Embed Size (px)
Citation preview
8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 1/31
CURVE PROGRESSION AFTER ANTERIORCURVE PROGRESSION AFTER ANTERIOR
SURGICAL CORRECTION OF SCOLIOSIS:SURGICAL CORRECTION OF SCOLIOSIS:TWO CASES REPORTTWO CASES REPORT
Nguyen Thanh Nguyen Thanh Nhan Nhan * *
, Do Tran Khanh,, Do Tran Khanh,Vo Quang Vo Quang Dinh Dinh Nam, Huynh Nam, Huynh Manh Manh Nhi Nhi , Vu Viet , Vu Viet Chinh Chinh
PaediatricPaediatric Orthopedic DepartmentOrthopedic Department ––Hospital forHospital for TraumatologyTraumatology andand OrthopaedicsOrthopaedics
Ho ChiHo Chi MinhMinh CityCity –– VietnamVietnam
* MD,* MD, PaediatricPaediatric OrthopaedicOrthopaedic Department, Medical UniversityDepartment, Medical University
8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 2/31
Peter O. Newton, Dennis R. WengerPeter O. Newton, Dennis R. Wenger
The indications for surgical correction of scoliosisThe indications for surgical correction of scoliosis::
-- Curve magnitudeCurve magnitude
-- Clinical deformityClinical deformity
-- Risk for progressionRisk for progression
-- Skeletal maturity, and curve pattern.Skeletal maturity, and curve pattern.
-- Thoracic curves of Cobb angle > 40 to 50Thoracic curves of Cobb angle > 40 to 50degrees in skeletally immature patientsdegrees in skeletally immature patientswhereas surgical correction is reserved forwhereas surgical correction is reserved forcurves of 50 degrees or more in mature patientscurves of 50 degrees or more in mature patients(lower risk of progression).(lower risk of progression).
-- Trunk deformity (rotation) and trunk balance areTrunk deformity (rotation) and trunk balance areimportant factors in deciding when to adviseimportant factors in deciding when to advise
surgical correction.surgical correction.
BACKGROUNDBACKGROUND

8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 3/31
Peter O. Newton, Dennis R. WengerPeter O. Newton, Dennis R. Wenger
Anterior instrumentation and fusionAnterior instrumentation and fusion generallygenerally
include those with a single structural deformityinclude those with a single structural deformity
(thoracic,(thoracic, thoracolumbarthoracolumbar or lumbar curves,or lumbar curves,
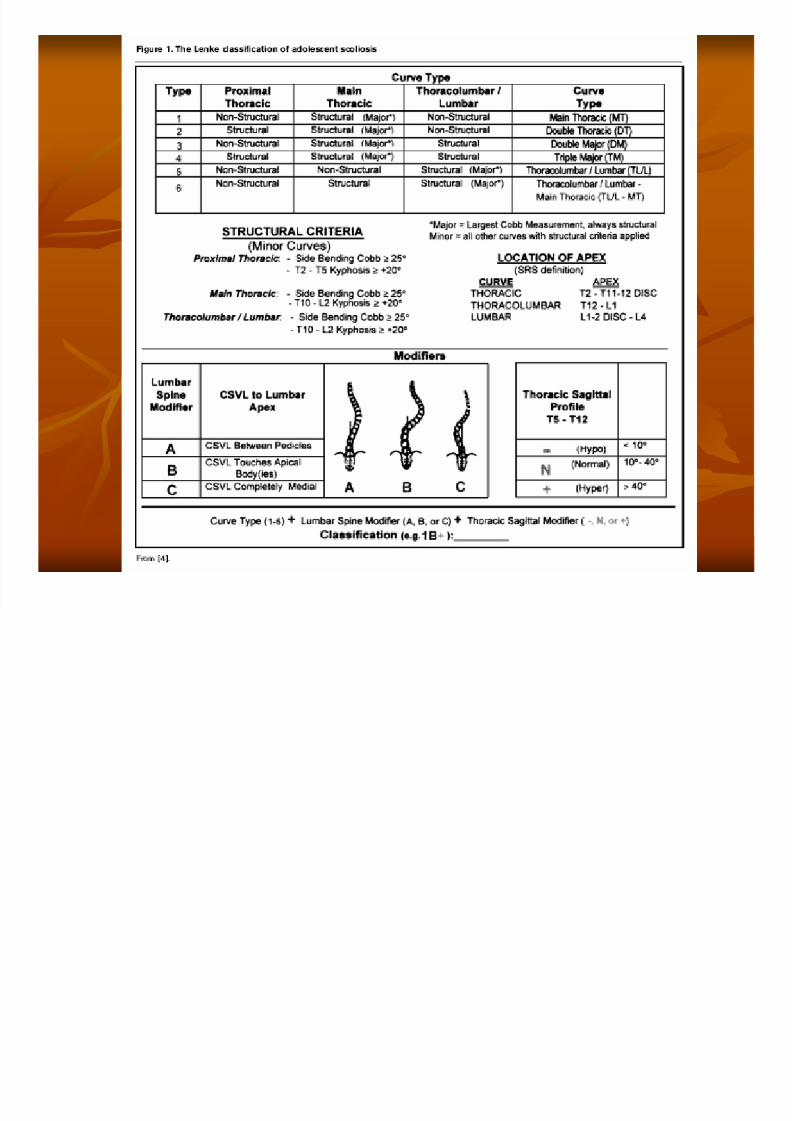
Lenke 1A B C, 5 C).Lenke 1A B C, 5 C).
