Embed Size (px)
Citation preview

Ž .International Journal of Gynecology & Obstetrics 72 2001 103]108
Article
Viral hepatitis during pregnancy
S.P.B. JaiswalU, A.K. Jain, G. Naik, N. Soni, D.S. Chitnis( )Choithram Hospital and Research Center, Indore MP , India
Received 1 October 1999; received in revised form 30 March 2000; accepted 5 April 2000
Abstract
Objecti e: A great degree of controversy prevails over the existing reports on the severity and outcome of acuteŽ .viral hepatitis AVH during pregnancy. The present study describes the outcome of AVH associated with pregnancy.
A correlation was also assessed for gestation period, viral etiology and outcome of AVH. Method: The serum samplesŽ .of 273 females with viral hepatitis age group 18]23 years were included in the study. Among them, 127 females
Ž .were pregnant and 146 were non-pregnant cases as a control group . The sera were screened for seromarkers of theŽ . Ž .hepatitis A virus HAV through to the hepatitis E virus HEV by the latest available generation ELISA kits.
Ž .Among the 127 pregnant females, 83 were AVH cases, while 44 were fulminant hepatic failure FHF cases. Amongthe 146 non-pregnant females, 129 were AVH and 17 were FHF cases. Result: Among the AVH pregnant females, 73Ž .57.5% had HEV infection. Fifty-eight percent of the HEV infected pregnant females were associated with FHF.
Ž .Among non-pregnant females HEV was documented in 67 46% cases. HBV infection was observed in 19% and18% of the pregnant and non-pregnant females, respectively. Twenty percent of the pregnant and 33% of the
Ž .non-pregnant females remained non-reactive for seromarkers of HAV]HEV. The mortality rate was highest 56%among HEV infected FHF cases during third trimester of pregnancy. The x2 test was applied to check the statisticalsignificance for the differences over the prevalence in various groups. Conclusion: In the present study, HEV wasfound to be the chief etiological agent, associated with higher morbidity and mortality. However, the incidence ofHEV in pregnant females was not significantly different from non-pregnant females. The prevalence of HAV, HCVand HDV were very low in the study. An increased incidence of FHF was noted among HEV infected pregnantfemales, while infection with an agent other than A]E was commonly associated with FHF among non-pregnantfemales. Q 2001 International Federation of Gynecology and Obstetrics. All rights reserved.
Ž . Ž .Keywords: Acute viral hepatitis AVH ; Fulminant hepatic failure FHF ; Females; Gestation period; Hepatitis viruses; Pregnancy
U Corresponding author. Tel.: q91-0731-362491-99; fax: q91-0731-470068.Ž .E-mail address: [email protected] S.P.B. Jaiswal .
0020-7292r01r$20.00 Q 2001 International Federation of Gynecology and Obstetrics. All rights reserved.Ž .PII: S 0 0 2 0 - 7 2 9 2 0 0 0 0 2 6 4 - 2

( )S.P.B. Jaiswal et al. r International Journal of Gynecology and Obstetrics 72 2001 103]108104
1. Introduction
Opinions differ over the maternal and fetaloutcome of pregnancies associated with viral hep-
w xatitis 1]10 . The studies from the developedcountries conclude that the pregnancy state, perse, has no adverse effect on the course of hepati-
w xtis, provided the nutrition is adequate 5]7 . How-ever, increased maternal and fetal mortality has
w xbeen reported by many groups 1]3 , mainly fromthe developing countries. Poor prenatal care andmaternal nutrition appear to have contributedsignificantly to the increased severity of infectionw x11,12 . Greater morbidity and mortality, particu-larly during epidemics of hepatitis, has been notedamong pregnant females in developing countriesw x1]3,8,9,11]16 . Earlier reports suggested thatnon-A non-B was the chief etiological agent for
w xsuch a severe disease 2,9,12]17 . Precise identi-fication of the viral agents could not be carriedout in the earlier studies because the serologicalidentification was not developed at the time, but
Ž .hepatitis E virus HEV -mediated hepatitis dur-ing pregnancy was assumed to lead to severe
w xdisease, with a poor prognosis in India 2,9,12 .Little data appeared from other parts of thedeveloping world over the poor maternal andfetal outcome of pregnancies associated with HEV
w xinfection 8,14,15 . The observations that HBVinfection can also adversely affect the outcome of
w xpregnancy 3 brought further controversy overthe sequelae of viral hepatitis during pregnancy.In view of this, we aimed to study the incidence of
Ž .hepatitis caused by viral agents HAV to HEVamong pregnant and non-pregnant females, andto study the outcome of the pregnancy.
