Embed Size (px)
Citation preview

http://cat.sagepub.com/Clinical and Applied Thrombosis/Hemostasis
http://cat.sagepub.com/content/19/4/357The online version of this article can be found at:
DOI: 10.1177/1076029613481105
2013 19: 357 originally published online 22 April 2013CLIN APPL THROMB HEMOSTRussell D. Hull, Tazmin Merali, Allan Mills, Abigail L. Stevenson and Jane Liang
Influence of Risk FactorsVenous Thromboembolism in Elderly High-Risk Medical Patients: Time Course of Events and
Published by:
http://www.sagepublications.com
can be found at:Clinical and Applied Thrombosis/HemostasisAdditional services and information for
http://cat.sagepub.com/cgi/alertsEmail Alerts:
http://cat.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://cat.sagepub.com/content/19/4/357.refs.htmlCitations:
What is This?
- Apr 22, 2013OnlineFirst Version of Record
- Jul 3, 2013Version of Record >>
at University of Texas at El Paso on August 18, 2014cat.sagepub.comDownloaded from at University of Texas at El Paso on August 18, 2014cat.sagepub.comDownloaded from

Original Article
Venous Thromboembolism in ElderlyHigh-Risk Medical Patients: Time Courseof Events and Influence of Risk Factors
Russell D. Hull, MBBS, MSc1, Tazmin Merali, BPharm, MBA2,Allan Mills, PharmD3, Abigail L. Stevenson, DPhil4, andJane Liang, MSc1
AbstractVenous thromboembolism (VTE) causes significant morbidity and mortality in hospitalized medical populations; however, medicalpatients do not currently receive thromboprophylaxis beyond their hospital stay. We reviewed the real-life occurrence of VTE-related care for 100 days post-hospitalization in Calgary, Canada. Using medical visit records with a unique patient identifier num-ber applied throughout the city’s hospitals, 989 high-risk patients were selected for review. Almost three-quarters of the elderlypatients received appropriate prophylaxis while in hospital, and only 2% received prophylaxis on discharge. Over the 100-dayfollow-up, 21% of the patients presented with clinically suspected VTE, of which 3.8% had confirmed VTE. Patients with multiplerisk factors (�3) had the highest frequency of confirmed VTE (�6.1%). This study suggests that the actual rate of VTE-relatedfollow-up care in patients post-hospitalization is high in the first 100 days, particularly among those who have multiple risk factors,warranting consideration of extended thromboprophylaxis in this population.
Keywordsvenous thromboembolism, thrombosis prophylaxis, anticoagulants, deep venous thrombosis, pulmonary embolism, thrombosis
Introduction
Hospitalized medical patients are at high risk of venous throm-
boembolism (VTE), with approximately one-quarter of all
VTE events occurring in this nonsurgical population.1 A
prospective cohort study suggested a symptomatic, clinically
evident VTE rate of 11% for hospitalized high-risk medical
patients not receiving prophylaxis,2 and there is strong evi-
dence that thromboprophylaxis in this population results in
fewer VTE events and reduced mortality.1 As such, the
American College of Chest Physicians recommends pharmaco-
logical prophylaxis for acutely ill hospitalized medical patients
at increased risk of thrombosis, but does not recommend
extending the duration of therapy beyond the period of immo-
bilization or hospital stay.1 The American College of Physi-
cians (ACP) also recommends prophylaxis with heparin (or
related drug) for medical patients, unless the assessed risk of
bleeding outweighs the benefits of thromboprophylaxis.3 Risk
factors for VTE in hospitalized medical patients include
increasing age (especially >70 years), previous VTE, known
thrombophilia, immobilization for �3 days, hormonal medica-
tions, and history of comorbid illness (eg, cancer, heart failure,
and respiratory failure).1 Further research is needed to validate
the risk factors for VTE, as prophylaxis may harm patients who
are at low risk of VTE but at high risk of bleeding; yet, its
underuse may result in avoidable mortality and morbidity.1
Much of the current evidence focuses on VTE risk of
medical patients during hospitalization, with some evidence
to suggest the risk extends beyond hospital stay. The
