Embed Size (px)
Citation preview
1
WELSH AMBULANCE SERVICES NHS TRUST
REFRESHED INTEGRATED MEDIUM TERM PLAN
A FOCUS ON DELIVERING 2015/16 PRIORITIES
Version 1.0
27th May 2015
2
INTRODUCTION
The Welsh Ambulance Services NHS Trust (WAST) provides ambulance services
for the people of Wales which delivers high quality and patient led clinical care –
emergency, urgent, scheduled – wherever and whenever needed.
The Trust is changing the focus of its service to establish it as a quality focussed,
clinically led, clinically driven emergency medical service, non-urgent patient care
service and a 24 hour health care and advice service that focuses on delivering the
best clinical outcomes for patients. The Trust should be seen as an integral part of
the „front line‟ of the seven healthcare systems in Wales, with emergency and urgent
care services a fundamental part of the national unscheduled care system. The
Trust also works closely with Public Health Wales in our public health messaging
and understanding the changing health demographics that impact on the
unscheduled care system.
Services
WAST‟s three primary „service lines‟ are:
Emergency Medical Services (EMS) and Urgent Care Services (UCS)
Patient Care Services (PCS) – non emergency/ elective patient transport
NHS Direct Wales services.
The Trust also provides and supports a range of specialist services including:
HART (Hazardous Area Response Team)
SORT (Special Operations Response Team)
Supporting the Emergency Medical Retrieval and Transfer Service (EMRTS)
CHANT (Cymru inter Hospital Acute Neo-natal Transfer service)
Volunteer Car Service
Community First Responders
Cycle Responder Unit
Co-responder service (use of fire and police services staff)
Training in first aid.
The Integrated Medium Term Plan (IMTP) covers the three year period from 2015/16
to 2017/18 and builds on, and replaces, Working Together for Success 2011-16, the
Integrated Business Plan 2014/15-2016/17 and the Annual Delivery Plan 2014/15.
The IMTP provides the framework for the Welsh Ambulance Services NHS Trust
(WAST) to:
provide a clear statement of ambition for the benefit of patients, the public of
Wales, Trust staff and NHS partners (together with other external
stakeholders)
3
set out how it will deliver the Commissioning & Quality Delivery Framework
(CQDF) agreed with the Emergency Ambulance Services Committee (EASC)
describe the modernisation of non-emergency transport services
support the transition of NHS Direct Wales to the planned 111 service
Formal feedback regarding the original IMTP was received from Welsh Government on April 22, 2015. The feedback highlighted the following: Welcome progression in areas of the plan from earlier draft versions shared.
Recognition that this year is a pivotal year in the transformation of WAST as
the new arrangements bed down and the new commissioning framework is implemented.
The subsequent recognition that, in light of the point above, an approvable IMTP is unrealistic at this point.
The realisation that Welsh Government needs to work alongside WAST, the Chief Ambulance Commissioner, the Emergency Ambulance Services Committee and LHBs to ensure that the new arrangements translate to a more stable service model, improved performance and result in tangible benefits for patients, staff and the wider system.
The need for further discussions on WAST‟s approaches to strengthening and embedding planning across WAST and how the organisation‟s plans will be developed with LHBs so that plans are aligned.
The need to understand the key milestones for the development of the organisation‟s 2016/17 IMTP.
Advise that, until such time as the Trust Board and Welsh Government have approved an IMTP, the organisation will continue to be held account against the NHS Quality Outcomes Framework through bi-lateral discussions with the Director General/NHS Wales Chief Executive, the Quality & Delivery Meetings and supporting performance management structures as well as by commissioners.
This refreshed IMTP takes into account feedback from Welsh Government and specifically highlights the priorities and actions required in the coming year 2015/16 which will form a robust platform on which to build the Trust‟s three year strategy and secure approval of a three year IMTP from 2016/17. The IMTP refresh therefore:
4
Places a greater emphasis on the priorities for Y1 to ensure there is a robust
platform and a plan for moving into Y2 & 3.
Describes robust plans for actual delivery of the priorities that demonstrate
achievement in this year and instil confidence in delivering in future years.
Demonstrates that the critical areas of the original Strategic Transformation
Programme are incorporated into the IMTP, mapped to the organisations
priorities for 2015/16 and beyond and are managed effectively.
Demonstrates a „golden thread‟ running through the IMTP, the Quality
Delivery Commissioning Framework, financial plans and workforce plans so
that plans are integrated with key dependencies identified and managed to
deliver the overall vision and strategy of the Trust.
PRIORITIES FOR 2015/16
1. Developing a community engagement strategy and implementation plan to enable us to interact with all relevant stakeholders and promote community ownership of the service.
2. Agreeing, embedding and sustaining new clinical models in EMS, NEPTS and the transition from NHSDW, establishing the role of the Trust as a healthcare provider and clinical service rather than simply a transport service
3. Developing plans that localise the delivery of the IMTP (LDPs) minimising demand on the Ambulance Service, promoting choice for patients and improving the quality of patient outcome
4. Developing and implementing a Quality Improvement Plan that promotes better service user/patient experience and outcomes and forms the backbone of the transformation agenda.
5. Developing an integrated service, workforce and financial planning framework, delivering a balanced financial and workforce plan for 2015/16 that ensures safe and affordable establishments and demonstrates value for money and secures ongoing financial stability.
6. Developing a robust performance management framework that demonstrates accountability and transparency, meets the needs of the Trust and Commissioners and is timely and sufficiently detailed for a range of stakeholders within and outside the Trust.
7. Developing a workforce, OD and improvement transformation programme that is aligned to delivering the IMTP, and enables the Trust to achieve its aspiration to become a high performing organisation.
8. Strengthening the infrastructure required to support delivery e.g. governance framework, estates strategy, health informatics
5
The key priorities identified for the coming year are supported by clear “plans
on a page”, have defined executive sponsorship and a robust performance
management framework for delivery.
OUR STRATEGY
WAST‟s strategy for the period to 2017/18 needs to be seen within the following
context:
An increasingly elderly population and the growing incidence and prevalence
of chronic disease will drive changes in demand for emergency care.
WAST must redesign at pace its current clinical/ service model for emergency
care, patient care services and its workforce , as well as preparing for the
transition to 111.
There is an opportunity for WAST to extend its role to include better
supporting primary care and other forms of OOH/ unscheduled care to
improve integrated working.
There is an imperative to provide high quality care and deliver improved
efficiency/ productivity.
Commissioner requirements of WAST are evolving and commissioning
arrangements will mature over time. WAST will work collaboratively with its
commissioners and partner Health Boards to collectively improve the delivery
of unscheduled and planned care across the health system in Wales and
improve the experience and outcomes for patients.
WAST‟s strategy for the next three years is to:
Move from an emergency transport service to a clinically led, clinically driven
healthcare provider of emergency medical services and urgent care services
that focuses on optimum clinical outcomes for patients
Establish a reputation as a credible organisation which is an integral and
respected part of the Unscheduled Care system.
Be seen as a key partner in the delivery of a responsive, efficient, effective
and fully integrated transport and clinical care service that delivers dependent
users to care
The Trust will achieve this through:
Stabilising operational and financial performance(S)
Improving quality and safety (I)
Re-orientating the organisation in line with its mission to provide high quality
and patient led clinical care – emergency, urgent, scheduled – wherever and
whenever they are needed (R)
6
Transforming the effectiveness and efficiency of the organisation through a
process of organisational development, efficiency improvement, technological
innovation and engagement with both other emergency services and local
communities (T)
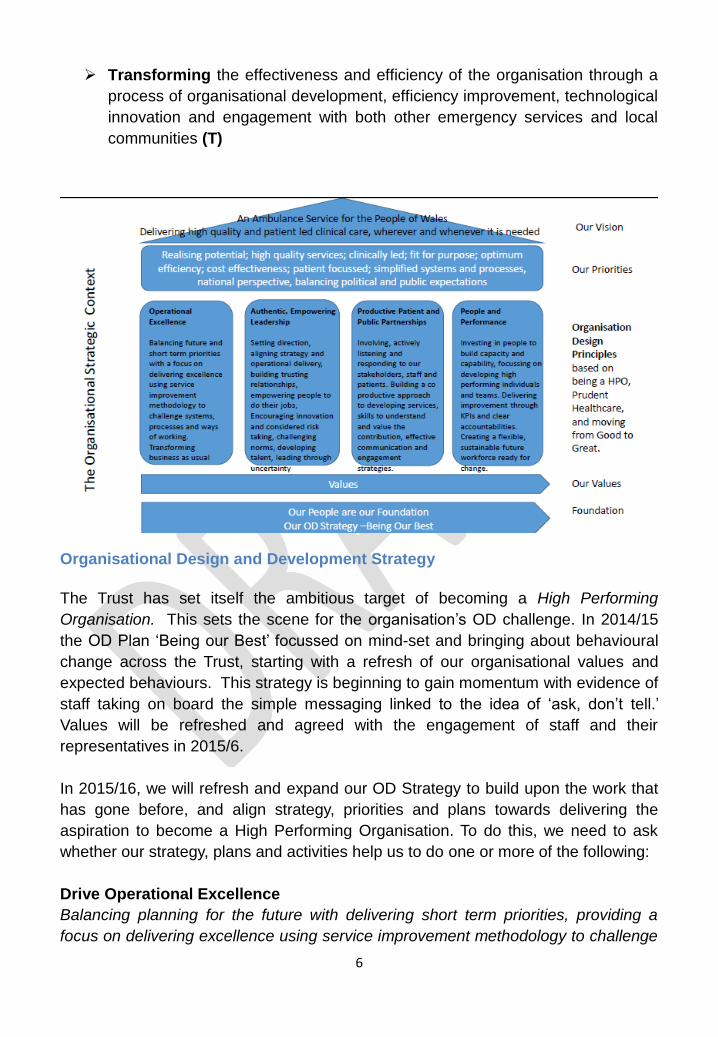
Organisational Design and Development Strategy
The Trust has set itself the ambitious target of becoming a High Performing
Organisation. This sets the scene for the organisation‟s OD challenge. In 2014/15
the OD Plan „Being our Best‟ focussed on mind-set and bringing about behavioural
change across the Trust, starting with a refresh of our organisational values and
expected behaviours. This strategy is beginning to gain momentum with evidence of
staff taking on board the simple messaging linked to the idea of „ask, don‟t tell.‟
Values will be refreshed and agreed with the engagement of staff and their
representatives in 2015/6.
In 2015/16, we will refresh and expand our OD Strategy to build upon the work that
has gone before, and align strategy, priorities and plans towards delivering the
aspiration to become a High Performing Organisation. To do this, we need to ask
whether our strategy, plans and activities help us to do one or more of the following:
Drive Operational Excellence
Balancing planning for the future with delivering short term priorities, providing a
focus on delivering excellence using service improvement methodology to challenge
7
systems, processes and ways of working. Identifying opportunities to transform
business as usual processes.
Develop Authentic, Empowering Leaders
Identifying and developing Leaders and true leadership behaviours; identifying
leaders capable of collaboratively involving others to develop a shared vision,
aligning strategy and operational delivery, listening and building trusting
relationships, and empowering people to do their jobs and operate at the top of their
scope of practice and competence. Developing clinical leaders who will provide
encouragement for innovation and support for considered risk taking; challenging
norms, developing talent, and importantly, leaders who can lead through uncertainty.
Create Co- Productive Partnerships
Involving, actively listening and responding to our patients, partners, staff, trade
unions and public expectations. Ensuring staff have the skills to understand and
value the contribution that engagement makes. Building a co productive
partnerships, to improve, develop and deliver services, ensuring real opportunities
for effective feedback, communication, engagement and listening.
Invest in People and Performance
Investing in our people to build capacity and capability, focussing on developing high
performing individuals and teams. Delivering improvement through performance
management processes, KPIs and ensuring clear accountabilities. Creating a
flexible, sustainable future workforce, resilient and ready for change.
The Trust‟s IMTP identifies 8 key enabling strategies and/or underpinning
programmes of work (including a need to ensure the infrastructure for delivery) as its
2015/16 priorities. The Workforce, OD & Improvement Programme is one of these
enabling programmes of work and will underpin and support the Trust to deliver
against all these ambitious OD aims and against IMTP priorities.
MEETING THE NATIONAL COLLABORATIVE COMMISSIONING: QUALITY &
DELIVERY FRAMEWORK AGREEMENT
Prior to the formation of EASC, there were inadequate arrangements and
documentation in place covering the commissioning of emergency ambulance
services between Health Boards and the Welsh Ambulance Services NHS Trust
(WAST).
The Emergency Ambulance Services Committee (EASC), at its inaugural meeting in
April 2014, sponsored the use of CAREMORE® for the creation of a Commissioning,
8
Quality & Delivery Framework Agreement („Framework Agreement‟) for Emergency
Ambulance Services.
A Collaborative Commissioning Project Group was established to lead the
production of the Framework Agreement, which consisted of representation, at
executive director level, from all Health Boards and WAST, together with Welsh
Government and Public Health Wales. Collaborative Commissioning was the
favoured methodology as it endorses the national „once for Wales‟ approach to
share and develop ideas in a non-competitive environment. This is the situation in
which CAREMORE® has been successfully applied to develop the „Framework
Agreement‟.
An Interim Collaborative Commissioning Agreement (ICCA) for 2014/15 was
developed by the Collaborative Commissioning Group and then agreed for 2014/15
between EASC and WAST. This agreement set out the original intentions for each
Section of the Framework Agreement, together with the interim arrangements for
2014/15 as a transitional year
The National Collaborative Commissioning Quality and Delivery Framework is an
agreement on key areas of service between NHS Wales Health Boards and WAST
through a new National Collaborative Commissioning: Quality & Delivery Framework
Agreement, which details:
what is required (commissioning);
how assurance is given for „what is required’ (quality); and
how the ‘what is required’ will be achieved (delivery).
The Quality and Delivery Framework, and the development of the new clinical
model, has a significant influence on the development of the revised Planning and
Performance Framework, the design and delivery of the workforce, organisational
development and improvement transformation programme and the finance and
resources plan that are detailed later.
EASC and WAST have sanctioned the Framework Agreement to become
operational from 1st April 2015 for a minimum of a three (3) year period that is
2015/16 to 2017/18.
It is recognised that the Framework Agreement will need to be a “live” document to
enable updating to take place as collaborative relationships/understandings of
service provision and required improvements between stakeholders develop.
Updating will also take place as and when policy changes are agreed and
implemented. Therefore, during 2015/16, there will be four refresh exercises
undertaken during quarterly intervals with updated elements of the Framework
Agreement issued at:
9
1st July 2015;
1st October 2015;
1st January 2016;
1st April 2016.
The refresh exercises will enable any documentation identified for inclusion within
the Framework Agreement but not yet finalised to be incorporated. Such changes
and documentation will be specified within the Document Management Section. It is
anticipated that the Framework Agreement may then be refreshed at six monthly
intervals during 2016/17 and 2017/18, that is:
1st October 2016;
1st April 2017;
1st October 2017.
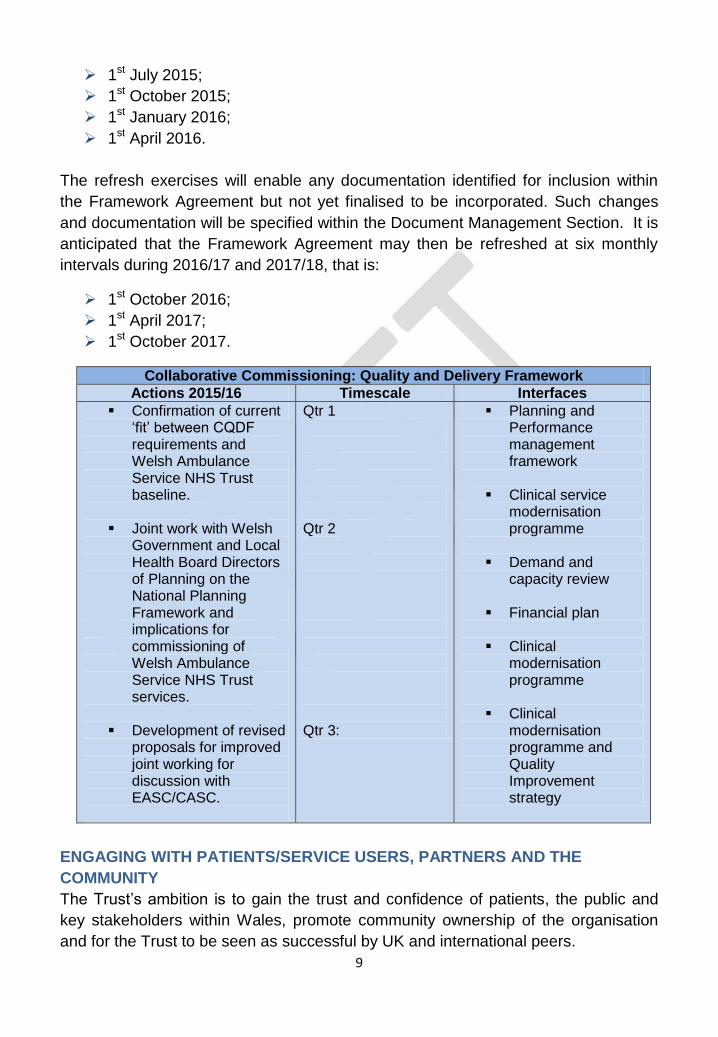
Collaborative Commissioning: Quality and Delivery Framework
Actions 2015/16 Timescale Interfaces
Confirmation of current „fit‟ between CQDF requirements and Welsh Ambulance Service NHS Trust baseline.
Joint work with Welsh Government and Local Health Board Directors of Planning on the National Planning Framework and implications for commissioning of Welsh Ambulance Service NHS Trust services.
Development of revised proposals for improved joint working for discussion with EASC/CASC.
Qtr 1 Qtr 2 Qtr 3:
Planning and Performance management framework
Clinical service
modernisation programme
Demand and
capacity review
Financial plan
Clinical modernisation programme
Clinical modernisation programme and Quality Improvement strategy
ENGAGING WITH PATIENTS/SERVICE USERS, PARTNERS AND THE
COMMUNITY
The Trust‟s ambition is to gain the trust and confidence of patients, the public and
key stakeholders within Wales, promote community ownership of the organisation
and for the Trust to be seen as successful by UK and international peers.
10
The Trust recognises that a lynchpin in the organisation‟s programme of operational
and cultural transformation, as well as its efforts to encourage responsible use of
999 and reduce demand, must be a coherent and comprehensive approach to
community engagement.
Such an approach must encompass patients/service users, stakeholders, partners
and the wider public, building shared understanding of the role and function of
WAST and developing community capacity and resilience through the development
of effective community partnerships. In addition, we must actively engage the public
in issues of service/model changes, both internal to WAST and across the wider
NHS Wales landscape and ensure that an effective programme of public education
and messaging supports appropriate use of 999 services.
In order to achieve this, the Trust recognises that its current engagement activities
need to be refreshed to ensure they are coherent and consistent with organisational
objectives, while acknowledging the good work already underway. The Trust has
committed to aligning its engagement activities through the development of a
discrete community engagement strategy, which will provide a clearly articulated
platform and delivery programme for this important aspect of our work.