2. Materials and methods
The study group comprised of 273 females withŽ .hepatitis age group 18]35 years coming to
Choithram Hospital and Research Center,Indore, India during the period of July 1992]May1999. Of these, 127 females were pregnant andamong them 83 females presented with acute
Ž . Ž .viral hepatitis AVH Group A while 44 femalesŽ .developed fulminant hepatitis FHF, Group B .
One hundred and forty-six females were non-pregnant and 129 of them presented as AVHŽ .Group C while the remaining 17 females devel-
Ž .oped fulminant hepatitis Group D . Among thepregnant females, 20, 33 and 30 with AVH, and 2,15 and 27 with fulminant hepatitis were in thefirst, second and third trimester of their gestationperiod, respectively. The selection of the candi-dates in groups B and D were based on the
w xaccepted standard criteria 18 and none of themhad a history of ingestion of known hepatotoxicdrugs or indigenous hepatotoxicity. The subjectsbelonged to the middle class income groups andthe nutritional status was satisfactory. The periodof gestation was calculated on the basis of datesof missed menstrual cycles and ultrasound find-ings.
The blood samples were collected by venepunc-ture from each patient and the sera kept at y208Cuntil analysis. All blood samples were subjectedto biochemical studies for liver function tests.Each patient’s serum was tested for viral hepatitisseromarkers using commercially available ELISA
Žkits. For the HBsAg Auszyme C, Abbott Diag-nostics, Illinois, USA; Hepanostika-Uniform-II,
.Organon Teknika, Boxtel, Netherlands , anti-ŽHBcIgM Hepanostika, Organon Teknika, Boxtel,
. ŽNetherlands ; anti-HAV IgM Hepanostika-,.Organon Teknika, Boxtel, Netherlands ; anti-
ŽHCV third generation ELISA kits Ortho HCV. Ž .4.0, USA and anti-HEV IgM Genelabs, Taiwan
kits were used. All HBsAg reactive samples wereŽ .also screened for anti-delta total antibodies by
ŽELISA kits Anti-Delta EIA, Abbott Diagnostics,.Illinois, USA .
3. Results
The data on viral etiological agents responsiblefor acute hepatitis andror fulminant hepatitis inpregnant and non-pregnant females is shown inTable 1. The prevalence of viral etiologies A]Ewas not different for pregnant and non-pregnantwomen. The incidence of acute viral hepatitis Bwas also similar for both pregnant and non-preg-nant females, but the incidence of fulminant hep-atitis B was greater among non-pregnant females

( )S.P.B. Jaiswal et al. r International Journal of Gynecology and Obstetrics 72 2001 103]108 105
Table 1aIncidence of various hepatitis viruses among pregnant and non-pregnant females with AVH and FHF
Subjects Gestation period No of Etiological Agentin trimester cases HAV HBV HCV HDV HEV AqE nA]nE
Pregnant First 20 0 7 0 0 10 0 3Ž . Ž . Ž . Ž . Ž . Ž . Ž .females with 0 35 0 0 50 0 15
Ž .AVH Group A Second 33 0 8 0 0 12 0 13Ž . Ž . Ž . Ž . Ž . Ž . Ž .0 24.24 0 0 36.36 0 39.39
