Most patients had ductal carcinoma in situ (n 5 5,
56%).
CONCLUSIONS: Patients with nipple discharge can be prospectively
identified based on radio-Richard J. Gray, M.D., F.A.C.S.a,*for
nipple discharge
Awais Ashfaq, M.D.a, Derek Senior, B.S.aarevised manuscript
November 4,
Elsevier Inc. All rights reserved.
13.12.035reatment algorithm
rbara A. Pockaj, M.D., F.A.C.S.a,b bgoal of this study was to
validate the proposed treatmentalgorithm after its implementation
in our practice.
-
f nip
The American Journal of Surgery, Vol -, No -, - 2014Methods
Figure 1 Algorithm for the treatment o
2All patients with the presenting symptom of nippledischarge
from 2005 to 2011 at a single institution wereidentified through a
database of electronic medical records,breast clinic complaints,
and billing records after the studywas approved by the
Institutional Review Board. Theelectronic medical records system
was queried for thephrases nipple discharge and breast discharge
withinany clinical note and for any patients with an
InternationalClassification of Diseases, Ninth Revision code
diagnosisof 611.79 (discharge nipple, discharge breast) to
identifythe cohort of patients. Thus, all patients treated for
nippledischarge after institution of the nipple discharge
manage-ment algorithm in our practice were reviewed for manage-ment
compliance and outcome.
The same treatment algorithm was followed by allsurgeons
practicing at our institution. Patients with patho-logic discharge
(defined as spontaneous, bloody, or serousdischarge from a single
duct), an otherwise benign physicalexamination, and a negative
mammogram and subareolarultrasound were offered clinical follow-up
according to thealgorithm.
Results
A total of 192 patients with nipple discharge wereidentified.
Data on whether the discharge was unilateral orbilateral were
available for 100% of the patients, whetherthe discharge was
spontaneous in 94%, characteristics of
ple discharge. Derived from Gray et al.14the discharged fluid in
98%, and single versus multiple ductdischarge in 81% of
patients.
Two patients were male and 190 patients were female(Table 1).
The mean age of the patients was 56 years (range19 to 94).
Unilateral nipple discharge was present in 77%, itwas spontaneous
in 72%, the discharge was bloody in 34%,and clear/serous in 43%.
Single duct discharge was presentin 69% of patients for whom this
information was available.
Radiologic imaging was performed in all patients.Mammography was
performed in 177 patients (92%) andin all patients aged 30 or
greater. Mammographic abnor-malities (defined as a mass,
indeterminate/suspiciouscalcifications, or architectural
distortion) were present in13 (7%) patients. Ultrasonography was
performed in 149patients (78%). Sonographic abnormalities (defined
as a
Table 1 Patient demographics and characteristics ofdischarge
Variables n (%)
Median age (years) 56 (1994)Female 190 (99%)Discharge
characteristics
Unilateral 148 (77%)Spontaneous 138 (72%)Single duct 132
(69%)Bloody 65 (34%)Clear/serous 83 (43%)
-
mass or intraductal mass(es)) were present in 46 (24%)patients.
Ductography was performed in 13 patients (7%).Ductographic
abnormalities (duct cutoff or filling defect)were present in 9
(64%) patients. Of the 9 patients who hadductogram abnormalities, 3
had intraductal papillomas, 3had duct ectasia, 2 had ductal
hyperplasia, and 1 had ductalcarcinoma in situ. Breast magnetic
resonance imaging(MRI) was performed in 8 patients (4%).
Abnormalitieson MRI (defined as a mass or suspicious
enhancementpattern) were present in 4 patients (50%). The single
MRIthat failed to identify a carcinoma was performed at another
institution and while it was of good quality, limitedsequence
imaging was provided to us for analysis. Thesensitivity and
specificity of these radiologic procedures arepresented in Table 2.
Each patient with an imaging abnor-mality had tissue sampling
performed.
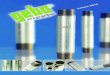
There were 142 (74%) patients who were evaluated by abreast
surgeon and the remaining 50 patients were seen byprimary care
physicians alone (Fig. 2). No patient who wasnot referred to a
breast surgeon developed breast cancerafter mean and median
follow-up of 25 and 17 months,respectively. Among patients
consulting a surgeon, a biopsy
Table 2 Sensitivity and specificity of radiologic procedures in
detecting carcinoma
Examination Total number of patients Sensitivity Specificity
Positive predictive value
Mammography 177 2/9 (22%) 157/168 (94%) 2/13
(15%)Ultrasonography 149 8/8 (100%) 102/140 (73%) 8/46
(17%)Ductography 13 1/1 (100%) 4/15 (33%) 1/9 (11%)Magnetic
resonance imaging 8 1/2 (50%) 4/7 (57%) 1/4 (25%)
A. Ashfaq et al. Treatment algorithm for nipple discharge
3Figure 2 Flow diagram of all patients reviewed and the risk of
developing carcinoma.