The Partners in Healthcare Team lead service user engagement and have fully
implemented the National Service User Experience Framework. The Service User
Engagement Strategy 2014-2016 and implementation plan was approved by the
Quality Delivery Committee (QDC) in 2014 and patient experience feedback reports
are presented on a quarterly basis. Additionally patient stories are included on the
QUEST Committee and Trust Board agendas with updates on improvements made,
as a standing agenda item.
Community engagement is a key priority in year one of this IMTP and will underpin
the cultural move for the organisation and the public in respect of steps one and two
of the new clinical model and the establishment of the planned 111 service. The
Trust‟s community engagement model will require the support of Local Health
Boards and other local partners including the Third sector in providing the
opportunity for the Trust to contribute and participate in their community engagement
processes so that the work of the Trust is aligned with and integral to, the service
delivery of LHBs and the advisory role of other stakeholders.
Key priorities for 2015/16 include:
Measuring Patient Experience to inform us what it is like to be a user of Welsh
Ambulance Services
Real time capture of patient experiences
o reporting themes
o working with colleagues to identify and implement learning
11
o identify services changes/benefits
Working with communities to raise awareness and educate on services such
as Community First Responders and Choose Well
Working with other emergency response organisations such as the fire service
and police force to consider how we better interface to streamline response
and meet community needs
Collaboration with NHS colleagues on shared capture of patient experience;
learning and actions to improve experiences of the NHS care/treatment
pathways
Integrated reporting of all methods of patient/service user feedback
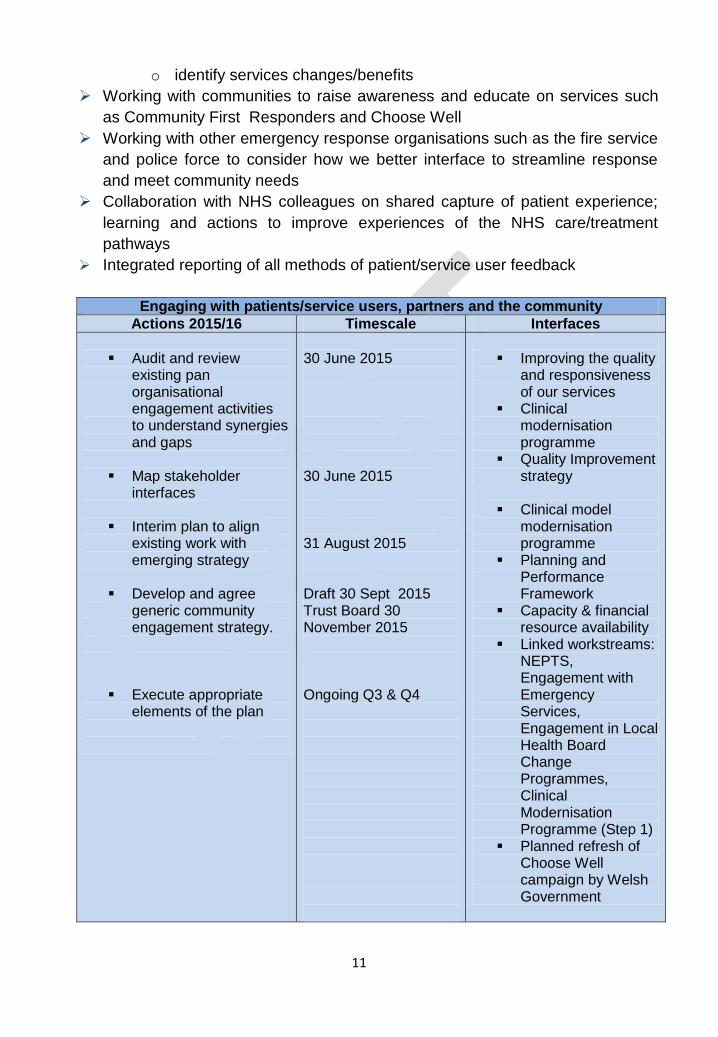
Engaging with patients/service users, partners and the community
Actions 2015/16 Timescale Interfaces
Audit and review
existing pan organisational engagement activities to understand synergies and gaps
Map stakeholder interfaces
Interim plan to align
existing work with emerging strategy
Develop and agree generic community engagement strategy.
Execute appropriate
elements of the plan
30 June 2015 30 June 2015 31 August 2015 Draft 30 Sept 2015 Trust Board 30 November 2015 Ongoing Q3 & Q4
Improving the quality
and responsiveness of our services
Clinical modernisation programme
Quality Improvement strategy
Clinical model
modernisation programme
Planning and Performance Framework
Capacity & financial resource availability
Linked workstreams: NEPTS, Engagement with Emergency Services, Engagement in Local Health Board Change Programmes, Clinical Modernisation Programme (Step 1)
Planned refresh of Choose Well campaign by Welsh Government
12
These activities represent a discrete Community engagement project which the
Trust has initiated. A plan on a page for this project is shown in annex 1.
DELIVERING FOR PATIENTS AND THE PUBLIC
The new clinical model for emergency medical services, non-emergency
patient transport and supporting the development of a 111 service
Emergency Medical Services
The current clinical/ service model focuses on time based response standards as a
means of recognising and meeting the needs of critically ill and injured patients.
Over time, however, increases in demand have forced changes in operational
practice, which, perversely, have resulted in inefficiencies and which have the
potential for unnecessarily high and unevenly distributed clinical risk. Recognised
examples cited in UK policy documents include:
Dispatching resources to a 999 call, on blue lights and sirens, before it has
been determined what the problem is, and whether an emergency ambulance
(EA) is actually required
Dispatching multiple ambulance vehicles to the same patient, on blue lights
and sirens, and then standing down the vehicles least likely to arrive first
Diverting ambulance vehicles from one call to another repeatedly, so that
ambulance clinicians do not focus on the care needs of the patient
Using a Rapid Response Vehicle (RRV) when this unit may provide little
clinical value to the patient (e.g. stroke victim), who then has to wait a long
time for a conveying ambulance to arrive
Very long waits for lower priority (“Green”) calls that nevertheless need
assessment and conveyance to hospital, and some of which have time
dependent conditions as determined by Health Care Professionals (HCP)
requesting patient transportation.
The new clinical model proposes a number of material changes to the current
model. The guiding principle underpinning the redesign process - improving patient
outcomes by offering the correct level of clinical intervention / care – is entirely
consistent with the Trust‟s commitment to prudent healthcare. The new model is
also entirely consistent with the requirement of commissioners to redesign EMS
along the five steps of the ambulance pathway.
Core elements
The core of the clinical model is the 5 step ambulance pathway agreed with
commissioners:

13
STEP 1 („Help Me to Choose‟) – This step focuses on public education regarding
the services provided by WAST and how/when to access them appropriately. This
step will include the development of appropriate linkages between WAST and the
future 111 service, building on the success of NHSDW and its website.
STEP 2 („Answer my Call‟) – This step focuses on the response to 999 and Health
Care Professional (HCP) calls by WAST‟s Clinical Contact Centres (CCCs). This
step incorporates the provision of adequate time to assess a call and the use of the
Medical Priority Dispatch System (MPDS) to identify the priority of the call before
offering / sending the most appropriate response.
STEP 3 („Come to See Me‟) – This step focuses on how WAST makes decisions
about what resources to dispatch to assessed/prioritised calls. Broadly, three
response options will be available:
Emergency Ambulances (EAs) will be allocated to RED calls, and high acuity
GREEN calls („see & treat‟)
Clinical Telephone Assessment (CTA - „hear & treat‟) will be offered to all
other low acuity GREEN calls
A dedicated patient transport service will be created for low acuity GREEN
patients who are assessed by HCPs as requiring admission to hospital.
STEP 4 („Give Me Treatment‟) – This step focuses on the development and
delivery of a range of clinical care services able to offer a variety of treatment
options. The selection of the most appropriate treatment will be supported by
decision support tools eg Paramedic Pathfinder for „see & treat‟; the Manchester
Triage System and the Clinical Assessment System for „hear & treat‟). Treatment
options will include the use of Alternative Care Pathways or ACPs (set out in a
Directory of Services) allowing patients to be referred to primary and community
care. WAST will develop a Clinical Hub to coordinate the delivery of care to patients
(„sign – posting‟ for clinical advice, managing referrals to alternative care pathways,
and arranging non-emergency transportation i.e. managing any element of WAST‟s
services that is not time critical or an emergency transport to ED).
STEP 5 („Take Me To...‟) – Patients who require ongoing care and treatment will be
transported to hospital or to alternative care settings (e.g. Minor Injury Unit or a
primary/community care facility). The clinical acuity of the patient will dictate the level
Step 1 –Help me to
choose
Step 2 –Answer my call
Step 3 -Come to see me
Step 4 –Give me
treatment
Step 5-Take me
to Hospital
14
of transport. For critical care patients or patients requiring ongoing treatment, EAs
will be utilised. All other patients will be transported by a combination of Urgent Care
Services (UCS) and non-emergency patient transport services (NEPTS).
The Trust is clear that the new service model/ model of care will deliver the following
benefits:
The sickest patient will always be treated first
The centrality of patient and public safety will maintained at all times
Patients will receive care which meets their clinical needs rather than wants
Delivery of the best clinical outcome for each and every patient on every
occasion and optimal patient experience
A reduction in overall clinical risk within the ambulance service model by
offering a range of treatment options, once the patient‟s need has been
identified.
Implementation will be enabled by:
The development of a robust demand and capacity model
Reconfiguration of the CCCs to provide the optimum level of control room
resource, consistency of operation and site interoperability
Implementation of the new Computer Aided Dispatch (CAD) system
Investment in new vehicles and the associated clinical equipment.
Continued development of clinical frontline staff described in the workforce
and OD section of the plan.
Enhanced clinical audit to evaluate the outcomes of the clinical model
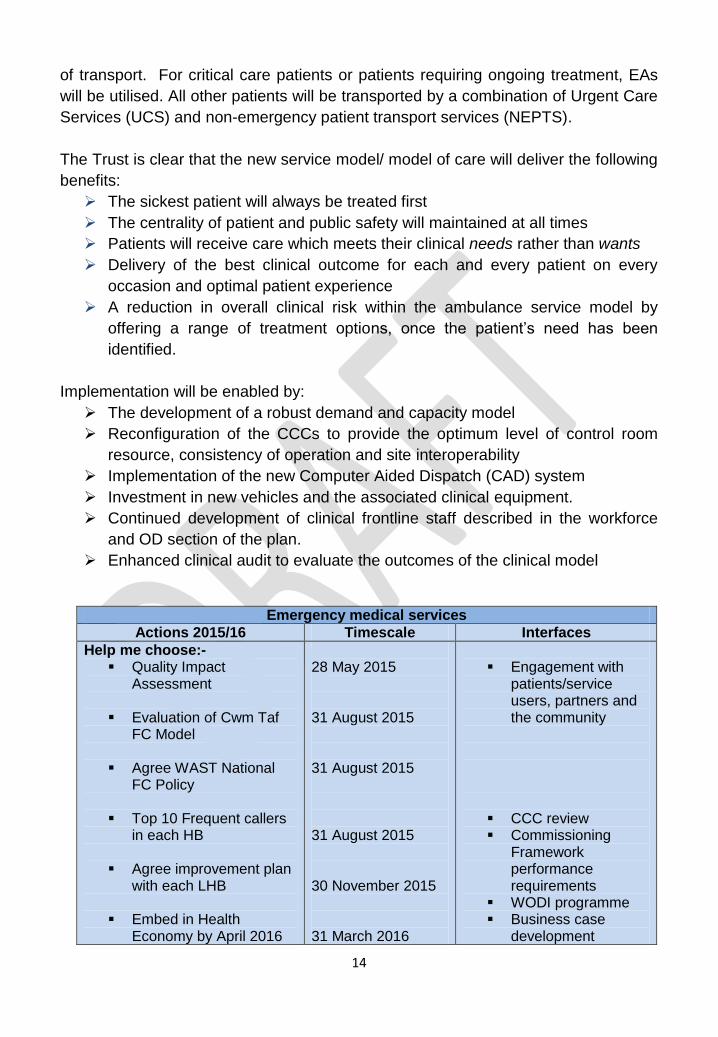
Emergency medical services
Actions 2015/16 Timescale Interfaces
Help me choose:- Quality Impact
Assessment
Evaluation of Cwm Taf FC Model
Agree WAST National FC Policy
Top 10 Frequent callers
in each HB
Agree improvement plan with each LHB
Embed in Health Economy by April 2016
28 May 2015 31 August 2015 31 August 2015 31 August 2015 30 November 2015 31 March 2016
Engagement with
patients/service users, partners and the community
CCC review Commissioning
Framework performance requirements
WODI programme Business case
development
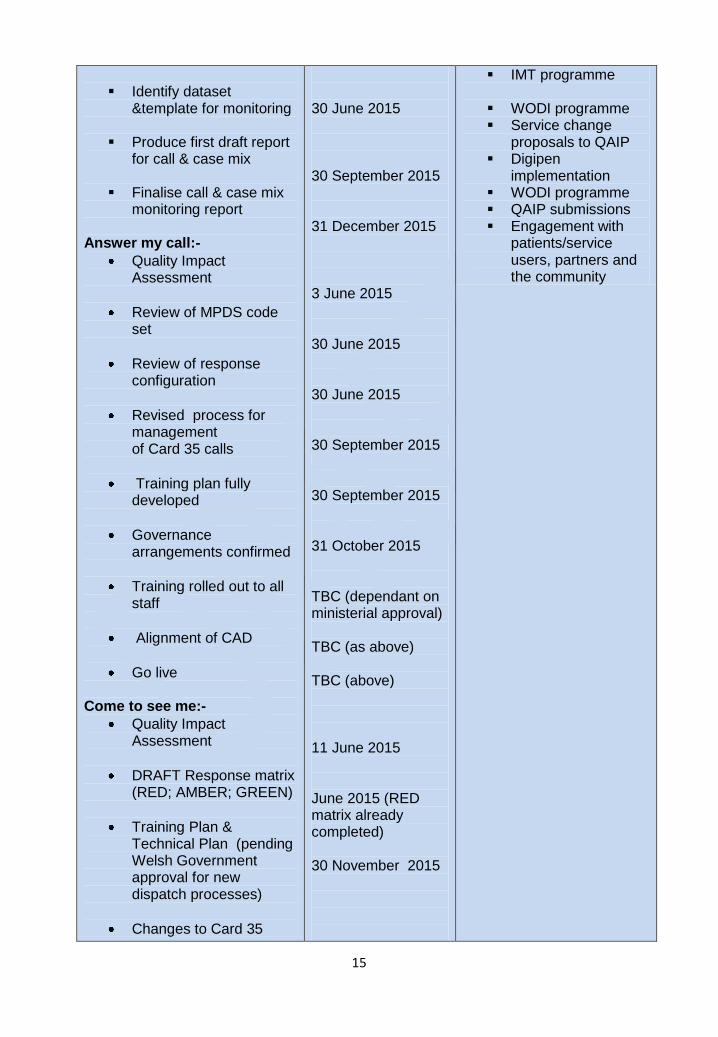
15
Identify dataset
&template for monitoring
Produce first draft report for call & case mix
Finalise call & case mix monitoring report
Answer my call:-
Quality Impact Assessment
Review of MPDS code set
Review of response configuration
Revised process for management of Card 35 calls
Training plan fully developed
Governance arrangements confirmed
Training rolled out to all staff
Alignment of CAD
Go live Come to see me:-
Quality Impact Assessment
DRAFT Response matrix (RED; AMBER; GREEN)
Training Plan & Technical Plan (pending Welsh Government approval for new dispatch processes)
Changes to Card 35
30 June 2015 30 September 2015 31 December 2015 3 June 2015 30 June 2015 30 June 2015 30 September 2015 30 September 2015 31 October 2015 TBC (dependant on ministerial approval) TBC (as above) TBC (above) 11 June 2015 June 2015 (RED matrix already completed) 30 November 2015
IMT programme
WODI programme Service change
proposals to QAIP Digipen
implementation WODI programme QAIP submissions Engagement with
patients/service users, partners and the community
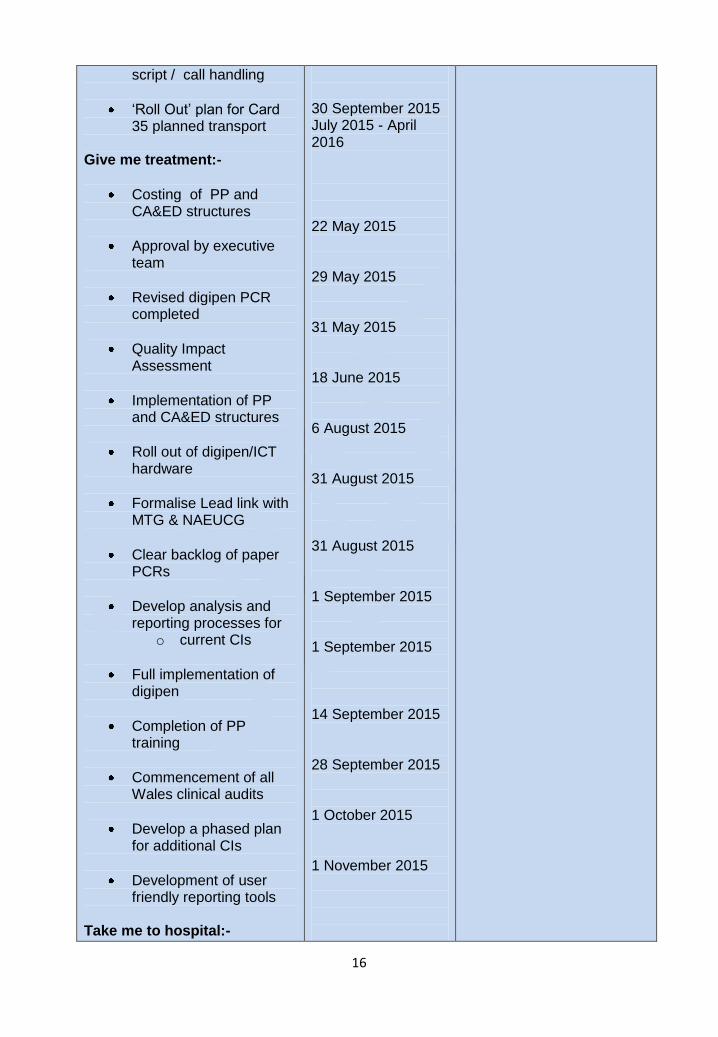
16
script / call handling
„Roll Out‟ plan for Card 35 planned transport
Give me treatment:-
Costing of PP and CA&ED structures
Approval by executive team
Revised digipen PCR completed
Quality Impact Assessment
Implementation of PP and CA&ED structures
Roll out of digipen/ICT hardware
Formalise Lead link with MTG & NAEUCG
Clear backlog of paper PCRs
Develop analysis and reporting processes for
o current CIs
Full implementation of digipen
Completion of PP training
Commencement of all Wales clinical audits
Develop a phased plan for additional CIs
Development of user friendly reporting tools
Take me to hospital:-
30 September 2015 July 2015 - April 2016 22 May 2015 29 May 2015 31 May 2015 18 June 2015 6 August 2015 31 August 2015 31 August 2015 1 September 2015 1 September 2015 14 September 2015 28 September 2015 1 October 2015 1 November 2015
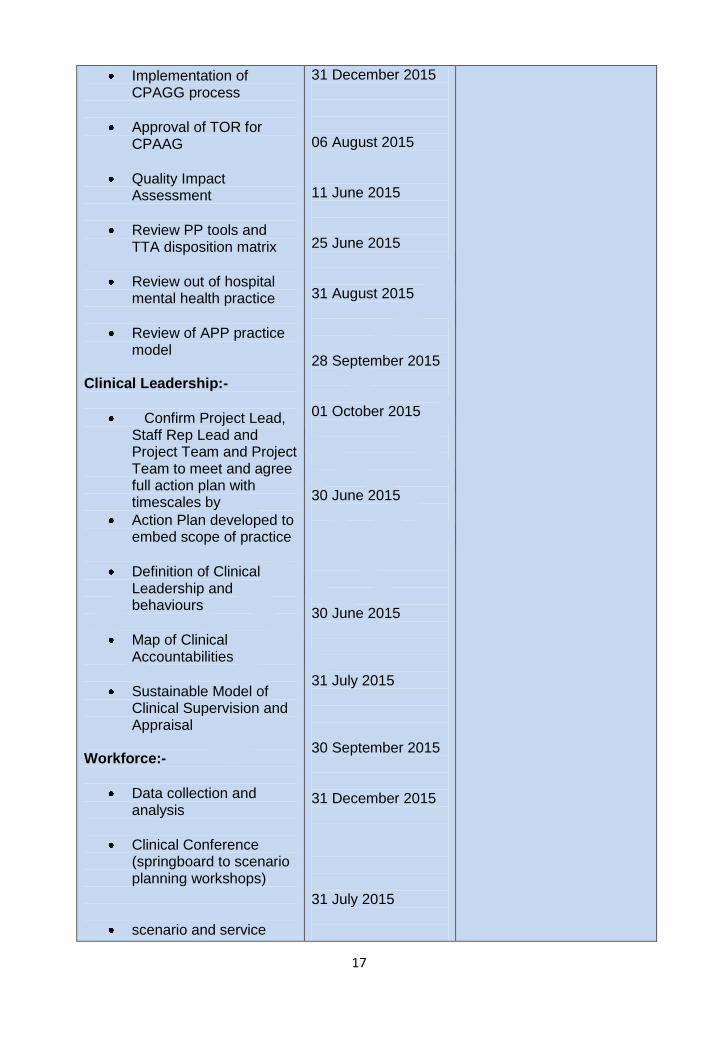
17
Implementation of CPAGG process
Approval of TOR for CPAAG
Quality Impact Assessment
Review PP tools and TTA disposition matrix
Review out of hospital mental health practice
Review of APP practice model
Clinical Leadership:-
Confirm Project Lead, Staff Rep Lead and Project Team and Project Team to meet and agree full action plan with timescales by
Action Plan developed to embed scope of practice
Definition of Clinical Leadership and behaviours
Map of Clinical Accountabilities
Sustainable Model of Clinical Supervision and Appraisal
Workforce:-
Data collection and analysis
Clinical Conference (springboard to scenario planning workshops)
scenario and service
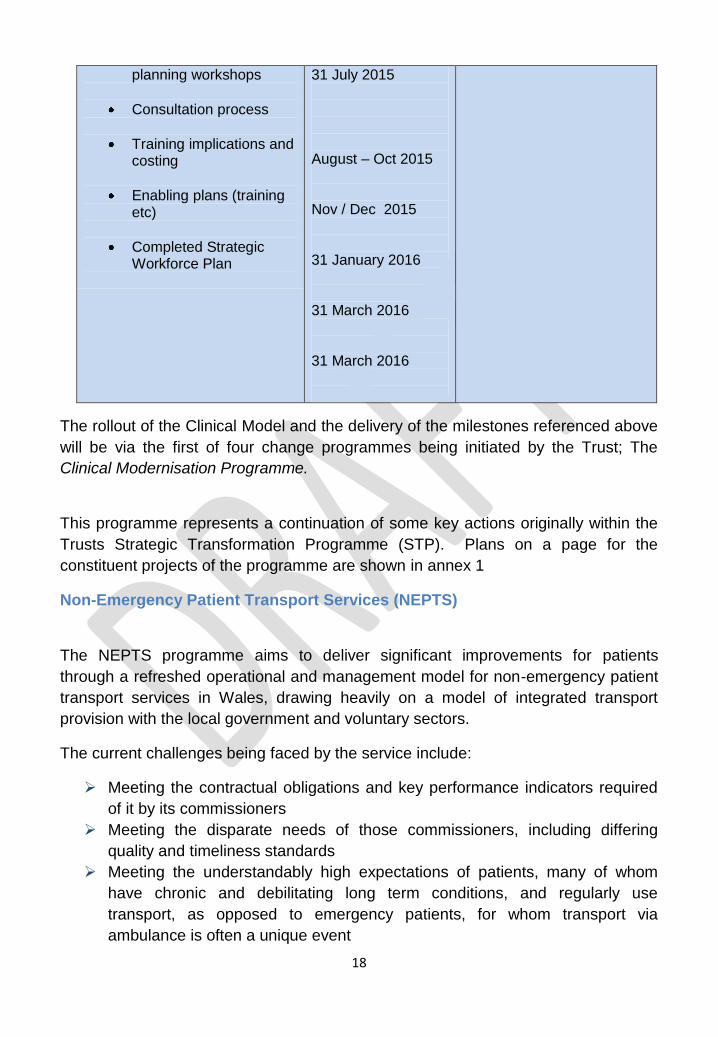
31 December 2015 06 August 2015 11 June 2015 25 June 2015 31 August 2015 28 September 2015 01 October 2015 30 June 2015 30 June 2015 31 July 2015 30 September 2015 31 December 2015 31 July 2015
