Embed Size (px)
Citation preview

SURVEY OF OPHTHALMOLOGY VOLUME 25 l NUMBER 2-SEPTEMBER-OCTOBER 1980
REVIEW
Vitreous Base Classification of Retinal
Tears: Clinical Application
JESSE SIGPLMAN, M.D.
Peripheral Retinal Disease Unit, New York Hospital-Cornell University Medical Center, Manhattan Eye. Ear and Throat Hospital, New York, New York
Abstract. The abundant data about retinal tears has shown that they are prevalent in the general- population and that the vast majority of retinal tears do not lead to retinal detachment. What remains to be clarified are the criteria for identifying the few retinal breaks which require prophylactic surgery to prevent their progression to retinal detachment. Numerous reports have identified clinical features which correlate with the risk of retinal detachment. These correlative data offer at best only a sugges- tion about the need for treatment of any specific retinal break. This paper demonstrates how the categorization of a retinal tear on the basis of vitreoretinal anatomic detail may be used clinically to make an objective and nonstatistical judg- ment about the prognosis of any specific retinal break. The application of this new categorization offers an advance in the care of patients with retinal tears. (Suw Ophthalmol 25:59-74, 1980)
Key words l aphakia l cryogenic surgery l lattice degeneration l
retina, break, detachment, pigment, tear l scleral buckle l vitreous base l
vitreous traction
T he treatment of retinal tears has en- tered a new era. A half century ago when Gonin wrote, “for every (retinal)
tear there is a detachment:“’ he proposed the earliest modern principle of retinal surgery: the need to treat every retinal tear. Now this teaching has been greatly revised.‘4*‘8 The dis- covery of a vastly higher prevalence of retinal tears than of retinal detachments has shown that most retinal tears do not lead to retinal detachment and do not require surgical treat- ment.
The area on which current attention has
been focused has been the criteria for iden- tifying those few retinal tears which have a high risk of causing detachment. What has emerged from these investigations is a vast collection of clinical data whose complexity and subtlety make it difficult to establish practical clinical criteria for the treatment of retinal tears. The first purpose of this review is to demonstrate which of the existing criteria are clinically significant and applicable. The second purpose is to emphasize new criteria which have not yet been applied to clinical judgment.
59

60 Surv Ophthalmol 25 (2) September-October 1980 SIGHMAN
I. Definition of Terms
Full thickness breaks of the retina have been labeled “holes” or “tears.” The distinc- tion between these has been based on the differences on their etiologies as suggested by their clinical appearance and history and anatomic findings in cadaver eyes.2g**2 Holes result from trophic changes in the retina, while tears result from vitreoretinal or zonuloretinal adhesions and traction.
This paper concerns itself primarily with tears because they are almost the exclusive cause of retinal detachment. However, in much of the literature cited in this review, the authors have referred to “breaks,” rather than to “holes” or “tears.” Thus, although it is my impression that most of these breaks were, in fact, tears, I have retained the more general term “breaks” in referring to specific data from reports which used that term.
The term, “retinal detachment,” must be subdivided for purposes of this discussion into “clinical detachment” and “subclinical detachment.“B8 Clinical detachment includes all retinal detachments which cause loss of peripheral visual field by the extension of the detachment into the percipient retina which includes all the retina posterior to the equator. Extension of the detachment into the macula causes loss of acuity. All clinical rhegmatogenous detachments warrant con- sideration of an attempt at surgical repair in order to improve visual function.
Subclinical detachment is used in this paper to describe the localized shallow retinal detachments which surround many retinal tears. These detachments may never extend to cause any visual loss. A subclinical detach- ment is asymptomatic because it involves the pre-equatorial retina which is nonpercipient. Photopsia and floaters which may accom- pany a subclinical detachment result from the tear rather than from the detachment. A sub- clinical detachment does not warrant surgery unless it threatens to progress to a clinical detachment.
II. Need for Improved Therapeutic Criteria
A. PREVALENCE OF TEARS VS. INCIDENCE OF CLINICAL DETACHMENTS
The importance of judging which retinal tears should undergo surgery and which can be left safely untreated is emphasized by com- paring the low incidence of clinical detach-
ment with the high prevalence of retinal tears accompanied by either no detachment or by subclinical detachment. The incidence of clinical detachment has been estimated from clinical study in small stable population groups.
In the Israeli national collaborative study, the incidence of clinical retinal detachment was 9 per 100,000 per year.6B In Canton Zurich in Switzerland, this incidence was 24.4 per 100,000 per year.8 No matter which of these figures is correct, it is clear that the in- cidence of clinical detachment is small. If the prevalence of retinal tears lies between 4% and 18% 2~6~50~37~s@~64~73 in the general adult pop- ulation, each tear carries a chance of less than l/70 leading to clinical detachment.11*14*6e In- cidence and prevalence rates may be com- pared by multiplying the incidence rate by the number of years of adult life (approximately 65).
B. RISKS OF SURGERY
In order for treatment of all clinically discovered retinal tears to be justified, the rate of complications from the treatment should be lower than the chance of a tear’s leading to clinical detachment. Evidence in- dicates that the rate of visual complication from prophylactic surgery of tears may ex- ceed the rate of complication of leaving these tears untreated. Development of new tears following treatment has had an incidence as high as 8.3%.62 Progression from subclinical to clinical detachment following treatment of a tear has been reported at 4.8%” while macular pucker has had an incidence as high as 2.2%.44*a2 Keratopathy presents the lowest rate of occurrence of the major complica- tions.” The incidence of these complications is variable. The exact clinical situation, the mode of therapy, the skill of the surgeon, and the details of treatment all have major bear- ing on the complication rate. Sufficient evi- dence exists to suggest that, on the average, there may be a higher rate of complications from treatment than from nontreatment of a random retinal tear. An additional argument against treating all tears comes from the Is- raeli national cooperative61*67*6S study which demonstrated that the prophylactic treatment of subclinical retinal tears did not lower the incidence of retinal detachment. In this study’s controlled population, treatment was given to all retinal breaks found either because of