BACKGROUNDBACKGROUND
8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 4/31
Lee S. Segal and Kelly L. Vanderhave
Anterior instrumentation is indicated for primarythoracic curves and thoracolumbar curves, with
the goal to save two or more levels compared
with that predicted for posterior
Fusion levels tend to extend from the proximal to
the distal end vertebrae measured in the Cobb
angle.
BACKGROUNDBACKGROUND
8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 5/31
The potential advantages
Avoiding disruption of the posterior extensormusculature
Decreased risk of junctional problems
Superior long-term correction of thecompensatory noninstrumented curves with lesspostoperative coronal decompensation
Improved ability to derotate the spine in thetransverse plane
Better correction of thoracic hypokyphosis
BACKGROUNDBACKGROUND

8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 6/31
The contraindications for anterior approach
- Significant preoperative kyphosis (>400),
- Curves greater than 800
- Impaired respiratory function (vital capacity < 50%)- And double or triple structural curves.
BACKGROUNDBACKGROUND
8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 7/31
Historical problems with anterior instrumentation
- Rod breakage- Pull-out of the proximal screw
- Pseudoarthrosis
- Kyphosis.
These problems have been addressed with theuse of larger rods, structural grafts and spacers to
provide anterior column reconstruction, andmaintaining lordosis for thoracolumbar curves.
BACKGROUNDBACKGROUND
8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 8/31
PURPOSEPURPOSE
To reviewTo review the indications for anterior surgicalthe indications for anterior surgical
correction of scoliosis.correction of scoliosis.
To evaluate used constructs.To evaluate used constructs.
To analyze the causes of progression ofTo analyze the causes of progression of
scoliosis.scoliosis.
8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 9/31
MATERIALS AND METHODSMATERIALS AND METHODS
Retrospective studyRetrospective study
10/200310/2003 -- 3/20093/2009
151 patients: 57 male, 94 female151 patients: 57 male, 94 female
Female.
62.25%
Male.
37.75%
8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 10/31
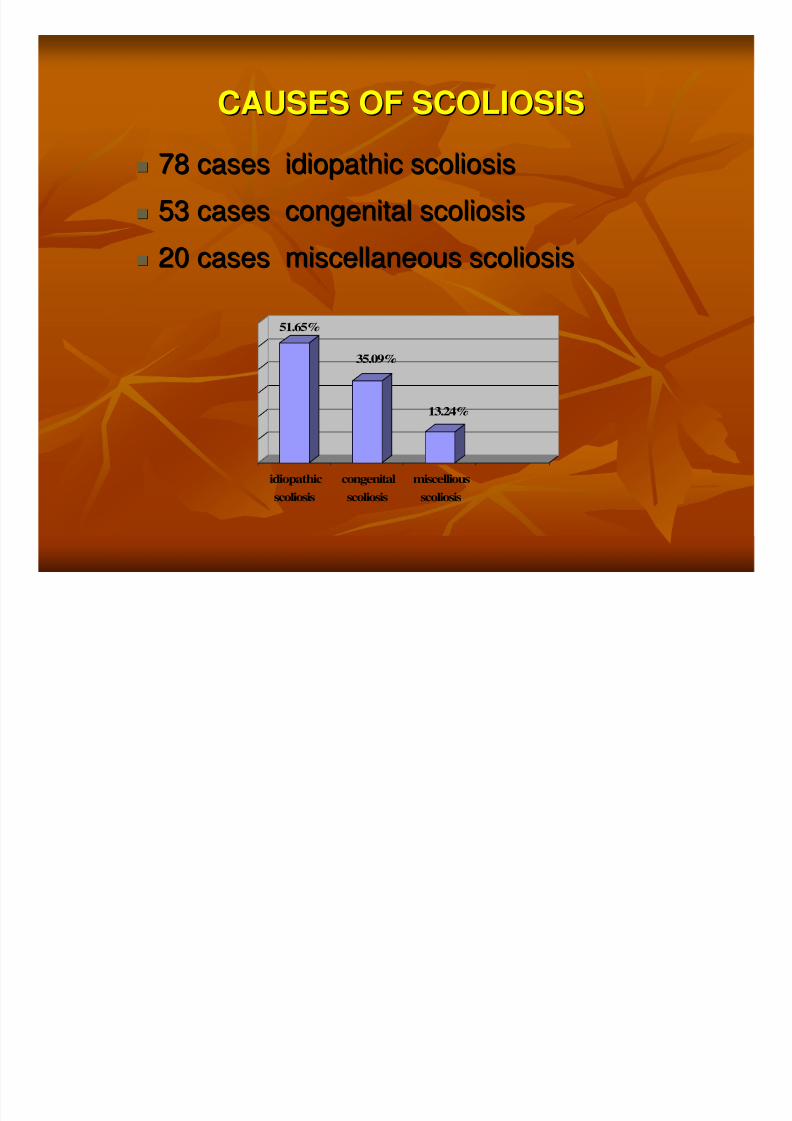
CAUSES OF SCOLIOSISCAUSES OF SCOLIOSIS
78 cases idiopathic scoliosis78 cases idiopathic scoliosis