EXCLAIM trial examined extended-duration thromboprophy-
laxis with enoxaparin in hospitalized medical patients, which
determined a 90-day VTE incidence of 4.4% in medical
patients not receiving postdischarge prophylaxis.4 Similarly,
the MEDENOX trial suggested that VTE risk in medical
patients extends for up to 3 months, with 8 VTE events (includ-
ing 4 fatal pulmonary embolisms) occurring between days 15
and 110 after discharge.5 However, both these studies were ran-
domized clinical trials that used routine diagnostic screening in
addition to clinical events to calculate the rates of VTE and had
strict exclusion criteria for their study populations, which
1 Department of Medicine, Thrombosis Research Unit, University of Calgary,
Canada2 Drug Intelligence Inc, Toronto, Ontario, Canada3 Trillium Health Centre, University of Toronto, Ontario, Canada4 Watermeadow Medical, Macclesfield, United Kingdom
Corresponding Author:
Russell D. Hull, Department of Medicine, Thrombosis Research Unit, University
of Calgary, Foothills Medical Center, 1403 29 Street NW, Calgary, Alberta,
Canada.
Email: [email protected]
Clinical and AppliedThrombosis/Hemostasis19(4) 357-362ª The Author(s) 2013Reprints and permission:sagepub.com/journalsPermissions.navDOI: 10.1177/1076029613481105cath.sagepub.com
at University of Texas at El Paso on August 18, 2014cat.sagepub.comDownloaded from

excluded risk factors for bleeding. In comparison, few ‘‘real-
life’’ studies have been performed which identified sympto-
matic, clinically evident VTE events in populations not
screened for risk factors for bleeding; an example is the
IMPROVE observational study, which showed that 45% of the
VTE events occurred after discharge in medical patients.6 Such
‘‘real-life data’’ regarding the timing of VTE events in high-
risk medical patients after leaving hospital are lacking, and the
relationship between risk factors and VTE in this population
has not been fully examined. Furthermore, data are lacking
on rates of VTE in high-risk subgroups of patients, such as
those with cancer. Previous retrospective cohort database stud-
ies have estimated the incidence of VTE in hospitalized
patients with cancer to be between 0.6% and 5.4%, but there are
few data on rates in discharged patients.7,8 Our objective was to
document the time course of symptomatic VTE events in high-
risk elderly medical patients over 100 days postdischarge and
to correlate the frequency of risk factors for the likelihood of
VTE development. A subgroup analysis of these medical
patients with cancer was also performed. These data recorded
in everyday clinical practice may help to clarify the VTE risk
of ‘‘real-world’’ medical patients and to determine the appro-
priateness of long-term VTE prophylaxis in high-risk elderly
medical patients, including those with cancer, as well as to
establish strategies regarding the frequency of clinical surveil-
lance postdischarge in these populations.
Methods
Study Design
Data from the charts of high-risk elderly medical patients
hospitalized in the Calgary region and discharged between Jan-
uary 1, 2008 and February 28, 2008 were collected using case
records and screened for eligibility. All identified patients were
followed for any subsequent medical attention related to VTE.
All hospitals in the region use a unique patient identifier num-
ber, enabling the tracking of subsequent patient visits to the
emergency room, inpatient admissions, or outpatient visits
occurring anywhere in the region’s acute care system. Data
were collected on patient’s risk factors, thromboprophylaxis
received in hospital or at discharge, and VTE-related events for
up to 100 days postdischarge. Statistical methods used were as
follows: Wilson procedure without correction for continuity
was applied to calculate the proportion of patients with VTE
symptoms and confirmed events, including 95% confidence
intervals. Chi-square tests of association were used for asses-
sing the association between the number of risk factors and the
rates of VTE. Further details of methods can be found in the
protocol in the Online Supplementary Information.