Third 30 0 7 0 0 18 0 5Ž . Ž . Ž . Ž . Ž . Ž . Ž .0 23.23 0 0 60 0 16.66
All 83 0 22 0 0 40 0 21Ž . Ž . Ž . Ž . Ž . Ž . Ž .0 26.5 0 0 48.19 0 25.38
Pregnant First 2 0 0 0 0 2 0 0Ž . Ž . Ž . Ž . Ž . Ž . Ž .females with 0 0 0 0 100 0 0
Ž .FHF Group B Second 15 0 1 0 0 12 0 2Ž . Ž . Ž . Ž . Ž . Ž . Ž .0 6.6 0 0 80 0 13.33
Third 27 0 1 0 1 19 1 5Ž . Ž . Ž . Ž . Ž . Ž . Ž .0 3.7 0 3.7 70.3 3.7 18.5
All 44 0 2 0 1 33 1 7Ž . Ž . Ž . Ž . Ž . Ž . Ž .0 4.5 0 2.27 75 2.27 15.9
Total pregnant females 127 0 24 0 1 73 1 28Ž . Ž . Ž . Ž . Ž . Ž . Ž .0 18.89 0 0.78 57.48 0.78 22.04
Non-pregnant females With AVH 129 2 21 0 0 65 2 39Ž . Ž . Ž . Ž . Ž . Ž . Ž . Ž .Group C 1.5 16.27 0 0 50.38 1.5 30.23
Non-pregnant females With FHF 17 0 5 0 0 2 0 10Ž . Ž . Ž . Ž . Ž . Ž . Ž . Ž .Group D 0 29.41 0 0 11.76 0 58.82
Total non-pregnant females 146 2 26 0 0 67 2 49Ž . Ž . Ž . Ž . Ž . Ž . Ž .1.36 17.8 0 0 45.89 1.36 33.56
a Values in parentheses are percentage positivity rate.
Ž .P-0.05 . It was interesting to note that viralagents other than HAV]HEV were more fre-quently responsible for fulminant hepatitis among
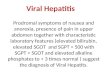
Ž .non-pregnant females P-0.001 , while HEV wasthe most common agent resulting in fulminant
Ž . Ž .hepatitis during pregnancy P-0.01 Fig. 1 .Ž .HEV infected pregnant females 50 and 51%
during the second and third trimester, respec-tively, developed fulminant hepatitis, in compar-ison to 16.66% of females developing FHF during
Ž .the first trimester P)0.05 , This shows an in-creased incidence of fulminant hepatitis with in-creasing gestation period among HEV infectedpregnant females. However, it cannot be con-cluded that HEV infection leads to fulminanthepatitis with advancing pregnancy, since the datadoes not establish the cause and effect relation-
ship. Mortality rates following acute and fulmi-nant hepatitis caused by different hepatotrophicviruses at varied gestation periods are depicted inTable 2. Mortality remained low among AVHcases, and mortality increased with the progres-sion of gestation periods, especially for HEV.
4. Discussion
Divergent opinions exist over the maternal andfetal outcome of the pregnancies associated with
w xviral hepatitis 1]17 . Subsequently, based on thedata from the developed world, it was concludedthat the course of viral hepatitis is not altered bythe pregnancy, per se, and the case fatality rateremains the same for pregnant and non-pregnant
w xwomen 5]7 . Poor nutritional status was sus-

( )S.P.B. Jaiswal et al. r International Journal of Gynecology and Obstetrics 72 2001 103]108106
Fig. 1. Incidence of hepatitis viruses among pregnant and non-pregnant fulminant females.
pected to be the major factor in the outcome ofpregnancies with viral hepatitis in developing
w xcountries 11,12 . However, in the present study,none of the pregnant females were malnourished.