18
planning workshops
Consultation process
Training implications and costing
Enabling plans (training etc)
Completed Strategic Workforce Plan
31 July 2015 August – Oct 2015 Nov / Dec 2015 31 January 2016 31 March 2016 31 March 2016
The rollout of the Clinical Model and the delivery of the milestones referenced above
will be via the first of four change programmes being initiated by the Trust; The
Clinical Modernisation Programme.
This programme represents a continuation of some key actions originally within the
Trusts Strategic Transformation Programme (STP). Plans on a page for the
constituent projects of the programme are shown in annex 1
Non-Emergency Patient Transport Services (NEPTS)
The NEPTS programme aims to deliver significant improvements for patients
through a refreshed operational and management model for non-emergency patient
transport services in Wales, drawing heavily on a model of integrated transport
provision with the local government and voluntary sectors.
The current challenges being faced by the service include:
Meeting the contractual obligations and key performance indicators required
of it by its commissioners
Meeting the disparate needs of those commissioners, including differing
quality and timeliness standards
Meeting the understandably high expectations of patients, many of whom
have chronic and debilitating long term conditions, and regularly use
transport, as opposed to emergency patients, for whom transport via
ambulance is often a unique event
19
Clear eligibility criteria understood by all
Developing new service model in co-production with service users
WAST has sought to bring together staff, trade unions, Welsh Government,
commissioners, voluntary sector providers and patient representatives in an
inclusive approach to change management, with a view to agreeing a revised model
of delivery which has credibility and the support of stakeholders.
The foci of the project include:
Agreeing the actions WAST will need to take to improve current NEPTS
performance
A generic specification for NEPTS in Wales that provides clarity in terms of
the quality and KPIs being commissioned
How NEPTS and other publicly funded/subsidised transport services (Social
Service, Special Educational Needs and Community Transport Association)
could be delivered in the future, the emphasis being to improve user
experience within a reduced financial envelope.
How a new way of delivering these services might be organised.
Expected outcomes include:
Improved current NEPTS operational performance
New specification providing clarity of KPIs, providing an increased opportunity
to monitor accurately and, therefore, measure provider services performance
Transference of low acuity NEPTS activity to alternative, more appropriate
transport provision
A blue print depicting how all partner organisations might work together.
Improved overall user satisfaction and experience.
A NEPTS model that can support the modernisation of the EMS and other
related services.
An organisation that holds the dedicated capacity and capability required to
lead the field in delivering efficient, effective and responsive services.
The programme has made significant progress in creating dialogue with
stakeholders about the future shape of NEPTS services in Wales and work
continues to develop a model for the future.
Understanding that the existing NEPTS model of service delivery may change
following the introduction of a new service specification, WAST is keen to progress,
with minimum delay, service development opportunities that we believe will help
modernise current service provision, improving operational performance,
relationships with stakeholders, new partners and, above all else, patient
experience.
20
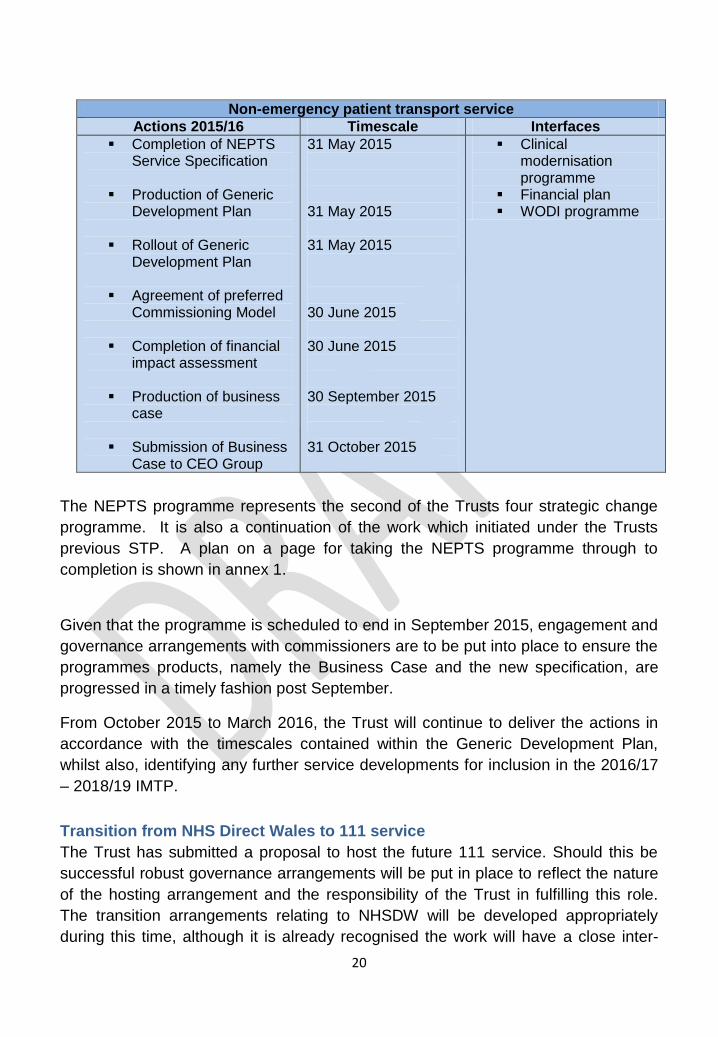
Non-emergency patient transport service
Actions 2015/16 Timescale Interfaces
Completion of NEPTS Service Specification
Production of Generic Development Plan
Rollout of Generic Development Plan
Agreement of preferred Commissioning Model
Completion of financial impact assessment
Production of business case
Submission of Business Case to CEO Group
31 May 2015
31 May 2015 31 May 2015
30 June 2015
30 June 2015
30 September 2015 31 October 2015
Clinical modernisation programme
Financial plan WODI programme
The NEPTS programme represents the second of the Trusts four strategic change
programme. It is also a continuation of the work which initiated under the Trusts
previous STP. A plan on a page for taking the NEPTS programme through to
completion is shown in annex 1.
Given that the programme is scheduled to end in September 2015, engagement and
governance arrangements with commissioners are to be put into place to ensure the
programmes products, namely the Business Case and the new specification, are
progressed in a timely fashion post September.
From October 2015 to March 2016, the Trust will continue to deliver the actions in
accordance with the timescales contained within the Generic Development Plan,
whilst also, identifying any further service developments for inclusion in the 2016/17
– 2018/19 IMTP.
Transition from NHS Direct Wales to 111 service
The Trust has submitted a proposal to host the future 111 service. Should this be
successful robust governance arrangements will be put in place to reflect the nature
of the hosting arrangement and the responsibility of the Trust in fulfilling this role.
The transition arrangements relating to NHSDW will be developed appropriately
during this time, although it is already recognised the work will have a close inter-
21
dependency with the Trust‟s Clinical Contact Centre (CCC) re-configuration
workstream (see Strategic Efficiency Programme).
IMPROVING THE QUALITY AND RESPONSIVENESS OF OUR SERVICES The Trust uses the principles of prudent health care, the requirements set out in the
NHS Wales Quality Outcomes Framework and assessment against the Health and
Care standards as a backdrop to the development and implementation of its quality
improvement strategy.
The Trust‟s Quality Improvement Strategy, Quality Delivery Plan and Quality
Improvement Assurance Framework incorporates the learning from local and
national reports including the Abertawe Bro Morgannwg University Health Board
“Trusted to Care” report and the Francis Report (2013) reviewing the care delivered
at Mid Staffordshire NHS Foundation Trust. This identified five key themes,
underpinned by the requirement of a fundamental quality improvement culture and
the adoption of common values across organisations focusing on:
fundamental standards;
openness, transparency and candour;
compassionate, caring and committed staff;
strong, patient-centred healthcare leadership; and
accurate, useful and relevant information.
One of the Trust‟s key strategic aims is to improve quality and safety: WAST‟s focus
- first, last, always – will be quality and safety.
22
The purpose of the quality improvement strategy is to support the delivery of this vision and our objectives to be a high quality clinically led service that:
Delivers high quality, cost-effective and sustainable health care services; Provides a working environment that is underpinned by our values and
behaviours; Is committed to patient-centred care and Treats staff and service users with dignity and respect.
This section sets out how this ambition will be realised. It describes in turn:
The structures and systems supporting quality management and improvement
The Trust‟s approach to infection prevention and control The Trust‟s approach to service user engagement The core elements of the emerging Quality Improvement Strategy together
with related quality improvement actions and activities How the Trust will progress the research and innovation agenda.
Year one of this strategy will focus on determining our position, strengthening our
foundations and developing and improving our indicators and measures. Years two
23
and three will be implementing, monitoring and reviewing, whilst making appropriate
changes.
Priorities for 2015/16 are:
Safeguarding
Infection Prevention & Control
Mortality reviews
Strengthening the Putting Things Right (PTR) process.
Structure and systems
The Trust Board has overarching accountability for the quality of services. The
Medical Director and Director of Quality & Nursing share joint accountability for
quality improvement at Executive Director level.
The portfolio of the Medical Director includes:
Clinical governance
Clinical/professional leadership of paramedicine
Putting Things Right
Clinical audit & effectiveness
Medical equipment
Public Health
Medicines management
Research & development
MPDS software – governance arrangements
Caldicott Guardian Executive lead
The portfolio of the Director of Quality & Nursing includes:
Quality & quality improvement plans in conjunction with the Medical Director
Implementation & monitoring of the Health and Care Standards
Service User Experience – Partners in Healthcare Team
Commissioning standards
Professional nurse leadership and nurse regulation/supervision of nurses
Executive lead for Infection Prevention & Control, Prudent Healthcare
Safeguarding / Mental Capacity Act / Deprivation of Liberty Safeguards
CAS software governance arrangements relating to NHSDW
The portfolio of the Director of Operations includes:
Frontline emergency medical services, non-emergency patient transport
services, Clinical Contact Centres and NHSDW
Specialist units (e.g. HART, HEMS, SORT)
Support services (e.g. fleet)
Civil contingencies/ emergency planning.
24
Quality Governance
In line with The Good Governance Guide for NHS Wales, the Board recognises that
a robust governance framework for quality is essential to deliver Trust-wide quality
services and to provide the Board with assurances over the effective and
sustainable management of quality across the organisation.
Through the medium of the Integrated Performance Report, each meeting of the
Trust Board includes scrutiny of a range of quality indicators and the extent to which
operational performance, HR and finance issues affect quality, safety and the patient
experience. The IPR is being redeveloped by June 2015/16 to support the
monitoring and management of the implementation of this IMTP, respond to
Commissioner requirements and provide meaningful performance information that
will support the delivery of services at all levels of the organisation.
The work of the Trust Board is currently supported by the Quality Patient Experience
and Safety Committee (QuEST). QuEST is a Board Committee with delegated
responsibility for all aspects of quality and safety and is chaired by a Non-Executive
Director. The IPR and Patient Experience Report / patient stories are standing
agenda items. In addition, reports relating to quality issues are included on the
annual work programme. The Committee reports to the Board following each
meeting (currently monthly).
The annual review of governance arrangements is currently in progress. This
includes:
a review of the terms of reference and minutes of the groups / committees
a review and defining of the reporting relationships between groups /
committees
information flows including appropriate escalation
implementation of the recommendations during 2015/16 from the review
monitoring during 2016/18 and actions taken accordingly.
Infection prevention and control
The Trust has adopted a zero tolerance of preventable healthcare associated
infections (HCAIs). Significant improvements in reducing HCAIs have been made in
recent years. However, more can and will be done to protect service users and our
staff to achieve world class standards of service user safety.
Key priorities for 2015/16-2017/18 include:
an agreed Code of Practice for Infection, Prevention and Control
development of an underpinning operational plan which will be monitored
through the Integrated Performance Report
25
an annual report on IPC reviewing progress, actual and potential risks and
informing future operational plans and staff development requirements.
The Trust quality strategy
The Trust aspires to be a quality driven organisation and an early priority is
developing a Quality Improvement Strategy (QIS) for the three years of the IMTP,
supported by a strong delivery plan for 2015/16.
The QIS will align with the requirements of the Quality Delivery Plan for Wales and
Safe Care, Compassionate Care, the NHS Delivery Framework and underpinning
delivery plans.
