Embed Size (px)
Citation preview

CONCEPTIONS
We need a prospective varicocelectomy trial
Controversy exists whether varicocelectomy improves preg-nancy rates in couples with male infertility. Unfortunately,the majority of data come from retrospective, poorlycontrolled studies (1), resulting in inadequate evidenceregarding the efficacy of this procedure in improving semenquality (2, 3). In addition, results from randomized,controlled trials are conflicting and methodologically ofpoor quality because of heterogeneous inclusion criteria,limited enrollment, and high dropout rates.
The Reproductive Medicine Network (RMN) is a multi-center clinical trial network funded by the Eunice KennedyShriver National Institute of Child Health and Human Devel-opment to design and conduct clinical trials focused onimproving reproductive outcomes in subfertile populations.Under the RMN a varicocele trial, ‘‘A Prospective, Random-ized Study of Microsurgical Varicocelectomy versus No Sur-gery in the Treatment of Male Partners with a PalpableVaricocele and an Abnormal Semen Analysis,’’was developedand prioritized to begin. Poor recruitment, however, led toclosure by the Data Safety Monitoring Board. Critical reviewof the investigators' collective experience from all fiveparticipating sites identified potential reasons for limitedrecruitment, including lack of interest by urologists (4). Wetherefore undertook a survey of US members of the Societyof Male Reproductive Urologist (SMRU) and Society of Repro-ductive Surgeons (SRS) to determine whether they considereda National Institutes of Health–funded varicocelectomy trialfor the treatment of male infertility to be important and bene-ficial. The survey also explored other potential recruitmentbarriers, including [1] previous treatment of couples beforereferral, [2] lack of full initial evaluation of the male partnerbeyond a semen analysis, [3] preference of infertile couplesfor aggressive treatment with IUI/IVF, and [4] lack of interestin a placebo arm.
The survey (Supplemental Materials, available online)was a brief Survey Monkey questionnaire assessing the levelof interest in prospectively studying outcomes of varicocelec-tomy surgery in infertile men. After institutional review boardreview, the American Society of Reproductive Medicine(ASRM) and SMRU boards approved an e-mail survey of USSMRU and SRS urology members. The survey was sent to100 US SMRU/SRS members who had e-mail addresses onfile with the ASRM. The 100 members represented 70SMRU-only members, 29 members of both SMRU and SRS,and 1 SRS-only member. Of these, 25 members responded.A second e-mail was sent to nonresponders from the same100-member cohort, resulting in eight additional responses.Last, 17 additional responses were obtained by providingthe same survey in paper form to US members attending the2012 SMRU annual meeting. Of the 50 responses, 2 wereexcluded for premature survey termination. Ultimately 48 re-sponses were used to tabulate results, yielding a 48% responserate (Supplemental Materials).
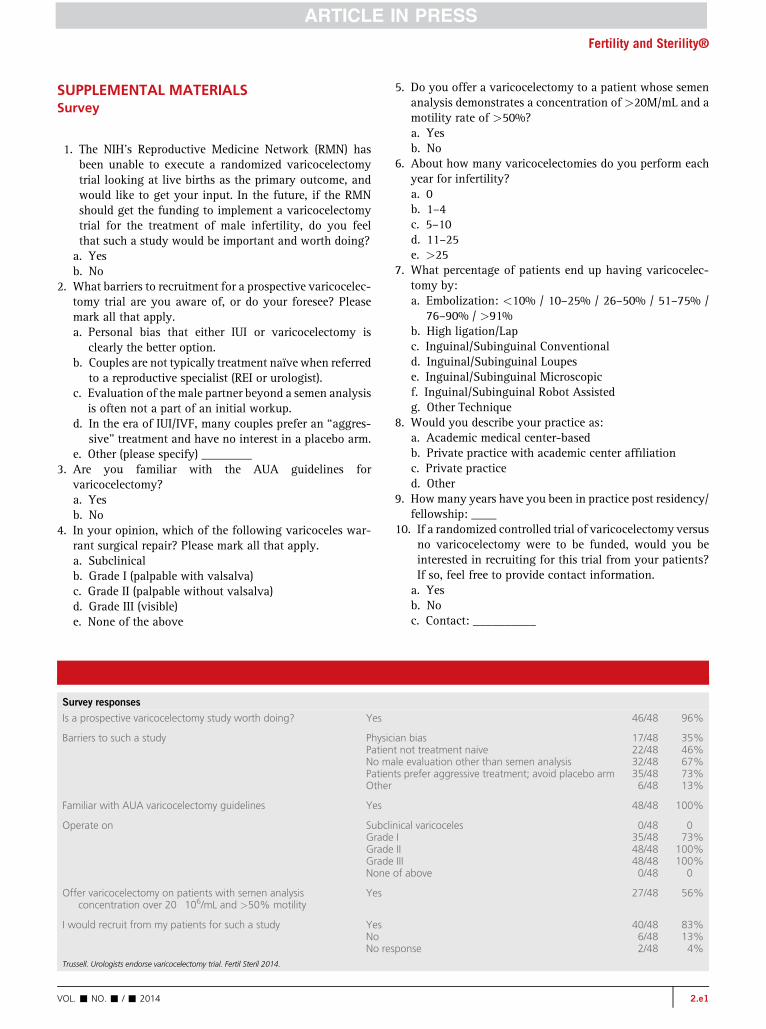
Of the 48 respondents, 46 (96%) indicated that a prospec-tive varicocelectomy trial for the treatment of male infertilityis important and should be performed. All respondents werefamiliar with the American Urological Association/ASRM
VOL. - NO. - / - 2014
varicocelectomy guidelines. A total of 83% perform a micro-scopic inguinal varicocelectomymost of the time, with no oneoperating on subclinical varicoceles. When given a scenarioof a patient with ‘‘normal’’ semen analysis (concentration>20 � 106/mL and motility >50%), 56% would still offer avaricocelectomy. Regarding ‘‘lessons learned’’ (perceivedrecruitment barriers), more than two-thirds of the respon-dents felt that two main recruitment impediments needed tobe addressed to improve future trial success: a lack of workup(beyond a semen analysis) and a couple's avoidance of a pla-cebo arm.