VITREOUS BASE CLASSIFICATION OF RETINAL TEARS 61
symptoms or in routine screening. This find- ing confirms that a subclinical retinal tear has little risk of being the cause of a clinical retinal detachment.
C. SOCIOECONOMIC CONSIDERATIONS
The other consideration in treating all retinal tears is the enormous number of patients who would require surgery. With the prevalence of retinal tears at approximately 5’S, approximately 18,840,OOO of the current 2 16,800,000 American population’a now have retinal tears and would require surgery. This year only approximately 2 1,680 Americans will develop a new (nonrecurrent) clinical retinal detachment. (This number is calculated from a rate of retinal detachment of 1/10,000 per year). Treatment of all retinal tears would pose an enormous burden to the American ophthalmic system with question- able benefit to the population.
III. Current Therapeutic Criteria
A. LACK OF SPECIFICITY
Once the risk of retinal detachment from a tear was recognized, many correlations were drawn between parameters related to the tear and the risk of retinal detachment. The clinical use of these data has been limited by the inherent difficulties of applying statistical correlates to specific cases. Each tear has a unique set of features which make it fit im- perfectly the data concerning a specific tear. These data, nevertheless, provide some useful information. The problem is to separate the useful from the misleading information.
B. SYMPTOMS
The most significant of the clinical conditions which correlate with the risk of retinal detachment is the history of symptoms due to the occurrence of the tear. A symp- tomatic retinal tear has been shown to have a 30% chance of leading to clinical retinal detachment within six weeks.20 The reason for the significance of symptoms is that the symptoms result from vitreous traction which is capable of causing progression of the tear to a clinical detachment. Photopsia results from retinal distortion caused by vitreous traction. The hemorrhage which produces floaters occurs when vitreous traction tears a previously normal section of retina with pa-
tent vasculature. Although a symptomatic tear has a 30% chance of leading rapidly to clinical detachment, it has a 70% chance of remaining localized. This indicates that ad- ditional factors about the tear determine whether or not the tractional force causes the progression to clinical detachment. Of patients with photopsia, only 23% have been found to have any ophthalmoscopic evidence of vitreoretinal disease and only 16% were found to have any retinal tears.66 Nor is a history of symptoms necessary for the development of a tear or the extension of a tear to a detachment. Of patients who develop clinical retinal detachment, only 50% have a history of symptoms .68 Using the history of symptoms as the only criterion for treating a retinal tear will result in a high rate of both overtreatment and undertreatment of tears.
C. MYOPIA
The presence of myopia has been considered a strong indication for the treat- ment of retinal tears because of the high rate of retinal detachment in myopic eyes (ap- proximately 10 times the rate in the general population).1e*42 The use of the degree of myopia as an indication for the treatment of a retinal tear is complicated by the higher prevalence of subclinical retinal tears in myopic than in emmetropic globes.11J4J6~4a This suggests that a subclinical retinal tear in a myopic eye may have no greater chance of leading to clinical detachment than would a retinal tear in an emmetropic eye. The low risk of progression to clinical detachment of a retinal break in a myopic eye is borne out by two studies from Israe1.43~57~58 Out of 25 round holes and six horseshoe tears in 19 myopic, aphakic eyes, none progressed to clinical detachment.4s In a separate group of 75 myopic eyes with retinal breaks only one developed a clinical detachment during a two- year history of observation.67 The only break which progressed to a clinical detachment was a go-degree flap tear. It has been es- timated that there are 35 myopic eyes with subclinical retinal breaks for every myopic eye which develops a retinal detachment.‘s The only data about myopic eyes which strongly suggests the value of prophylactic treatment is the 40% chance of retinal detach- ment following cataract surgery in male patients with myopia greater than 10 diopters.6S

62 SW Ophthclmol 25 (2) September-October 1980 SIGELMAN
D. VITREORETINAL SYNDROMES
The syndromes of generalized vitreoretinal degeneration76 include Marfan’s syndrome,“*76 Ehlers-Danlos syndrome,61 Wagner’s vitreo- retinal degeneration,38 and x-linked juvenile retinoschisis.46*71
Similarly to myopic eyes, eyes with generalized vitreoretinal degeneration have a higher than normal rate of retinal detach- ment. The rarity of these syndromes has precluded detailed analysis of the fate of asymptomatic retinal breaks in eyes with these syndromes. It remains to determine whether a retinal tear in an eye with one of these syndromes has a greater than average chance of leading to clinical detachment.
E. CATARACT SURGERY
Performing cataract surgery on an eye with a retinal tear has been demonstrated to in- crease the risk of retinal detachment from that tear. Of eight eyes to undergo cataract surgery in the presence of untreated retinal breaks, five developed retinal detachment during two years of followup.2’ This was a substantially higher rate of retinal detach- ment than the 9% overall rate of retinal detachment during the same period in phakic eyes with retinal breaks. Although these data do not control for myopia or contralateral retinal detachment, the risk of a retinal detachment appears to be made so much greater by cataract surgery that prophylactic treatment is warranted for all retinal breaks prior to cataract surgery.”
Although cataract surgery has been shown to greatly increase the risk from a retinal tear, it is uncIear whether the risk from a tear remains high after the immediate postopera- tive period. Asymptomatic breaks have been found in 9% of emmetropic and 18% of my- opic (greater than 6 diopters) aphakic eyes.33*43 In the myopic group, one-third of the breaks were horseshoe type tears. In one group of 14 aphakic eyes with retinal breaks, none de- veloped retinal detachment during two years of follow-up.” In another study of ten aphakic eyes each with a retinal break, four developed retinal detachment during followup.2o Al- though the increased risk found in the latter study may reflect a longer followup period, these data offer no clear clue of the effect of aphakia on the risk from a tear. That 50% of aphakic retinal detachments occur within six
months of cataract surgery4*66 is of little use for a clinical judgment of risk.
F. RETINOSCHISIS
Although a tear may occur in an eye with retinoschisis, the tear is almost always outside the area of the schisis cavity.3s There is no known association between retinoschisis and the risk of detachment from a tear outside the schisis cavity.
The retinoschisis cavity itself presents the problem of management of retinal breaks in the inner and/or the outer retinal layer. Breaks in the inner layer are atrophic holes. They are common but carry no significant as- sociation with retinal detachment.36 Breaks in the outer layer differ from inner layer holes because they are large, relatively rare, and are more like tears than holes because they may result from the contraction of a glial mem- brane on the inner aspect of the outer layer.12*36 This produces the characteristic rolling of the tear’s edge. In my experience, outer layer tears in the absence of inner layer breaks do not require prophylactic treatment. They carry a low risk of producing a retinal detach- ment which results from the disection of retinoschisis fluid into the subretinal space. These detachments remain localized for many years without progression beyond the mar- gins of the retinoschisis cavity. The presence of breaks in both layers has been shown to carry a significant risk of retinal detachment; in Dobbie’s series of eyes with untreated breaks in both layers, only one eye did not develop a detachment.24 The risk of detachment in the presence of inner layer holes can be greatly decreased by prophylactic treatment of outer layer tears.
G. POSTERIOR VITREOUS DETACHMENT
Posterior vitreous detachment has been implicated as a cause of retinal tears and of retinal detachmentTo Anatomic study of cadaver eyes has shown that complete posterior vitreous detachment is accompanied by a rate of retinal tears of 14%~~~ What is noteworthy about this study is that of the ap- proximately 300 eyes of patients over age 50 with posterior vitreous detachment, none showed a clinical retinal detachment. This in- dicates that posterior vitreous detachment is associated with three times the average rate of retinal tears but that it does not increase the likelihood that an already formed retinal