The QIS, the delivery plan and the performance management system will be based
on the following seven quality domains (as per the NHS Wales Quality Outcomes
Framework) below:
Domain / Theme Outcomes
Staying Healthy People in Wales are well informed to manage their own physical
and mental health
Safe Care
Prudent Healthcare
‘Do no harm’
People in Wales are safe and protected from harm and protect
themselves from known harm
Dignified Care People in Wales are treated with dignity and respect and treat
others the same
Effective Care
Prudent Healthcare
‘Carry out the
minimum appropriate
intervention’
People in Wales receive the right care and support as locally as
possible and are enabled to contribute to making that care
successful
Timely Care People in Wales have timely access to services based on clinical
need and are actively involved in decisions about their care
Individual Care
Prudent Healthcare
‘Promote equity & co-
production’
People in Wales are treated as individuals with their own needs
and responsibilities
Our Staff & Resources
Prudent Healthcare
‘Organise the
workforce around the
'Only Do, What Only
You Can Do’’
People in Wales can find information about how their NHS is
resourced and make careful use of them
Person Centred
Governance, Leadership & Accountability
26
The QIS will be refreshed on an annual basis and, in the first two years of the
planning cycle, will incorporate the following:
The outputs of the outcomes based internal assessment of the Standards for
Health Services in Wales 2013/14 and 2014/15, development of quality
indicators and a monitoring process for the key approved documents
associated with the Health and Care Standards.
development of „early warning quality triggers‟ & safety thermometer at Trust
level, then health board level, and progressing to locality / ambulance station
level with local ownership
using our information more intelligently in our reports, triangulating hard and
soft information, to provide a more informed picture of the quality of services
we provide e.g. incidents, complaints, internal and clinical audit reports,
service user feedback, staff feedback and external reports / visits
strengthen the clinical audit capability in terms of timeliness of data and scope
development with pace of the functions and outputs of the Organisational
Learning Group
introduction of Quality Impact Assessments (QIAs) incorporating the
principles of Prudent Healthcare for projects, cost improvement programmes
and service transformation / reconfiguration, including initial screening and
monitoring of quality indicators for medium or high risk schemes
introduction of mortality reviews
strengthen the process for reviewing and addressing external guidance and
recommendations
strengthen peer review and benchmarking with other NHS ambulance
services
continued implementation of the 1000 Lives + programme and use of
improvement methodologies including statistical process charts and other
measurements tools
walk around schedules covering all health board areas to obtain feedback
from staff to focus priorities
meeting the quality standards agreed with our commissioners using the
CAREMORE Framework.
Alongside the development and execution of the QIS, there are a range of other
actions and activities which the Trust will progress to improve quality. These include:
taking forward the priorities and actions identified in the Annual Quality
Statement including:-
o continued work to improve care for the frail elderly including working with
local dementia training groups to educate our staff
o supporting patients who fall to stay at home if appropriate
27
o an increase in the number of alternative care pathways
o improved working with Primary Care/GP and out of hours to better
manage patients within primary and community care
o improve the management of calls from Health Care Professionals (Card
35) to improve the flow of patients needing transport to hospital
the Partners in Healthcare Service User Engagement Strategy 2014-2016 to
inform our priorities on a rolling basis
membership and active participation in the NHS Wales National Quality &
Safety Forum
reviewing our process for responding to and learning from Putting Things
Right during 2014/15
the outcomes from reviewing our safeguarding processes during 2014/15.
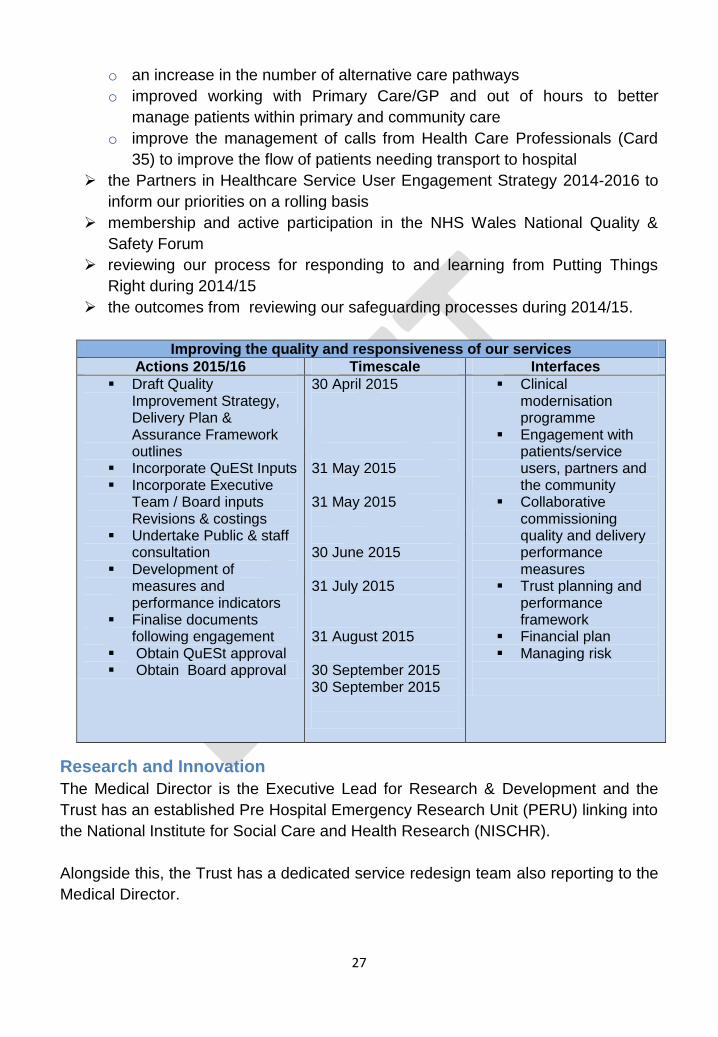
Improving the quality and responsiveness of our services
Actions 2015/16 Timescale Interfaces
Draft Quality Improvement Strategy, Delivery Plan & Assurance Framework outlines
Incorporate QuESt Inputs Incorporate Executive
Team / Board inputs Revisions & costings
Undertake Public & staff consultation
Development of measures and performance indicators
Finalise documents following engagement
Obtain QuESt approval Obtain Board approval
30 April 2015 31 May 2015 31 May 2015 30 June 2015
31 July 2015
31 August 2015
30 September 2015 30 September 2015
Clinical modernisation programme
Engagement with patients/service users, partners and the community
Collaborative commissioning quality and delivery performance measures
Trust planning and performance framework
Financial plan Managing risk
Research and Innovation
The Medical Director is the Executive Lead for Research & Development and the
Trust has an established Pre Hospital Emergency Research Unit (PERU) linking into
the National Institute for Social Care and Health Research (NISCHR).
Alongside this, the Trust has a dedicated service redesign team also reporting to the
Medical Director.
28
As part of the Clinical Modernisation Project within the STP, the Trust developed a
draft research & development strategy for the period to 2019. An early priority for
the Trust is to review this strategy in order to ensure ‟fit‟ with the IMTP.
Consideration in Y1 will be given to bringing PERU and the service redesign team
together to ensure joint working.
MANAGING RISK
The Trust has continued to develop and embed its approaches to risk management as set out in the 2014/15 Annual Governance Statement. The Trust sees active and integrated risk management as a key element in the
successful delivery of its business and remains committed to ensuring staff
throughout the organisation are trained and equipped to assess, manage, escalate
and report risks.The Trust also understands that effective risk management
processes must run in parallel with its clinical governance arrangements to ensure
the delivery of sustainable quality services and effective assurance mechanisms. In
order to strengthen our current risk management systems and processes during
2015/16, a risk management strategy (supported by an implementation plan) will be
developed and will include:
development of a revised Board Assurance Framework
a baseline risk maturity assessment with milestones for improvement
clear authorities for the management of risk
revision of the risk register framework
strengthening of the reporting / escalation mechanisms
a definition of our risk appetite
strengthening of the systems in place for policy & guideline development and
monitoring including archiving arrangements
an increase in incident reporting with a reduction in the severity of incidents
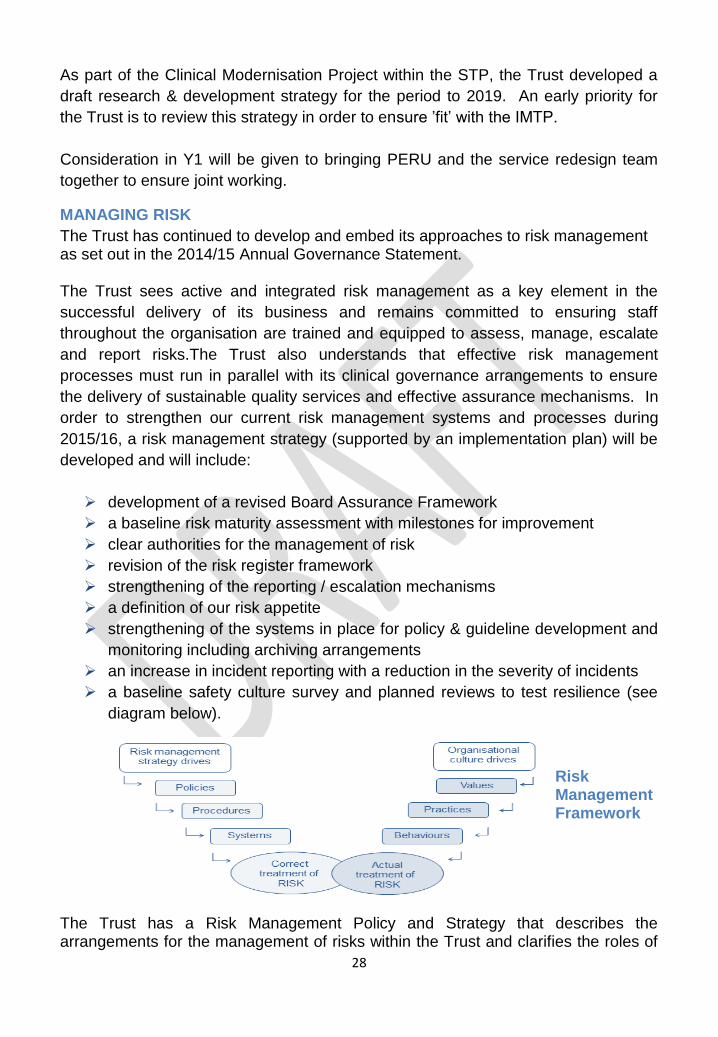
a baseline safety culture survey and planned reviews to test resilience (see
diagram below).
Risk Management Framework
The Trust has a Risk Management Policy and Strategy that describes the arrangements for the management of risks within the Trust and clarifies the roles of
29
individuals and committees. The risk assessment and risk register procedures provide for the identification and assessment of all categories of risks including clinical, financial and corporate risks. The Corporate Risk Register is available on the Trust intranet site for staff, managers and Board members to review. Risk Appetite The Trust recognises that effective risk management is a key component of corporate and clinical governance and is integral to the delivery of our objectives in service provision to the public. Whilst risk is inherent in many of our activities, the Trust will not accept risks that materially impair the ability to deliver services to a high standard of safety and quality. As such, the Trust will not accept risks that materially impair its reputation or cause any disrepute with stakeholders. In common with other NHS providers, the Trust is limited in the extent to which it is permitted to use public funds to reduce/eliminate risks. This is a major influence in determining the risk appetite of the Trust. Risk Profile The risk profile of the Trust is subject to ongoing in-year revision but, as at March
2015, there were eleven strategic risks on the Trust (High Level) Corporate Risk
Register. The risks and mitigation is detailed within the Trust Annual Governance
Statement and is subject to review by the appropriate committee.
Control framework The Trust uses the Health and Care Standards as its framework for gaining assurance on its ability to fulfil its aims and objectives for the delivery of safe, high quality health services. This involves self-assessment of performance against the standards across all activities and at all levels throughout the organisation. The Trust has recently completed its self-assessment against the standards and this demonstrates that there needs to be a greater maturity in respect of managing risk across the organization. This will be addressed through the action plan developed for 2015/16.
Managing risk
Actions 2015/16 Timescale Interfaces
30
Review risk management and assurance framework
Ensure corporate governance structures are embedded and ToR are reviewed
Develop and agree Annual Governance Statement
Produce Annual report
30 June 2015 31 July 2015 30 June 2015
30 September 2015
Improving quality and responsiveness
Planning and performance framework
MANAGING RESOURCES
Workforce and Organisational Development
The purpose of this section is to:
Set out key challenges currently facing the Trust in respect of the workforce
and the plans in place to address them
Provide a profile of the Workforce, OD and Improvement Project within the
Trust‟s Transformation Programme
A profile of the current WAST workforce and relevant KPIs
As assessment of the factors determining the future shape and size of the
workforce required to support delivery of the new clinical model for EMS and
an initial revised profile
Outline the changes expected to the education and training of paramedic staff
and the support needed to implement that change
The current WAST workforce
On the 1st April 2015, the Trust successfully transferred its HCS service and staff
(approximately 118 people) across to the NHS Wales Shared Services Partnership.
The Trust‟s workforce (as the end of April 2015) now totals 3,106 members of staff
broken down as follows:-
Directorate/ Service Headcount
CHIEF EXECUTIVE & CORPORATE SERVICES 20
CLINICAL 48
FINANCE & ICT 69
31
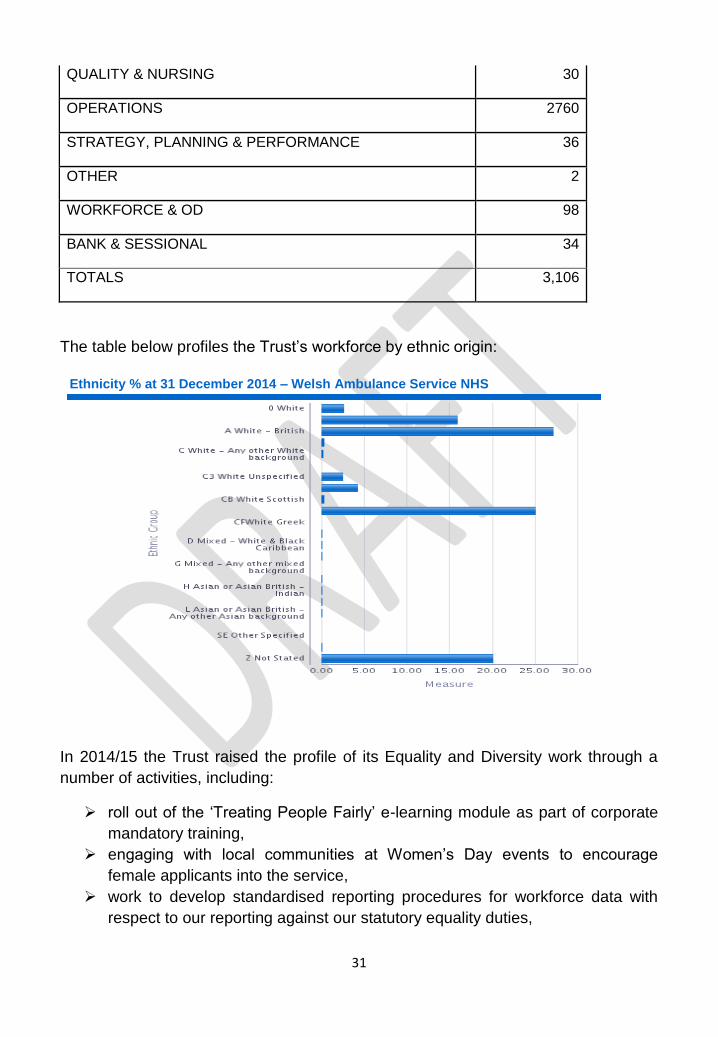
QUALITY & NURSING 30
OPERATIONS 2760
STRATEGY, PLANNING & PERFORMANCE 36
OTHER 2
WORKFORCE & OD 98
BANK & SESSIONAL 34
TOTALS 3,106
The table below profiles the Trust‟s workforce by ethnic origin:
In 2014/15 the Trust raised the profile of its Equality and Diversity work through a
number of activities, including:
roll out of the „Treating People Fairly‟ e-learning module as part of corporate
mandatory training,
engaging with local communities at Women‟s Day events to encourage
female applicants into the service,
work to develop standardised reporting procedures for workforce data with
respect to our reporting against our statutory equality duties,
Ethnicity % at 31 December 2014 – Welsh Ambulance Service NHS Trust
32
participation in Pride events across Wales, gaining positive feedback from
LGBT service users,
developed „transgender guidance‟ for call handlers and paramedics,
embedded within mandatory training (CPD) programmes,
work with Assistance Dog users across Wales to develop procedures and
guidance for the conveyance of assistance dogs.
2015/16 will see us review of our Strategic Equality Plan „Treat me Fairly,‟ through a
process of evidence gathering, literature review and staff and public engagement.
This will also include a review of our Strategic Equality Objectives. We also plan to
develop a Gender Action Plan, which will include working with the Women Adding
Value to the Economy (WAVE) toolkit, and working with Swansea University on
improving the gender split in paramedic education. We also intend to continue, and
increase where appropriate, our presence at relevant events across Wales such as
Pride, the development of staff networks, and action to embed a robust process of
Equality Impact Assessment (EQIA) across the Trust.
Reproduced below are our workforce and OD KPIs with accompanying commentary,
reported within the Trust:
Key Performance Indicator
WAST Indicator
Commentary
Turnover Period turnover rate covering 01/10/14 to 31/12/14 equates to 1.89%. Current year to date (31/12/14) turnover percentage is 5.52%
This is above the KPI <5% and further analysis work will be undertaken to identify reasons for staff leaving.
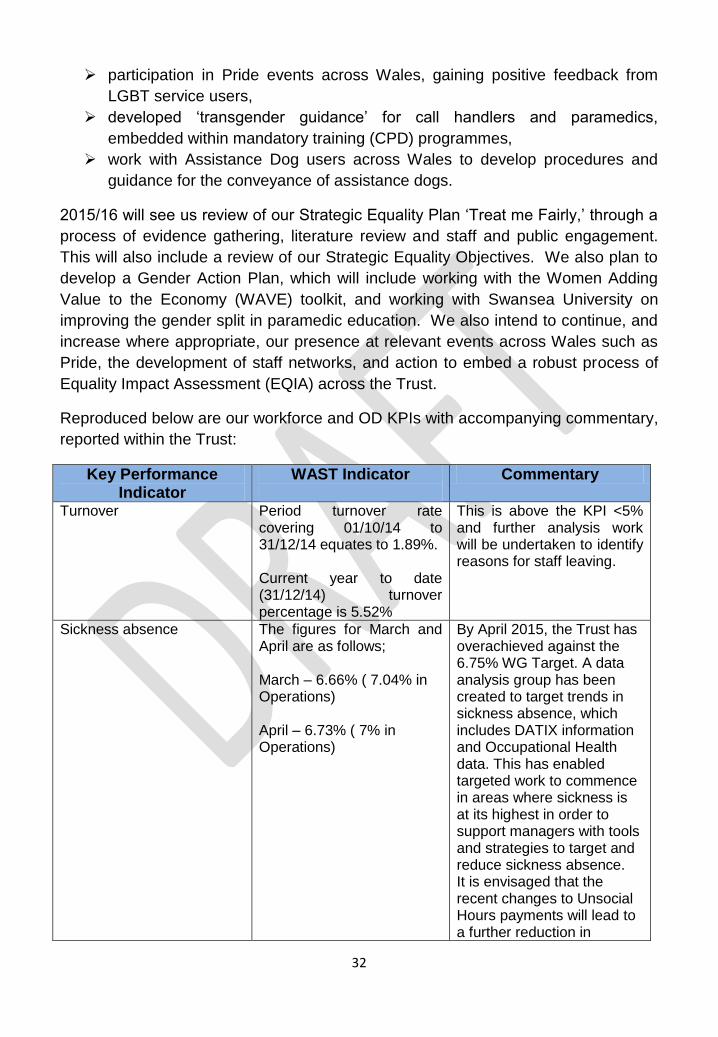
Sickness absence The figures for March and April are as follows; March – 6.66% ( 7.04% in Operations) April – 6.73% ( 7% in Operations)
By April 2015, the Trust has overachieved against the 6.75% WG Target. A data analysis group has been created to target trends in sickness absence, which includes DATIX information and Occupational Health data. This has enabled targeted work to commence in areas where sickness is at its highest in order to support managers with tools and strategies to target and reduce sickness absence. It is envisaged that the recent changes to Unsocial Hours payments will lead to a further reduction in
33
absence.
