Embed Size (px)
Citation preview

Vascular Antithrombin and ClinicalOutcome in Heart Transplant Patients
Carlos A. Labarrere, MD, Ronald J. Torry, PhD, David R. Nelson, MS,Steven J. Miller, PhD, Douglas E. Pitts, MD, Philip C. Kirlin, MD, and
Harold G. Halbrook, MD
A procoagulant microvasculature is associated with ac-celerated development of coronary artery disease (CAD)and failure in heart transplant patients. This study wasperformed to evaluate how changes in natural antico-agulation within cardiac allografts affect outcome. Weprospectively studied 141 consecutive cardiac allograftrecipients who underwent transplantation between1988 and 1997. Serial endomyocardial biopsy speci-mens (6.5 6 0.1 biopsy specimens/patient) obtainedduring the first 3 months after transplantation werestudied immunohistochemically to evaluate vascular an-tithrombin, and annual coronary angiograms (3.8 6 0.2angiograms/patient) were studied to evaluate CAD. An-tithrombin was present in arteries and veins, but not incapillaries, of all donor heart biopsy samples. Allograftsthat maintained vascular antithrombin had the bestprognosis. Allografts with early and persistent loss ofvascular antithrombin (n 5 21) developed CAD earlier (p
<0.001), developed more severe disease (p <0.001),showed more disease progression (p <0.001), andfailed more often (p 5 0.003) and earlier (p <0.001)than allografts retaining normal vascular antithrombin(n 5 45). However, allografts that lost and recoveredvascular antithrombin while developing unusual capil-lary antithrombin binding (n 5 75) had less CAD, de-veloped CAD later, had less severe disease and lessdisease progression (p <0.01), and failed less often (p 50.01) and later (p 5 0.03) than allografts with persistentloss of vascular antithrombin. The persistent lack of athromboresistant microvasculature increases risk of sub-sequent CAD and graft failure. However, recovery ofvascular antithrombin and development of unusual cap-illary antithrombin binding improves allograft outcome.Q2001 by Excerpta Medica, Inc.
(Am J Cardiol 2001;87:425–431)
The assessment of the status of the microvasculatureafter transplantation provides reliable data associ-
ated with clinical outcome of cardiac allograft recip-ients.1,2 Early depletion of tissue plasminogen activa-tor from arteriolar smooth muscle cells and expressionof endothelial activation markers such as intercellularadhesion molecule-1 and class II major histocompat-ibility antigens on arterial and arteriolar endotheliumare associated with development of transplant coro-nary artery disease (CAD) and/or allograft failure.1,2
The expression of endothelial activation markers andthe loss of vascular fibrinolytic activators are relatedto increased thrombogenicity within the microvascu-lature, resulting in fibrin deposition.3 Indeed, myocar-dial fibrin deposition is an independent determinant ofallograft dysfunction and failure.4,5 In addition, anti-thrombin is present in the microvasculature of normaldonor hearts, and depletion of vascular antithrombin
occurs in some grafts after transplantation.4 We askedif the early and persistent loss of vascular antithrom-bin after transplantation was associated with develop-ment of transplant CAD and/or graft failure and if therecovery of vascular antithrombin, which includes thedevelopment of unique capillary antithrombin bind-ing, was associated with improved outcome.
METHODSPatients: We prospectively studied 141 consecutive
adult cardiac allograft recipients who underwent trans-plantation at Methodist Hospital of Indiana between1988 and 1997. Patients were enrolled in the study ifthey survived at least 6 months after transplant, hadpretransplantation biopsy specimens and serial endo-myocardial biopsy specimens obtained during the first3 months after transplantation for light microscopyand immunohistochemical studies, and had angio-graphic or histopathologic evaluations of coronaryarteries.1,2,5,6 Coronary angiography was performedyearly and averaged 3.86 0.2 angiograms/patient.
Immunosuppression therapy consisted of pred-nisone at an initial dose of 1 mg/kg/day, with the dosetapered to 0.5 mg/kg/day during the first month aftertransplantation, to 0.2 mg/kg/day during months 1 and2, and to 0.1 mg/kg/day 3 months after transplanta-tion. Patients were maintained on this dose unless theydeveloped steroid complications. Azathioprine wasadministered at a dose of 1.5 to 2.0 mg/kg/day andcyclosporine at an initial dose of 7 to 10 mg/kg/day,with the dose tapered to 3 to 5 mg/kg/day to maintain
From the Methodist Research Institute, Methodist Transplant Center,Clarian Health Partners (Methodist, Indiana University, Riley Hospi-tals), Indianapolis, Indiana; College of Pharmacy and Health Sci-ences, Drake University, Des Moines, Iowa; and Department of Bio-statistics and Epidemiology, Cleveland Clinic Foundation, Cleveland,Ohio. This research was supported by Methodist Research Institute,Clarian Health, Showalter Foundation (Methodist Hospital), and Amer-ican Heart Association, Midwest Affiliate, Indianapolis, Indiana.Manuscript received May 1, 2000; revised manuscript received andaccepted August 18, 2000.
Address for reprints: Carlos A. Labarrere, MD, Methodist ResearchInstitute, Clarian Health Partners (Methodist, Indiana University, RileyHospitals), 1701 North Senate Boulevard, Indianapolis, Indiana46202. E-mail: [email protected].