VITREOUS BASE CLASSIFICATION OF RETINAL TEARS 63
tear will progress to a clinical retinal detach- ment. The reason for this surprising lack of correlation between posterior vitreous detachment and the progression of a retinal tear to a clinical retinal detachment is that the behavior of a retinal tear is determined by traction at the vitreous base at the point of the tear and not by the detachment of the posterior vitreous at the optic disc. If posterior vitreous detachment is unaccom- panied by traction by the vitreous base at the point of the tear, there will be no increased risk of clinical retinal detachment from the posterior vitreous detachment. In the absence of other data, a posterior vitreous detachment is not a strong indication for prophylactic sur- gery of a tear.
H. LATTICE DEGENERATION
1. Lattice Lesion
The finding of lattice degeneration in approximately 30% of eyes with retinal detachment1s*68 has made lattice degeneration the retinal lesion with the highest association with retinal detachment.13*90 Does this association imply that the presence of lattice degeneration in an eye with a retinal tear in- creases the risk that the retinal tear will progress to a clinical retinal detachment? To answer this, separate consideration must be given to two groups of tears. One group con- sists of tears which occur at the margins of 2% of lattice lesions.lo~ls The danger presented by these tears is indicated by the finding that 30% of eyes with retinal detachment have lat- tice degeneration. The reason for this danger is the strong vitreoretinal adhesion which characterizes lattice degeneration. What remains to determine is whether a tear at the margin of lattice carries any greater risk than does a tear unassociated with lattice. The position of a tear at the margin of a lattice degeneration patch is a suggestive but not definitive indication for prophylactic surgery.
2. Pathology Separate from Lattice
The second group of tears whose prognosis is affected by lattice degeneration are those tears which occur in eyes with lattice but which are geographically removed from any detectable lattice lesion.18~so This group con- stitutes one-third of tears which occur in eyes with lattice.*’ Scanty data indicate a 33% risk of detachment from an isolated tear in an eye
with lattice. This suggests that the vitreoretinal adhesion characteristic of lattice is present in eyes with lattice even in regions of the retina where no obvious lattice degeneration is evident. This worsens the prognosis of any retinal tear in an eye with lattice degeneration so that the presence of lattice is an indication for prophylactic sur- gery of tears unassociated with the lattice.
3. Holes in Lattice
Tears associated with lattice must be distinguished from round holes which are common within the lattice patch. These holes carry a very low risk of causing retinal detachment (approximately 0.274%).” The risk of clinical detachment is low despite the 1.5% prevalence of localized stationary detachment which may extend as far as 1 disc diameter from the lattice lesion.la
I. PERIPHERAL VITREORETINAL TRACTION
Generalized vitreoretinal traction in the retinal periphery causes the ophthalmoscopic appearance of “retinal white without pressure” or of “retinal white with pressure.“B1 These occur most likely because of distortion of the retinal internal limiting membrane by generalized vitreous base traction.‘* Although this vitreous base traction theoretically could result in tears of the retina, there is no evi- dence that the presence of these lesions in an eye with a retinal tear alters the prognosis of the tear.
J. MIOTIC THERAPY
Whether the inauguration of miotic therapy increases the risk from a retinal tear is unknown. It is well established that both strong (anticholinesterase) and weak miotics may cause tears and subsequent detach- ments.l~eo The miotic-induced detachments occur predominantly in myopes (75% of casesp and aphakes (24% of cases). These data and the theoretical movement of the vitreous body in accommodation” suggest that a retinal tear should be treated prior to the inaugura- tion of miotics.
K. CONTRALATERAL DETACHMENT
The approximately 25% incidence of bi- laterality of clinical retinal detachment21~2a~48 requires special consideration of the risk of detachment from a retinal tear in an eye con- tralateral to one with the history of detach-

64 Surv Ophthalmol 25 (2) September-October 1980 SIGELMAN
ment. Because there are no published data tion which forms a demarcation line along the which analyze specific risk factors for tears in margin of a retinal detachment.‘O The finding contralateral eyes, the risk factors must be in- of intraretinal pigment associated with the ferred from studies of contralateral retinal retinal tear in 47% (126/267) of cases of detachments. Tears comprise the bulk (71%ya clinical retinal detachments4 indicates that of retinal breaks that cause contralateral Pigmentation offers no Protection against detachments, compared to the rarity of round Progression of a retinal tear to retinal de- trophic holes (15%), disinsertions (2%) and a tachment. This is true for all types of retinal mixture of breaks (13%) as the cause. There is breaks. Among 95 horseshoe tears found in a great tendency for symmetry in the tear in clinical retinal detachment, 35 (39%) had the pair of eyes with detachment both in the Pigmentation at the Posterior edge of the flap. type of tear (89%) and its location (68%). Of 115 cases of retinal detachment secondary Cataract surgery increases the risk of con- to lattice degeneration, 74 (64%) showed in- tralateral detachment to a level between 26%’ traretinal pigmentation at the site of at least and 40%.16 The mean interval between one of the retinal breaks. Of 14 retinal de- detachment in the first and second eyes is five tachments caused solely by atrophic round years in both phakic and aphakic patients?* holes, 2 (14%) showed pigmentation. Pigmen- The risk of contralateral detachment is tation at the retinal break is evidence only of largely unaffected by the patient’s age.Pz*28 prolonged vitreoretinal traction which either
Although these data offer no direct infor- caused the retinal tear or which caused an mation about the risk from a tear in a con- atrophic retinal break to progress to retinal tralateral eye, they do suggest that any tear in detachment. The pigmentation is not a sign of such an eye should receive prophylactic treat- a retinal-pigment epithelial bond strong ment. enough to prevent the progression of the
Prophylactic treatment of tears in this retinal detachment at the retinal break.
group of eyes has been shown to lower the C.DEMARCATION LINE rate of contralateral retinal detachment to 7%2a from the expected rate of approximately The presence of a pigmented demarcation
25%. The detachments which occurred in this line outlining the localized retinal detachment
series following treatment of a tear were surrounding a retinal tear has been inter-
caused by a previously undocumented break preted as a sign that the retinal detachment is
either adjacent to the treated area (40%) or unlikely to extend to become a clinical
remote from the treated area (60%). This detachment.le This concept is not justified by
limits the effectiveness of prophylactic sur- existing data.“‘*” The presence of a pigment
gery. demarcation line indicates only that the boun- daries of the detachment have been stable for
IV. Anatomic Data the three months necessary for the pigment to
A.SIGNS OF VITREOUS TRACI-ION accumulate from hyperplasia and metaplasia of pigment epithelial cells which have broken
Anatomic detail at the site of a tear has loose from Bruch’s membrane to proliferate received great attention for its potential value in the subretinal space.48 The finding of the as a prognostic sign. Upon objective scrutiny, extension of retinal detachment beyond a however, some of the traditionally valued demarcation line indicates that the presence anatomic signs have shown no significant of a demarcation line does not render a prognostic value. These include pigmenta- retinal tear safe from leading to clinical tion, size of the tear and location of the tear. retinal detachment.O The signs which have been shown to be prognostically valuable are those that reff ect DS ‘rZE OF TEAR the state of vitreous traction on the tear. The size of a retinal break also is only a These signs relate to the operculum and suggestive index of the risk of retinal detach- margins of the tear which are the potential ment. Of 153 retinal breaks observed without points of vitreous attachment and traction. treatment, 20 (13%) of the horseshoe tears
B.PICMENTATION were larger than one-half disc diameter in size [9 (6%) of these being larger than 1 disc
Pigmentation at the site of a tear has the diameter] and had acute symptoms.s7 The same prognostic insignificanceb’ as pigmenta- asymptomatic retinal break was a horseshoe