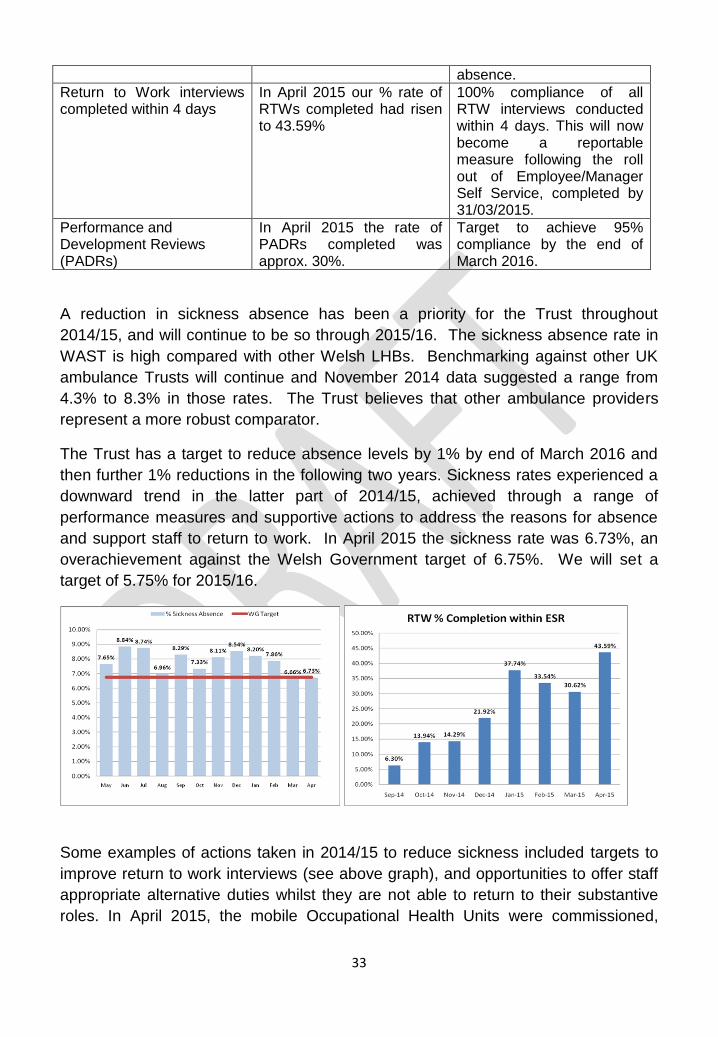
Return to Work interviews completed within 4 days
In April 2015 our % rate of RTWs completed had risen to 43.59%
100% compliance of all RTW interviews conducted within 4 days. This will now become a reportable measure following the roll out of Employee/Manager Self Service, completed by 31/03/2015.
Performance and Development Reviews (PADRs)
In April 2015 the rate of PADRs completed was approx. 30%.
Target to achieve 95% compliance by the end of March 2016.
A reduction in sickness absence has been a priority for the Trust throughout
2014/15, and will continue to be so through 2015/16. The sickness absence rate in
WAST is high compared with other Welsh LHBs. Benchmarking against other UK
ambulance Trusts will continue and November 2014 data suggested a range from
4.3% to 8.3% in those rates. The Trust believes that other ambulance providers
represent a more robust comparator.
The Trust has a target to reduce absence levels by 1% by end of March 2016 and
then further 1% reductions in the following two years. Sickness rates experienced a
downward trend in the latter part of 2014/15, achieved through a range of
performance measures and supportive actions to address the reasons for absence
and support staff to return to work. In April 2015 the sickness rate was 6.73%, an
overachievement against the Welsh Government target of 6.75%. We will set a
target of 5.75% for 2015/16.
Some examples of actions taken in 2014/15 to reduce sickness included targets to
improve return to work interviews (see above graph), and opportunities to offer staff
appropriate alternative duties whilst they are not able to return to their substantive
roles. In April 2015, the mobile Occupational Health Units were commissioned,
34
offering an innovative mobile service to staff for health screening and checks,
increasing access to early interventional support for staff.
Improving the wellbeing of our staff and achieving a continuous reduction in absence
rates remains a key priority for us through 2015/16. In order to do this, we will be
taking action to gain a deeper understanding of the reasons for sickness absence
and refreshing our annual action plan as part of the work of a sickness task and
finish group established to drive forward this agenda within our Workforce, OD and
Improvement Programme.
„Our People‟ Strategy
Our People Strategy will ensure that we have a clear understanding of the strategic,
organisation, economic and demographic context within which we operate, and an
evidence based approach to developing and implementing innovative workforce and
OD (WOD) activities.
The illustration below provides a simple model of four key stages in the employment
journey around which WOD activity will be focussed.
Through a combination of getting the focus right, ensuring clear linkage between
WOD actions and organisation outcomes, and maximising use of our people and
their full capabilities, we will help make the Trust a great place to work for our staff,
and have a positive impact on patient safety, care and user experience.
The Trust has already made good progress towards addressing some of the
underlying issues of concern and in 2014/15, took positive action to improve the
health and wellbeing of staff and their working conditions. These can be summarised
as follows;
Significant leadership development support for colleagues across the
Trust at all levels of the organisation
•Planned deployment, safe staffing and future workforce
PLAN
•Right person, right behaviours, right job, right time
RECRUIT•Skills and Knowledge
to excel in the Job
DEVELOP
•Creating a Great Place to Work
RETAIN
35
Recruitment of 119 additional staff
Establishment of an in house Occupational Health service
Achievement of the bronze and silver Corporate Health Standards
Updating and approval of key workforce policies
Improving working relationships with Trade Unions partners.
Organisation development plan focussed on changing mind-sets and
behaviours to address previously identified issue of the bullying culture
Staff long service awards ceremonies
However, there are still significant ongoing operational challenges to be addressed,
alongside the need to deliver sustainable, long term culture change;
The need to identify and fill vacancies more swiftly
To complete the review of rotas in EMS, PCS and the Clinical Contact
Centres, and identify opportunities to increase efficiency and productivity
among the workforce
To improve retention rates and create a culture where the Trust is an
employer of choice in Ambulance Services
Further reduction in levels of absence and improved health and
wellbeing of our staff
In 2015/16 we will move into another phase of workforce, OD and improvement
transformation across the Trust, with the development of an ambitious programme of
activity (WODI Programme) that will enable the Trust to achieve its aspiration to
become a high performing organisation, and underpin delivery of all IMTP priorities,
and operational priorities highlighted above.
This WODI programme represents the third of the Trusts four change programmes.
Outstanding activity from the Trusts STP will be picked up here.
The Operational Workforce Plan 2015/16
The workforce plan supports delivery of the 2015/16 Integrated Medium Term Plan
(IMTP). Approximately 76.5% of total expenditure is on pay costs. Ensuring that
workforce numbers and skill mix are appropriate for the services being provided, is
key to delivering both service and financial plans, and essential to ensuring the Trust
has the right workforce in place to support the delivery of high quality patient care.
Our workforce plan headlines for 2015/16 are:
Identified savings from workforce of approximately £1.9m to be delivered
from a reduction in variable pay and improved efficiency,
A planned increase in our whole time equivalent workforce numbers across
the year by 24 wte.
36
Work to identify opportunities to reshape the workforce and change service
models in line with the developing new clinical model, and the consequent
impact on workforce numbers will be progressed through this coming year, as
we develop our strategic future workforce plan.
The required reduction in variable pay expenditure will be delivered through a range
of actions designed to reduce sickness absence by a further 1% to a target rate of
5.75%; action to fill existing vacancies to full establishment levels and streamlined
recruitment process with quicker time to hire, and through identified opportunities to
increase efficiency and productivity within teams – particularly within the Clinical
Contact Centre.
In 2014/15, the Trust took action to recruit an additional 119wtes (a mixture of UCS,
PCS and EMS posts). These new posts were intended to be additional to the
existing whole time equivalent establishment, with the intention of reducing reliance
on and need for overtime. This uplift in the fixed establishment has been factored
into the baseline establishments for 2015/16, shown in table 1 below. These new
staff will be fully operational from June 2015.
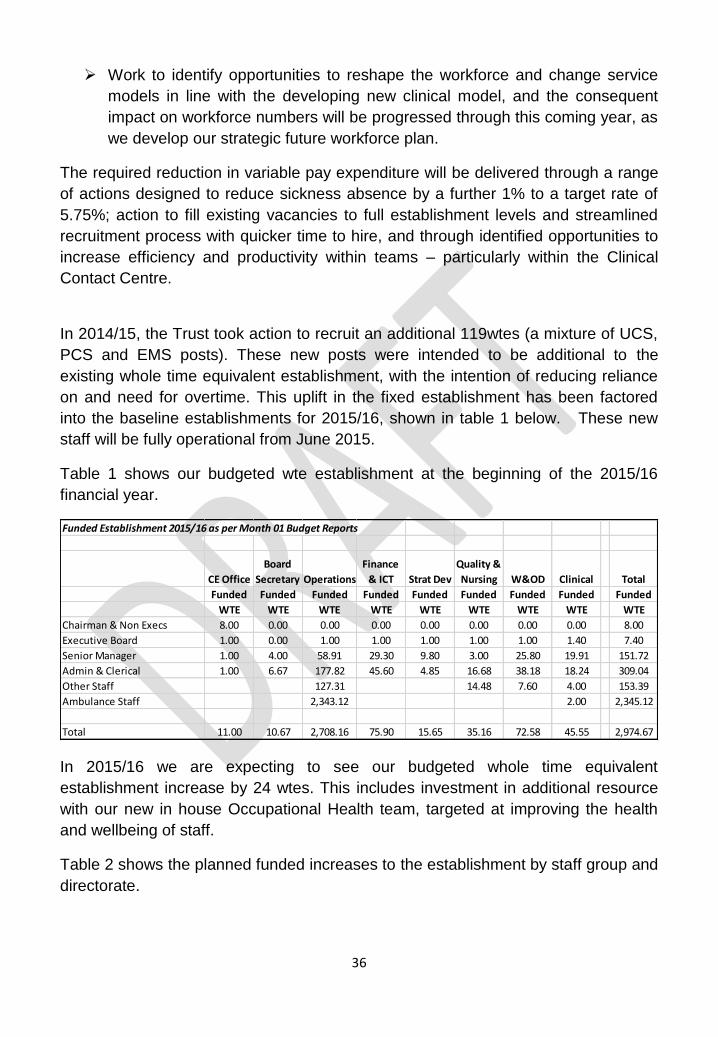
Table 1 shows our budgeted wte establishment at the beginning of the 2015/16
financial year.
In 2015/16 we are expecting to see our budgeted whole time equivalent
establishment increase by 24 wtes. This includes investment in additional resource
with our new in house Occupational Health team, targeted at improving the health
and wellbeing of staff.
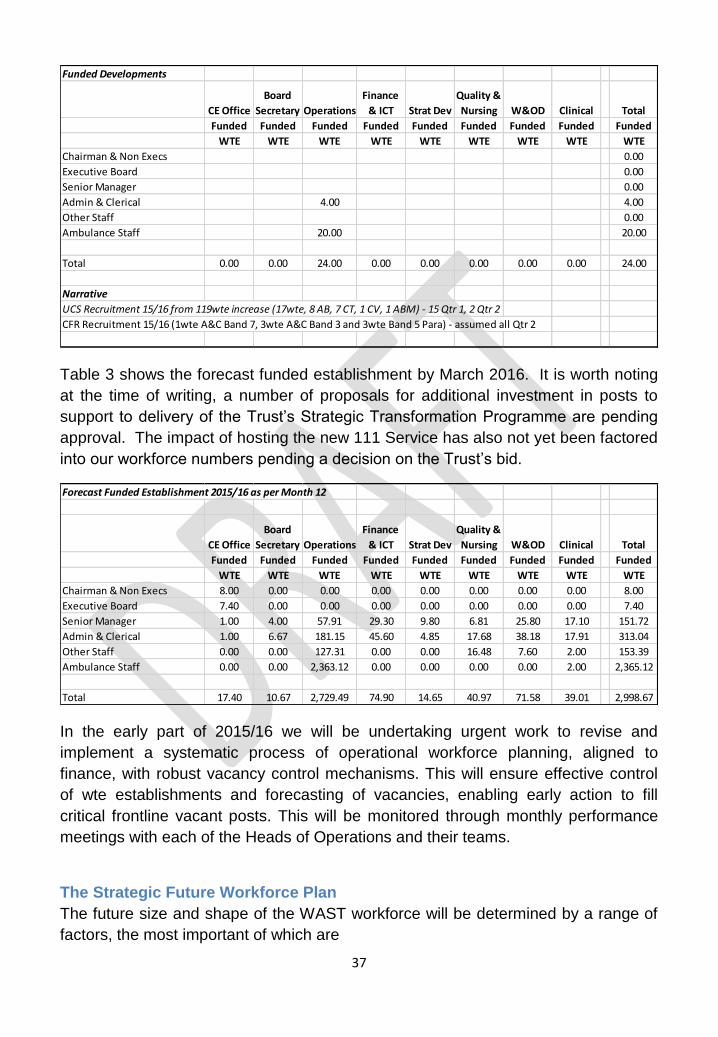
Table 2 shows the planned funded increases to the establishment by staff group and
directorate.
Funded Establishment 2015/16 as per Month 01 Budget Reports
CE Office
Board
Secretary Operations
Finance
& ICT Strat Dev
Quality &
Nursing W&OD Clinical Total
Funded Funded Funded Funded Funded Funded Funded Funded Funded
WTE WTE WTE WTE WTE WTE WTE WTE WTE
Chairman & Non Execs 8.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 8.00
Executive Board 1.00 0.00 1.00 1.00 1.00 1.00 1.00 1.40 7.40
Senior Manager 1.00 4.00 58.91 29.30 9.80 3.00 25.80 19.91 151.72
Admin & Clerical 1.00 6.67 177.82 45.60 4.85 16.68 38.18 18.24 309.04
Other Staff 127.31 14.48 7.60 4.00 153.39
Ambulance Staff 2,343.12 2.00 2,345.12
Total 11.00 10.67 2,708.16 75.90 15.65 35.16 72.58 45.55 2,974.67
37
Table 3 shows the forecast funded establishment by March 2016. It is worth noting
at the time of writing, a number of proposals for additional investment in posts to
support to delivery of the Trust‟s Strategic Transformation Programme are pending
approval. The impact of hosting the new 111 Service has also not yet been factored
into our workforce numbers pending a decision on the Trust‟s bid.
In the early part of 2015/16 we will be undertaking urgent work to revise and
implement a systematic process of operational workforce planning, aligned to
finance, with robust vacancy control mechanisms. This will ensure effective control
of wte establishments and forecasting of vacancies, enabling early action to fill
critical frontline vacant posts. This will be monitored through monthly performance
meetings with each of the Heads of Operations and their teams.
The Strategic Future Workforce Plan
The future size and shape of the WAST workforce will be determined by a range of
factors, the most important of which are
Funded Developments
CE Office
Board
Secretary Operations
Finance
& ICT Strat Dev
Quality &
Nursing W&OD Clinical Total
Funded Funded Funded Funded Funded Funded Funded Funded Funded
WTE WTE WTE WTE WTE WTE WTE WTE WTE
Chairman & Non Execs 0.00
Executive Board 0.00
Senior Manager 0.00
Admin & Clerical 4.00 4.00
Other Staff 0.00
Ambulance Staff 20.00 20.00
Total 0.00 0.00 24.00 0.00 0.00 0.00 0.00 0.00 24.00
Narrative
UCS Recruitment 15/16 from 119wte increase (17wte, 8 AB, 7 CT, 1 CV, 1 ABM) - 15 Qtr 1, 2 Qtr 2
CFR Recruitment 15/16 (1wte A&C Band 7, 3wte A&C Band 3 and 3wte Band 5 Para) - assumed all Qtr 2
Forecast Funded Establishment 2015/16 as per Month 12
CE Office
Board
Secretary Operations
Finance
& ICT Strat Dev
Quality &
Nursing W&OD Clinical Total
Funded Funded Funded Funded Funded Funded Funded Funded Funded
WTE WTE WTE WTE WTE WTE WTE WTE WTE
Chairman & Non Execs 8.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 8.00
Executive Board 7.40 0.00 0.00 0.00 0.00 0.00 0.00 0.00 7.40
Senior Manager 1.00 4.00 57.91 29.30 9.80 6.81 25.80 17.10 151.72
Admin & Clerical 1.00 6.67 181.15 45.60 4.85 17.68 38.18 17.91 313.04
Other Staff 0.00 0.00 127.31 0.00 0.00 16.48 7.60 2.00 153.39
Ambulance Staff 0.00 0.00 2,363.12 0.00 0.00 0.00 0.00 2.00 2,365.12
Total 17.40 10.67 2,729.49 74.90 14.65 40.97 71.58 39.01 2,998.67
38
The new clinical model for emergency ambulance services falling out of the
STP clinical modernisation project
The workforce requirements of the 111 service together with management
arrangements for that service
The outputs of the Strategic Transformation Programme‟s Non-Emergency
Patient Transport Project
Commissioner requirements in respect of EMS/UCS workload and the
affordability of any additional investment required in WAST capacity
The impact of changes in flows and journey times resulting from the South
Wales Programme, The Mid Wales Healthcare Collaboration and the ongoing
review of acute services in Betsi Cadwaladr University LHB
Turnover, age profile and the impact of working longer hours
The move to paramedicine becoming a degree profession with the first intake
to the degree programme in Wales expected to be in 2016.
The Trust has the tools and skills to model the future size and shape of the WAST
workforce. The model can be flexed to accommodate - to a degree - the uncertainty
inherent in the above list of variables. This work will be informed primarily by the new
clinical model, commissioner requirements and the supply of suitable trained staff.
