Embed Size (px)
Citation preview

Editorial
Vitamin D and autoimmune rheumatic diseases
Introduction
Vitamin D is classified as a secosteroid in which one of the ringshas been broken, in this case by ultraviolet B sunlight, and themain source of vitamin D is de novo synthesis in the skin.Although vitamin D is consumed in food, dietary intake alone isoften insufficient, supplying only 20% of the body’s requirements.
In recent years, the discovery of the vitamin D receptor (VDR)in the cells of the immune system and the fact that several ofthese cells produce the vitamin D hormone suggested that it couldhave immunoregulatory properties.
However, vitamin D insufficiency is emerging as a clinicalproblem of global proportions and epidemiology has linkedvitamin D status with autoimmune disease susceptibility andseverity [1].
Therefore, 1,25-dihydroxyvitamin D3 [1,25(OH)2D3] thebiologically active metabolite of Vitamin D3, not only regulatesbone and calcium metabolism but also exerts immunomodulationvia the nuclear VDR expressed in antigen-presenting cells andactivated T/B cells [2]. In particular, this regulation is mediatedthrough interference with nuclear transcription factors such asNF-AT and NF-�B or by direct interaction with vitamin Dresponsive elements in the promoter regions of cytokine genes.
The mechanisms of vitamin D immunomodulation
Dendritic cells (DCs) are primary targets for the immunomodu-latory activity of 1,25(OH)2D3, as indicated by inhibited DCdifferentiation and maturation, leading to down-regulated expres-sion of MHC-II, costimulatory molecules (CD40, CD80 andCD86) and decreased production of IL-12. Moreover,1,25(OH)2D3 enhances IL-10 production and promotes DCapoptosis. Together, these effects of 1,25(OH)2D3 inhibitDC-dependent T-cell activation [2] (Fig. 1).
In particular, the active synthesis of 1,25(OH)2D3 seems toexert an autoregulatory function by inhibiting the differentiationof monocyte precursors into immature DCs and the subsequentability of the immature DCs to undergo terminal differentiationin response to maturation stimuli [3] (Fig. 1).
Tolerogenic DCs induced by a brief treatment with1,25(OH)2D3 or its analogues can induce CD4þCD25þ Tregulatory (Treg) cells that are able to mediate transplantationtolerance and arrest the development of autoimmunity(i.e. autoimmune diabetes) [4].
Tolerogenic DCs may not always be necessarily involved inthe generation of Treg cells by VDR agonists, however, anda combination of 1,25(OH)2D3 and dexamethasone has beenshown to induce naı̈ve CD4þ T cells (Th0) to differentiate in vitrointo IL-10-producing Treg cells, even in the absence of antigen-presenting cells [4] (Fig. 1).
VDR agonists not only favour induction of CD4þCD25þ Treg
cells and enhance their suppressive activity, but can alsopromote their recruitment at inflammatory sites. Furthermore,1,25(OH)2D3 treatments induced natural killer (NK) T-cellfunctions in vitro and in vivo [5] (Fig. 1).
NKT cells are early innate regulatory cells that can alter theoutcome of autoimmunity. Therefore, two types of cells areinduced by 1,25(OH)2D3, the Treg and the NKT cells; induction ofthese regulatory cells and direct inhibition of Th1 cells are the
mechanisms by which 1,25(OH)2D3 suppresses experimentalautoimmunity [5].
In addition, treatment with VDR agonists inhibits the T-cellproduction of IL-17, a pro-inflammatory cytokine that isproduced by pathogenic T cells (Th17) in various models oforgan-specific autoimmunity in the brain, heart, synovium andintestines [6] (Fig. 1).
Interestingly, IL-17 production is sustained by IL-23, an IL-12family member consisting of p19 and p40 chains, the latter ofwhich is strongly inhibited by VDR agonists [6].
Recently, 1,25(OH)2D3 treatment induced a significant inhibi-tion of normal lymphoid cell progenitors growth of both T and Blineage and inhibited significantly also the growth of malignant B-cell lineage lymphoid progenitors, without inducing cytotoxiceffect [7].