Inclusion and Exclusion Criteria
High-risk elderly medical patients were defined as aged >60
years and having at least one of the following risk factors:
history of malignancy, respiratory illness, neurological illness,
inflammatory bowel disease, previous VTE, acute infection, or
heart failure. Medical patients with cancer were defined as
those aged >60 years with a cancer diagnosis at hospital admis-
sion, had a planned cancer surgery, were receiving cancer/pal-
liative treatment or whose cancer treatment was not specified;
patients with a remote history of cancer were excluded.
Records were excluded if the patient was originally admitted
for VTE, or to rule out VTE, receiving chronic anticoagulation,
experiencing an acute coronary syndrome, had a hospital stay
� 3 days, was a surgical or orthopedic patient, or was pregnant.
Outcome Measures
Outcomes included any medical attention for VTE symptoms
up to 100 days postdischarge, including emergency room
admissions, outpatient visits, or readmissions. The patients
were classed as confirmed VTE if they were subsequently
confirmed by diagnostic testing.
Results
Study Population: High-risk Elderly Medical Patients
Of the 1134 hospital discharges in the review period, 989
(87%) were identified as consecutive high-risk elderly medical
patients that met eligibility criteria and were selected for
Table 1. Rate and Time Course of VTE Events: All High-Risk Elderly Medical Patients Compared With Elderly Medical Patients With Cancer.a
All high-risk acute medicalpatients (n ¼ 989)
Acute medical patientswith cancer (n ¼ 358)
% Female 55% (543) 51% (181)Mean age/median age, years 79/79 79/78Age range, years 62–107 64–101Clinically suspected VTE requiring medical care and objective testing 21.0% [18.5–23.7] (208) 22.9% [18.7–27.6] (82)VTE event confirmed by diagnostic testing 3.8% [2.7–5.2] (38) 4.7% [2.8–7.5] (17)Negative/inconclusive diagnostic test for VTE 17.2% [14.9–19.7] (170) 18.2% [14.3–22.5] (65)Mean time to VTE event (days + SE [95% CI]) 33.5 + 5.1 [23.1–43.9] 38.2Median time to VTE event (days) 23 28
Abbreviations: CI, confidence interval; SD, standard error; VTE, venous thromboembolism.a Data are % [95% CI], (n) unless otherwise stated. In the subpopulation of high-risk elderly medical patients receiving inhospital prophylaxis, the frequency ofconfirmed VTE was 4.2% (31 of 733). Statistical analysis of the mean time to VTE event in the cancer subgroup was not performed.
358 Clinical and Applied Thrombosis/Hemostasis 19(4)
at University of Texas at El Paso on August 18, 2014cat.sagepub.comDownloaded from
follow-up as the high-risk group. Baseline demographics are
shown in Table 1. This population included all cases with risk
factors, but ruled out those where a complicating factor may
cloud the causation of VTE (eg, currently has/suspected of
having VTE, surgical cases, and acute coronary syndromes).
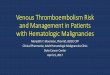
Data extracted from patient charts determined the incidence
of medical risk factors for the study population and VTE
prophylaxis prescribed (Figure 1A and B).
Symptomatic VTE Rates and Time Course Postdischarge:High-Risk Elderly Medical Patients
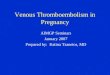
Rates of VTE and length of time from discharge to first
confirmed VTE event for the high-risk group are shown in
Table 1. The cumulative event rate over time determined that
80% of the confirmed VTE events occurred within 57 days
after discharge (Figure 2).