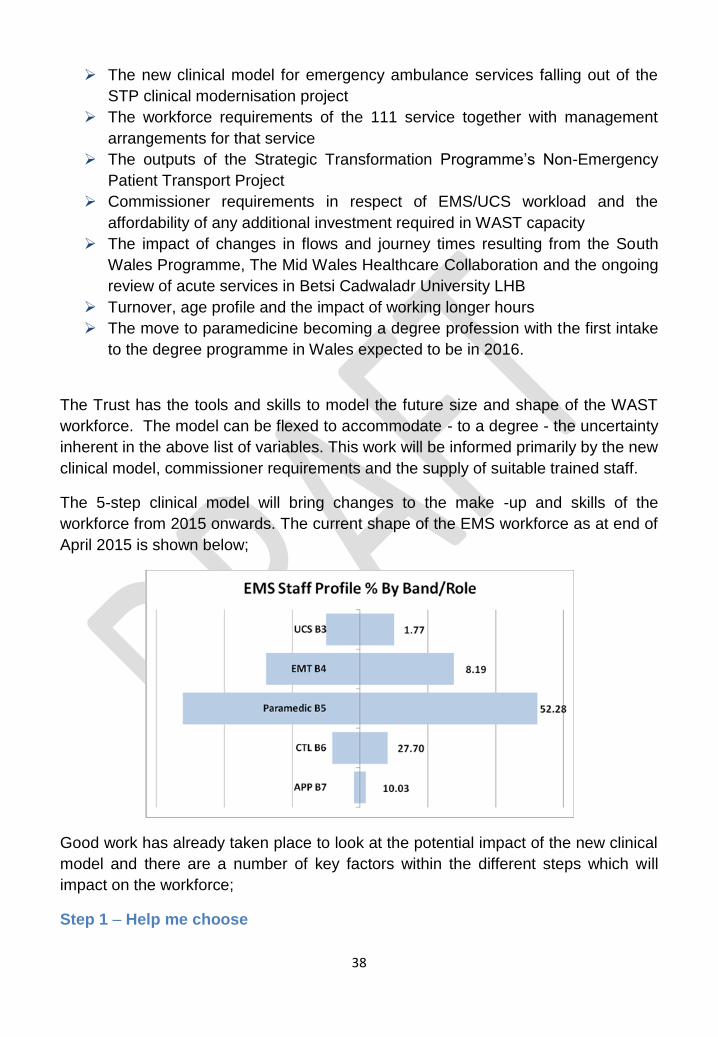
The 5-step clinical model will bring changes to the make -up and skills of the
workforce from 2015 onwards. The current shape of the EMS workforce as at end of
April 2015 is shown below;
Good work has already taken place to look at the potential impact of the new clinical
model and there are a number of key factors within the different steps which will
impact on the workforce;
Step 1 – Help me choose
39
This will require staff to have the necessary skills to be able to educate and inform
the public at every appropriate contact opportunity. It will require strengthening the
management of local Community First responders so they become the local
community experts, particularly in rural areas. The Trust will use the examples of
community champions established by other agencies and not seek to duplicate but
work closely with other partners in those settings.
The web based Directory of Services will be enhanced and there will be an increase
in clinical staff within the Clinical Contact Centres (CCCs) to inform callers on the
correct pathway. The outcome of the decision on the hosting of 111 will inform the
shape of the service going forward and the staffing numbers.
Step 2 – Answer my call
The main workforce impact of this will be within the CCCs as more calls are dealt
with by clinical staff and callers directed to the correct pathway. It is envisages that
this will see an increase in the number of band 6 staff but the final shape of the
workforce will be impacted by the decision on the 111 service and the future
arrangements for the staff currently in NHSDW.
Step 3 – Come and see me
This requires the most appropriate clinician to attend and deal with life threatening
issues or make decisions on the appropriate pathway. It is envisaged that the
requirement to see and treat will require an increase in the numbers of staff qualified
at a higher clinical level; band 8 and 7 advanced skills practitioners, band 6
“specialist” practitioners. There will, over time, be a reduction in the number of band
5 and 4 staff but an increase in band 3 staff who will provide the back-up transport to
clinicians but also to manage the Card 35, Health Care Professional calls. The
numbers of staff in this group will also be determined by the outcome of the non-
emergency patient care review.
Step 4 – Give me treatment
In terms of the current staffing model of the Trust, it is this area which will see the
biggest changes. The intention is that only those patients who need to attend an
Emergency Department will be taken there having been assessed on scene by
skilled clinicians operating within their scope of practice. These staff will be able to
provide disease specific care and make decisions on referral to other services. This
role will predominately be delivered by staff and bands 6 and 7.
Step 5 – Take me to...
This will require suitably competent and trained staff to transport patients who are
deemed by clinicians to require transport, to a hospital or other facility.
40
It is important to stress that the above model will still mean that patients who require
a time critical emergency response will receive that response from the right staff with
the right skills and will be taken to the appropriate centre for care.
Further work is needed through 2015/16 to assess current capability and resource
against anticipated future skill mix and role requirements, aligned to the developing
clinical model and changing population need. This work will also enable us to identify
and plan for future training and professional development needs, and consider the
issue of affordability.
To achieve this we plan to hold a number of scenario planning / workforce planning
events through the year, involving key partners and stakeholders to enable us to
develop our Strategic Future Workforce Plan.
The Trust will be supported in this by the Workforce, Education Development
Service.
The development of the future workforce will also be supported by a series of
technological advances which WAST intends to implement to streamline and
transform processes. These include
The roll out of ESR Manager Self Service & Business Intelligence
The procurement of a single roster system.
Developing an Integrated service, workforce and finance plan
Development of a Strategic Workforce Plan is an integral part of detailed cross
directorate modelling in order to create an integrated service, workforce and finance
plan for the Trust. Delivery of the overall plan will be driven and owned by the
Strategy, Planning and Performance Directorate. An outline timetable for delivery of
this plan is shown below.
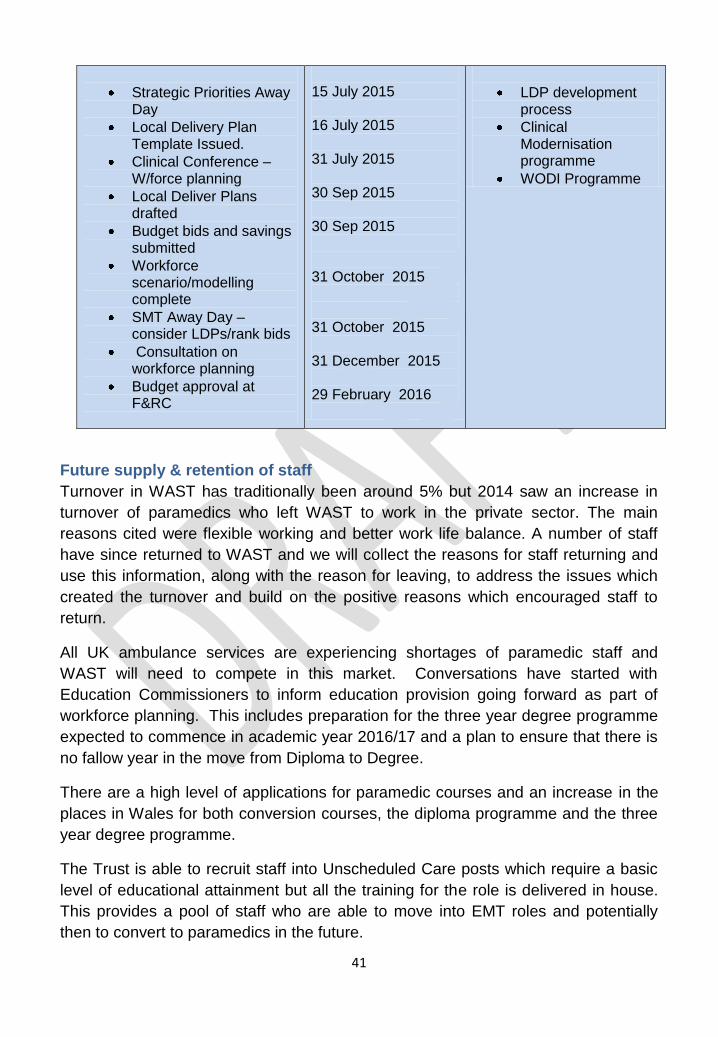
Integrated service, workforce and finance plan
Actions 2015/16 Timescale Interfaces
41
Strategic Priorities Away Day
Local Delivery Plan Template Issued.
Clinical Conference – W/force planning
Local Deliver Plans drafted
Budget bids and savings submitted
Workforce scenario/modelling complete
SMT Away Day – consider LDPs/rank bids
Consultation on workforce planning
Budget approval at F&RC
15 July 2015
16 July 2015
31 July 2015
30 Sep 2015
30 Sep 2015 31 October 2015 31 October 2015 31 December 2015 29 February 2016
LDP development process
Clinical Modernisation programme
WODI Programme
Future supply & retention of staff
Turnover in WAST has traditionally been around 5% but 2014 saw an increase in
turnover of paramedics who left WAST to work in the private sector. The main
reasons cited were flexible working and better work life balance. A number of staff
have since returned to WAST and we will collect the reasons for staff returning and
use this information, along with the reason for leaving, to address the issues which
created the turnover and build on the positive reasons which encouraged staff to
return.
All UK ambulance services are experiencing shortages of paramedic staff and
WAST will need to compete in this market. Conversations have started with
Education Commissioners to inform education provision going forward as part of
workforce planning. This includes preparation for the three year degree programme
expected to commence in academic year 2016/17 and a plan to ensure that there is
no fallow year in the move from Diploma to Degree.
There are a high level of applications for paramedic courses and an increase in the
places in Wales for both conversion courses, the diploma programme and the three
year degree programme.
The Trust is able to recruit staff into Unscheduled Care posts which require a basic
level of educational attainment but all the training for the role is delivered in house.
This provides a pool of staff who are able to move into EMT roles and potentially
then to convert to paramedics in the future.
42
We will continue to advertise to fill existing vacancies through NHS Jobs, using
social media and linking with the military careers services to attract military medical
personnel who may be leaving the armed forces and are interested in working in
WAST. Over the next year, our Recruitment Task & Finish Group will be exploring
opportunities to change the way in which we attract and recruit new staff, looking at
one stop shop bulk recruitment events targeted at students due to complete their
studies, and developing our employee value proposition to ensure we are the
Ambulance Service employer of choice.
Retention of staff is also a key piece of this jigsaw. There is a considerable body of
research evidence and knowledge that supports the link between employee
engagement, motivation and organisational success, with engagement impacting on
key performance indicators such as absenteeism and turnover rates.
Building a highly engaged, responsive and agile workforce will be critical as we enter
a period of unprecedented change and development. Creating a framework for the
engagement and recognition of our people, that is evidence-based and grounded in
research, will be the starting point for developing a programme of activities aimed
specifically at increasing levels of staff engagement. Research shows that a focus
on this agenda will positively impact on patient experience and the delivery of high
quality, safe care for all.
The development of this framework and the collection of staff stories to inform and
shape our future actions and behaviours will be a key output of Project 2 WODI
Programme, aimed at delivering sustainable culture change.
Education and Training
The move to paramedicine becoming a degree profession with the first intake to the
degree programme in Wales in 2016 brings with it a number of issues which the
Trust and its partners will need to work through in 2015/16:
The release of EMTs to convert to paramedics using the one year +
programme
Sufficient hospital and other clinical placements for students
University support for training additional numbers
Sufficient internal resources to support students
Development of a one year programme for diploma/IHCD paramedics to
become degree paramedics
The impact of the banding of newly qualified paramedics from 2019 onwards
(potentially Band 6 rather than the current Band 5).
The Trust currently provides induction and CPD for all clinical and non-clinical staff
in-house through the National Training College based in Swansea which is an IHCD
43
accredited centre. For all other non-medical clinical groups in Wales, all basic and
post basic education (including all CPD) is provided by the HEI sector through
service level agreements with LHBs and Trusts.
Discussions are at a very early stage about the potential transfer of the CPD
provision for registered clinical staff into HEIs with the Trust retaining the training
and development of other clinical groups, CCC staff and managerial staff in house,
working with LHB partners.
It is vital that the CPD programmes for clinical staff reflect the changing nature of
clinical practice for paramedicine and that HEIs are part of that work going forward.
The outcome of the review of Education Commissioning established by the Minister
for Health and Social Services will be an important influence on how the Trust takes
forward its ambition to be a provider of clinical services across Wales and implement
the clinical model. There are a range of different disciplines who work in
communities with some common but many different skills. The Trust will work with
other partners to avoid duplication but there is a need for support to enable easier
transfer of skills across disciplines. At the present time a nurse who wishes to
become a paramedic has to undertake the full two year diploma. The ability to better
transfer and recognise skills within an appropriate governance and regulatory
framework is a key piece of work for the future.
Workforce, Organisation Design and Improvement (WODI) Programme
Underpinning all of the above activity and enabling delivery of the Trust‟s broader
OD strategy and IMTP priorities will be our WODI Programme of work. This
programme will provide the means to ensure pace, discipline and momentum to
delivery of our workforce, OD and improvement objectives.
The programme has been scoped through a process of stakeholder discussion and
review of existing organisational commitments and risks. This is a dynamic and
ongoing process. It identifies an ambitious programme of workforce, organisational
design and improvement activity that distinguishes key business as usual activities,
and focuses delivery on two projects, with a number of workstreams, designed to
underpin delivery of the Year 1 priorities, and those designed to deliver sustainable
organisational and cultural change.
Project 1: „Year 1 Priorities‟ aims to deliver us the following benefits;
a sustainable reduction in sickness absence rates of 1% across the Trust
a streamlined recruitment process and reduced time to hire
44
a refreshed (TU) partnership working infrastructure, and robust, positive
partnership behaviours and relationships across the Trust
completion of the current rostering project, and identification of further
opportunities to increase workforce efficiency and productivity
completion of the “roster centre review“ which represents a legacy piece of
work from the Trusts previous Strategic Transformation Programme.
successful achievement of the Gold Corporate Health Standard
Project 2: focusses on delivering our (expanded) OD strategic objectives, with
multiple, interdependent workstreams (which commence now) aimed at delivering
sustainable organisational and cultural change. Benefits will include:
a refreshed set of agreed values and expected behaviours, and agreed
common principles which represent the WAST „way of doing things.‟
reinforcement of leadership and clinical leadership behaviours
continued development of a „Future Leaders Pathway‟ as a mechanism for
succession planning and talent management,
clear decision making and accountability framework
a stronger team and team working ethos (and skills) across the Trust
a sustainable model and strategy for service improvement
a training needs analysis and plan to ensure a safe, skilled and sustainable
workforce
* Note that Clinical Leadership development will formally sit as part of the Trust‟s
Clinical Modernisation Programme, as will the development of a Strategic Future
Workforce Plan aligned to the new Clinical Model.
Successful delivery of the Programme will be contingent on ensuring all these factors are in place:
The right attitude, determination and will to deliver change
A clear and shared vision for the future
Ensuring projects and plans aligned to organisational strategy
Focus and execution, with the capacity to deliver
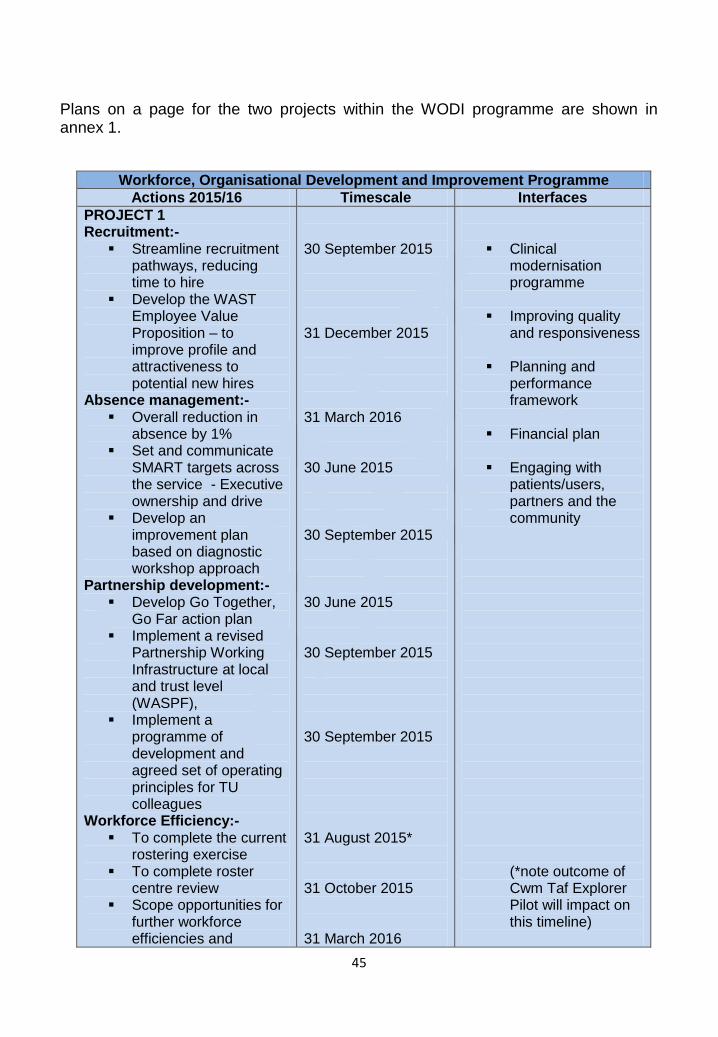
45
Plans on a page for the two projects within the WODI programme are shown in annex 1.