-
or subareolar duct excision at the time of initial evaluationwas
performed in 48 (34%) patients including 12% (13/107) of those with
no imaging abnormality and 100%(35/35) of the patients with an
imaging abnormality. Therates of carcinoma were 0% (0/13) for those
with no imag-ing abnormality and 23% (8/35) for those with an
imagingabnormality.
Of the 94 patients undergoing close clinical follow-up by
asurgeon, 1 (1%) was subsequently found to have ductalcarcinoma in
situ (DCIS) at her 6-month follow-up visit. Thispatient had not
undergone a subareolar ultrasound at initialevaluation, as called
for on the algorithm, and whenperformed at the 6-month follow-up
appointment, thisdemonstrated intraductal abnormalities prompting
the sub-areolar duct excision that provided the diagnosis. The
9carcinomas diagnosed (Table 3) includedDCIS (n5 5, 56%),invasive
ductal carcinoma (n 5 2, 22%), invasive papillarycarcinoma (n 5 1,
11%), and invasive lobular carcinoma (n5 1, 11%). The stages at
diagnosis were stage 0 (n 5 5,56%), stage I (n5 3, 33%), and stage
III (n5 1, 11%). Me-dian follow-up for those with cancer was 46
months and allpatients remained cancer-free. The single patient
with more
Table 3 Characteristics of patients with carcinoma
Variables n (%)
Total no. of patients with carcinoma 9 (4.6%)Histology
Ductal carcinoma in situ 5 (56%)Invasive ductal carcinoma 2
(22%)Invasive papillary carcinoma 1 (11%)Invasive lobular carcinoma
1 (11%)
Stage at diagnosisStage 0 5 (56%)Stage I 3 (33%)Stage II 0
(0%)Stage III 1 (11%)
Median follow-up (months) 46 (1102)Disease-free survival 9
(100%)
4advanced disease (stage III invasive ductal carcinoma) wasa
74-year-old woman who had a normal mammogram but amarkedly abnormal
physical examination and subareolar ul-trasound. These findings
allowed an immediate diagnosis bypercutaneous core needle biopsy
and the institution of multi-modality treatment. She remains free
of disease at 49 monthsof follow-up.
Of the patients undergoing close clinical follow-up by asurgeon,
21% (20/94) underwent subsequent subareolarduct excision because of
developing an imaging abnormal-ity (1/94, 1%) or for bothersome,
persistent discharge (19/94, 20%). The median follow-up was 28
months for the 74patients not undergoing subareolar duct excision
and 81%of these patients had resolution of their discharge at
lastfollow-up. None of these patients developed carcinoma.
The risk of carcinoma among the entire cohort was 5%,including
4% among women and 50% (1/2) among men.The incidence of carcinoma
in the bloody discharge group
lactation. Periductal mastitis is another frequent cause
of a multicolored, sticky nipple discharge.17 Mammaryduct
ectasia is often associated with chronic duct inflam-mation
(periductal mastitis). This results in a multicolorednipple
discharge (green, yellow, white, brown, gray, or red-dish brown).
Usually the discharge originates from multi-ple ducts and is often
bilateral. All these entities can besafely managed with routine
screening imaging and phys-ical examination. In our study, the risk
of carcinoma forthese patients was 0%.
For patients with pathologic discharge, we performeddiagnostic
mammography (for those 30 years and older)was 11% (7/65) versus 2%
(2/127) in the nonbloody group.All patients with carcinoma had an
imaging abnormality(although 1 patient did not have that
abnormality identifieduntil the 6-month follow-up evaluation as
noted above)including 2 with an abnormal mammogram (sensitivity22%,
specificity 15%), 8 with an abnormal subareolarultrasound
(sensitivity 100%, specificity 17%), 1 with anabnormal ductogram
(sensitivity 100%, specificity 11%),and 1 with an abnormal breast
MRI (sensitivity 50%,specificity 25%) (Table 2).