VITREOUS BASE CLASSIFICATION OF RETINAL TEARS 65
tear which occupied the whole of the lower nasal quadrant. The other 17 horseshoe tears greater in size than one-half disc diameter failed to cause clinical retinal detachment during one to six years of followup. Large size would seem to increase the risk from a horseshoe tear although the overall risk, even for very large tears, remains low.
E. MERIDIONAL LOCATION OF TEAR
A retinal tear located in a superior quadrant has been interpreted as carrying a worse prognosis than one in an inferior location.C~C40S62 This traditional concept is in- consistent with established data. Horseshoe tears have been found to have only a slight preponderance among both myopic and non- myopic detachments.” The relative safety from an inferior tear derives from the slower spread of an inferior detachment compared to a superior detachment so that an inferior detachment may be diagnosed and treated before macular involvement occurs.
F. ANTEROPOSTERIOR LOCATION OF TEAR
Another traditional teaching has been that the more posterior the tear’s location, the greater the risk of detachment.16*40~55 Published data do not support this concept. In both phakic and aphakic nonmyopic eyes with retinal detachment, tears have been found to be most prevalent anterior to the equator.76 In myopic detachments, either phakic or aphakic, the tears are located more anteriorly so that they are near the ora serrata.
V. Objective Determination of Tear’s Risk
A. IMPORTANCE OF VITREOUS TRACTION
Out of this entire collection of data correlating the risk of retinal detachment with parameters of clinical history and ex- amination, there emerges no single parameter or group of parameters consistently useful for judging the risk of retinal detachment from a retinal tear. At best, these data offer statistical risks based on only a few of the many significant parameters available for determination in each eye. In order to make a judgment based on more than a statistical correlation, it is necessary to isolate the fac- tors which cause a retinal tear to lead to retinal detachment. The element common to all the correlations between clinical
parameters and the risk of retinal detachment is the degree of vitreous traction on the retinal tear. Traction is transmitted by the anatomic connection between the vitreous fibers and the inner retina.2s Without significant trac- tion, a retinal tear may remain stable for many years. With traction on the retinal tear, the binding force between the retina and the pigment epithelium is overwhelmed so that the retina first separates locally from the pig- ment epithelium. 8s This allows greater hydra- tion of the mucopolysaccharide matrix between the retina and the pigment epithelium. As this matrix hydrates, the adhe- sion between the retina and pigment epithelium is 1ost.82 As tractional force con- tinues to elevate the retina, the matrix becomes increasingly hydrated and the retinal detachment progressively enlarges. If the dehydrational force of the pigment epithelium is stronger than the tractional force, the detachment may remain partial. If the dehydrational mechanism is completely overwhelmed, the retinal detachment will become complete.
The best objective of a tear’s risk would be to determine directly the degree of vitreous traction on the margins of the tear. Although this remains a clinical impossibility, a method is available for directly determining the anatomic relationship between the retinal tear and the vitreous traction on it. The details of this anatomic relationship provide the most direct of all available clinical clues of vitreous traction at the point of the retinal tear.
B. VITREOUS BASE CATEGORIZATION
In his study of autopsy eyes, Foos~~~~~ has originated a system for categorizing retinal tears on the basis of their relationship to the vitreous base. The terminology of the Foos system has great potential for clinical use because it emphasizes the traction by the vitreous base as the most important determi- nant of a break’s prognosis. In his categoriza- tion, Foos has divided retinal breaks into tears, which result from vitreoretinal traction, and holes, which result from trophic retinal changes. This review has directed itself toward tears because they are the significant cause of retinal detachments. Foos has suggested dividing tears into four anatomic categories to aid in determining their clinical prognosis. These categories are: oral, in- trabasal, juxtabasal and extrabasal.
Oral tears occur at the ora serrata. In-

66 Surv Ophthalmol 25 (2) September-October 1980 SIGELMAN
trabasal tears are located within the vitreous base. Juxtabasal tears are located at the posterior border of the vitreous base. Ex- trabasal tears are located in the equatorial zone of the peripheral retina posterior to the vitreous base. Foos states, “with rare excep- tions, the cause of a retinal tear can be iden- tified by its location and, to a lesser extent, its morphologic features as well as the presence or absence of posterior vitreous detach- ment.“sO Determining the cause for a retinal tear may provide a more direct, objective and reliable guide to the prognosis of the tear than any of the multitudinous clinical features which correlate with the risk of retinal detachment.
C. CLINICAL METHODOLOGY
1. Indirect Ophthalmoscopy
In order to apply this system of categorization to clinical use, it is necessary to be able to identify the exact location of the vitreous base. Binocular indirect ophthal- moscopy may show the vitreous base inser- tion onto the retina as a peripheral band of white without pressure, or of white with pres- sure.81 This extends from the ora serrata to the posterior edge of the vitreous base. This ophthalmoscopic appearance probably results from distortion of the internal limiting mem- brane by the inserting fibers of the overlying vitreous base. An occasionally evident subtle sign of the location of the posterior edge of the vitreous base is a white ridge which is seen as scleral depression passes under the posterior edge of the vitreous base. In detached retina, the location of the vitreous base may be identified in some cases by a linear circumferential ridge of elevation in the detached retina.
2. Indentation Biomicroscopy
Slitlamp biomicroscopy provides a view of the central vitreous and posterior hyaloid. Although the Goldmann lens may allow a view of the peripheral vitreous up to the inser- tion of the vitreous base, the view is distorted and unclear because of the extreme angula- tion of the lens’ mirror necessary for a view of the extreme periphery. The use of indentation simultaneously with the contact lens permits the extreme retinal periphery and the vitreous base to be brought into clear view.2E Move- ment of the globe during indentation biomicroscopy causes the posterior hyaloid to
wave so that the point of its insertion to the retina at the posterior edge of the vitreous base may be determined with certainty.
The advantage of slitlamp biomicroscopy with scleral depression is that it allows a direct view of the vitreous base.24 The impor- tance of this view is that the behavior of the vitreous base can be judged independently from the remainder of the vitreous, including the posterior vitreous attachment at the disc or macula. The separate behavior of the vitreous base accounts for the retinal breaks and detachments which occur despite the lack of a posterior vitreous detachment.‘O In addi- tion, the width of the vitreous base is variable in different patients and in different locations of one eye. This requires a separate deter- mination in each individual at the meridian of the retinal break of how far posteriorly on the retina is the posterior edge of the anterior vitreous base.
VI. Oral Tears
A. ETIOLOGY
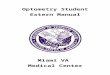
In the Foos classification of retina1 tears, oral tears are the most anterior. They occur at the ora serrata. The vitreous traction which causes these tears results from the posterior movement of the vitreous base (Fig. 1). This is opposite to the anterior direction of trac- tion which is responsible for all other retinal tears. The posteriorly directed traction results from complete avulsion of a section of the vitreous base from trauma or from a developmental abnormality.1B~72 Blunt trauma produces immediate vitreous base avulsion and oral tears which usually become evident within three weeks after injury.‘” The post- traumatic oral tears which are diagnosed long after injury may result from the slow progres- sion of the tear and of the accompanying retinal detachment.s Avulsion of the vitreous base in the superonasal or inferotemporal quadrants is thought to be pathognomonic for trauma. Some inferotemporal and superonasal oral tears have no relationship to trauma.80 The occasional occurrence of a bilateral inferotemporal oral tear may result from bilateral birth trauma or from a developmental defect, as in the autosomal recessive inherited cases.
The posterior traction by the vitreous base causes relentless progression in either the length of the oral tear or in the elevation of the posterior lip or in both. The accom-