Correlation of VTE Rates with Risk Factors: High-riskElderly Medical Patients
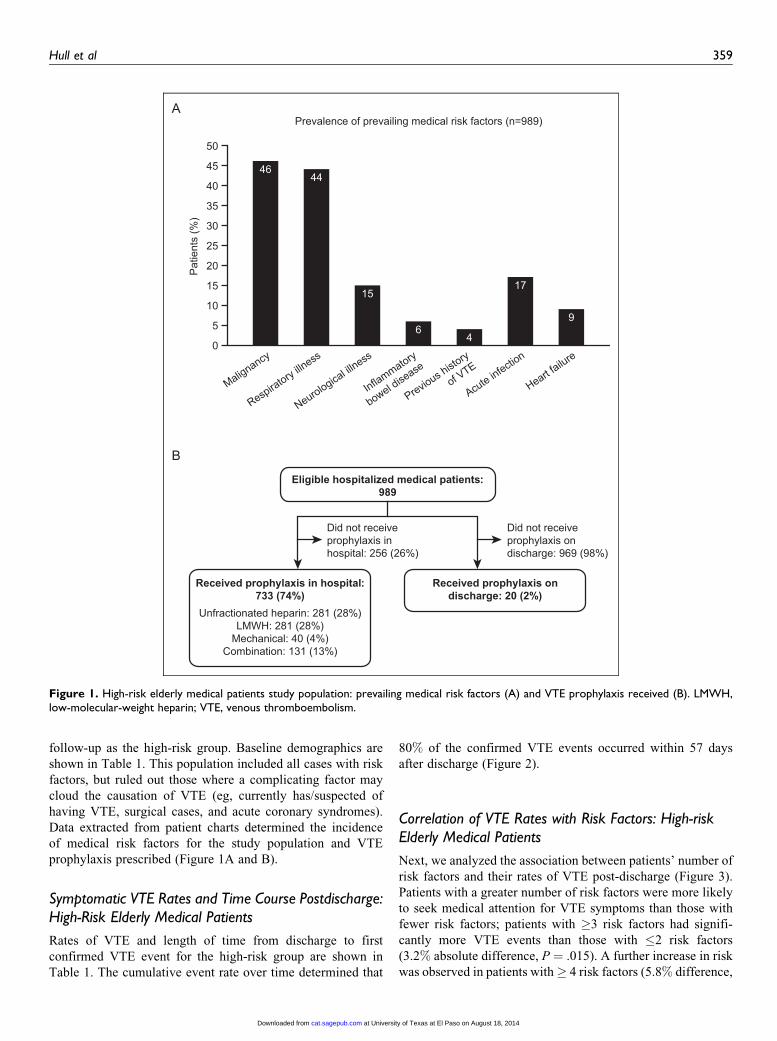
Next, we analyzed the association between patients’ number of
risk factors and their rates of VTE post-discharge (Figure 3).
Patients with a greater number of risk factors were more likely
to seek medical attention for VTE symptoms than those with
fewer risk factors; patients with �3 risk factors had signifi-
cantly more VTE events than those with �2 risk factors
(3.2% absolute difference, P ¼ .015). A further increase in risk
was observed in patients with� 4 risk factors (5.8% difference,
50
A
B
45
40
35
30
25
20
15
10
5
0
Prevalence of prevailing medical risk factors (n=989)
Pat
ient
s (%
)
Malignancy
46
Respiratory illness
44
Neurological ill
ness
15
Inflammatory
bowel disease
6
Previous h
istory
of VTE
4
Acute infection
17
Heart failure
9
Eligible hospitalized medical patients:989
Did not receiveprophylaxis inhospital: 256 (26%)
Did not receiveprophylaxis ondischarge: 969 (98%)
Received prophylaxis in hospital:733 (74%)
Unfractionated heparin: 281 (28%)LMWH: 281 (28%)
Mechanical: 40 (4%)Combination: 131 (13%)
Received prophylaxis ondischarge: 20 (2%)
Figure 1. High-risk elderly medical patients study population: prevailing medical risk factors (A) and VTE prophylaxis received (B). LMWH,low-molecular-weight heparin; VTE, venous thromboembolism.