Workforce, Organisational Development and Improvement Programme
Actions 2015/16 Timescale Interfaces
PROJECT 1 Recruitment:-
Streamline recruitment pathways, reducing time to hire
Develop the WAST Employee Value Proposition – to improve profile and attractiveness to potential new hires
Absence management:- Overall reduction in
absence by 1% Set and communicate
SMART targets across the service - Executive ownership and drive
Develop an improvement plan based on diagnostic workshop approach
Partnership development:- Develop Go Together,
Go Far action plan Implement a revised
Partnership Working Infrastructure at local and trust level (WASPF),
Implement a programme of development and agreed set of operating principles for TU colleagues
Workforce Efficiency:- To complete the current
rostering exercise To complete roster
centre review Scope opportunities for
further workforce efficiencies and
30 September 2015
31 December 2015
31 March 2016 30 June 2015
30 September 2015 30 June 2015
30 September 2015
30 September 2015
31 August 2015*
31 October 2015
31 March 2016
Clinical modernisation programme
Improving quality and responsiveness
Planning and performance framework
Financial plan
Engaging with patients/users, partners and the community (*note outcome of Cwm Taf Explorer Pilot will impact on this timeline)
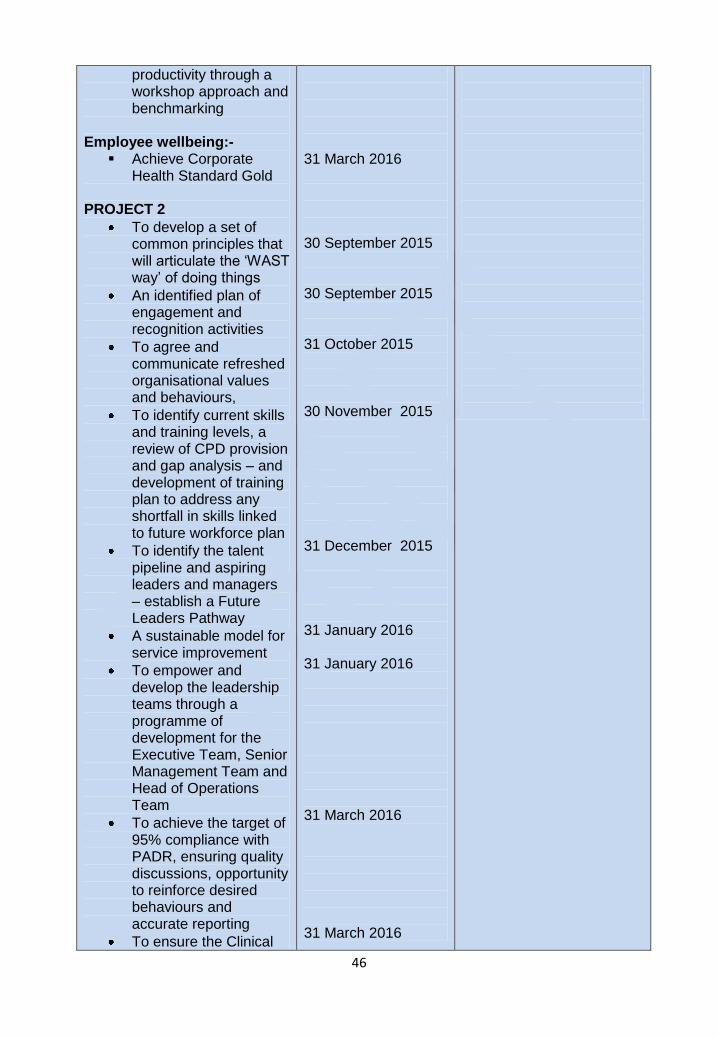
46
productivity through a workshop approach and benchmarking
Employee wellbeing:- Achieve Corporate
Health Standard Gold PROJECT 2
To develop a set of common principles that will articulate the „WAST way‟ of doing things
An identified plan of engagement and recognition activities
To agree and communicate refreshed organisational values and behaviours,
To identify current skills and training levels, a review of CPD provision and gap analysis – and development of training plan to address any shortfall in skills linked to future workforce plan
To identify the talent pipeline and aspiring leaders and managers – establish a Future Leaders Pathway
A sustainable model for service improvement
To empower and develop the leadership teams through a programme of development for the Executive Team, Senior Management Team and Head of Operations Team
To achieve the target of 95% compliance with PADR, ensuring quality discussions, opportunity to reinforce desired behaviours and accurate reporting
To ensure the Clinical
31 March 2016
30 September 2015 30 September 2015 31 October 2015
30 November 2015
31 December 2015
31 January 2016 31 January 2016
31 March 2016
31 March 2016
47
Team Leader role is effective, and supported by a clear development programme
MANAGEMENT OF RESOURCES
The financial outlook for the Welsh Ambulance Service in the financial year 2015/16
is significantly better than in previous years. This is primarily due to the following
three things:
1. The recurrent investment of £7.5m to support the underlying infrastructure of
the Trust; this is predominately the recruitment of additional front line staff
and the introduction of a clinical desk in the Clinical Control Centre. This
funding is being used alongside reductions in overtime, reductions in
sickness and better alignment of rotas;
2. The investment of a further £8m (see below for details);
3. Knowing the level of income at the start of the financial year.
There are, however, risks associated with the ability to continue to improve
performance against the 65% target and breakeven financially. Improvement
initiatives in place at the start of the financial year are not affordable within the
current financial envelope for a sustained period of time. This includes, but is not
limited to, the additional resources being used to support the „Explorer Project‟ in
Cwm Taf, continued use of private providers to increase capacity and paying double
time for overtime worked by frontline EMS staff.
Income assumptions for 2015/16
The Trust Board has approved the budget set for 2015/16 as per the income detailed on the table below. This reconciles with the income schedule (RE4) contained within the National Collaborative Commissioning: Quality & Delivery Framework Agreement. It should, however, be noted that not all of the income received by the Trust and included in the table below comes via the Emergency Ambulance Service Committee (EASC). The key income assumptions for 2015/16 are as follows:
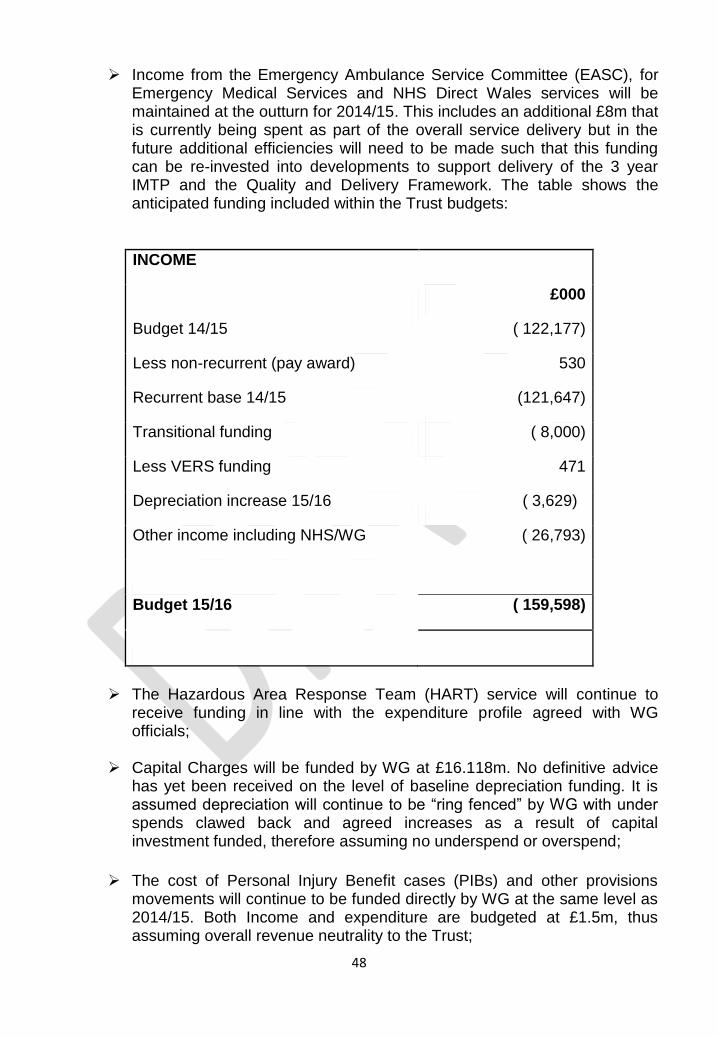
48
Income from the Emergency Ambulance Service Committee (EASC), for Emergency Medical Services and NHS Direct Wales services will be maintained at the outturn for 2014/15. This includes an additional £8m that is currently being spent as part of the overall service delivery but in the future additional efficiencies will need to be made such that this funding can be re-invested into developments to support delivery of the 3 year IMTP and the Quality and Delivery Framework. The table shows the anticipated funding included within the Trust budgets:
INCOME
£000
Budget 14/15 ( 122,177)
Less non-recurrent (pay award) 530
Recurrent base 14/15 (121,647)
Transitional funding ( 8,000)
Less VERS funding 471
Depreciation increase 15/16 ( 3,629)
Other income including NHS/WG ( 26,793)
Budget 15/16 ( 159,598)
The Hazardous Area Response Team (HART) service will continue to
receive funding in line with the expenditure profile agreed with WG officials;
Capital Charges will be funded by WG at £16.118m. No definitive advice has yet been received on the level of baseline depreciation funding. It is assumed depreciation will continue to be “ring fenced” by WG with under spends clawed back and agreed increases as a result of capital investment funded, therefore assuming no underspend or overspend;
The cost of Personal Injury Benefit cases (PIBs) and other provisions movements will continue to be funded directly by WG at the same level as 2014/15. Both Income and expenditure are budgeted at £1.5m, thus assuming overall revenue neutrality to the Trust;
49
Capital funding will be in line with the indicative expenditure plans submitted to WG with any consequential in-year increase in depreciation also being funded;
The cash allocation settlement from other Welsh Health Partners, including LHBs, will be at the same level as last financial year i.e. flat cash with adjustments only for agreed activity variances;
Income and costs for the Non-Emergency Patient Transport Service (PCS) has been included at historic rates;
Following discussions, HCS was transferred to NWSSP as of 1st April 2015; as such, the income and expenses valued at £4.62m will be transferred over to Shared Services. The terms of the transfer assumes no net financial impact to WAST;
It is assumed that WAST will continue to receive the same level of service provided by HCS in 2014/15 at no additional cost and HCS will continue to receive the same access to WAST facilities and support at 14/15 baseline levels at no additional cost other than where a transfer of relevant identifiable HCS overheads to NWSSP has been agreed enabling costs to be recharged.
Using a zero based budgeting approach, Directorate Accountants have worked with their Directorate Managers to produce budgets for the 2015/16 financial year within the framework of the Trust‟s overall anticipated resource envelope. Detailed proposals were presented at the Finance and Resources Committee (FRC) for full scrutiny on April 21, 2015 and commended for Board approval. The Trust Board subsequently approved the full, detailed proposed budget on 8th May 2015 having previously approved a very high level summary budget at the end of March 2015.
Revenue 2015/16
The Trust is required to set expenditure budgets within the total resource income available i.e. achieve financial balance in line with the Trust‟s statutory break even duty as set out in WG circular WHC (2007) 049. The revised 2015/16 financial plan delivers a forecast breakeven position; however, this assumes that the full 3% savings will be achieved. Below is a table which shows the current forecast position.
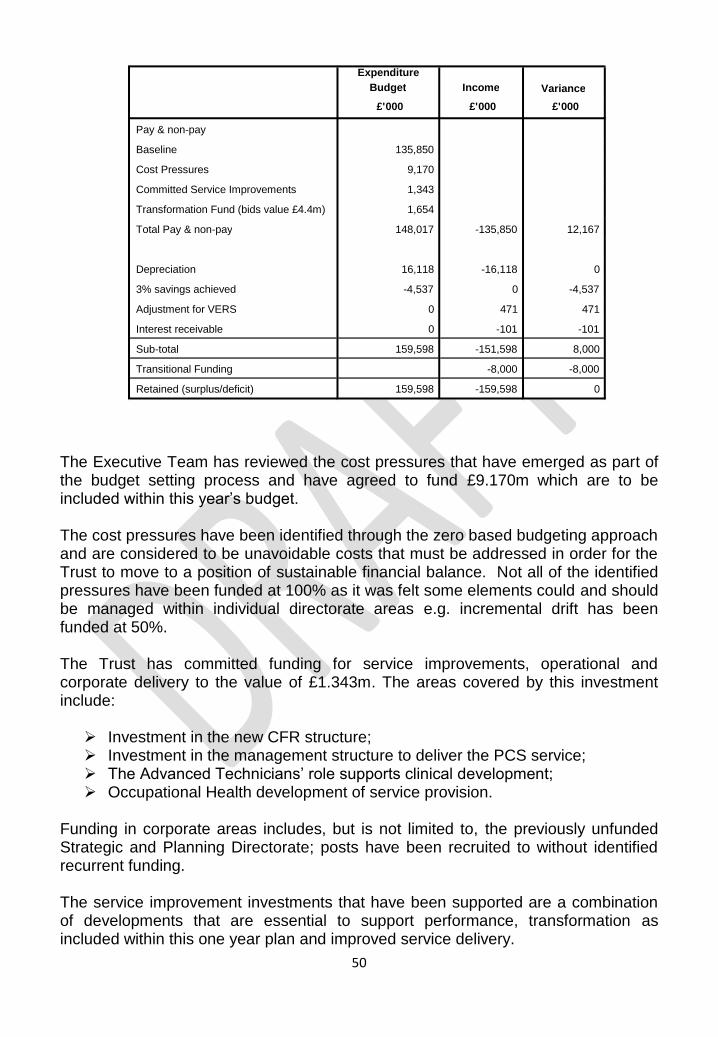
50
The Executive Team has reviewed the cost pressures that have emerged as part of the budget setting process and have agreed to fund £9.170m which are to be included within this year‟s budget. The cost pressures have been identified through the zero based budgeting approach and are considered to be unavoidable costs that must be addressed in order for the Trust to move to a position of sustainable financial balance. Not all of the identified pressures have been funded at 100% as it was felt some elements could and should be managed within individual directorate areas e.g. incremental drift has been funded at 50%. The Trust has committed funding for service improvements, operational and corporate delivery to the value of £1.343m. The areas covered by this investment include: Investment in the new CFR structure; Investment in the management structure to deliver the PCS service; The Advanced Technicians‟ role supports clinical development; Occupational Health development of service provision.
Funding in corporate areas includes, but is not limited to, the previously unfunded Strategic and Planning Directorate; posts have been recruited to without identified recurrent funding. The service improvement investments that have been supported are a combination of developments that are essential to support performance, transformation as included within this one year plan and improved service delivery.
Expenditure Budget Income Variance £ ' 000 £ ' 000 £ ' 000
Pay & non-pay
Baseline 135,850
Cost Pressures 9,170
Committed Service Improvements 1,343
Transformation Fund (bids value £4.4m) 1,654
Total Pay & non-pay 148,017 -135,850 12,167
Depreciation 16,118 -16,118 0
3% savings achieved -4,537 0 -4,537
Adjustment for VERS 0 471 471
Interest receivable 0 -101 -101
Sub-total 159,598 -151,598 8,000
Transitional Funding -8,000 -8,000
Retained (surplus/deficit) 159,598 -159,598 0
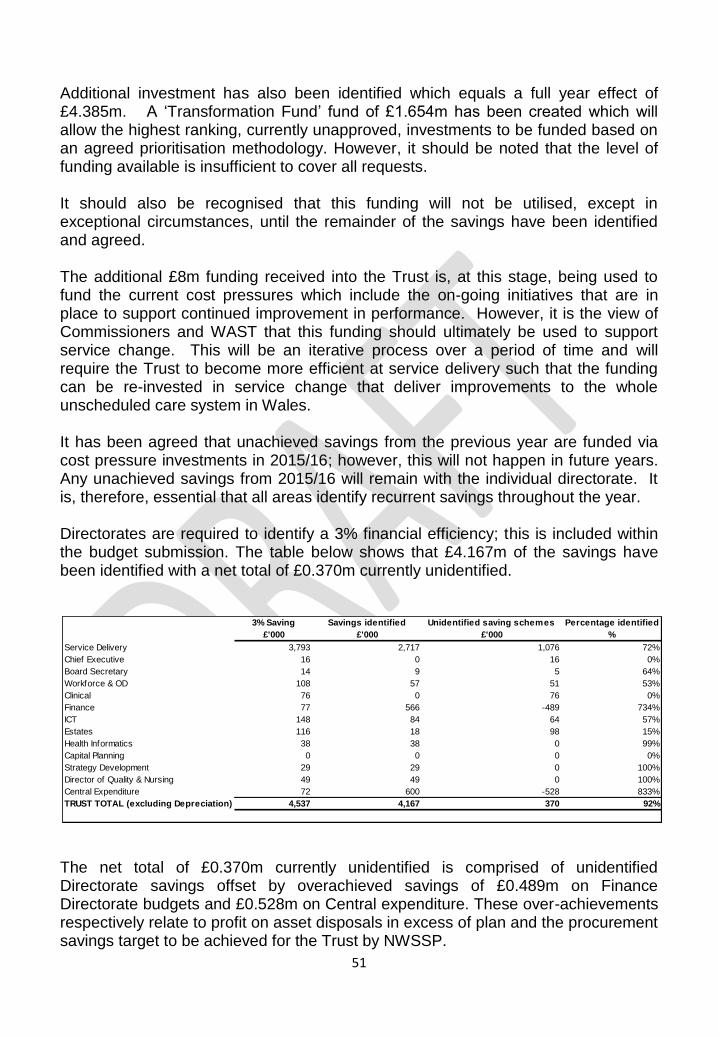
51
Additional investment has also been identified which equals a full year effect of £4.385m. A „Transformation Fund‟ fund of £1.654m has been created which will allow the highest ranking, currently unapproved, investments to be funded based on an agreed prioritisation methodology. However, it should be noted that the level of funding available is insufficient to cover all requests. It should also be recognised that this funding will not be utilised, except in exceptional circumstances, until the remainder of the savings have been identified and agreed. The additional £8m funding received into the Trust is, at this stage, being used to fund the current cost pressures which include the on-going initiatives that are in place to support continued improvement in performance. However, it is the view of Commissioners and WAST that this funding should ultimately be used to support service change. This will be an iterative process over a period of time and will require the Trust to become more efficient at service delivery such that the funding can be re-invested in service change that deliver improvements to the whole unscheduled care system in Wales. It has been agreed that unachieved savings from the previous year are funded via cost pressure investments in 2015/16; however, this will not happen in future years. Any unachieved savings from 2015/16 will remain with the individual directorate. It is, therefore, essential that all areas identify recurrent savings throughout the year. Directorates are required to identify a 3% financial efficiency; this is included within the budget submission. The table below shows that £4.167m of the savings have been identified with a net total of £0.370m currently unidentified.
The net total of £0.370m currently unidentified is comprised of unidentified Directorate savings offset by overachieved savings of £0.489m on Finance Directorate budgets and £0.528m on Central expenditure. These over-achievements respectively relate to profit on asset disposals in excess of plan and the procurement savings target to be achieved for the Trust by NWSSP.
3% Saving Savings identified Unidentified saving schemes Percentage identified
£'000 £'000 £'000 %
Service Delivery 3,793 2,717 1,076 72%
Chief Executive 16 0 16 0%
Board Secretary 14 9 5 64%
Workforce & OD 108 57 51 53%
Clinical 76 0 76 0%
Finance 77 566 -489 734%
ICT 148 84 64 57%
Estates 116 18 98 15%
Health Informatics 38 38 0 99%
Capital Planning 0 0 0 0%
Strategy Development 29 29 0 100%
Director of Quality & Nursing 49 49 0 100%
Central Expenditure 72 600 -528 833%
TRUST TOTAL (excluding Depreciation) 4,537 4,167 370 92%
52
A planned saving of £0.5m on Clinical Contact Centre -led modernisation of operational services is currently being taken forward by the Head of Operations with timescales for achievement yet to be finally confirmed. All savings schemes have been developed by Directorate teams in conjunction with finance managers. There is a phasing plan for each scheme and this will be monitored through the monthly performance management meetings. Given the Directorate of Operations consumes the majority of the resources, it follows that the largest element of the savings requirements falls in that area. A significant facet of the plan is delivered through a reduction in the cost of sickness. The savings target has been calculated at an individual health board area level using the average cost of sickness in 2014/15 as a baseline. Where areas are currently below the national level required, no additional target has been applied. The reduction in cost of sickness equates to a c.2% reduction; this is a stretch target but takes into account that many areas have reached the 1% target as at 31 March 2015. This is thought to be as a result of the new National terms and conditions that have removed the unsocial hours uplift from sickness payments. An investment of £133k in the Occupational Team has been supported to enable delivery of the Trust wide sickness reduction plan.
Financial Plans 2015/16 to 2017/18
The table below provides an overview of the estimated financial outturn position for
each of the following three years; this assumes the additional £8m is funded
recurrently.
As can be seen from the table, given the assumptions made, the Trust is forecasting
a balanced financial position for all three years of the plan. This is based on the
assumption that WAST will deliver recurrent savings of 3% over each of the years;
the savings plans are not yet fully developed but will cover the following areas:
Sustainable savings linked to reduced sickness levels;
Sustainable savings and improved operational effectiveness following the
implementation of the rota review;
Longer term savings in relation to work currently underway to rationalise the
estate;
Corporate and support services efficiencies.
In order to balance the financial plan on a recurrent and sustainable basis, there will
need to be agreements in place to cover the additional cost of the added capacity as
described at the start of this section.