425©2001 by Excerpta Medica, Inc. All rights reserved. 0002-9149/01/$–see front matterThe American Journal of Cardiology Vol. 87 February 15, 2001 PII S0002-9149(00)01395-3

a specific whole blood level of 300 to 480 ng/mlduring months 1 to 3, 180 to 360 ng/ml during months3 to 6, 90 to 180 ng/ml during months 6 to 12, and 75to 120 ng/ml 12 months after transplantation, depend-ing on renal function. Grades 3 and 4 rejection epi-sodes7 were treated with steroids (methylpredniso-lone, 1 g/day for 3 days) and antithymocyte globulin(horse, 10 to 20 mg/kg/day for 3 days, or rabbit, 1.5mg/kg/day for 3 days). Clinical function was deter-mined by New York Heart Association criteria, andejection fractions were measured by radionuclide ven-triculography. Patients with functional classificationsIII or IV and decreasing ejection fractions were clas-sified as being clinically unstable, and patients withclinical function scores I or II and nondecreasingejection fractions were classified as being clinicallystable. Graft failure was defined as death associatedwith cardiac allograft dysfunction or need for a secondtransplant.
Donor hearts were perfused with Stanford cardio-plegia solution, and the mean ischemic time was138.06 5.0 minutes. A control biopsy from the rightventricle was obtained from all donor hearts beforetransplantation. Endomyocardial biopsy specimenswere then obtained from all donor hearts by rightcardiac catheterization at 7 to 10 days, every 2 weeksduring the first 2 months, and at 3, 4.5, 6, 9, and 12months after transplantation. All biopsy specimensobtained before transplantation and during the firstyear after transplantation for each patient (9.96 0.2biopsy specimens/patient) were analyzed. Cellular in-filtrates were graded according to the InternationalSociety for Heart Transplantation.7 Cytomegalovirusinfection was defined as a fourfold increase in anti-body, cytomegalovirus inclusion bodies, or positivecultures.8
Criteria for diagnosis of coronary artery disease:CAD was diagnosed with any decrease in luminaldiameter, whether in the left main coronary artery orprimary or branch vessels, as described.9 Primary ves-sels refer to the proximal or anatomic middle third ofthe left anterior descending and circumflex coronaryarteries and the distal third of the dominant or codomi-nant right coronary artery, including the origin of theposterior descending coronary artery. Branch vesselsrefer to the diagonal branches, obtuse marginalbranches, distal third of a primary vessel, or any partof a nondominant right coronary artery. CAD wasclassified as (1) mild, if there was a#50% lesion inthe left main coronary artery, a maximum lesion of#70% in primary vessels, and an isolated singlebranch stenosis of.70%, or any branch stenosis,70% (including diffuse narrowing); (2) moderate, ifthere was a lesion of 50% to 70% in the left maincoronary artery, 1 primary vessel.70%, and isolatedbranch stenosis.70% in branches of 2 systems; and(3) severe, if there was a lesion of.70% in the leftmain coronary artery,$2 primary vessels.70%, andisolated branch stenosis.70% in all 3 systems. Theclass of disease (mild, moderate, severe) was deter-mined by the most severe CAD reported in eachcoronary angiogram.9 Annual arteriograms were com-
pared with identical projections in serial studies andevaluated by side-by-side comparisons. The presence,severity, and progression of disease were determinedby a consensus of 2 experienced angiographersblinded to the results of the immunohistochemicalstudies for vascular antithrombin. Progression of dis-ease was evaluated comparing serial angiograms sideby side with the baseline angiogram obtained the firstyear after transplantation. Coronary arteries were ex-amined histopathologically6 in recipients who diedbefore their first angiogram was performed, and thepresence of intimal thickening exceeding the thicknessof the media and/or the presence of plaques indicatedCAD. The degree of luminal narrowing was estimatedvisually, and degrees of,50%, 51% to 75%, and.75% were considered mild, moderate, and severe,respectively, as described.6
Biopsies, antibodies, and control experiments: Bi-opsy specimens were embedded in optimum cuttingtemperature compound (Miles, Elkhart, Indiana), snapfrozen in liquid nitrogen, and stored at220°C. Cry-ostat sections (4mm) were air-dried overnight withoutchemical fixation. Endomyocardial biopsy sampleswere studied immunohistochemically for antithrombinusing polyclonal (A296, Dako, Carpinteria, Califor-nia) and monoclonal antibodies (2333, American Di-agnostica, Greenwich, Connecticut) and monoclonalantibody to the heparin-binding site of antithrombin(2331, American Diagnostica). Arteries and arterioleswere identified by using monoclonal antibody tosmooth-muscle-specifica-actin (1A4, Biomakor, Re-hovot, Israel). Endothelial cells were identified using apolyclonal antibody to von Willebrand factor (A082,Dako). Second antibodies consisted of affinity-puri-fied fluorochrome-labeled F(ab9)2 antibody fragmentsto species-specific immunoglobulins (Protos Immu-noResearch, San Francisco, California). Control ex-periments were performed as described.1,2,4,5
Immunohistochemistry: Antibody experiments andtheir evaluations were performed as described.1,2,4,5
Vascular antithrombin reactivity was precisely locatedusing double and triple antibody experiments.1,2,4,5
Antithrombin in arterial and arteriolar smooth musclecells, arterial intima, and venous endothelium wasconsidered a normal pattern of vascular antithrombin,and absence of vascular antithrombin or presence ofcapillary antithrombin was considered an abnormalpattern.4,10,11 Allografts that persistently showed anormal pattern of vascular antithrombin during thefirst 3 months after transplantation were considered tohave normal antithrombin. Allografts that persistentlylost and never recovered vascular antithrombin bind-ing during the first 3 months after transplantation wereconsidered to have negative antithrombin. Allograftsthat initially lost vascular antithrombin immunoreac-tivity and subsequently recovered antithrombin immu-noreactivity with concomitant development of capil-lary antithrombin binding during the first 3 monthsafter transplantation were considered to have capillaryantithrombin.