53 cases congenital scoliosis53 cases congenital scoliosis 20 cases miscellaneous scoliosis20 cases miscellaneous scoliosis
51.65%
35.09%
13.24%
idiopathic
scoliosis
congenital
scoliosis
miscellious
scoliosis
8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 11/31
SURGERY OF IDOPATHIC SCOLIOSISSURGERY OF IDOPATHIC SCOLIOSIS
1. POSTERIOR INSTRUMENTATION (69 cases)1. POSTERIOR INSTRUMENTATION (69 cases)
5 cases Harrington rods without fusion5 cases Harrington rods without fusion
4 cases Harrington rods with4 cases Harrington rods with sublaminarsublaminar wireswires
1 case hooks only1 case hooks only
20 cases hybrid constructs with segmental translation20 cases hybrid constructs with segmental translation – – pedicle screws and hooks ( 4 cases used 3 rods )pedicle screws and hooks ( 4 cases used 3 rods )
39 cases all pedicle screws39 cases all pedicle screws
22.. ANTERIOR SURGERY TECHNIQUES (9 cases)ANTERIOR SURGERY TECHNIQUES (9 cases)
9 cases with an anterior single9 cases with an anterior single--rod construct / 2rod construct / 2
cases revision due to progressive scoliosiscases revision due to progressive scoliosis

8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 12/31
METHODSMETHODS
2/9 cases of anterior surgical correction of2/9 cases of anterior surgical correction of
scoliosis.scoliosis. ThoracoThoraco – – lumbar approach, discslumbar approach, discs discectomydiscectomy,,
vertebral screw with one single rod Moss Miami.vertebral screw with one single rod Moss Miami.
The results of correction are evaluated by CobbThe results of correction are evaluated by Cobbangle.angle.
PostPost--Op, wearing brace in 3Op, wearing brace in 3 – – 6 months.6 months.
Progressive scoliosis > 50Progressive scoliosis > 50
00
: posterior CD: posterior CDinstrumentation.instrumentation.
8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 13/31
RESULTSRESULTS
Time follow up (12, 30 months)Time follow up (12, 30 months)
First correction results: Percentage correctedFirst correction results: Percentage corrected(63%, 76%).(63%, 76%).
Curve progressed (Cobb angle: 26Curve progressed (Cobb angle: 2600 565600,,
202000 525200))
Posterior CD instrumentation. PercentagePosterior CD instrumentation. Percentage
corrected (82%, 35%), trunk balance, nocorrected (82%, 35%), trunk balance, no
complications.complications.