More recently, by testing the effects of 1,25(OH)2D3 on B-cellresponses, it was found that it inhibited the ongoing proliferationof activated B cells and induced their apoptosis, whereas initialcell division was unimpeded [8] (Fig. 1).
The generation of plasma cells and post-switch memoryB cells was significantly inhibited by 1,25(OH)2D3 although theup-regulation of genetic programmes involved in B-cell dif-ferentiation was only modestly affected. B cells expressedmRNAs for proteins involved in vitamin D activity, including1�-hydroxylase, 24-hydroxylase and the VDR, each of which wasregulated by 1,25(OH)2D3 and/or activation. Interestingly,1,25(OH)2D3 up-regulated the expression of p27, but not of p18and p21, which may be important in regulating the proliferation ofactivated B cells and their subsequent differentiation in plasmacells [8].
Vitamin D and autoimmune rheumatic diseases
The net effect of the vitamin D endocrine system on the immuneresponse is an enhancement of innate immunity coupled withmultifaceted regulation of adaptive immunity [9].
Epidemiological evidence indicates a significant associationbetween vitamin D deficiency and an increased incidence ofautoimmune diseases, and clarification of the physiological role ofendogenous VDR agonists in the regulation of autoimmuneresponses will support the pharmacological VDR agonists for usein the clinic. The anti-proliferative, pro-differentiative, immuno-modulatory and anti-inflammatory properties of synthetic VDRagonists could be exploited to treat a variety of autoimmunerheumatic diseases, from RA to SLE, and possibly also multiplesclerosis, type 1 diabetes or IBDs [9].
Low serum levels of vitamin D3 might be partially related,among other factors, to prolonged daily darkness (reducedactivation of the pre-vitamin D by the ultraviolet B sunlight),different genetic background (i.e. vitamin D receptor polymorp-hism) and nutritional factors, and explain to the latitute-relatedprevalence of autoimmune diseases such as RA, by consideringthe potential immunosuppressive roles of vitamin D [10].Treatment of vitamin D deficiency could be particularly impor-tant in SLE patients due to concomitant insults on their tissuessuch as bone, and in view of the discovered immunomodulatoryeffects exerted by vitamin D [11].
Rheumatology 2009;48:210–212 doi:10.1093/rheumatology/ken394Advance Access publication 17 October 2008
210� The Author 2008. Published by Oxford University Press on behalf of the British Society for Rheumatology. All rights reserved. For Permissions, please email: [email protected]
at UC
SF Library and C
enter for Know
ledge Managem
ent on Decem
ber 8, 2014http://rheum
atology.oxfordjournals.org/D
ownloaded from

RA
Regarding RA, a recent study evaluated the association of dietaryand supplemental vitamin D intake with RA incidence [12].Through 11 yrs of follow-up, 152 cases of RA were validatedagainst medical records. Greater intake (highest versus lowesttertile) of vitamin D was inversely associated with risk of RA(P for trend¼ 0.05). Inverse associations were apparent for bothdietary (P for trend¼ 0.16) and supplemental (P for trend¼ 0.03)vitamin D. No individual food item, high in vitamin D contentand/or calcium was strongly associated with RA risk, but acomposite measure of milk products was suggestive of an inverseassociation with risk of RA (P for trend¼ 0.06). In conclusion,greater intake of vitamin D may be associated with a lower riskof RA in older women, although this finding is hypothesis-generating [12].
An older study in 19 RA patients evaluated the effects oforal �-calcidiol 2�g/day added to regular drug regimen [13].
After 3 months, high-dose oral �-calcidiol therapy showeda positive effect on disease activity in 89% of the patients (45% ornine patients with complete remission and 44% or eight patientswith a satisfactory effect). Only two patients (11%) showed noimprovement, but no new symptoms occurred. No side-effectswere observed. These results suggest that �-calcidiol is a powerfulimmunomodulatory agent with fairly low hypercalcaemic activity.Clinical improvement was strongly correlated with the immu-nomodulating potential of this agent; in fact, dual effects onlymphocyte proliferation and apoptosis according to the prior cellactivation state were observed. �-Calcidiol could thereforepossibly be used as an adjunct therapy with DMARDs in patientswith active RA [13].