VITREOUS BASE CLASSIFICATION OF RETINAL TEARS 67
FIG. I. Left: An oral dialysis (A) results from posteriorly directed traction by the vitreous base on the posterior flap of the tear. Right: This traction causes the posterior eversion of the edge (B). (Alice R. Sigelman, aGist).
parrying retinal detachment may progress as slowly as the change in the vitreous base con- figuration. In very slowly progressive cases, this allows adequate time for the formation of demarcation lines at the posterior edges of the consecutively larger detachments.
B. CLINICAL APPEARANCE
The traditional clinical name for an oral tear is dialysis.25*7g These tears are charac- terized by occurring at the ora, having no anterior flap but showing elevation and pos- terior rolling of the posterior flap. They range in size from minute (less than one-quarter clock hour) to 360 degrees. The flap is rolled most posteriorly in large, superior tears. In- ferior tears tend to show less rolling of the flap because of the lesser gravitational effect. Similarly, with the same extent of detach- ment, the height of the detachment tends to be greater with superior tears than with in- ferior tears.
The accompanying detachment may show a pigment demarcation line at the posterior border if the detachment has remained at that point for more than three months. Demarca- tion lines within the area of detachment result from the temporarily stationary position of the detachment before it progressed more posteriorly.
Because of the association of oral tears
with trauma and possible developmental ab- normalities, they occur at a much younger age than do the other types of tears. The peak age of occurrence is 20 years. They are rare after age 45.
(‘. MANAGEMENT
All oral tears should be considered to carry a sufficiently high risk of clinical retinal detachment to warrant prophylactic surgery. The surgery differs from that of other types of tears because of the posterior direction of vitreous traction on the posterior flap. In comparison, juxtabasal tears have traction primarily in the anterior direction on the anterior flap.
Closure of the posterior margin of the flap must extend to the ora serrata at both ends of the tear. Surgical scars joining the retina to the pigment epithelium may be placed without any scleral buckling procedure if the scars are placed in attached retina. This type of delimitation of a peripheral retinal detach- ment will be successful as long as the traction by the vitreous base does not increase. Inferior oral tears with limited detachment are safely managed with these noninvasive techniques.
Oral tears whose vitreous traction is likely to increase should undergo either a temporary or a permanent scleral buckling procedure to

Surv Ophthalmol 25 (2) September-October 1980 SIGELMAN 68
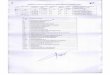
FIG. 2. Left: Intrabasal lesions include most areas of lattice degeneration (A) and operculated glial tufts (B). Right: These lesions do not progress to clinical detachment despite local surrounding subclinical detachment because of the lack of vitreous base traction. (Alice R. Sigelman, artist)
allow the margins of the tear to be sealed. Anchoring the tear’s margins may serve to stabilize the avulsed vitreous base which is at- tached to the tear’s posterior margin. Stabilization of the vitreous base lessens the risk of extension of the tear or of the detach- ment by the movements in the avulsed vitreous base which are caused by ocular movement.
The scleral buckling procedure should be performed to place the buckle beneath the posterior flap so that the band of retina ex- tending posteriorly from the anterior margin of the flap will be abutted to the pigment epithelium. This will allow a binding scar to form along the posterior margin. In tears with little retinal elevation, the buckle may be a temporary one, as provided by a cir- cumferentially placed sponge. In a case with a long or highly elevated tear, a permanent scleral buckle provides the advantage of per- manently alleviating severe vitreous traction.
VII. Intrabasal Tears
A. ETIOLOGY
Intrabasal tears are positioned within the
vitreous base and have zonuloretinal traction as their basic cause (Fig. 2). The tear results from either partial or complete avulsion of a preexisting zonular traction tuft.28 These tears are unrelated either to traction along the posterior edge of the vitreous base or to posterior vitreous detachment. The vitreous base and retina surrounding all sides of the tear are unremarkable. These tears may oc- cur at any age, 30 and unrelated to trauma and to lattice degeneration and usually, but not always, are single lesions. They comprised 6.1% of all full-thickness tears on autopsy study.30 The most important feature of in- trabasal tears is that the retina surrounding them is not under traction from the vitreous base. It is because of this lack of traction on the surrounding retina that intrabasal tears carry a good prognosis and rarely lead to clinical detachment.
B. CLINICAL APPEARANCE
Intrabasal tears may be flap tears or operculated tears. Autopsy studyZQ has shown most of them to be operculated. The hallmark of all intrabasal tears is that they are between

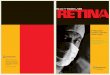
FIG. 3. Left: Juxtabasal tears have traction exerted primarily on their anterior edge by the posterior edge of the vitreous base. The posterior edge is free of traction. Right: Their earliest detachment is along the anterior margin. (Alice R. Sigelman, artist).
the ora serrata and the posterior edge of the vitreous base. They are more anterior than juxtabasal or retrobasal tears. Both the flap and the operculated intrabasal tears show the vestige of their zonoloretinal origin - a glial tuft with zonular attachments to the tip of the tuft. The operculated tears show an oper- culum which retains the linear form of the traction tuft. The avulsed tuft is drawn anterior to the ovoid break of retina which marks the previous location of the base of the tuft. The intrabasal flap tear shows a long narrow operculum which has the remnant glial tuft at the tip of the flap. Although the flap may be highly elevated, there is at most a very shallow and small surrounding retinal detachment which is most prominent on the anterior edge of the tear.
C. CLINICAL MANAGEMENT
Intrabasal tears do not warrant prophyl- actic surgery. They are unlikely to progress to clinical retinal detachment. The small shallow localized detachment which may sur- round the intrabasal flap tear remains sta- tionary because the traction exerted by the overlying vitreous is limited to a minor force on the tip of the operculum where the traction tuft connects the retina to the vitreous cortex. No generalized vitreoretinal force is exerted along either the anterior or posterior edges of an intrabasal tear.
VIII. Juxtabasal Tears
A. ETIOLOGY
When the posterior vitreous detaches, it may allow a sudden increase of the tractional force along the posterior border of the vitreous base. In a region of the vitreous base where the posterior border shows significant irregularity, the sudden increase in force may produce a flap tear. In regions of the vitreous base where there is no irregularity, the force is distributed evenly so that there is insufficient force to cause a tear.
B. CLINICAL APPEARANCE
The hallmark of all juxtabasal tears is that they are flap tears with the posterior margin lying along the posterior margin of the vitreous base (Fig. 3). Almost all juxtabasal tears are associated with posterior vitreous detachment. Juxtabasal flap tears are ovoid to round except for the anterior margin which is linear and parallel to the ora serrata. When the tear is fully developed, the base of the flap corresponds with the line of the posterior border of the vitreous on the sides at the base tear.
C. CLINICAL MANAGEMENT
Of the three anatomic groups of postoral tears, juxtabasal flap tears carry the highest risk of detachment. The risk of retinal detach-