8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 14/31
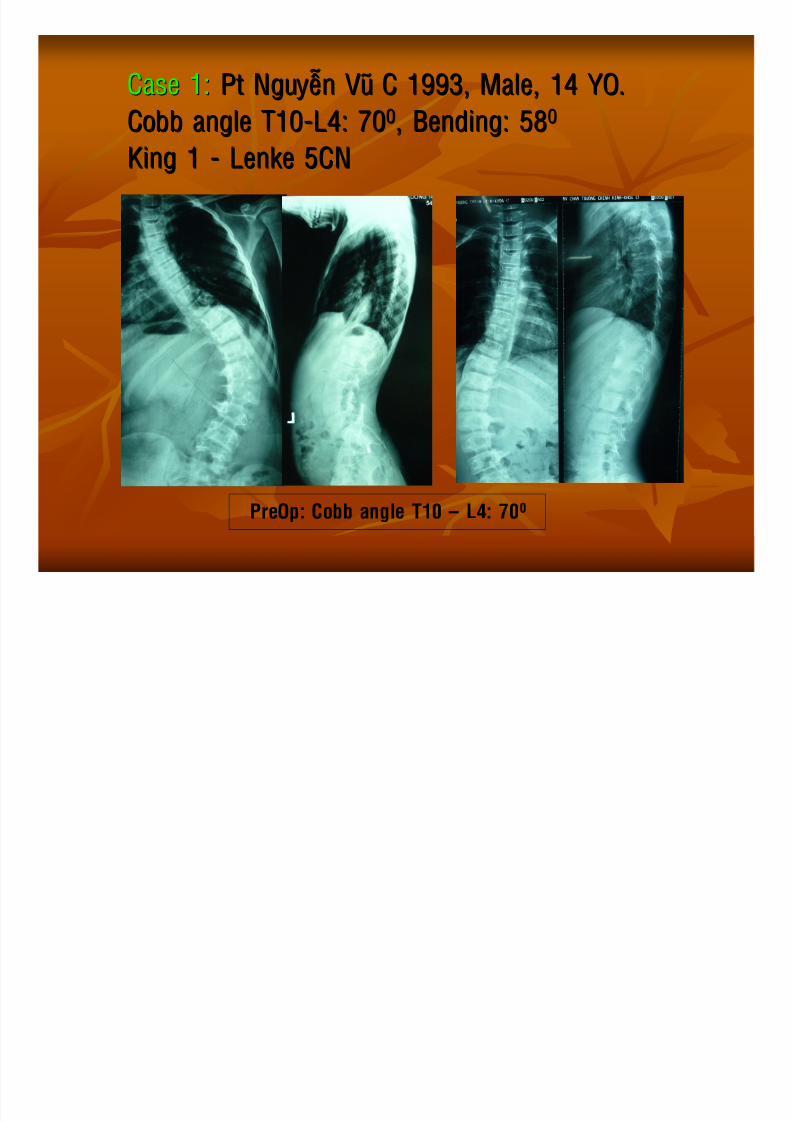
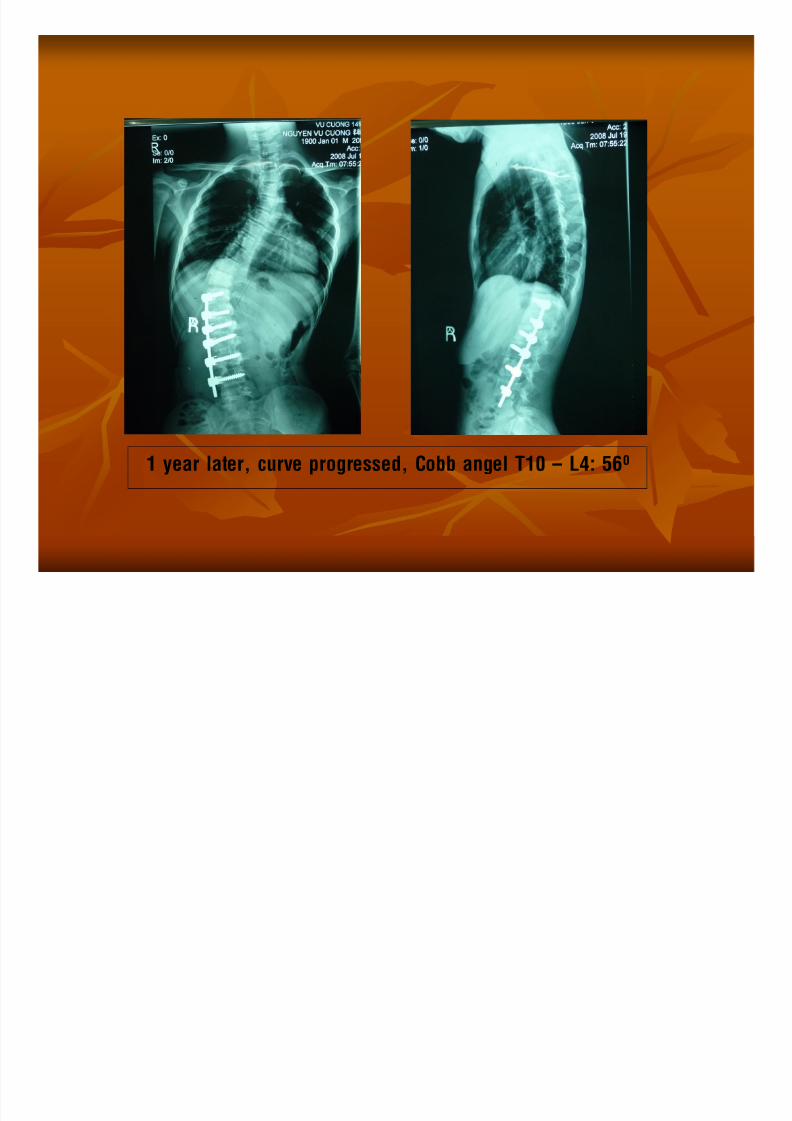
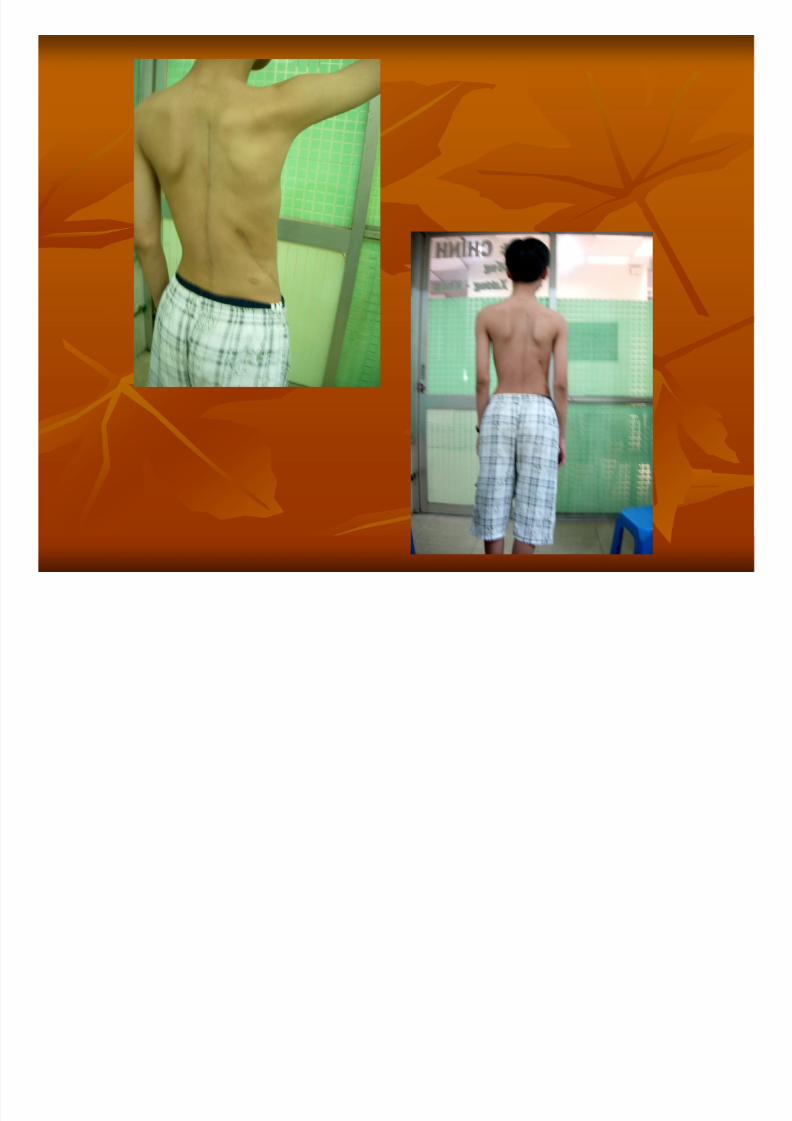
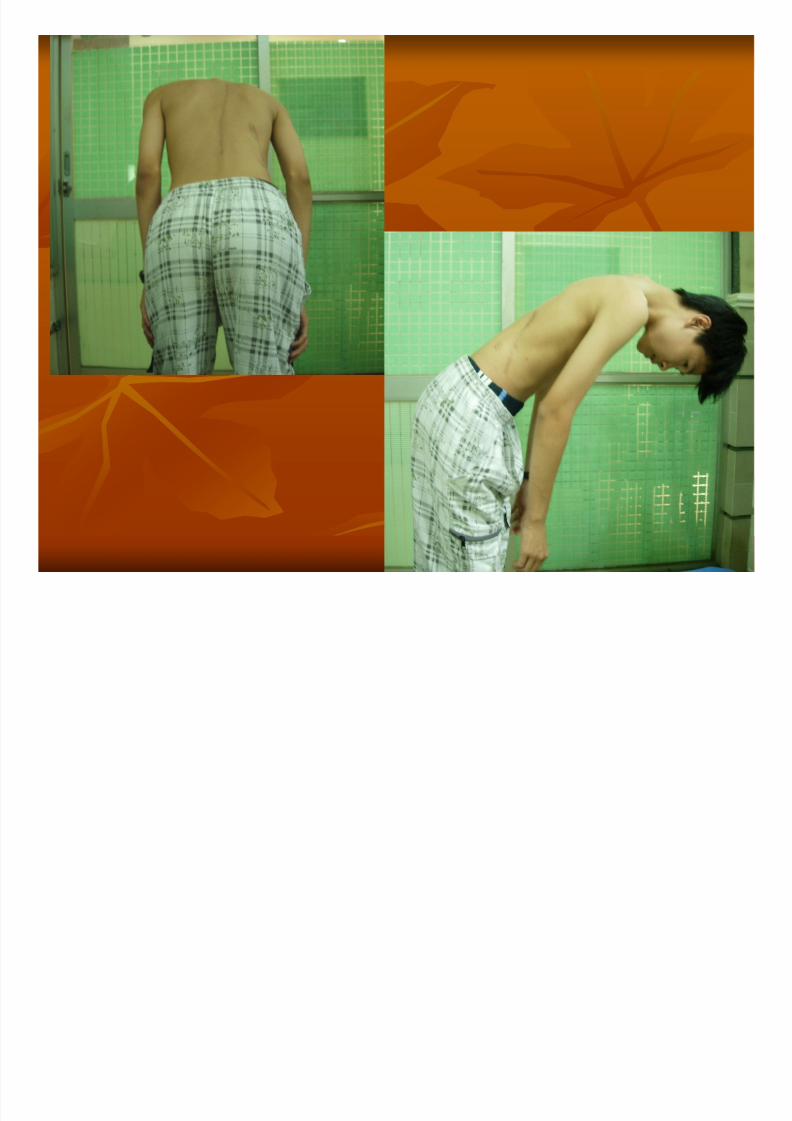
Case 1:Case 1: Pt Nguyeãn Vuõ C 1993, Male, 14 YO.Pt Nguyeãn Vuõ C 1993, Male, 14 YO.
Cobb angle T10Cobb angle T10--L4: 70L4: 7000, Bending: 58, Bending: 5800
King 1King 1 -- LenkeLenke 5CN5CN
PreOp: Cobb angle T10 – L4: 700
8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 15/31
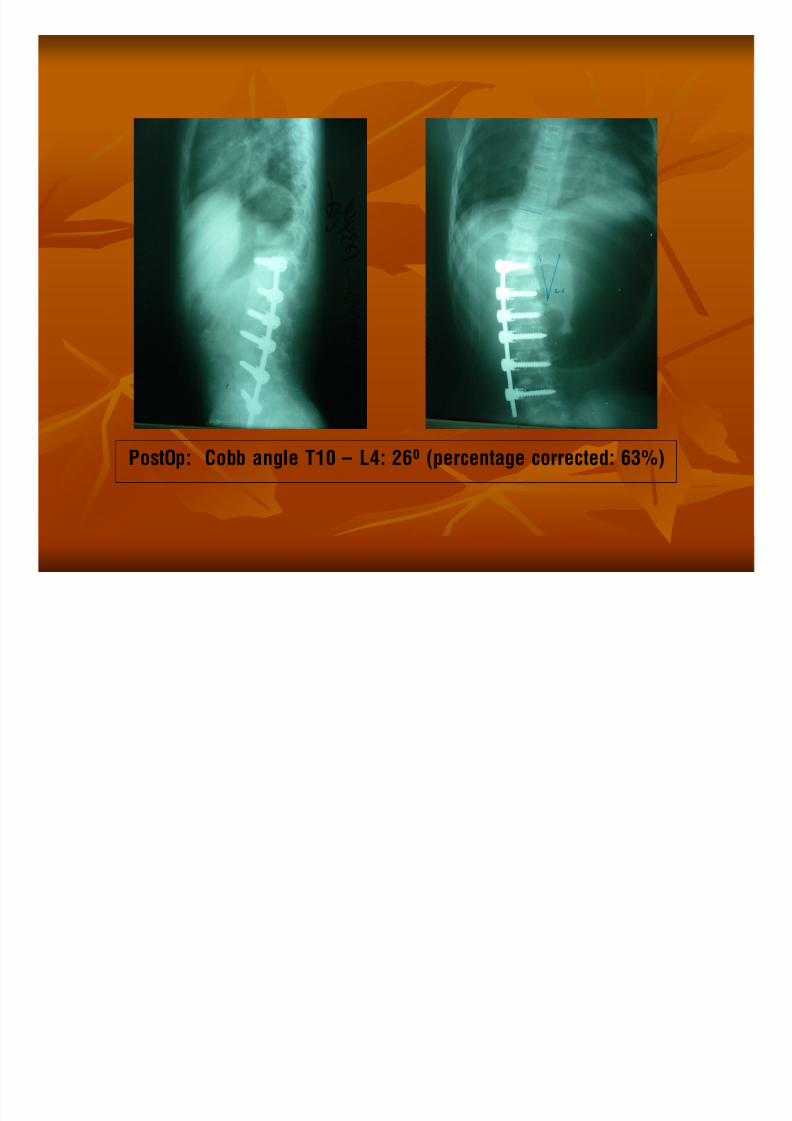
PostOp: Cobb angle T10 – L4: 260 (percentage corrected: 63%)
8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 16/31
1 year later, curve progressed, Cobb angel T10 – L4: 560