Therefore, greater intake of vitamin D has been associated witha lower risk of RA but low serum vitamin D together with higher
prevalence of RA seem common among North European peoplewhen compared with Southern Europe. A recent study evaluatedserum 25(OH)D levels in female RA patients from North(Estonia) and South (Italy) Europe and to correlate them withthe disease activity score (DAS28) during winter and summer [14].
The 25(OH)D levels were found significantly higher in south vsnorth (P¼ 0.0116) both in winter and in summer time. Differenceswere observed also in controls. The variations (increase) of25(OH)D levels between winter and summer were found to besignificant (P¼ 0.0005) in both south and north. Differenceswere also observed in controls. No significant differences werefound concerning 25(OH)D levels between RA patients and theircontrols in either country. Interestingly, a significant negativecorrelation between 25(OH)D and DAS28 was found in summeronly in south (r¼�0.57, P< 0.0001) and in winter in north(r¼�0.40, P< 0.05). In conclusion, significantly lower 25(OH)Dserum levels were observed in RA patients from north vs southEurope with a circannual rhythm in winter and summer time.In addition, 25(OH)D values showed a significant correlation(negative) with RA clinical status (DAS28) in both North andSouth European RA patients, suggesting possible effects ofvitamin D among other factors on disease activity [14].
More recently, it was investigated if serum vitamin D metab-olites may be inversely associated with current disease activity,severity and functional disability in patients with early RA [15].
At baseline, there was an inverse relationship between25(OH)D levels and the tender joint count, DAS28 score andHAQ score. The only inverse relationship with 1,25(OH)2D3 waswith the HAQ score. Each 10-ng/ml increase in the level of25(OH)D was associated with a decrease in the DAS28 score of0.3 and in the CRP level of �25%. At 1 yr, the only significantresult was an inverse association between baseline vitamin D
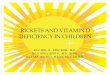
FIG. 1. Mechanisms involved in vitamin D modulation of the immune responses. DCs are primary targets for the immunomodulatory activity of 1,25(OH)2D3, as indicated byinhibited DC differentiation and maturation, together with inhibition of differentiation of monocyte precursors into immature DCs. 1,25(OH)2D3 suppresses Th1 (and Th17)-driven cytokine responses, induces Treg cells, induces IL-4 production (Th2) and enhances NKT-cell function. Differentiation and maturation of B cells is also inhibited. Thare CD4þ helper cell subsets (Th1, Th2, Th3-Treg, Th17) originating from naı̈ve T cell (Th0). Thin arrows (left) indicate cytokines that induce differentiation of Th0 cells andthicker arrows (right) indicate cytokines produced by activated Th cell subsets. All T cells that have been tested express the VDR. B cells and NKT cells are also reported.The yellow circles indicate the cytokines/activities inhibited by vitamin D. On the contrary, the green circles indicate the cytokines enhanced by vitamin D.
Editorial 211
at UC
SF Library and C
enter for Know
ledge Managem
ent on Decem
ber 8, 2014http://rheum
atology.oxfordjournals.org/D
ownloaded from

metabolite levels and the HAQ score; that is, those with highermetabolite levels had lower HAQ scores. These data providefurther support that vitamin D plays an immunomodulatoryrole in inflammatory arthritis and, if confirmed, the vitamin Dsupplementation should be also examined in early RA [15].
SLE
A number of recent studies have highlighted the associationbetween SLE and vitamin D deficiency. Vitamin D deficiencyskews the immunological response towards loss of tolerance.Adding vitamin D in vitro reverses immunological abnormalitiescharacteristic of SLE.
Serum 25(OH)D levels between recently diagnosed SLE casesand matched controls, as well as disease characteristics inrelationship to 25(OH)D among cases, were recently studied [16].