A lack of consensus in the field regarding the efficacy ofvaricocelectomy repair in infertile men would benefit fromreliable evidence to determine best practice (2, 3). Wecontinue to believe that a randomized, clinical trial isnecessary to more definitively address this issue.
The goal of this study was to survey US reproductive urol-ogists to learn whether there is support for a varicocelectomyrandomized, controlled trial. Broad support for a trial shouldminimize the potential for physician recruitment bias. Forexample, it is possible that urologists could unwittinglycommunicate to potential patients that a varicocelectomywas their best option, believing that a randomized trial wasneither necessary nor important. On the contrary, this surveyshows that urology-based physician bias for a varicocelec-tomy trial was minimal. Not only did 96% of respondentsfeel that this study was valuable, but 85% were also willingto recruit patients from their own practice for such a trial.Thus, motivation for such a critical clinical trial exists, leav-ing trial design as the next step to be carefully considered.
A secondary goal of the survey was to consider ways toimprove recruitment for future trials. Respondents focusedon two areas: [1] 67% felt a more detailed evaluation of themale was in order, whereas [2] 73% felt that a couple's innatedesire to avoid the placebo arm needed to be addressed. Themale evaluation could include expanding the semen analysisto assess DNA damage and sperm function. The second arearelates to the lack of incentive for men to participate in a studywith a placebo arm, especially for those already failing priortreatment attempts. To overcome the ‘‘placebo barrier,’’ afuture study should offer ovarian stimulation and IUI cyclesto both the treatment and placebo arms, in addition to offer-ing men in the non-varicocelectomy (placebo) group cross-over to the varicocelectomy arm after a predetermined periodof unsuccessful procreative cycles.
This survey was limited by its small sample size, with 100surveys only forwarded to members of two ASRM subspe-cialty societies within the United States. Furthermore, col-leagues within the field who provide male fertility(varicocele) referrals were not included in this survey. It isnot possible to know whether the 52 nonresponders weremore likely to think the study was important or unimportant.
Nonetheless, this survey demonstrated overwhelming(96%) support of US male fertility surgeons for a prospectivevaricocelectomy trial, with most respondents willing to re-cruit from their own practices. In addition to carefully consid-ered male- and female-factor inclusion criteria, future trialsshould attempt to optimize recruitment by offering both
1

Use your smartphone
CONCEPTIONS
stimulated IUI cycles and a placebo-arm cross-over tovaricocelectomy.
Acknowledgments: The authors thank Paul J. Turek, M.D,for his role as the RMN advisory board; Mark Sigman, M.D.and the ASRM board of trustees; Christy Davis for herASRM technical support; Robert Oates, M.D. and Paul J.Turek, M.D. for facilitating the survey of SMRU annualmeeting attendees.
The RMN also includes Ruben Alvero, M.D., Kurt T. Barn-hart M.D., Robert G. Brzyski, M.D., Ph.D., Peter R. Casson,M.D., Christos Coutifaris, M.D., Ph.D., M.S.C.E., Michael Dia-mond, M.D., Esther Eisenberg, M.D., M.P.H., Richard S. Legro,M.D., Randall Meacham, M.D., Nanette Santoro, M.D.,William D. Schlaff, M.D., David Shin, M.D., Tracey Thompson,M.P.H., Heping Zhang, Ph.D., and Meizhuo Zhang, Ph.D.