Statistical analysis: Groups with varying antithrom-bin reactivities were compared with Kruskal-Wallis
426 THE AMERICAN JOURNAL OF CARDIOLOGYT VOL. 87 FEBRUARY 15, 2001
tests for continuous variables (e.g., age) and chi-square tests for categorical variables (e.g., sex). Sig-nificant demographic variables were included in sub-sequent group comparisons. Logistic regression (forthe rates of graft failure and CAD) and Cox regression(for the interval to graft failure and CAD) were used totest the effect of antithrombin distribution. Pairwisegroup comparisons used Fisher’s exact and log-ranktests. A subset of allografts with capillary antithrom-bin at 3-month and 2-year follow-ups was examined todetermine whether the CAD status at 2 years wasrelated to the antithrombin status 3 to 12 months after
transplantation using repeated-measures (generalized estimatingequations) logistic regression. Sta-tistical significance was assessedusing 2-tailed tests at the p,0.05level and calculated using PC-SAS8 software (SAS Institute Inc.,Cary, North Carolina). Summarystatistics included mean6 SE.
RESULTSAll 141 donor hearts studied
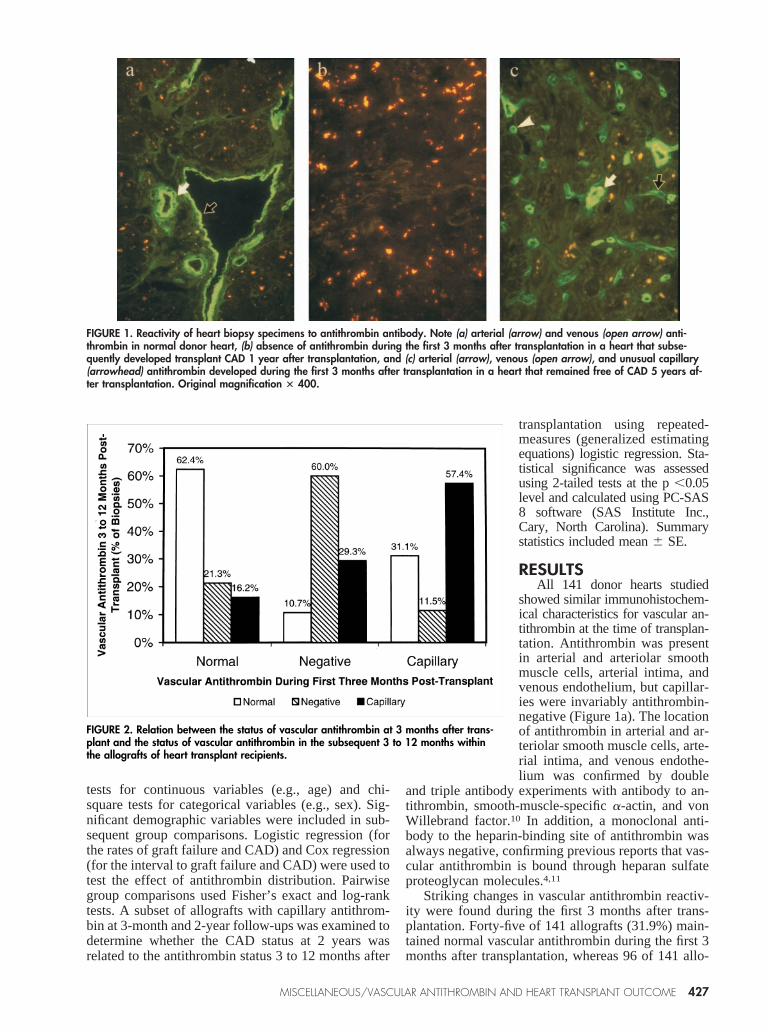
showed similar immunohistochem-ical characteristics for vascular an-tithrombin at the time of transplan-tation. Antithrombin was presentin arterial and arteriolar smoothmuscle cells, arterial intima, andvenous endothelium, but capillar-ies were invariably antithrombin-negative (Figure 1a). The locationof antithrombin in arterial and ar-teriolar smooth muscle cells, arte-rial intima, and venous endothe-lium was confirmed by double
and triple antibody experiments with antibody to an-tithrombin, smooth-muscle-specifica-actin, and vonWillebrand factor.10 In addition, a monoclonal anti-body to the heparin-binding site of antithrombin wasalways negative, confirming previous reports that vas-cular antithrombin is bound through heparan sulfateproteoglycan molecules.4,11
Striking changes in vascular antithrombin reactiv-ity were found during the first 3 months after trans-plantation. Forty-five of 141 allografts (31.9%) main-tained normal vascular antithrombin during the first 3months after transplantation, whereas 96 of 141 allo-
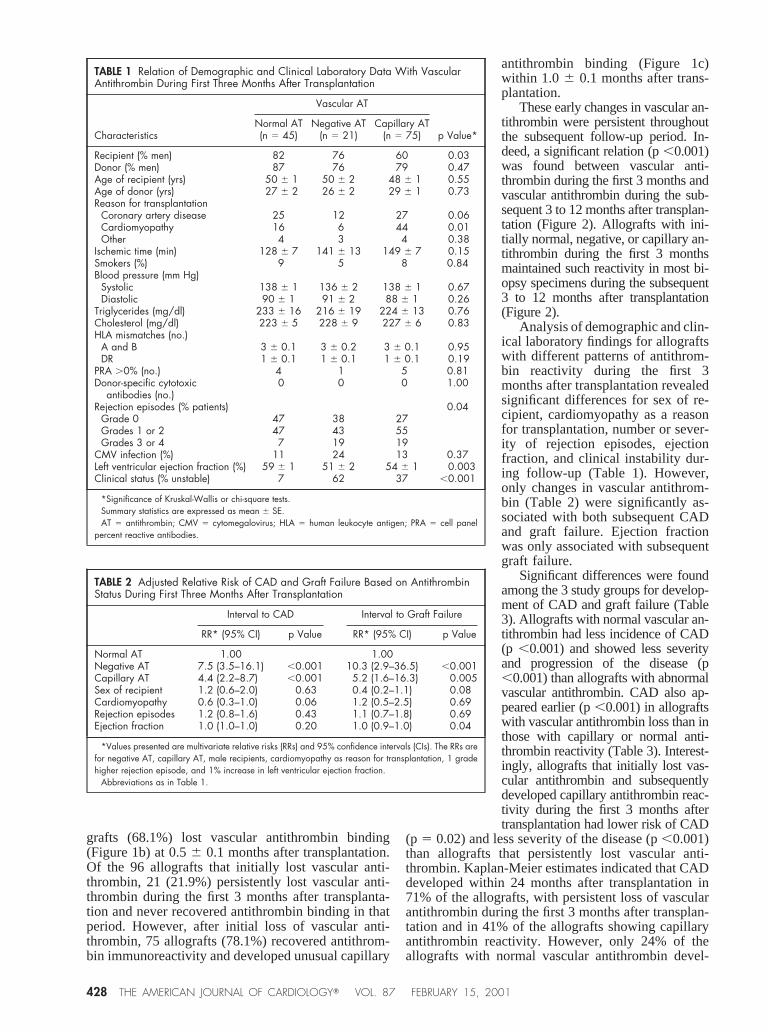
FIGURE 2. Relation between the status of vascular antithrombin at 3 months after trans-plant and the status of vascular antithrombin in the subsequent 3 to 12 months withinthe allografts of heart transplant recipients.