8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 17/31
X ray PostOp:Cobb angle T10 – L4: 100
(percentage corrected 82%)

8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 18/31
g
8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 19/31
8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 20/31
8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 21/31
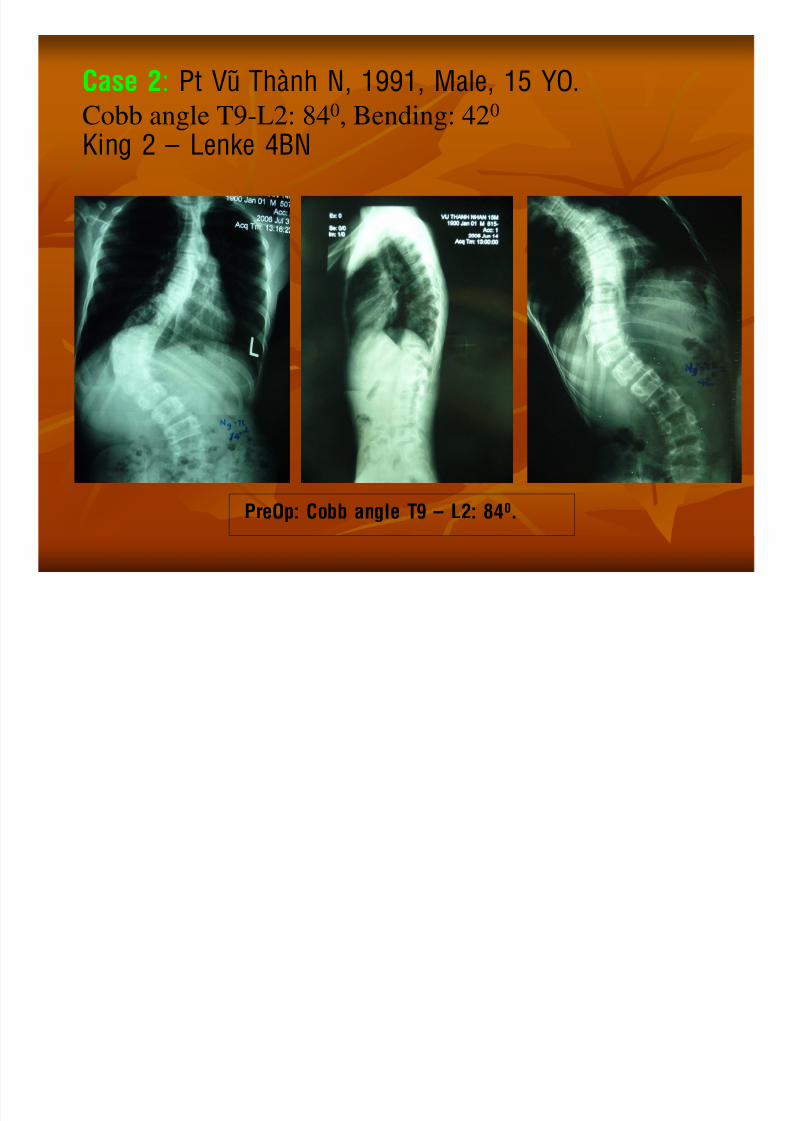
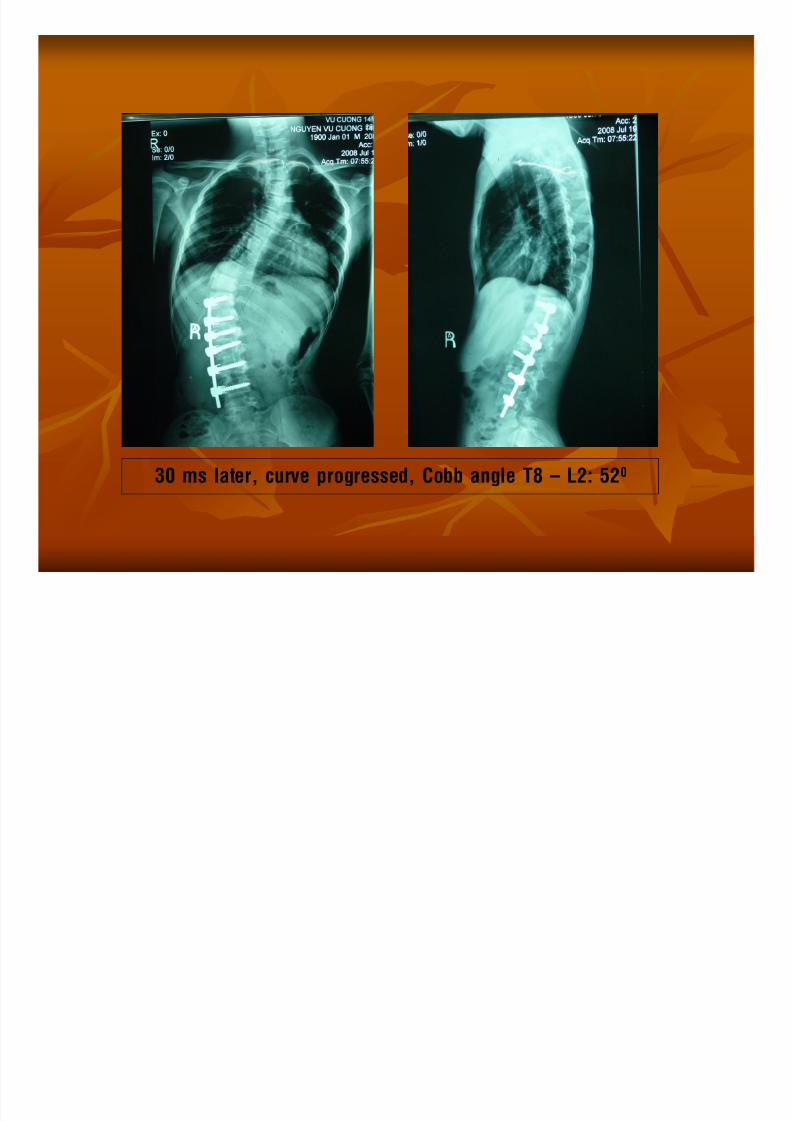
Case 2: Pt Vuõ Thaønh N, 1991, Male, 15 YO.
Cobb angle T9-L2: 840, Bending: 420
King 2 – Lenke 4BN
PreOp: Cobb angle T9 – L2: 840.

8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 22/31
PostOp: Cobb angle T9 – L2: 200 (percentage corrected: 76%)