JC Trussell, M.D.a
Dana A. Ohl, M.D.b
Stephen A. Krawetz, Ph.D.c
Peter J. Snyder, M.D.d
Alex J. Polotsky, M.D.e
Pasquale Patrizio, M.D., M.B.E.f
Gregory M. Christman, M.D.g
For the Reproductive Medicine Networka Department of Urology, Upstate University Hospital,
Syracuse, New York; b Division of Sexual and ReproductiveMedicine, University of Michigan, Ann Arbor, Michigan;
c Department of Obstetrics and Gynecology, Center forMolecular Medicine and Genetics, Wayne State University,
Detroit, Michigan; d Department of Medicine, PerelmanSchool ofMedicine, University of Pennsylvania, Philadelphia,
2
Pennsylvania; e Department of Obstetrics and Gynecology,University of Colorado, Denver, Colorado; f Department of
Obstetrics and Gynecology, Yale University School ofMedicine, New Haven, Connecticut; and g Department of
Obstetrics and Gynecology University of Florida, Gainesville,Florida
http://dx.doi.org/10.1016/j.fertnstert.2014.02.041
You can discuss this article with its authors and with otherASRM members at
http://fertstertforum.com/trusseljc-reproductive-urologists-prospective-varicocelectomy-trial/
to scan this QR codeand connect to thediscussion forum forthis article now.*
* Download a free QR code scanner by searching for “QRscanner” in your smartphone’s app store or app marketplace.
REFERENCES
1. Ficarra V, Cerruto MA, Ligouri G, Mazzoni G, Minnuci S, Tracia A, et al. Treat-ment of varicocele in subfertile men: The Cochrane Review—a contraryopinion. Eur Urol 2006;49:258–63.
2. Evers JLH, Collins J, Clarke J. Surgery or embolisation for varicoceles in subfer-tile men. Cochrane Database of Systematic Reviews 2009:CD000479.
3. Will MA, Swain J, Fode M, Sonksen J, Christman GM, Ohl D. The greatdebate: varicocele treatment and impact on fertility. Fertil Steril 2011;95:841–52.
4. Trussell JC, Christman GM, Ohl DA, Legro RS, Krawetz SA, Snyder PJ, et al.Recruitment challenges of a multicenter randomized controlled varicocelec-tomy trial. Fertil Steril 2011;96:1299–305.
VOL. - NO. - / - 2014
Fertility and Sterility®
SUPPLEMENTAL MATERIALSSurvey
1. The NIH's Reproductive Medicine Network (RMN) hasbeen unable to execute a randomized varicocelectomytrial looking at live births as the primary outcome, andwould like to get your input. In the future, if the RMNshould get the funding to implement a varicocelectomytrial for the treatment of male infertility, do you feelthat such a study would be important and worth doing?a. Yesb. No
2. What barriers to recruitment for a prospective varicocelec-tomy trial are you aware of, or do your foresee? Pleasemark all that apply.a. Personal bias that either IUI or varicocelectomy is
clearly the better option.b. Couples are not typically treatment naïve when referred
to a reproductive specialist (REI or urologist).c. Evaluation of the male partner beyond a semen analysis
is often not a part of an initial workup.d. In the era of IUI/IVF, many couples prefer an ‘‘aggres-
sive’’ treatment and have no interest in a placebo arm.e. Other (please specify) ________
3. Are you familiar with the AUA guidelines forvaricocelectomy?a. Yesb. No
4. In your opinion, which of the following varicoceles war-rant surgical repair? Please mark all that apply.a. Subclinicalb. Grade I (palpable with valsalva)c. Grade II (palpable without valsalva)d. Grade III (visible)e. None of the above
Survey responses
Is a prospective varicocelectomy study worth doing? Yes
Barriers to such a study PhysicPatienNo maPatienOther
Familiar with AUA varicocelectomy guidelines Yes
Operate on SubcliGradeGradeGradeNone
Offer varicocelectomy on patients with semen analysisconcentration over 20�106/mL and >50% motility
Yes
I would recruit from my patients for such a study YesNoNo res
Trussell. Urologists endorse varicocelectomy trial. Fertil Steril 2014.
VOL. - NO. - / - 2014
5. Do you offer a varicocelectomy to a patient whose semenanalysis demonstrates a concentration of >20M/mL and amotility rate of >50%?a. Yesb. No
6. About how many varicocelectomies do you perform eachyear for infertility?a. 0b. 1–4c. 5–10d. 11–25e. >25
7. What percentage of patients end up having varicocelec-tomy by:a. Embolization: <10% / 10–25% / 26–50% / 51–75% /
76–90% / >91%b. High ligation/Lapc. Inguinal/Subinguinal Conventionald. Inguinal/Subinguinal Loupese. Inguinal/Subinguinal Microscopicf. Inguinal/Subinguinal Robot Assistedg. Other Technique
8. Would you describe your practice as:a. Academic medical center-basedb. Private practice with academic center affiliationc. Private practiced. Other
9. Howmany years have you been in practice post residency/fellowship: ____
10. If a randomized controlled trial of varicocelectomy versusno varicocelectomy were to be funded, would you beinterested in recruiting for this trial from your patients?If so, feel free to provide contact information.a. Yesb. Noc. Contact: __________
46/48 96%
ian bias 17/48 35%t not treatment naive 22/48 46%le evaluation other than semen analysis 32/48 67%ts prefer aggressive treatment; avoid placebo arm 35/48 73%
6/48 13%
48/48 100%
nical varicoceles 0/48 0I 35/48 73%II 48/48 100%III 48/48 100%of above 0/48 0
27/48 56%
40/48 83%6/48 13%
ponse 2/48 4%
2.e1





