Data from a population-based cohort of 123 recently diagnosedSLE patients and 240 controls were used. A trend towards lower25(OH)D levels in SLE cases compared with controls, whichwas statistically significant in Caucasians (P¼ 0.04), controllingfor age, sex, season and smoking was detected. Overall, 67% ofthe subjects were vitamin D deficient, with mean levels signifi-cantly lower among African Americans (15.9 ng/ml) comparedwith Caucasians (31.3 ng/ml). Critically low vitamin D levels(<10 ng/ml) were found in 22 of the SLE cases, with the presenceof renal disease being the strongest predictor [odds ratio (OR)13.3, P< 0.01] followed by photosensitivity (OR 12.9, P< 0.01).These results further suggest vitamin D deficiency as a possiblerisk factor for SLE and provide guidance for future investigationslooking at a potential role of vitamin D in the prevention and/ortreatment of SLE [16].
Recently, serum levels of 25(OH)D were measured in 37 femaleSLE patients and correlated with clinical and immunologicalmeasures [17].
Approximately 65% of the SLE patients had values <80 nmol,which is accepted as the lower limit of vitamin D adequacy.In addition, 20% of the patients had levels of 25(OH)D that werelower than the normal range for the assay (<47.7 nmol/l). Thegroup of SLE patients with these lowest levels showed diseaseactivity measures, including global assessment scores, that werehigher than in those with levels considered normal in the assay(P� 0.003). However, in this study, levels of autoantibodiesincluding dsDNA were higher in the group with levels of vitaminD that were >47.7 nmol/l (P¼ 0.0069) [17].
The increased disease symptoms present in SLE patients withvery low levels of vitamin D suggest a role for supplementationwith exogenous vitamin D to optimize therapeutic outcomes.However, the possibility that such treatment could lead toincreased autoantibody levels requires further study.
In a further study in 92 SLE patients (90% women, 98% white)69 (75%) and 14 (15%) patients presented with vitamin Dinsufficiency and deficiency, respectively [18].
Female sex (P¼ 0.001), treatment with HCQ (P¼ 0.014) andtreatment with calcium and vitamin D (P¼ 0.049) predictedhigher levels of 25(OH)D. Photosensitivity (OR 3.5) and photo-protection (OR 5.7) predicted vitamin D insufficiency anddeficiency, respectively. Higher age (OR 0.95) and HCQ use(OR 0.29) protected against vitamin D deficiency. Patients withvitamin D deficiency had a higher degree of fatigue as quantifiedby a 0–10 VAS (mean 5.32 vs 4.03, P¼ 0.08). No relation wasseen between vitamin D insufficiency or deficiency and diseaseduration. This recent study further showed that vitamin Dinsufficiency and deficiency are common in patients with SLEand are associated with sun avoidance. Vitamin D deficiency wasrelated to a higher degree of fatigue, but vitamin D levels had nosignificant relation with SLE severity [18].
Conclusions
The vitamin D endocrine system is recognized as an importantimmune modulatory factor involved in autoimmune rheumaticdiseases.
VDR agonists seem primarily to inhibit DC differentiation,pathogenic pro-inflammatory T cells such as Th1 and Th17 cellsand, under appropriate conditions, they seem to favour adeviation to the Th2 pathway.
These immunomodulatory and anti-inflammatory activitiesmight be particularly efficient in RA patients and support atherapeutic role of 1,25(OH)2D3 in such a disease.
In addition, vitamin D may play an important role in themaintenance of B-cell homeostasis, and the correction of vitaminD deficiency may be useful in the treatment of B cell-mediatedautoimmune rheumatic disorders such as SLE.
Disclosure statement: The author has declared no conflicts ofinterest.
M. CUTOLO1
1Research Laboratories and Clinical Academic Unit ofRheumatology, University of Genova, Genova, ItalyAccepted 9 September 2008
Correspondence to: M. Cutolo, Research Laboratories andClinical Academic Unit of Rheumatology, University of Genova,Viale Benedetto XV, 6, 16132 Genova, Italy.E-mail: [email protected]
References
1 Adams JS, Hewison M. Unexpected actions of vitamin D: new perspectives on theregulation of innate and adaptive immunity. Nat Clin Pract Endocrinol Metab.2008;4:80–90.