Hull et al 359
at University of Texas at El Paso on August 18, 2014cat.sagepub.comDownloaded from
P ¼ 0.011 vs �2 risk factors), but this was not statistically
significant when compared to patients with �3 risk factors.
Subpopulation Analysis: VTE Rates and Time Course inPatients With Acute Cancer
Of the 1134 hospital discharges in the review period, 358
(32%) patients met the criteria for inclusion as medical patients
with cancer in the subpopulation analysis. In all, 73% (261 of
358) of the subgroup received mechanical or pharmacological
prophylaxis in hospital, whereas only 2% of all the patients
received anticoagulation prophylaxis after discharge. The
results of the subpopulation analysis of patients with cancer are
shown in Table 1.
Interpretation
We selected the records of high-risk elderly medical patients,
including a subset of elderly medical patients with cancer,
discharged from hospital in Calgary during a 2-month period
in 2008 and followed them for 100 days for subsequent VTE
events. Almost three-quarters of the patients in both the groups
received appropriate prophylaxis while in hospital and only 2%received prophylaxis on discharge, in keeping with current
ACP guidelines not to prescribe prophylaxis on discharge.3
Throughout the entire follow-up, a considerable proportion of
the study population presented with clinically suspected VTE,
requiring medical care and objective testing (21% of the entire
study population and 23% for the cancer subgroup), resulting in
rates of confirmed VTE diagnoses of 4% for the entire study
population and 5% in the cancer subgroup. The cumulative
event rate over time revealed that the majority of these cases
occurred just over 1 month after discharge (mean time to VTE
event: 34/38 days in the high-risk/cancer subgroup). In the sub-
group population with cancer, it was noted that 23% sought out
medical attention for VTE symptoms, with 5% having a con-
firmed VTE diagnosis. Furthermore, this population followed
the same pattern of VTE event rates with a mean time to VTE
of 38 days. As expected, patients with a greater number of risk
factors had a higher prevalence of VTE: 6% of hospitalized
medical patients with �3 risk factors developed symptomatic
VTE confirmed by diagnostic testing, which increased to
8.7% for those with �4 risk factors. Only 2.9% of the patients
with �2 risk factors developed VTE.
The age criterion of >60 years was chosen due to the signif-
icantly increased rates of VTE in older patients compared with
younger patients,9 which ensured enough events would occur
to achieve statistical significance. The high-risk criteria chosen
for this study are supported by risk factors identified in the
EXCLAIM study, where patients >75 years were identified
as a key group to target for prophylaxis, being at a greater risk
of VTE than bleeding.4 As such, the majority of the discharged
population were classified as high risk in our study, but this
may not reflect the demographics of all centers or those of other
countries. Also, this study had a high proportion of patients
with malignancy (46%) when compared to a previous analysis
(9%),10probably due to 1 of the 3 hospitals chosen being a
major cancer treatment center. Notably, the rate of high-risk
elderly medical patients seeking out medical attention for VTE
symptoms in our real-life review (21%) was higher than rates
observed in clinical studies; in MEDENOX, only 17% of the
patients in the placebo group experienced VTE up to 110 days
after discharge.5 Despite inhospital prophylaxis, our real-life
study showed dramatically higher symptomatic VTE rates
postdischarge than the LIFENOX study: only 0.7% in the
placebo group.11 This result was not unexpected, since routine
screening for thrombosis is often performed in clinical trials,
but not in everyday clinical practice, so it is thought sympto-
matic VTE rates are underestimated in clinical trials compared
to real-life settings; screening and/or treating for asymptomatic
VTE in clinical trials reduces the potential for these thrombi to
progress and become symptomatic.1 Also, LIFENOX studied a
40
35
30
25
20
15
10
5
00 10 20 30
Interquartilerange
40 50 60 70 80 90 100Days (post-discharge)
Cum
ulat
ive
num
ber o
f VTE
eve
nts
Figure 2. Cumulative event rate over time: high-risk elderly medicalpatients. VTE, venous thromboembolism.