Comments
Nipple discharge may be caused by benign conditionssuch as
galactorrhea, physiologic stimulation, apocrineglandular secretion,
or intraductal papilloma, but is gener-ally idiopathic. Only a
small proportion of patients withnipple discharge are found to have
a malignancy. However,because it has been felt that the risk of
carcinoma cannot beexcluded without surgical duct excision, this
operation hasbeen widely recommended for all patients with
pathologicnipple discharge.3,6,1013 In our previous retrospective
re-view,14 we found that the subset of patients with
pathologicnipple discharge, a benign physical examination, a
negativemammogram, and a negative subareolar ultrasound has alow
risk of underlying carcinoma and proposed followingthese patients
clinically. The current cohort allows the re-porting of outcomes of
patients evaluated and treated ac-cording to that systematic
approach.
In this study, we used the previously proposed
treatmentalgorithm14 to evaluate patients with nipple discharge.
His-tory and physical examination are an important first step
inidentifying benign nipple discharge including galactor-rhea,
physiologic, pregnancy-associated, periductalmastitis-associated,
and ductal ectasia-associated.12 Galac-torrhea is milky, from
multiple ducts and/or bilateral. It ismost commonly observed after
pregnancy and can last for1 to 2 years.15 Physiologic nipple
discharge is not sponta-neous and is generally bilateral, serous,
and arises frommultiple ducts. Pregnancy-associated nipple
dischargemay be unilateral or bilateral, bloody, without
significantunderlying breast pathology, usually in the 2nd
trimester,and can continue as long as 2 years after pregnancy
and
16
The American Journal of Surgery, Vol -, No -, - 2014and
subareolar ultrasound. All patients with an imaging
-
in this cohort remained cancer-free. So among patients
withabnormality underwent a subareolar duct excision orpercutaneous
biopsy and 23% of these were found tohave a carcinoma. Among the 13
patients with no physicalexamination or imaging abnormality who
underwent exci-sion because of personal preference or concern of
cancerrisk, 0% had malignancy. The risk of carcinoma for
thosefollowed clinically was only 1% and this patient wouldhave
likely undergone initial duct excision had thealgorithm been
applied appropriately. This patients sub-areolar ultrasound was not
performed until the 6-monthfollow-up visit and it was abnormal at
that time asexplained above. Together these findings demonstrate
thatthe algorithm can prospectively identify the patients athighest
risk for underlying malignancy.
The excellent sensitivity of this evaluation process, andin
particular of subareolar ultrasound, has nearly
eliminatedductography from the diagnostic evaluation of patients
withnipple discharge in our practice. Only 13 ductograms
wereperformed among this cohort and all were performed atanother
institution before presentation at our facility. Thesensitivity and
specificity of subareolar ultrasound wereequal or superior to that
of ductography in this cohort(Table 2) and as previously
reported.36 Therefore, if reli-able breast sonographers are
available, we do not recom-mend routine diagnostic ductography
because it is a muchmore uncomfortable procedure. It is important
to notethat patients in this series were evaluated by
experiencedbreast imagers, which may limit the reproducibility of
theseresults among less experienced radiologists, especially inthe
user-dependent application of subareolar ultrasound.Breast MRI was
used sparingly in this cohort, eitherbecause of mammographically
occult disease or becauseit had been obtained at another
institution. There weretoo few MRIs among this cohort to draw any
conclusionsabout its usefulness in nipple discharge. Barring
substantialadditional data, it would be hard to justify the
addition ofsuch an expensive examination into a diagnostic
algorithmthat already performs well.
Patients who made an informed choice for close clinicalfollow-up
underwent physical examination and subareolarsonography and/or
mammography every 6 months for 1 to2 years or until the discharge
resolved, whichever camefirst. Examining the results of this and
the previous study14
cohorts, we recommend that the follow-up imaging
includesubareolar ultrasound every 6 months as this is more
sensi-tive than mammography, despite its lower
specificity.Mammography can be done yearly according to
screeningguidelines.
Despite the low risk for subsequent detection ofcarcinoma in the
patients followed clinically over a medianperiod of 28 months, a
substantial number of patients (20%)chose to undergo subareolar
duct excision for symptomaticrelief. There are no clear findings we
could identify thatcould predict patients who would subsequently
choosesubareolar excision. On the other hand, among the patientswho
never underwent operation, 81% had documented
A. Ashfaq et al. Treatment algorithm for nipple
dischargeresolution of their discharge. Thus, the majority of
low-riskcarcinoma as the cause for their nipple discharge, mosthave
early stage, lower risk disease and they can expect agood outcome.