2 van Etten E, Mathieu C. Immunoregulation by 1,25-dihydroxyvitamin D3: basicconcepts. J Steroid Biochem Mol Biol 2005;97:93–101.
3 Sigmundsdottir H, Pan J, Debes GF et al. DCs metabolize sunlight-induced vitaminD3 to ‘program’ T cell attraction to the epidermal chemokine CCL27. Nat Immunol2007;8:285–93.
4 Gregori S, Giarratana N, Smiroldo S, Uskokovic M, Adorini L. A 1,25-dihydroxyvitamin D3 analog enhances regulatory T cells and arrests autoimmunediabetes in NOD mice. Diabetes 2002;51:1367–74.
5 Yu S, Cantorna MT. The vitamin D receptor is required for iNKT cell development.Proc Natl Acad Sci USA 2008;105:5207–12.
6 Steinman L. A brief history of TH17, the first major revision in the TH1/TH2hypothesis of T cell-mediated tissue damage. Nat Med 2007;13:139–45.
7 Consolini R, Pala S, Legitimo A, Crimaldi G, Ferrari S, Ferrari S. Effects of vitamin Don the growth of normal and malignant B-cell progenitors. Clin Exp Immunol2001;126:214–9.
8 Chen S, Sims GP, Chen XX, Gu YY, Chen S, Lipsky PE. Modulatory effects of1,25-dihydroxyvitamin D3 on human B cell differentiation. J Immunol.2007;179:1634–47.
9 Adorini A, Penna G. Control of autoimmune diseases by the vitamin D endocrinesystem. Nat Clin Pract Rheumatol 2008;4:404–12.
10 Cutolo M, Otsa K, Uprus M, Paolino S, Seriolo B. Vitamin D in rheumatoid arthritis.Autoimmun Rev 2007;7:59–64.
11 Cutolo M, Otsa K. Review: vitamin D, immunity and lupus. Lupus 2008;17:6–10.12 Merlino LA, Curtis J, Mikuls TR, Cerhan JR, Criswell LA, Saag KG. Iowa Women’s
Health Study. Arthritis Rheum 2004;50:72–7.13 Andjelkovic Z, Vojinovic J, Pejnovic N et al. Disease modifying and immunomodu-
latory effects of high dose 1 alpha (OH) D3 in rheumatoid arthritis patients. Clin ExpRheumatol 1999;17:453–6.
14 Cutolo M, Otsa K, Laas K et al. Circannual vitamin D serum levels and diseaseactivity in rheumatoid arthritis: Northern versus Southern Europe. Clin ExpRheumatol 2006;24:702–4.
15 Patel S, Farragher T, Berry J, Bunn D, Silman A, Symmons D. Association betweenserum vitamin D metabolite levels and disease activity in patients with earlyinflammatory polyarthritis. Arthritis Rheum 2007;56:2143–9.
16 Kamen DL, Cooper GS, Bouali H, Shaftman SR, Hollis BW, Gilkeson GS. Vitamin Ddeficiency in systemic lupus erythematosus. Autoimmun Rev 2006;5:114–7.
17 Thudi A, Yin S, Wandstrat AE, Li QZ, Olsen NJ. Vitamin D levels and diseasestatus in Texas patients with systemic lupus erythematosus. Am J Med Sci2008;335:99–104.
18 Ruiz-Irastorza G, Egurbide MV, Olivares N, Martinez-Berriotxoa A, Aguirre C.Vitamin D deficiency in systemic lupus erythematosus: prevalence, predictors andclinical consequences. Rheumatology 2008;47:920–3.
212 Editorial
at UC
SF Library and C
enter for Know
ledge Managem
ent on Decem
ber 8, 2014http://rheum
atology.oxfordjournals.org/D
ownloaded from