20181614121086420
≤2Pat
ient
s w
ith a
con
firm
ed V
TE e
vent
(%)
2.9
Number of risk factors
p=0.015
≥3
p=0.01
p=NS
6.1
≥4
8.7
Figure 3. Influence of risk factors on rates of VTE. Data are the per-centage of patients with confirmed VTE, according to the presence ofrisk factors for VTE. Error bars represent 95% CIs. CI, confidenceinterval; VTE, venous thromboembolism.
360 Clinical and Applied Thrombosis/Hemostasis 19(4)
at University of Texas at El Paso on August 18, 2014cat.sagepub.comDownloaded from

patient population discharged with elastic stockings, which is
unrepresentative of Canadian practices.11 In our study, 4% of
the high-risk elderly medical patients had a VTE confirmed
by diagnostic testing in the postdischarge follow-up period, a
total of 38 events. This is consistent with EXCLAIM, which
reported a VTE incidence of 4.4% in a 90-day period in
medical patients not receiving postdischarge prophylaxis.4 Our
100-day follow-up was chosen to ensure the plateau in the time
course of VTE events was captured in order to identify an
optimal time to consider prophylaxis; indeed our design was
successful, identifying the plateau of events, with the number
of events reducing after day 50. Previous clinical trials studying
postdischarge VTE rates in medical patients have shorter
follow-ups (ADOPT: 30 days)12; our study suggests these
follow-up periods are not long enough for a complete evalua-
tion of the benefits of prolonged prophylaxis.
As expected, patients with a greater number of risk factors
had a higher prevalence of VTE events than those with fewer
risk factors. This correlation is in agreement with risk assess-
ment models of similar at-risk groups, both in hospitalized
patients2 and in those post-discharge.6 However, are the rates
of VTE in a high-risk older population sufficient to outweigh
the risks of bleeding? Our data, showing a VTE risk of over
6% in patients with � 3 risk factors, increasing to 9% in those
with �4, suggests targeting prophylaxis to these high-risk
subgroups has a more favorable risk-benefit profile than
observed in the overall medical populations examined in
previous studies, such as EXCLAIM, ADOPT, and MAGEL-
LAN.4,12,13 Patients with �2 risk factors had a lower rate of
VTE (2.9%). Our results need to be balanced with the outcomes
of EXCLAIM, which while not supporting a general need
for extended thromboprophylaxis in a hospitalized medical
population, identified high-risk subgroups where the benefit
did outweigh the risks.4 Prolonged use of enoxaparin prevented
6 fewer symptomatic VTE cases per 1000 patients but at a cost
of 5 more major bleeding events per 1000; however, the bene-
fits of additional prophylaxis outweighed the risks of bleeding
in high-risk subgroups: women, patients >75 years and those
without bathroom privileges.4 Our real-life study shows that
a subset of high-risk patients >60 years may also benefit from
extended use of thromboprophylaxis. In particular, patients >60
years with cancer may benefit, since approximately 1 in 20
patients experienced a confirmed VTE event in our review
post-discharge. Our data support the use of clinical risk factors
at hospital admission to predict VTE risk in medical patients
and suggest that the short courses of prophylaxis currently
prescribed predischarge may not adequately provide coverage
for those at highest risk.
Strengths and Limitations
Traditionally, chart review data are seen as weak due to their
many limitations; however, our study design has unique
strengths, making it a more robust study. The Calgary region
has a single, integrated information system used across acute
care sites, so tracking of all subsequent visits was possible
using the unique Calgary patient identifier. Also, the location
is geographically isolated, minimizing the likelihood of
patients seeking medical attention elsewhere, maximizing the
chances of patient follow-up. However, there are inherent lim-
itations of chart reviews; unlike clinical trials, our review was
an uncontrolled, epidemiological study carried out in everyday
clinical practice, not designed to measure efficacy or safety. As
safety outcomes were not measured, a comprehensive risk-
benefit analysis was not possible. Also, as our study relied on
data accuracy in the patients’ charts, incomplete
documentation may be a limitation. Our study relied on the
patient to seek out medical attention for VTE symptoms to
determine event rates, so patients not seeking attention, who
died or went to alternative care providers would not be
captured. Finally, the prophylaxis practices and the patient
population in the Calgary region may not be representative
of, or be applicable to, other centers and/or countries.