Hepatitis E was the most common form ofhepatitis, both in non-pregnant and pregnantwomen in the present series. The course of acutehepatitis E was similar in both groups, but thepresentation as fulminant hepatitis was morecommon during pregnancy, and this observation
supports the view that pregnancy state increasesthe severity of HEV infection and not the suscep-
w xtibility to the virus. Khuroo et al. 2 supportedthe concept on the basis of the increased fre-quency of pregnant women contracting the ictericform of the disease in comparison to non-preg-nant women and men during the epidemic. Hehad also observed that fulminant hepatic failuredeveloped more often in pregnant women than innon-pregnant women. In his series, none of the
Table 2Mortality rate among pregnant females with AVH and FHF
Period No. of AVH pregnant females expired No. of FHF pregnant females expiredŽ . Ž .pregnancy Group A Group B
in trimester HBV HEV nA]nE Total HBV HEV nA]nE Total
I 0r7 0r10 0r3 0r20 0r0 1r2 0r0 1r2II 0r8 0r12 1r13 1r33 0r1 4r12 1r2 5r15III 0r7 1r18 1r5 2r30 2r2 10r19 3r5 15r27All periods 0r22 1r40 2r21 3r83 2r3 15r33 4r7 21r43

( )S.P.B. Jaiswal et al. r International Journal of Gynecology and Obstetrics 72 2001 103]108 107
non-pregnant females developed FHF, while twoof the 12 FHF cases associated with HEV weredocumented among the non-pregnant group inthe present study. The data by Khuroo and his
w xgroup 12 are based on the study wherein thewater-borne hepatitis was labeled as non-A]non-B, and the precise identification as HEV was notpossible at that time. Observations by other In-dian workers have been similar to those of Khuroow x1]4 . Furthermore, the mortality among preg-nant cases that presented with FHF progressivelyincreased with the gestation period, and appearedto be at a maximum during the third trimester.Once again, these observations are similar to
w xthose reported by other groups 2,14 and theprecise identification of HEV infection remainsthe salient feature of the present study. A similarobservation of pregnancy state predisposition todevelop the severe liver disease was also found
w xduring the sporadic episode of hepatitis 10 .However, it was noted that during sporadicepisodes, the development of fulminant hepatitiswas not specifically related to any particular hep-
w xatotrophic virus. Furthermore, Acharya et al. 10also concluded that HEV seems to behave in aclinical manner similar to other hepatotrophicviruses, and has a less severe course than thatobserved during epidemics. The higher HEV inci-dence rate and severe course of disease, particu-larly during second and third trimester of preg-nancy in the present series, could be due to asmall suspected outbreak of HEV during the
Ž .period unpublished data .An increased severity of infection during preg-
nancy was not seen for hepatitis A and B in thew xstudy by Khuroo et al. 12 , while the outcome of
pregnancy was reported to be bad for HBV byw xNayak et al. 3 . In the present study, the inci-
dence of acute HBV was similar for both preg-nant and non-pregnant women, and the incidenceof FHF was somehow greater among non-preg-nant females.
Data appear to be scanty for the follow-up ofpregnancies associated with infections by A]Ehepatotrophic viruses. The prevalence of viralagents A]E in pregnant and non-pregnantfemales was similar for AVH in the present study.An important observation that was noted was the
higher incidence of viral hepatitis caused by agentsother than HAV]HEV. An etiological agent,other than HAV]HEV, was responsible for AVHamong 22% of the pregnant and 33.5% of thenon-pregnant subjects. Furthermore, there was astriking observation that an etiological agent otherthan A]E was associated with FHF among 58.8%of the non-pregnant females, in contrast to only16.6% among pregnant females.
The incidence of HAV was low for both preg-nant and non-pregnant females, and matched theHAV incidence in the general adult population in
w xIndia 19 . Similarly, none of the pregnantfemales had were positive for HCV, and amongthe non-pregnant females, HCV incidence wasvery low in the present series. Infection withHDV was seen only in one case in the pregnantgroup, and the overall incidence of HDV in the
w xregional population was also low 20 . Co-infec-tion of HAV and HEV was seen in occasionalcases in both groups.
To conclude, HEV was the most common hep-atotrophic virus associated with severe hepatitisin the form of FHF among pregnant females, andwas associated with the highest mortality duringthe third trimester of pregnancy. The incidence ofnon-A]non-E and hepatitis B was next in orderamong both pregnant and non-pregnant women,and was the most common cause of fulminanthepatitis among non-pregnant females. The inci-dence of HAV, HCV and HDV was low in bothpregnant and non-pregnant women.
Acknowledgments
The financial support from the Council ofŽ .Scientific and Industrial Research CSIR , New
Delhi, to the first author is acknowledged. Theauthors are grateful to Dr Ravikant Saxena, Med-ical Director, and management of ChoithramHospital and Research Center, for providing thenecessary facilities.
References
w x1 Ramalingaswami V, Purcell RH. Waterborne non-a,non-b hepatitis. Lancet 1988;1:571]573.