8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 23/31
30 ms later, curve progressed, Cobb angle T8 – L2: 520

8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 24/31
PostOp:
Cobb angle T8 – L2: 340
(percentage corrected 35%)
8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 25/31
DISCUSSION
1. Surgery indication:
Case 1 (King 1, Lenke 5CN), anterior instrumentationindication is exact.
Case 2 (King 2, Lenke 4BN), anterior instrumentation
indication is wrong because of triple structural curve,
Cobb angle > 800 (840).
8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 26/31
DISCUSSION
2. Anterior constructs gave good correction results
(63%, 76%) but both are not enough long because of
not reaching the proximal end and distal endvertebrae of Cobb angle.
We wish to do longer but the approach not enough
long Choosing the approach in anterior surgery
must be exact, long enough to gain effective
construct . Case 1 need to put 2 levels higher.Anterior instrumentation should only indicated for type
of short single structural curve, thoraco-lumbar or low
thoracic. .
8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 27/31
DISCUSSION
3. Patient must wear brace enough time to have good
fusion. Need to closely follow up to detect progressive
curve.4. Adolescent patient (14, 15 YO, Risser V), still have
potential progressive scoliosis. Why?5. Have the problems in posterior instrumentation in
patient with anterior instrumentation?
Put pedicle screws.Have any interaction between different kinds of metal?
8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 28/31
CONCLUSION
Anterior spinal instrumentation gave good correction,
but need to indicate exactly.
Instruments need enough strong and long (from the
proximal end to distal end vertebrae of the Cobbangle).
Need to programe follow up the curve. Posterior
correction instrumentation may be a good option.
8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 29/31
8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 30/31
8/3/2019 Veo CS - Hoi Nhi, Tieng Anh - BS NHAN Hanoi 2009
http://slidepdf.com/reader/full/veo-cs-hoi-nhi-tieng-anh-bs-nhan-hanoi-2009 31/31





