70 Surv Ophthalmol 25 (2) September-October 1980 SIGELMAN
Fto. 4. Left: This juxtabasal horseshoe tear has a localized surrounding detachment. Treatment of only its posterior and lateral margins (middle) is insufficient because traction is primarily on the anterior margin. Treatment must extend along the anterior margin to prevent the extension of the localized detachment to a clinical detachment (right).
ment is high because traction by the posterior edge of the vitreous base increased acutely at the time of the occurrence of a posterior vitreous detachment. Compared to the low risk intrabasal flap tear, the juxtabasal flap tear carries a much greater risk because vitreous base traction is severe. It is severe because of the change in conformation of the vitreous and because the vitreous base trac- tion is exerted not only on the posterior edge of the flap but also along the anterior margin of the tear. This anatomic change creates the two conditions necessary for a detachment: a tear and traction on the margin of the tear. In comparison, the intrabasal flap tear does not have significant traction on its anterior margin.
The risk from the juxtabasal flap tear is greatest in the time immediately after the change in conformation of the vitreous body. This principle would place the greatest danger in periods following posterior vitreous detachment or cataract surgery. The risk may decrease after these acute events because the vitreous has had its opportunity to peel off the retina from the pigment epithelium at the site of the tear. The failure of detachment to oc- cur in the acute phase indicates that the bind- ing force of the retina to the pigment epithelium equals the tractional force on the retina at the site of the tear by the vitreous base.
D. SURGICAL INDICATIONS
All juxtabasal flap tears should be con- sidered as carrying significant risk of detach- ment. Those tears which have an acute symp- tomatic onset and those asymptomatic tears
which are discovered a short time (several months) after a posterior vitreous detach- ment or cataract surgery should undergo prophylactic surgery. Juxtabasal flap tears which are not part of an acute change in vitreous conformation remain vulnerable because of the potential for development of greater vitreous base traction at a future time. With expert surgical care, it probably is safer to treat than to leave untreated those tears which are unassociated with an acute posterior vitreous detachment and/or photopsia or floaters other than the floater of a posterior vitreous detachment. The tears which are not acute warrant further study by observing a group of these tears at close time intervals without treatment to determine their prognosis.
E. SURGICAL PRINCIPLES
The surgery of a juxtabasal flap tear should be aimed at preventing the development of a clinical detachment from the tear. This is done by sealing all the margins of the tear with a surgical adhesion between the pigment epithelium and the retina. It is the anterior margin of the tear which is the most overlookedso site of the treatment (Fig.. 4). Failure to treat the anterior margin of the tear allows traction by the vitreous base on the anterior flap of the tear to cause the ac- cumulation of subretinal fluid under the anterior flap. This fluid may progress to cause a clinical detachment despite sealing of the posterior and lateral edges.
F. SURGICAL TECHNIQUE
The surgical scars may be placed with xenon

FIG. 5. Left: An extrabasal break has no vitreoretinal adhesion at its margins. Right: Operculation of the tear frees it from the residual traction.
arc photocoagulation, laser,eg cryothermy47 or diathermy without a scleral buckle’* if the detachment surrounding the tear does not ex- tend more than 1 or 2 disc diameters from the margins of the tear. The treatments must be applied in the attached retina at the margins of the detached retina surrounding the tear. If treatments are placed in retina which is detached at the time of treatment or which becomes detached in the approximately two- week interval between treatment and the for- mation of permanent scarring, the treat- ments will be ineffective in halting the pro- gression of detachment.
If the detachment surrounding the tear ex- tends more than 2 disc diameters, including the extent of shallow detachment, a perma- nent or temporary scleral buckling procedure is warranted. The advantage of the buckling procedure is that it prevents the spread of subretinal fluid into the treated area during the postoperative period. This allows the for- mation of a permanent tight union between the retina and the pigment epithelium.
IX. Extrabasal Tears
A. ETIOLOGY
Extrabasal tears occur in the equatorial zone of the peripheral retina posterior to the posterior edge of the vitreous base (Fig. 5). They result at the time of a posterior vitreous detachment from vitreoretinal traction
focally concentrated on a preexisting cystic retinal tuft.
B. CLINICAL APPEARANCE
Extrabasal tears are almost always opercu- lated. In rare cases, a partially avulsed tuft may form an atypical flap tear with the flap occurring on the posterior margin of the tear instead of on the anterior margin as in jux- tabasal and intrabasal tears.
C. CLINICAL MANAGEMENT
Extrabasal tears should not be treated if they are operculated because they are free of any traction at the margins of the tear. They are unlikely to develop any more than a stationary localized surrounding detachment of less than 1 or 2 disc diameters from the margins of the tear. Serial observation should show no change in the tear except the possible development of pigment at the margins of the surrounding detachment.
If an extrabasal tear is in a transition phase where the operculum is only partially avulsed, the tear should be observed at close intervals without treatment. Only in the rare instance that the detachment should spread because of continued traction by the flap should surgery be performed. This surgery should consist of a scarring procedure to surround the localized detachment. This usually requires no tem-