( )S.P.B. Jaiswal et al. r International Journal of Gynecology and Obstetrics 72 2001 103]108108
w x2 Khuroo MS, Teli MR, Skidmou S, Sofi MA, Khuroo MI.Incidence and severity of viral hepatitis in pregnancy.Am J Med 1981;70:252]255.
w x3 Nayak NC, Panda SK, Datta R, Zuckerman AJ, GuhaDK, Madangopalan N, Buckshee K. Aetiology and out-come of acute viral hepatitis in pregnancy. J Gastroen-terol Hepatol 1989;4:345]352.
w x4 Acharya SK, Dasrathy S, Kumer TL, Sushma S, PrasannaKSU, Tandon A et al. Fulminant hepatitis in a tropicalpopulation: clinical course, cause, and early predictorsof outcome. Hepatology 1996;23:1448]1455.
w x5 Medhat A, el-Sharkawy MM, Shaaban MM, MakhloufMM, Ghaneima SE. Acute viral hepatitis in pregnancy.Int J Gynecol Obstet 1993;40:25]31.
w x6 Yoshiba M, Dehra K, Inoue K, Okamoto H, Mayumi M.Contribution of hepatitis C virus to non-A, non-B fulmi-nant hepatitis in Japan. Hepatology 1994;19:829]835.
w x7 Dinsmoor MJ. Hepatitis in the obstetric patients. InfectDis Clin North America. 1997;11:77]91.
w x8 Shrestha SM, Kane MA. Preliminary report of an out-break of non-A, non-B viral hepatitis in Kathmandu
Ž .valley. I Inst Med Nepal 1983;5:1]10.w x9 Tripathi BM, Misra NP. Viral hepatitis with pregnancy.
J Assoc Physicians India 1981;29:463]469.w x10 Acharya SK, Dasrathy S, Panda SK. A prospective eval-
uation of outcome of fulminant hepatitis in pregnancyrelated to hepatitis E virus. In: BN Tandon, SK Acharya,editors. Hepatitis E virus: epidemiology to candidatevaccine. Trop gastroenterol, New Delhi, India, 1996:102]118.
w x11 Krawczyuski K. Hepatitis E. Hepatology 1993;17:932]941.
w x12 Khuroo MS, Deurmeyer W, Zargar SA, Ahanger MA,Shah MA. Acute sporadic non-A, non-B hepatitis inIndia. Am J Epidemiol 1983;118:360]364.
w x13 Khuroo MS. Hepatitis E: The enterically transmittednon-A, non-B hepatitis. Indian J Gastroenterol1991;10:96]100.
w x14 Mirghani OA, Saeed OK, Basama FM. Viral hepatitis inpregnancy. East Afr Med J 1992;69:445]449.
w x15 DeSilva HJ, Jayawardena J, Pethiyagoda AU, SirisenaJL. Viral hepatitis complicating pregnancy } a 5-yearhospital based retrospective study. Ceylon Med J1993;38:15]17.
w x16 Myint H, Soe MM, Khin T, Myint TM, Tin KM. Aclinical and epidemiological study of an epidemic ofnon-A, non-B hepatitis in Rangoon. Am J Trop MedHyg 1985;34:1183]1189.
w x17 Nousaria B, Ainati A, Bernau J, Rueff B, Benhamou JP,Gaudebout C et al. Fulminant viral hepatitis and preg-nancy in Algeria and France. Ann Trop Med Parasitol1986;80:623]629.
w x18 Bernau J, Rueff B, Benhamou JP. Fulminant and sub-fulminant hepatic failure: definitions and causes. SeminLiv Dis 1986;6:97]101.
w x19 Jaiswal SPB, Chitnis DS, Jain A, Inamdar S, Jain K, JainSC, Naik G. Etiologic spectrum among acute viral hep-atitis cases in central India. Indian J Gastroenterol1998;17:113.
w x20 Jaiswal SPB, Chitnis DS, Jain A, Naik G, Artwani KK.Prevalence of anti-delta antibodies in central India andcomparison of data from other parts of India. TropGastroenterol, 1999;20:29]32.