FIGURE 1. Reactivity of heart biopsy specimens to antithrombin antibody. Note (a) arterial (arrow) and venous (open arrow) anti-thrombin in normal donor heart, (b) absence of antithrombin during the first 3 months after transplantation in a heart that subse-quently developed transplant CAD 1 year after transplantation, and (c) arterial (arrow), venous (open arrow), and unusual capillary(arrowhead) antithrombin developed during the first 3 months after transplantation in a heart that remained free of CAD 5 years af-ter transplantation. Original magnification 3 400.
MISCELLANEOUS/VASCULAR ANTITHROMBIN AND HEART TRANSPLANT OUTCOME 427
grafts (68.1%) lost vascular antithrombin binding(Figure 1b) at 0.56 0.1 months after transplantation.Of the 96 allografts that initially lost vascular anti-thrombin, 21 (21.9%) persistently lost vascular anti-thrombin during the first 3 months after transplanta-tion and never recovered antithrombin binding in thatperiod. However, after initial loss of vascular anti-thrombin, 75 allografts (78.1%) recovered antithrom-bin immunoreactivity and developed unusual capillary
antithrombin binding (Figure 1c)within 1.0 6 0.1 months after trans-plantation.
These early changes in vascular an-tithrombin were persistent throughoutthe subsequent follow-up period. In-deed, a significant relation (p,0.001)was found between vascular anti-thrombin during the first 3 months andvascular antithrombin during the sub-sequent 3 to 12 months after transplan-tation (Figure 2). Allografts with ini-tially normal, negative, or capillary an-tithrombin during the first 3 monthsmaintained such reactivity in most bi-opsy specimens during the subsequent3 to 12 months after transplantation(Figure 2).
Analysis of demographic and clin-ical laboratory findings for allograftswith different patterns of antithrom-bin reactivity during the first 3months after transplantation revealedsignificant differences for sex of re-cipient, cardiomyopathy as a reasonfor transplantation, number or sever-ity of rejection episodes, ejectionfraction, and clinical instability dur-ing follow-up (Table 1). However,only changes in vascular antithrom-bin (Table 2) were significantly as-sociated with both subsequent CADand graft failure. Ejection fractionwas only associated with subsequentgraft failure.