72 Surv Ophthalmol 25 (2) September-October 1980
porary or permanent scleral buckling procedure because of the lack of traction around the tear except at the point of the flap.
I.
2.
3.
4.
5.
6.
7.
8.
9.
10.
I I.
12.
13.
14.
15.
16.
17.
18.
19.
20.
References
Ackerman AL: Retinal detachment and miotic therapy, in Pruett RC, Regan CD (eds): Retina Congress. New York, Appleton- Century-Crofts, 1972, pp 533-540. Adams ST: Retinal breaks in eye bank eyes. Arch Ophthalmol 55:254-260, 1956 Arentsen JJ, Welch RB: Retinal detachment in the young individual: A survey of 100 cases seen at the Wilmer Institute. J Pedatr
Ophthalmol 11: 198-202, 1974 Ashrafzadeh MT, Schepens CL, Elzeneiny II, et al: Aphakic and phakic retinal detachment. Arch Ophthalmol 89:476-483, 1973 Barishak Y R, Stein R: Retinal breaks without retinal detachment in autopsy eyes. Acta Ophthalmol (Kbh) 50:147-158, 1972 Benson WE: Prophylactic therapy of retinal breaks. Surv Ophthalmol 22:41-47, 1977 Benson WE, Grand MG, Okun E: Aphakia and retinal detachment. Arch Ophthalmol
931245-249, 1975 Bohringer HR: Statistiches zu Hautigkeit and Risiko der Netzhautablosung. Ophthalmol-
ogica 131:331-334, 1956 Byer NE: A clinical definition of lattice degeneration of the retina and its variations. Mod Probl Ophthalmol 15:58-67, 1875 Byer NE: Changes in and prognosis of lattice degeneration of the retina. Trans Am Acad Ophthalmol Otolaryngol 78:114-125, 1974 Byer NE: Clinical study of retinal breaks. Trans Am Acad Ophthalmol Otolaryngol
71:461-473, 1967 Byer NE Clinical study of senile retinoschisis. Arch Ophthalmol 79:36-44, 1968 Byer NE: Lattice degeneration of the retina. Surv Ophthalmol 23:2 13-248, 1979 Byer NE: Prognosis of asymptomatic retinal breaks. Arch Ophthalmol 92:208-210, 1974 Campbell CJ, Rittler MC: Cataract extraction in the retinal detachment-prone patient. Am J
Ophthalmol 73: 17-24, 1972 Cockerham WD, Freeman HM: Molehills, mountains and prophylaxis of retinal detach- ment. Arch Ophthalmol 79:655-656, 1968 Coleman DJ: Unified model for accom- modative mechanism. Am J Ophthalmol 69:1063-1079, 1970
Colyear BM, Pischel DK: Clinical tears without detachment. Am J Ophthalmol 41~773-792, 1956 Cox MS, Schepens CL, Freeman HM: Retinal detachment due to ocular contusion. Arch Ophthalmol 76:678-685, 1966 David MD: The natural history of retinal
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
SIGELMAN
breaks without detachment. Trans Am
Ophthalmol Sot 71:343-372, 1973 Davis MD, Segal PP, MacCormick A: The natural course followed by the fellow eye in patients with rhegmatogenous retinal detach- ment, in Pruett RC, Regan DJ (eds): Retina Congress. New York, Appleton-Century- Crofts, 1974, pp 643-659 Delaney WV: Equatorial lens pigmentation, myopia and retinal detachment. Am J
Ophthalmol 79: 194- 195, 1975 Delaney WV, Oates RP: Retina1 detachment in the second eye. Arch Ophthalmol
96:629-634, 1978 Dobbie JG: Cryotherapy in the management of senile retinoschisis. Trans Am Acad
Ophthalmol Otolaryngol 73:1059, 1969 Duke-Elder S, Dobree JH: System of Ophthalmology. Volume X. Diseases of the
Retina. London, Henry Kimpton, 1967, pp 789-790 Eisner G: Biomicroscopy of the Peripheral
Fundus. Berlin, Springer Verlag, 1973 Fine BS, Yanoff M: Ocular Histology.
Hagerstown, Md, Harper and Row, ed 2, 1979, p 38 Foos RY: Zonular traction tufts of the peripheral retina in cadaver eyes. Arch
Ophthalmol 82:620-632, 1969 Foos RY: Tears of the peripheral retina; pathogenesis, incidence and classification in autopsy eyes. Mod Probl Ophthalmol
15:68-81, 1975 Foos RY: Postoral peripheral retinal tears. Ann Ophthalmol 6:679-687, 1977 Foos RY: Posterior vitreous detachment. Trans Am Acad Ophthalmol Otolaryngol
76:480-496, 1972 Foos RY, Allen RA: Retinal tears and lesser lesions of the peripheral retina in autopsy eyes. Am J Ophthalmoi 64:643-655, 1967 Friedman Z, Neumann E, Hyans S: Vitreous and peripheral retina in aphakia. Br J Ophthalmol 57:52-57. 1973 Gonin J: Le decollement de la retina: Pathogenie-traitement. Lausanne, Librarie Payot et tie, 1934 GSttinger W: Senile Retinoschisis. Stuttgart, Georg Thieme Verlag, 1978 Graether JM: Retinal changes in degenerative myopia. Int Ophthalmol Clin 2:109-132, 1962
Halpern JL: Routine screening of the retinal periphery. Am J Ophthalmol 62:99-102, 1966 Hirose T, Lee KY, Schepens CL: Wagner’s hereditary vitreoretinal degeneration and retinal detachment. Arch Ophthalmol 89:176-185, 1973 Hirose T, Marcil G, Schepens CL, Freeman HM: Acquired retinoschisis: observations and treatment, in Pruett RC, Regan CDJ (eds): Retina Congress. New York, Appleton-