Conclusion
Our study suggests that in a real-life setting, cumulative risk
factors (including cancer) result in an increased risk of VTE
events post-discharge in a hospitalized medical population. A
mean prevalence of 4% confirmed VTE (increasing to 6% and
9% in patients with �3 or �4 risk factors, respectively) was
recorded, with patients continuing to seek medical attention for
VTE symptoms up to 100 days postdischarge, with 34 days
being the mean time to first event. Evidence-based guidelines
do not currently support extended prophylaxis for medical
patients,1 yet our data show that the risk extends well beyond
a typical hospital stay. The 4% VTE rate was greater than
expected for a real-life study and may change the perception
of a low benefit-to-risk ratio of prophylaxis upon discharge.
Coupled with the results of the EXCLAIM study, the VTE rates
observed here may suggest that prolonged VTE prophylaxis
may be of benefit in high-risk medical populations, such as
older patients. These data also highlight the problem of early
discharge before adequate prophylaxis can be administered.14
However, such extended prophylaxis would increase the cost
of therapy and may increase the bleeding risk of certain
patients. Indeed, recent trials have failed to show an increased
benefit-to-risk ratio of novel oral anticoagulants over
traditional subcutaneous (sc) thromboprophylaxis; the MAGEL-
LAN study determined an increased bleeding profile of oral
rivaroxaban compared with sc enoxaparin,13 whereas the
ADOPT study found increased bleeding and no superior efficacy
with oral apixaban compared with sc enoxaparin.12 Therefore, a
patient’s individual benefit-risk assessment must always be
taken into account1 when considering prophylaxis. Further,
large-scale clinical trials and real-life studies are warranted to
confirm the relative risks and benefits of extended thrombo-
prophylaxis in high-risk elderly medical patients postdischarge.
Authors’ Note
This study was presented orally at the annual meeting of the American
Society for Hematology (ASH) in Orlando, FL, December 2010.
Hull et al 361
at University of Texas at El Paso on August 18, 2014cat.sagepub.comDownloaded from

Authors’ Contribution
R.D. Hull had the original idea for the study, provided guidance and
input into all drafts, and is the guarantor of the study. J. Liang
performed the statistical analyses and reviewed and approved all
drafts. A.L. Stevenson interpreted data, wrote the first draft, and
approved the final draft. T. Merali developed the study protocol,
supervised data collection, data management, analysis, and reviewed
all drafts. A. Mills provided clinical assistance in reviewing the
results, provided input into the drafts, and reviewed all drafts.
Declaration of Conflicting Interests
The author(s) declared a potential conflict of interest as follows: R.D.
Hull has received grants/research support from Bayer Pharmaceuticals
Corp, LEO Pharma Inc, and Sanofi-Aventis; been a consultant for
Bayer Pharmaceuticals Corp, LEO Pharma Inc, Pfizer Inc, GlaxoS-
mithKline, and Wyeth Pharmaceuticals; and sat on advisory boards for
Bayer Pharmaceuticals Corp, Pfizer Inc, and Sanofi-Aventis. A. Ste-
venson is an employee of Watermeadow Medical, which received
payment from the Medical Continuing Education Fund, University
of Calgary for work on this manuscript. Editorial assistance was
provided by Watermeadow Medical. T. Merali is an employee of Drug
Intelligence, which received payment from the Thrombosis Research
Group, University of Calgary for work on this study. J. Liang and A.