Significant differences were foundamong the 3 study groups for develop-ment of CAD and graft failure (Table3). Allografts with normal vascular an-tithrombin had less incidence of CAD(p ,0.001) and showed less severityand progression of the disease (p,0.001) than allografts with abnormalvascular antithrombin. CAD also ap-peared earlier (p,0.001) in allograftswith vascular antithrombin loss than inthose with capillary or normal anti-thrombin reactivity (Table 3). Interest-ingly, allografts that initially lost vas-cular antithrombin and subsequentlydeveloped capillary antithrombin reac-tivity during the first 3 months aftertransplantation had lower risk of CAD
(p 5 0.02) and less severity of the disease (p,0.001)than allografts that persistently lost vascular anti-thrombin. Kaplan-Meier estimates indicated that CADdeveloped within 24 months after transplantation in71% of the allografts, with persistent loss of vascularantithrombin during the first 3 months after transplan-tation and in 41% of the allografts showing capillaryantithrombin reactivity. However, only 24% of theallografts with normal vascular antithrombin devel-
TABLE 1 Relation of Demographic and Clinical Laboratory Data With VascularAntithrombin During First Three Months After Transplantation
Characteristics
Vascular AT
p Value*Normal AT(n 5 45)
Negative AT(n 5 21)
Capillary AT(n 5 75)
Recipient (% men) 82 76 60 0.03Donor (% men) 87 76 79 0.47Age of recipient (yrs) 50 6 1 50 6 2 48 6 1 0.55Age of donor (yrs) 27 6 2 26 6 2 29 6 1 0.73Reason for transplantation
Coronary artery disease 25 12 27 0.06Cardiomyopathy 16 6 44 0.01Other 4 3 4 0.38
Ischemic time (min) 128 6 7 141 6 13 149 6 7 0.15Smokers (%) 9 5 8 0.84Blood pressure (mm Hg)
Systolic 138 6 1 136 6 2 138 6 1 0.67Diastolic 90 6 1 91 6 2 88 6 1 0.26
Triglycerides (mg/dl) 233 6 16 216 6 19 224 6 13 0.76Cholesterol (mg/dl) 223 6 5 228 6 9 227 6 6 0.83HLA mismatches (no.)
A and B 3 6 0.1 3 6 0.2 3 6 0.1 0.95DR 1 6 0.1 1 6 0.1 1 6 0.1 0.19
PRA .0% (no.) 4 1 5 0.81Donor-specific cytotoxic
antibodies (no.)0 0 0 1.00
Rejection episodes (% patients) 0.04Grade 0 47 38 27Grades 1 or 2 47 43 55Grades 3 or 4 7 19 19
CMV infection (%) 11 24 13 0.37Left ventricular ejection fraction (%) 59 6 1 51 6 2 54 6 1 0.003Clinical status (% unstable) 7 62 37 ,0.001
*Significance of Kruskal-Wallis or chi-square tests.Summary statistics are expressed as mean 6 SE.AT 5 antithrombin; CMV 5 cytomegalovirus; HLA 5 human leukocyte antigen; PRA 5 cell panel
percent reactive antibodies.
TABLE 2 Adjusted Relative Risk of CAD and Graft Failure Based on AntithrombinStatus During First Three Months After Transplantation
Interval to CAD Interval to Graft Failure
RR* (95% CI) p Value RR* (95% CI) p Value
Normal AT 1.00 1.00Negative AT 7.5 (3.5–16.1) ,0.001 10.3 (2.9–36.5) ,0.001Capillary AT 4.4 (2.2–8.7) ,0.001 5.2 (1.6–16.3) 0.005Sex of recipient 1.2 (0.6–2.0) 0.63 0.4 (0.2–1.1) 0.08Cardiomyopathy 0.6 (0.3–1.0) 0.06 1.2 (0.5–2.5) 0.69Rejection episodes 1.2 (0.8–1.6) 0.43 1.1 (0.7–1.8) 0.69Ejection fraction 1.0 (1.0–1.0) 0.20 1.0 (0.9–1.0) 0.04
*Values presented are multivariate relative risks (RRs) and 95% confidence intervals (CIs). The RRs arefor negative AT, capillary AT, male recipients, cardiomyopathy as reason for transplantation, 1 gradehigher rejection episode, and 1% increase in left ventricular ejection fraction.
Abbreviations as in Table 1.
428 THE AMERICAN JOURNAL OF CARDIOLOGYT VOL. 87 FEBRUARY 15, 2001
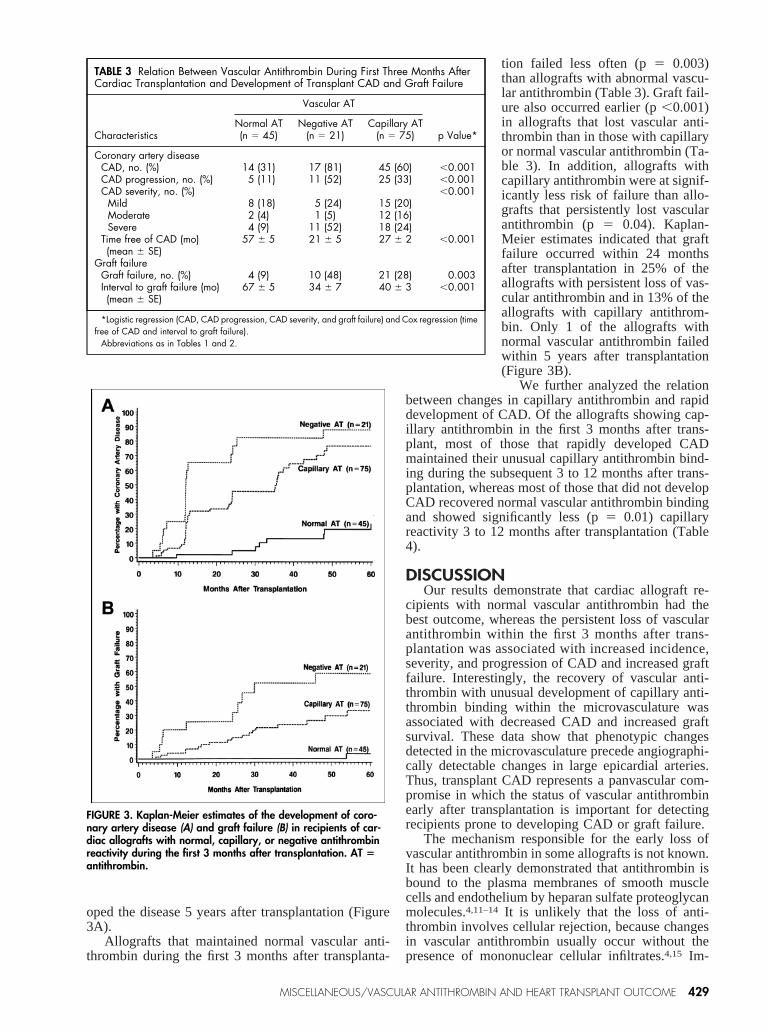
oped the disease 5 years after transplantation (Figure3A).