The one patient with advanced disease wasable to be immediately
identified through physical exam-ination and ultrasound findings,
despite a normal mammo-gram, and has had a good outcome to date as
well.
In conclusion, the implementation of an evidence-basedevaluation
and treatment algorithm for patients with nippledischarge
successfully stratified patients into the low-riskand high-risk
categories. Low-risk patients were safelyfollowed clinically,
whereas high-risk patients had a 23%rate of cancer on subareolar
duct excision. By using thisapproach, one can not only select out
the high-risk patientsfor intervention but also spare 66% of
patients with nippledischarge an unnecessary operation.
References
1. Gulay H, Bora S, Kilicturgay S, et al. Management of
nipple
discharge. J Am Coll Surg 1994;178:4714.
2. Newman HF, Klein M, Northrup JD, et al. Nipple discharge.
Frequency and pathogenesis in an ambulatory population. N Y
State
J Med 1983;83:92833.
3. Adepoju LJ, Chun J, El-Tamer M, et al. The value of clinical
charac-
teristics and breast-imaging studies in predicting a
histopathologic
diagnosis of cancer or high-risk lesion in patients with
spontaneous
nipple discharge. Am J Surg 2005;190:6446.
4. Dawes LG, Bowen C, Venta LA, et al. Ductography for
nipple
discharge: no replacement for ductal excision. Surgery
1998;124:
68591.
5. Gioffre Florio M, Manganaro T, Pollicino A, et al. Surgical
approach
to nipple discharge: a ten-year experience. J Surg Oncol
1999;71:
2358.
6. King TA, Carter KM, Bolton JS, et al. A simple approach to
nipple
discharge. Am Surg 2000;66:9605; discussion, 9656.
7. Locker AP, Galea MH, Ellis IO, et al. Microdochectomy for
single-
duct discharge from the nipple. Br J Surg 1988;75:7001.
8. Murad TM, Contesso G, Mouriesse H. Nipple discharge from
thepatients benefit from avoiding initial operation becausetheir
discharge resolves or never is symptomatic enough towarrant
intervention.
For patient who undergo subareolar duct excision, eitherfor
definitive diagnosis or for treatment of symptomaticdischarge, we
prefer major duct excision. Major subareolarduct excision has been
shown to detect a higher percentageof occult carcinoma than
microdochotomy9 (excision of asingle ductal system with
preservation of remaining ductalsystems in continuity with the
nipple), result in fewer pa-tients requiring repeat duct excision,9
and to be associatedwith a 0% rate of breast cancer diagnosis over
a subsequent5 years.11 The exception to this is for women
planningpossible future breast feeding in whom microdochotomyis
preferred.
The risk of carcinoma among the entire cohort was 5%,including
4% among women and 50% among 2 men. Amajority of patients with
malignancy had DCIS. After amedian follow-up of 46 months, all
patients with carcinoma
5breast. Ann Surg 1982;195:25964.
-
9. Sharma R, Dietz J, Wright H, et al. Comparative analysis of
minimally
invasive microductectomy versus major duct excision in patients
with
pathologic nipple discharge. Surgery 2005;138:5916;
discussion,
5967.
10. Simmons R, Adamovich T, Brennan M, et al. Nonsurgical
evaluation
of pathologic nipple discharge. Ann Surg Oncol 2003;10:1136.
11. Nelson RS, Hoehn JL. Twenty-year outcome following central
duct
resection for bloody nipple discharge. Ann Surg
2006;243:5224.
12. Sakorafas GH. Nipple discharge: current diagnostic and
therapeutic
approaches. Cancer Treat Rev 2001;27:27582.
13. Sauter ER, Schlatter L, Lininger J, et al. The association
of bloody
nipple discharge with breast pathology. Surgery
2004;136:7805.
14. Gray RJ, Pockaj BA, Karstaedt PJ. Navigating murky waters: a
mod-
ern treatment algorithm for nipple discharge. Am J Surg
2007;194:
8504; discussion, 8545.
15. Fiorica J. Nipple discharge. Obstet Gynecol Clin North Am
1994;21:
45360.
16. Isaacs J. Other nipple discharge. Clin Obstet Gynecol
1994;37:898902.
17. Peters F, Schuth W. Hyperprolactinemia and non-puerperal
mastitis
(duct ectasia). JAMA 1989;262:161823.
6 The American Journal of Surgery, Vol -, No -, - 2014
Validation study of a modern treatment algorithm for nipple
dischargeMethodsResultsCommentsReferences