Mills have no conflicts of interest to declare.
Funding
The author(s) disclosed receipt of the following financial support for
the research and/or publication of this article: This work was funded
by Sanofi-Aventis, Canada.
References
1. Kahn SR, Lim W, Dunn AS, et al; American College of Chest
Physicians. Prevention of VTE in nonsurgical patients: antithrom-
botic therapy and prevention of thrombosis. 9th ed. American
College of Chest Physicians Evidence-Based Clinical Practice
Guidelines. Chest. 2012;141(suppl 2):e195S-e226S.
2. Barbar S, Noventa F, Rossetto V, et al. A risk assessment model
for the identification of hospitalized medical patients at risk for
venous thromboembolism: the padua prediction score. J Thromb
Haemost. 2010;#8(11):2450-2457.
3. Qaseem A, Chou R, Humphrey LL, Starkey M, Shekelle P.
Venous thromboembolism prophylaxis in hospitalized patients:
a clinical practice guideline from the American college of physi-
cians. Ann Intern Med. 2011;155(9):625-632.
4. Hull RD, Schellong SM, Tapson VF, et al. Extended-duration
venous thromboembolism prophylaxis in acutely ill medical
patients with recently reduced mobility: a randomized trial. Ann
Intern Med. 2010;153(1):8-18.
5. Samama MM, Cohen AT, Darmon JY, et al. A comparison of
enoxaparin with placebo for the prevention of venous throm-
boembolism in acutely ill medical patients. N Engl J Med.
1999;341(11):793-800.
6. Spyropoulos AC, Anderson FA Jr, Fitzgerald G, et al. Predictive
and associative models to identify hospitalized medical patients at
risk for VTE. Chest. 2011;140(3):706-714.
7. Levitan N, Dowlati A, Remick SC, et al. Rates of initial and
recurrent thromboembolic disease among patients with malig-
nancy vs. those without malignancy. Risk analysis using Medi-
care claims data. Medicine. 1999;78(5):285-291.
8. Khorana AA, Francis CW, Culakova E, Fisher RI, Kuderer NM,
Lyman GH. Thromboembolism in hospitalized neutropenic
cancer patients. J Clin Oncol. 2006;24(3):484-490.
9. Stein PD, Hull RD, Kayali F, Ghali WA, Alshab AK, Olson
RE. Venous thromboembolism according to age: the impact
of an aging population. Arch Intern Med. 2004;164(20):
2260-2265.
10. Kahn SR, Panju A, Geerts W, et al. Multicenter evaluation of
the use of venous thromboembolism prophylaxis in acutely ill
medical patients in Canada. Thromb Res. 2007;119(2):
145-155.
11. Kakkar AK, Cimminiello C, Goldhaber SZ, Parakh R, Wang C,
Bergmann JF. Low-molecular-weight heparin and mortality in
acutely ill medical patients. N Engl J Med 2011;365(26):
2463-2472.
12. Goldhaber SZ, Leizorovicz A, Kakkar AK, et al. Apixaban vs.
enoxaparin for thromboprophylaxis in medically ill patients.
N Engl J Med. 2011;365(23):2167-2177.
13. Cohen AT, Spiro T, Buller H, et al; On behalf of the MAGELLAN
Steering Committee and Investigators. Rivaroxaban compared
with enoxaparin for the prevention of venous thromboembolism
in acutely ill medical patients. Paper presented at: American Col-
lege of Cardiology 60th Annual Scientific Session; April 2–5,
2011. Presentation number: 3015-6.
14. Stein PD, Hull RD, Matta F, Yaekoub AY. Early discharge of
patients with venous thromboembolism: implications regarding
therapy. Clin Appl Thromb Hemost. 2010;16(2):141-145.
362 Clinical and Applied Thrombosis/Hemostasis 19(4)
at University of Texas at El Paso on August 18, 2014cat.sagepub.comDownloaded from