Allografts that maintained normal vascular anti-thrombin during the first 3 months after transplanta-
tion failed less often (p5 0.003)than allografts with abnormal vascu-lar antithrombin (Table 3). Graft fail-ure also occurred earlier (p,0.001)in allografts that lost vascular anti-thrombin than in those with capillaryor normal vascular antithrombin (Ta-ble 3). In addition, allografts withcapillary antithrombin were at signif-icantly less risk of failure than allo-grafts that persistently lost vascularantithrombin (p 5 0.04). Kaplan-Meier estimates indicated that graftfailure occurred within 24 monthsafter transplantation in 25% of theallografts with persistent loss of vas-cular antithrombin and in 13% of theallografts with capillary antithrom-bin. Only 1 of the allografts withnormal vascular antithrombin failedwithin 5 years after transplantation(Figure 3B).
We further analyzed the relationbetween changes in capillary antithrombin and rapiddevelopment of CAD. Of the allografts showing cap-illary antithrombin in the first 3 months after trans-plant, most of those that rapidly developed CADmaintained their unusual capillary antithrombin bind-ing during the subsequent 3 to 12 months after trans-plantation, whereas most of those that did not developCAD recovered normal vascular antithrombin bindingand showed significantly less (p5 0.01) capillaryreactivity 3 to 12 months after transplantation (Table4).
DISCUSSIONOur results demonstrate that cardiac allograft re-
cipients with normal vascular antithrombin had thebest outcome, whereas the persistent loss of vascularantithrombin within the first 3 months after trans-plantation was associated with increased incidence,severity, and progression of CAD and increased graftfailure. Interestingly, the recovery of vascular anti-thrombin with unusual development of capillary anti-thrombin binding within the microvasculature wasassociated with decreased CAD and increased graftsurvival. These data show that phenotypic changesdetected in the microvasculature precede angiographi-cally detectable changes in large epicardial arteries.Thus, transplant CAD represents a panvascular com-promise in which the status of vascular antithrombinearly after transplantation is important for detectingrecipients prone to developing CAD or graft failure.
The mechanism responsible for the early loss ofvascular antithrombin in some allografts is not known.It has been clearly demonstrated that antithrombin isbound to the plasma membranes of smooth musclecells and endothelium by heparan sulfate proteoglycanmolecules.4,11–14 It is unlikely that the loss of anti-thrombin involves cellular rejection, because changesin vascular antithrombin usually occur without thepresence of mononuclear cellular infiltrates.4,15 Im-
FIGURE 3. Kaplan-Meier estimates of the development of coro-nary artery disease (A) and graft failure (B) in recipients of car-diac allografts with normal, capillary, or negative antithrombinreactivity during the first 3 months after transplantation. AT 5antithrombin.
TABLE 3 Relation Between Vascular Antithrombin During First Three Months AfterCardiac Transplantation and Development of Transplant CAD and Graft Failure
Characteristics
Vascular AT
p Value*Normal AT(n 5 45)
Negative AT(n 5 21)
Capillary AT(n 5 75)
Coronary artery diseaseCAD, no. (%) 14 (31) 17 (81) 45 (60) ,0.001CAD progression, no. (%) 5 (11) 11 (52) 25 (33) ,0.001CAD severity, no. (%) ,0.001
Mild 8 (18) 5 (24) 15 (20)Moderate 2 (4) 1 (5) 12 (16)Severe 4 (9) 11 (52) 18 (24)
Time free of CAD (mo)(mean 6 SE)
57 6 5 21 6 5 27 6 2 ,0.001
Graft failureGraft failure, no. (%) 4 (9) 10 (48) 21 (28) 0.003Interval to graft failure (mo)(mean 6 SE)
67 6 5 34 6 7 40 6 3 ,0.001
*Logistic regression (CAD, CAD progression, CAD severity, and graft failure) and Cox regression (timefree of CAD and interval to graft failure).
Abbreviations as in Tables 1 and 2.
MISCELLANEOUS/VASCULAR ANTITHROMBIN AND HEART TRANSPLANT OUTCOME 429

provements in immunosuppressive therapy have notreduced the incidence of transplant CAD,16 and, inthis study, only changes in vascular antithrombin, notthe presence or severity of cellular rejection episodes,were associated with increased risk of CAD and graftfailure.
The loss of vascular antithrombin could be relatedto ischemia and reperfusion injury, which causes mi-crovascular damage and is associated with develop-ment of transplant CAD.17 Interestingly, thrombinplays a critical role in reperfusion-induced leukocyterecruitment as well as increased microvascular perme-ability alterations.18 Neutrophils can subsequentlycleave heparan sulfate proteoglycan molecules fromthe cell surfaces through enzymatic degradation byneutrophil elastase or heparanase,19 promoting the de-pletion of vascular heparan sulfate proteoglycans andsubsequent intravascular thrombosis.