40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51
52.
53.
54.
55.
56.
57.
Century-Crofts, 1972, 489-504 Hosni FA: Management of peripheral retinal breaks. Ophthalmologica 166:265-288, 1973 Hudson JR: Marfan’s syndrome with retinal detachment. Br J Ophthalmol 35:244-245, 1951 Hyams SW, Friedman Z, Neumann E: The peripheral retina in myopia with particular reference to retinal breaks. Br J Ophthalmol
53:300-306, 1969
Hyams SW, Neumann E, Friedman Z: Myopia-aphakia. II. Vitreous and peripheral retina. Br J Ophthalmol 59:483-486, 1975 Kanski JJ, Daniel R: Prophylaxis of retinal detachment. Am J Ophthalmol 79:197-205, 1975
Kraushar MF, Schepens CL, Kaplan JA, Freeman HM: Congenital retinoschisis, in Bellows JG (ed): Contemporary Ophthalmol- ogy. Baltimore. Williams and Wilkins, 1972, QQ 265-290
Lincoff HA: The prophylactic treatment of retinal detachment. Arch Ophthalmol 66:48-60, 1961 Lincoff HA, Kreissig I: The retinal adhesion after thermal injury, in Pruett RC, Regan CDJ (eds): Retina Congress. New York, Appleton-Century-Crofts, 1972, 597-609 Machemer R, Lagua H: Pigment epithelial proliferation in retinal detachment. Am J Ophthalmol 80:1, 1975
Merin S, Feiler V, Hyams S, et al: The fate of fellow eye in retinal detachment. Am J
Ophthalmol 71:477-481, 1971 Meyer-Schwickerath G: Light Coagulation (translated by Drance SM). St Louis, CV Mosby, 1960, pp 56-65
Michaelson IC, Stein R, Neumann E, Hyams S: A national cooperative study in the preven- tion of retinal detachment, in Pruett RC, Regan CDJ (eds): Retina Congress. New York, Appleton-Century-Crofts, 1972, 533-540 Morse PH: Prophylactic treatment of retinal degeneration and retinal breaks without detachment, in Brockhurst RJ (ed): Controver- sy in Ophthalmology. Philadelphia, WB Saunders, 1977, pp 518-525 Morse PH: Symptomatic floaters as a clue to vitreoretinal disease. Ann Ophthalmol
7:865-868, 1975 Morse PH, Eagle RC: Pigmentation and retinal breaks. Am J Ophthalmol 79:190-193,
1975 Morse PH, Scheie HG: Prophylactic cryoretinopexy of retinal breaks. Arch
Ophthalmol 92:204-207, 1974 Morse PH, Scheie HG, Aminlari A: Light flashes as a clue to retinal disease. Arch
Ophthalmol 91:179-180, 1974 Neumann E, Hymas S: Conservative manage-
58.
59.
60.
61.
62.
63.
64.
65.
66.
67.
68.
69.
70.
71.
72.
13.
ment of retinal breaks. 56:482-486, 1972 Neumann E, Hyams S, Natural history of retinal
73
Br J Ophthalmol
Brakai S, et al: holes with specific
reference to the development of retinal detach- ment and time factor involved, in Michaelson IC, Berman ER (eds): Causes and Prevention of Blindness. New York/London, Academic Press, 1972, pp 404-408 Okun E: Gross and microscopic pathology in autopsy eyes. III. Retinal breaks without detachment. Am J Ophthalmol 51:369-391,
1961 Pape LG, Forbes M: Retinal detachment and miotic therapy. Am J Ophthalmol85:558-566, 1978
Pemberton JW, Freeman HM, Schepens CL: Familial retinal detachment and Ehlers- Danlos syndrome. Arch Ophthalmol 76:8 17-824, 1966
Robertson DM, Norton EWD: Long-term follow up of treated retinal breaks. Am J
Ophthalmol 75:395-414, 1973
Ruben M, Rajpuroht P: Distribution of myopia in aphakic retinal detachments. Br J Ophthalmol 60:517-521, 1976 Rutnin U, Schepens CL: Fundus appearance in normal eyes. IV. Retinal breaks and other findings. Am J Ophthalmol C&1063-1078,
1967
Scheie HG, Morse PH, Aminlari A: Incidence of retinal detachment following cataract ex- traction. Arch Ophthalmol 89:293-295, 1973 Schepens CL, Marden D: Data on the natural history of retinal detachment. Arch Ophthalmol 66:631-642, 1961 Sigelman J, Eisner G: Laser photocoagulation
with biomicroscopic scleral indentation. Arch Ophthalmol (in press) Stein R, Feller-Ofry V, Roman0 A: The effect of treatment in the prevention of retinal detachment, in Michaelson IC, Berman ER (eds): Causes and Prevention of Blindness. New York/London, Academic Press, 1972, pp 409-4 10 Straatsma BR, Zeegan PD, Foos RY, et al: Lattice degeneration of the retina. Trans Am Acad Ophthalmol Otolaryngol 78:87-l 13, 1974
Tasman WS: Posterior vitreous detachment and retinal breaks. Trans Am Acad Ophthalmol Otolaryngol 71:760, 1967 Tasman W, Shields JA: Disorders of the Peripheral Fundus. Hagerstown, Md, Harper and Row, 1980, pp 36-41 Tasman W, Shields JA: Disorders of the Peripheral Fundus. Hagerstown, Md, Harper and Row, 1980, p 205 Teng CC, Katzin HM: An anatomic study of the periphery of the retina. 1. Non-pigmented epithelial cell proliferation and hole forma-

74 Surv Ophthalmol 25 (2) September-October 1980 SIGELMAN
tion. Am J Ophthalmol 34:1237-1248, 1951 F. Retinoschisis 74. Tillery WV, Lucier AC: Round atrophic holes G. Posterior vitreous detachment
in lattice degeneration - an important cause H. Lattice degeneration of phakic retinal detachment. Trans Am Acad I. Lattice lesion Ophthalmol Otolaryngol 81:509-518, 1976 2. Pathology separate from lattice
75. Tolentino FI, Schepens CL, Freeman HM: 3. Holes in lattice Vitreoretinal Disorders. Philadelphia, WB I. Peripheral vitreoretinal degeneration Saunders, 1976, 269-284 J. Miotic therapy
76. Tolentino FI, Schepens CL, Freeman HM: K. Contralateral detachment Vitreoretinal Disorders. Philadelphia, WB IV. Anatomic data Saunders, 1976, 372-394 A. Signs of vitreous traction
77. Tulloh CC? Distribution of holes and tears in B. Pigmentation primary retinal detachment. Br J Ophthalmol C. Demarcation line 49:413-431, 1965 D. Size of tear
E. Meridional location of tear F. Anteroposterior location of tear
V. Objective determination of tear’s risk A. Importance of vitreous traction B. Vitreous base categorization C. Clinical methodology
I. Indirect ophthalmoscopy 2. Indentation biomicroscopy
VI. Oral tears A. Etiology
78. U.S. Bureau of the Census: Statistical
Abstract of the United States: 1978 (99th edi- tion) Washington, DC, p 6
79. Watzke RC: The ophthalmoscopic sign “white with pressure.” Arch Ophthalmol 66:8 12-823,
1961 80. Winslow R, Tasman W: Juvenile retinal
detachment. Trans Am Acad Ophthalmol Otolaryngol 85:607-618, 1978
8 I. Wedlenthal DT, Schepens CL: Peripheral fun- dus changes associated with ocular contusion. Am J Ophthalmol 62:465-477, 1966
82. Zauberman H: Normal chorioretinal adhe- sion, in Pruett RC, Regan DCJ (eds): Retina
Congress. New York, Appleton-Century- Crofts, 1972, 572-58 1
83. Zauberman H, deGuillebon H, Holly FJ: Retinal traction in vitro. Biophysical aspects. Invest Ophthalmol 11:46-55, 1972
Outline
I. Definition of terms II. Need for improved therapeutic criteria
A. Prevalence of tears vs. incidence of clin- ical detachments
B. Risks of surgery C. Socioeconomic considerations
III. Current therapeutic criteria A. Lack of specificity B. Symptoms C. Myopia D. Vitreoretinal syndromes E. Cataract surgery
B. Clinical appearance C. Management
VII. Intrabasal tears A. Etiology B. Clinical appearance C. Clinical management
VIII. Juxtabasal tears A. Etiology B. Clinical appearance C. Clinical management D. Surgical indications E. Surgical principles F. Surgical technique
IX. Extrabasal tears A. Etiology B. Clinical appearance C. Clinical management
Supported in part by the Glorney-Raisbeck Fund of the New York Academy of Medicine.
Reprint requests should be addressed to Jesse Sigelman, M.D., Cornell Ophthalmology Associates, 5 15 East 71st Street, New York, New York 10021.