Other potential mechanisms for antithrombin lossinvolve alterations of the heparan sulfate proteoglycancore protein or its polysaccharide chains,13,20 inade-quate sulfation of heparan,21 or antibody-mediatedcomplement activation,22,23 which induces release ofheparan sulfate proteoglycan molecules from endothe-lial cells. Regardless of the mechanism, vessels with-out antithrombin become thrombogenic and microvas-cular fibrin is deposited. Interestingly, the availabilityof thrombin under these circumstances may directly orindirectly induce loss of heparan sulfate proteoglycanfrom cell surfaces,18,19,24and this could facilitate thepersistent loss of antithrombin binding in the cardiacmicrovasculature. The generation of thrombin andconcomitant loss of antithrombin in a subpopulationof allografts may be associated with a genetic trait,because cardiac transplant recipients with a 2/2 plas-minogen activator inhibitor-1 genotype have increasedrisk of developing transplant CAD.25
An important finding from our data is that manyallografts that initially lost vascular antithrombin re-covered vascular antithrombin and showed unusualcapillary antithrombin binding. The exact mechanismpromoting capillary antithrombin binding under these
conditions is not known. We suggestthat this capillary response repre-sents a type of wound-healing pro-cess involving vascular remodelingand/or neovessel formation26,27 be-cause (1) the capillary antithrombinresponse only occurs after microvas-cular fibrin deposition,4,27 (2) wehave shown that microvascular fibrindeposition is associated with vascu-lar endothelial growth factor expres-sion,26 (3) thrombin and thrombinpeptides facilitate neovascularizationand wound healing,28 and (4) hepa-ran sulfate proteoglycan expressionis induced in capillaries within heal-ing wounds.29 Collectively, our re-sults suggest that changes in micro-vascular antithrombin binding afterfibrin deposition mimic many of the
changes associated with angiogenesis/vascular remod-eling typically found during wound healing.
Another important finding is that allografts thatdeveloped capillary antithrombin binding soon aftertransplantation maintained that reactivity during thefirst year after transplantation, and the maintenance ofcapillary antithrombin was associated with increasedCAD. This suggests that allografts with sustained cap-illary antithrombin binding persistently generatethrombin, which could promote smooth muscle cellmigration and proliferation in the micro- and macro-vasculature of the allografts, ending in the develop-ment of CAD.
The present study is limited in 2 ways. First, thestatus of the coronary arteries could not be evaluatedangiographically at the time each serial endomyocar-dial biopsy was performed to establish the preciserelation between changes in vascular antithrombin anddevelopment of CAD. Second, the status of the coro-nary arteries was evaluated angiographically ratherthan by intravascular ultrasonography. Nevertheless,coronary angiography has the distinct advantage ofallowing assessment of distal lesions in smaller arter-ies not accessible by intravascular ultrasonography.2,30
Furthermore, the measurement error would be thesame in all recipients.
Acknowledgment: We thank our colleagues in theDepartment of Transplantation, especially the trans-plant coordinators, Sandra Mitchell, Alicia Currin,and William Johnson, for their continued support ofthis work; Denise R. Miller for her technical assis-tance; and Karen Spear for editing.
1. Labarrere CA, Pitts D, Nelson DR, Faulk WP. Vascular tissue plasminogenactivator and the development of coronary artery disease in heart transplantrecipients.N Engl J Med1995;333:1111–1116.2. Labarrere CA, Nelson DR, Faulk WP. Endothelial activation and developmentof coronary artery disease in transplanted human hearts.JAMA 1997;278:1169–1175.3. Labarrere CA. Relationship of fibrin deposition in microvasculature to out-comes in cardiac transplantation.Curr Opin Cardiol 1999;14:133–139.
TABLE 4 Relation Between Status of Vascular Antithrombin Three to 12 MonthsAfter Transplantation and Rapid Development of CAD in Recipients WhoDeveloped Capillary Antithrombin Binding During First Three Months AfterTransplant
Characteristics
CAD Two YearsAfter Transplantation
Yes(n 5 31)
No(n 5 27) p Value
No. of biopsy specimens/patient obtained3 to 12 mo after transplantation (mean 6 SE)
4 6 0.3 4 6 0.3 0.44
Vascular AT 3 to 12 mo aftertransplantation (% of biopsies)*
0.01
Normal 26 40Negative 13 16Capillary 61 44
*Percentage of biopsy samples with normal, negative, or capillary AT during the period 3 to 12months after transplantation. Analysis performed using repeated-measures (GEE) logistic regression.
Abbreviations as in Table 1.
430 THE AMERICAN JOURNAL OF CARDIOLOGYT VOL. 87 FEBRUARY 15, 2001

4. Faulk WP, Labarrere CA. Fibrinolytic and anticoagulant control of hemostasisin human cardiac and renal allografts.Major Probl Pathol1994;30:49–65.5. Labarrere CA, Nelson DR, Faulk WP. Myocardial fibrin deposits in the firstmonth after transplantation predict subsequent coronary artery disease and graftfailure in cardiac allograft recipients.Am J Med1998;105:207–213.6. Johnson DE, Gao SZ, Schroeder JS, De Campli WM, Billingham ME. Thespectrum of coronary artery pathologic findings in human cardiac allografts.J Heart Transplant1989;8:349–359.7. Billingham ME, Cary NRB, Hammond ME, Kemnitz J, Marboe C, McCallisterHA, Snovar DC, Winters GL, Zerbe A. A working formulation for the standard-ization of nomenclature in the diagnosis of heart and lung rejection: HeartRejection Study Group. The International Society for Heart Transplantation.J Heart Transplant1990;9:587–593.8. Grattan MT, Moreno-Cabral CE, Starnes VA, Oyer PE, Stinson EB, ShumwayNE. Cytomegalovirus infection is associated with cardiac allograft rejection andatherosclerosis.JAMA 1989;261:3561–3566.9. Costanzo MR, Naftel DC, Pritzker MR, Heilman JK III, Boehmer JP, BrozenaSC, Dec GW, Ventura HO, Kirklin JK, Bourge RC, Miller LW. Heart transplantcoronary artery disease detected by coronary angiography: a multi-institutionalstudy of preoperative donor and recipient risk factors. Cardiac Transplant Re-search Database.J Heart Lung Transplant1998;17:744–753.10. Faulk WP, Labarrere CA. Antithrombin III in normal and transplanted humanhearts: indications of vascular disease.Semin Hematol1994;31:26–34.11. Faulk WP, Labarrere CA, Nelson DR, Pitts D. Coronary artery disease incardiac allografts: association with arterial antithrombin.Transplant Proc1995;27:1944–1946.12. Marcum JA, Rosenberg RD. Role of endothelial cell surface heparin-likepolysaccharides.Ann NY Acad Sci1989;556:81–94.13. Wight TN. Cell biology of arterial proteoglycans.Arteriosclerosis1989;9:1–20.14. Absher E, Labarrere CA, Carter C, Haag B, Faulk WP. The endothelialheparan sulfate-antithrombin III natural anticoagulant pathway in normal andtransplanted human kidneys.Transplantation1992;53:828–834.15. Faulk WP, Labarrere CA, Pitts D, Halbrook H. Vascular lesions in biopsyspecimens devoid of cellular infiltrates: qualitative and quantitative immunocy-tochemical studies of human cardiac allografts.J Heart Lung Transplant1993;12:219–229.16. Hosenpud JD, Shipley GD, Wagner CR. Cardiac allograft vasculopathy:current concepts, recent developments, and future directions.J Heart LungTransplant1992;11:9–23.17. Day JD, Rayburn BK, Gaudin PB, Baldwin WM III, Lowenstein CJ, Kasper
EK, Baughman KL, Baumgartner WA, Hutchins GM, Hruban RH. Cardiacallograft vasculopathy: the central pathogenetic role of ischemia-induced endo-thelial cell injury.J Heart Lung Transplant1995;14:S142–S149.18. Ostrovsky L, Woodman RC, Payne D, Teoh D, Kubes P. Antithrombin IIIprevents and rapidly reverses leukocyte recruitment in ischemia/reperfusion.Circulation 1997;96:2302–2310.19. Key NS, Platt JL, Vercellotti GM. Vascular endothelial cell proteoglycans aresusceptible to cleavage by neutrophils.Arterioscler Thromb1992;12:836–842.20. Kinsella MG, Wight TN. Structural characterization of heparan sulfateproteoglycan subclasses isolated from bovine aortic endothelial cell cultures.Biochemistry1988;27:2136–2144.21. Pejler G, David G. Basement-membrane heparan sulfate with high affinity forantithrombin synthesized by normal and transformed mouse mammary epithelialcells.Biochem J1987;248:69–77.22. Platt JL, Vercellotti GM, Lindman BJ, Oegema TR, Bach FH, Dalmasso AP.Release of heparan sulfate from endothelial cells. Implications for pathogenesisof hyperacute rejection.J Exp Med1990;171:1363–1368.23. Platt JL, Dalmasso AP, Lindman BJ, Ihrcke NS, Bach FH. The role of C5aand antibody in the release of heparan sulfate from endothelial cells.EurJ Immunol1991;21:2887–2890.24. Subramanian SV, Fitzgerald ML, Bernfield M. Regulated shedding of syn-decan-1 and -4 ectodomains by thrombin and growth factor receptor activation.J Biol Chem1997;272:14713–14720.25. Benza RL, Grenett HE, Bourge RC, Kirklin JK, Naftel SC, Castro PF,McGriffin DC, George JF, Booyse FM. Gene polymorphisms for plasminogenactivator inhibitor-1/tissue plasminogen activator and development of allograftcoronary artery disease.Circulation 1998;98:2248–2254.26. Torry RJ, Labarrere CA, Torry DS, Holt VJ, Faulk WP. Vascular endothelialgrowth factor expression in transplanted human hearts.Transplantation1995;60:1451–1457.27. Labarrere CA, Faulk WP. Antithrombin determinants of coronary arterydisease in transplanted human hearts.Semin Hematol1995;32:61–66.28. Carney DH, Mann R, Redin WR, Pernia SD, Berry D, Heggers JP, HaywardPG, Robson MC, Christie J, Annable C, et al. Enhancement of incisional woundhealing and neovascularization in normal rats by thrombin and synthetic thrombinreceptor-activating peptides.J Clin Invest1992;89:1469–1477.29. Elenius K, Vainio S, Laato M, Salmivirta M, Thesleff I, Jalkanen M. Inducedexpression of syndecan in healing wounds.J Cell Biol 1991;114:585–595.30. Topol EJ, Nissen SE. Our preoccupation with coronary luminology: thedissociation between clinical and angiographic findings in ischemic heart disease.Circulation 1995;92:2333–2342.
MISCELLANEOUS/VASCULAR ANTITHROMBIN AND HEART TRANSPLANT OUTCOME 431





