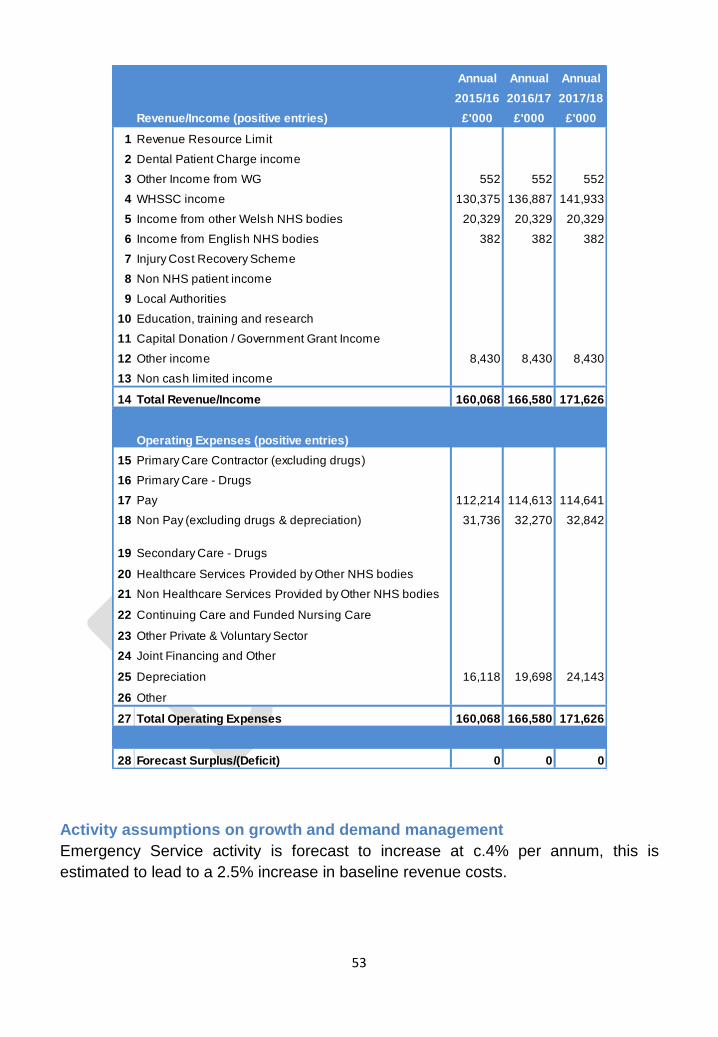
53
Activity assumptions on growth and demand management
Emergency Service activity is forecast to increase at c.4% per annum, this is
estimated to lead to a 2.5% increase in baseline revenue costs.
Annual Annual Annual
2015/16 2016/17 2017/18
Revenue/Income (positive entries) £'000 £'000 £'000
1 Revenue Resource Limit
2 Dental Patient Charge income
3 Other Income from WG 552 552 552
4 WHSSC income 130,375 136,887 141,933
5 Income from other Welsh NHS bodies 20,329 20,329 20,329
6 Income from English NHS bodies 382 382 382
7 Injury Cost Recovery Scheme
8 Non NHS patient income
9 Local Authorities
10 Education, training and research
11 Capital Donation / Government Grant Income
12 Other income 8,430 8,430 8,430
13 Non cash limited income
14 Total Revenue/Income 160,068 166,580 171,626
Operating Expenses (positive entries)
15 Primary Care Contractor (excluding drugs)
16 Primary Care - Drugs
17 Pay 112,214 114,613 114,641
18 Non Pay (excluding drugs & depreciation) 31,736 32,270 32,842
19 Secondary Care - Drugs
20 Healthcare Services Provided by Other NHS bodies
21 Non Healthcare Services Provided by Other NHS bodies
22 Continuing Care and Funded Nursing Care
23 Other Private & Voluntary Sector
24 Joint Financing and Other
25 Depreciation 16,118 19,698 24,143
26 Other
27 Total Operating Expenses 160,068 166,580 171,626
28 Forecast Surplus/(Deficit) 0 0 0
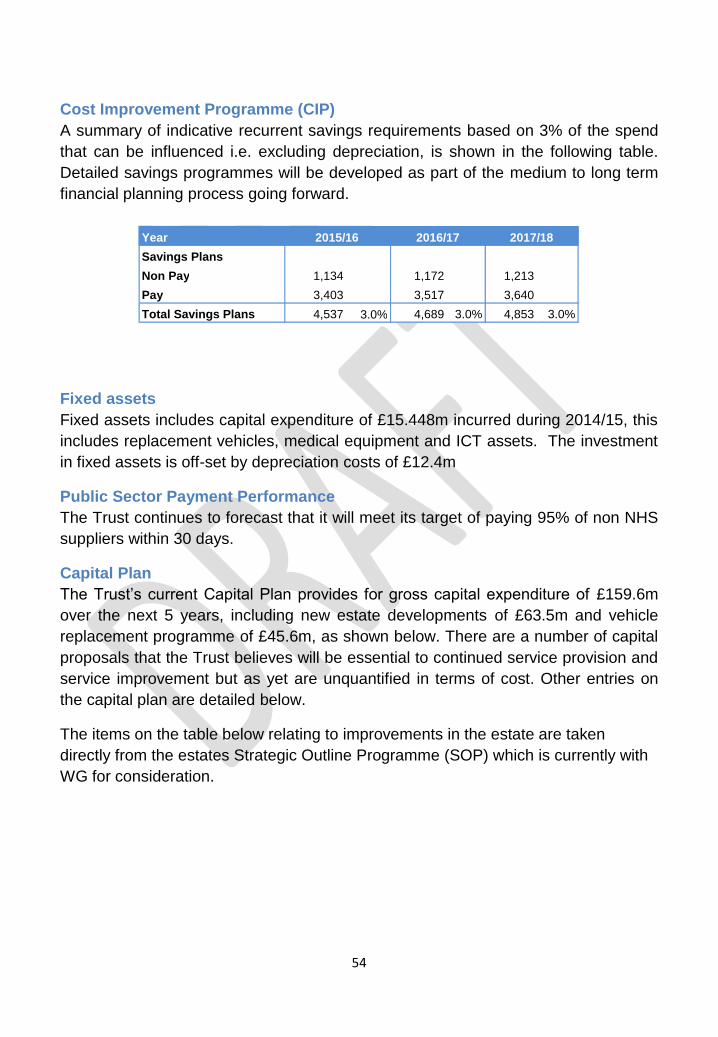
54
Cost Improvement Programme (CIP)
A summary of indicative recurrent savings requirements based on 3% of the spend
that can be influenced i.e. excluding depreciation, is shown in the following table.
Detailed savings programmes will be developed as part of the medium to long term
financial planning process going forward.
Fixed assets
Fixed assets includes capital expenditure of £15.448m incurred during 2014/15, this
includes replacement vehicles, medical equipment and ICT assets. The investment
in fixed assets is off-set by depreciation costs of £12.4m
Public Sector Payment Performance
The Trust continues to forecast that it will meet its target of paying 95% of non NHS
suppliers within 30 days.
Capital Plan
The Trust‟s current Capital Plan provides for gross capital expenditure of £159.6m
over the next 5 years, including new estate developments of £63.5m and vehicle
replacement programme of £45.6m, as shown below. There are a number of capital
proposals that the Trust believes will be essential to continued service provision and
service improvement but as yet are unquantified in terms of cost. Other entries on
the capital plan are detailed below.
The items on the table below relating to improvements in the estate are taken
directly from the estates Strategic Outline Programme (SOP) which is currently with
WG for consideration.
Year
Savings Plans
Non Pay 1,134 1,172 1,213
Pay 3,403 3,517 3,640
Total Savings Plans 4,537 3.0%
4,689 3.0% 4,853 3.0%
2015/16 2016/17 2017/18
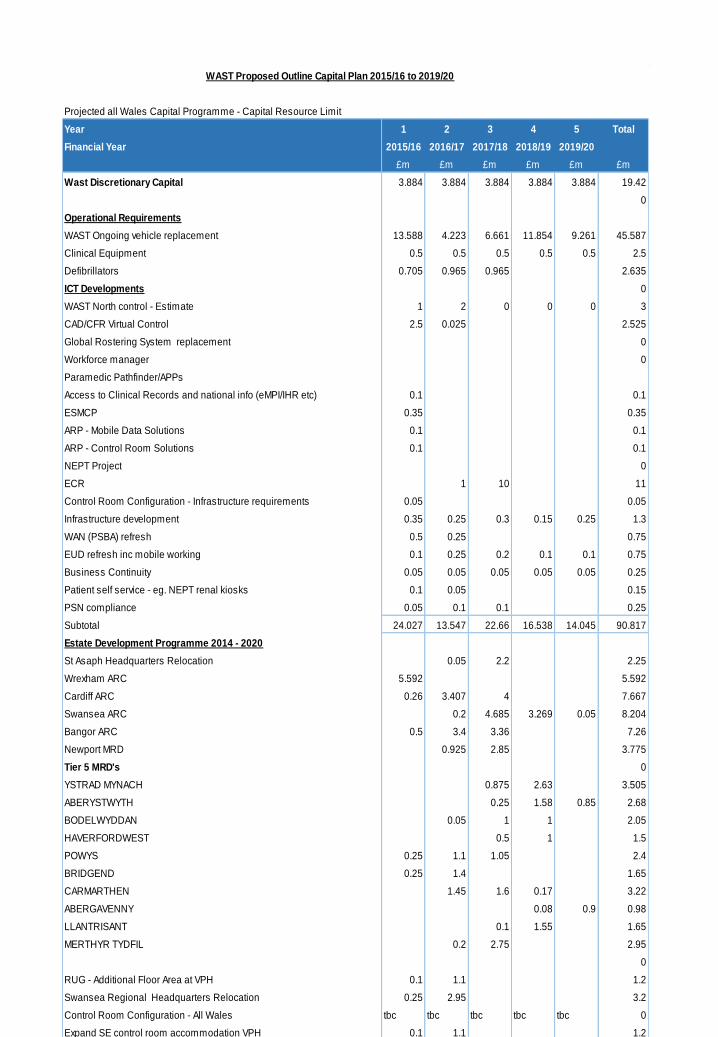
55
Projected all Wales Capital Programme - Capital Resource Limit
Year 1 2 3 4 5 Total
Financial Year 2015/16 2016/17 2017/18 2018/19 2019/20
£m £m £m £m £m £m
Wast Discretionary Capital 3.884 3.884 3.884 3.884 3.884 19.42
0
Operational Requirements
WAST Ongoing vehicle replacement 13.588 4.223 6.661 11.854 9.261 45.587
Clinical Equipment 0.5 0.5 0.5 0.5 0.5 2.5
Defibrillators 0.705 0.965 0.965 2.635
ICT Developments 0
WAST North control - Estimate 1 2 0 0 0 3
CAD/CFR Virtual Control 2.5 0.025 2.525
Global Rostering System replacement 0
Workforce manager 0
Paramedic Pathfinder/APPs
Access to Clinical Records and national info (eMPI/IHR etc) 0.1 0.1
ESMCP 0.35 0.35
ARP - Mobile Data Solutions 0.1 0.1
ARP - Control Room Solutions 0.1 0.1
NEPT Project 0
ECR 1 10 11
Control Room Configuration - Infrastructure requirements 0.05 0.05
Infrastructure development 0.35 0.25 0.3 0.15 0.25 1.3
WAN (PSBA) refresh 0.5 0.25 0.75
EUD refresh inc mobile working 0.1 0.25 0.2 0.1 0.1 0.75
Business Continuity 0.05 0.05 0.05 0.05 0.05 0.25
Patient self service - eg. NEPT renal kiosks 0.1 0.05 0.15
PSN compliance 0.05 0.1 0.1 0.25
Subtotal 24.027 13.547 22.66 16.538 14.045 90.817
Estate Development Programme 2014 - 2020
St Asaph Headquarters Relocation 0.05 2.2 2.25
Wrexham ARC 5.592 5.592
Cardiff ARC 0.26 3.407 4 7.667
Swansea ARC 0.2 4.685 3.269 0.05 8.204
Bangor ARC 0.5 3.4 3.36 7.26
Newport MRD 0.925 2.85 3.775
Tier 5 MRD's 0
YSTRAD MYNACH 0.875 2.63 3.505
ABERYSTWYTH 0.25 1.58 0.85 2.68
BODELWYDDAN 0.05 1 1 2.05
HAVERFORDWEST 0.5 1 1.5
POWYS 0.25 1.1 1.05 2.4
BRIDGEND 0.25 1.4 1.65
CARMARTHEN 1.45 1.6 0.17 3.22
ABERGAVENNY 0.08 0.9 0.98
LLANTRISANT 0.1 1.55 1.65
MERTHYR TYDFIL 0.2 2.75 2.95
0
RUG - Additional Floor Area at VPH 0.1 1.1 1.2
Swansea Regional Headquarters Relocation 0.25 2.95 3.2
Control Room Configuration - All Wales tbc tbc tbc tbc tbc 0
Expand SE control room accommodation VPH 0.1 1.1 1.2
SDP'S - Social Deployment Points 0.112 0.112 0.112 0.112 0.112 0.56
Other points of presence tbc tbc tbc tbc tbc 0
Estate Dev.Prog.Total 7.414 17.444 25.332 11.391 1.912 63.493
Capital Receipts 0.185 0.324 0.964 0.976 2.826 5.275
Overall Capital Programme 31.626 31.315 48.956 28.905 18.783 159.585
WAST Proposed Outline Capital Plan 2015/16 to 2019/20
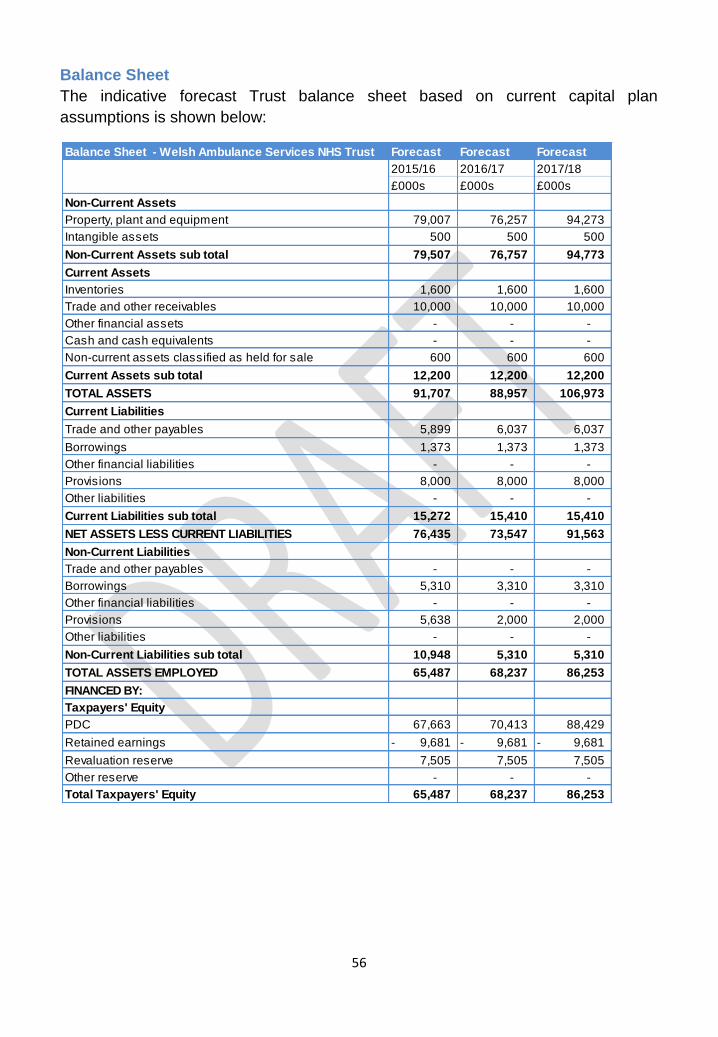
56
Balance Sheet
The indicative forecast Trust balance sheet based on current capital plan
assumptions is shown below:
Balance Sheet - Welsh Ambulance Services NHS Trust Forecast Forecast Forecast
2015/16 2016/17 2017/18
£000s £000s £000s
Non-Current Assets
Property, plant and equipment 79,007 76,257 94,273
Intangible assets 500 500 500
Non-Current Assets sub total 79,507 76,757 94,773
Current Assets
Inventories 1,600 1,600 1,600
Trade and other receivables 10,000 10,000 10,000
Other financial assets - - -
Cash and cash equivalents - - -
Non-current assets classified as held for sale 600 600 600
Current Assets sub total 12,200 12,200 12,200
TOTAL ASSETS 91,707 88,957 106,973
Current Liabilities
Trade and other payables 5,899 6,037 6,037
Borrowings 1,373 1,373 1,373
Other financial liabilities - - -
Provisions 8,000 8,000 8,000
Other liabilities - - -
Current Liabilities sub total 15,272 15,410 15,410
NET ASSETS LESS CURRENT LIABILITIES 76,435 73,547 91,563
Non-Current Liabilities
Trade and other payables - - -
Borrowings 5,310 3,310 3,310
Other financial liabilities - - -
Provisions 5,638 2,000 2,000
Other liabilities - - -
Non-Current Liabilities sub total 10,948 5,310 5,310
TOTAL ASSETS EMPLOYED 65,487 68,237 86,253
FINANCED BY:
Taxpayers' Equity
PDC 67,663 70,413 88,429
Retained earnings 9,681- 9,681- 9,681-
Revaluation reserve 7,505 7,505 7,505
Other reserve - - -
Total Taxpayers' Equity 65,487 68,237 86,253
57
ENABLING STRATEGIES
Estates strategy
The Trust operates from 113 buildings across Wales (either owned or leased). This
total includes 2 Area Ambulance Centres, 6 Control Centres, 75 ambulance stations,
4 fleet workshops, 17 social deployment points and 7 administration centres.
The National Estates Strategy
Currently, the Trust continues to implement its ten year National Estates Strategy.
For the period 2015/16-2017/18, the focus of the strategy remains:
Maintaining the Trust‟s estate to the statutory minimum standard, recognising
that most of the 113 buildings owned/operated by the Trust are operationally
outdated, attract significant backlog maintenance and require rationalisation
through the Estate Strategy
Completion of the following major projects
o Ambulance & Fire Services Resource Centre (AFSRC) Wrexham
o Relocation of Headquarters (North)
o Review and ensure appropriate numbers of Clinical Contact Centres
and Points of Presence across Wales
o ISO 14001 accreditation for Trust ( 2016)
Development of proposals for
o Ambulance Resource Centre (ARC) Cardiff
o ARC Bangor
o ARC Swansea
Development of outline proposals for Make Ready Depots.
The outline proposals for the further development of Make Ready Depots will seek to
maximise the benefits of the concept:
Improved operational performance
Improvements in vehicle cleaning processes, stocking and washing.
Estate rationalisation –operational estate which is fit for purpose and in the
right location
Enhanced Status Plan Management - centralisation of staff rosters.
Improve synergy with other services – collocation and collaboration for
Social Deployment Points
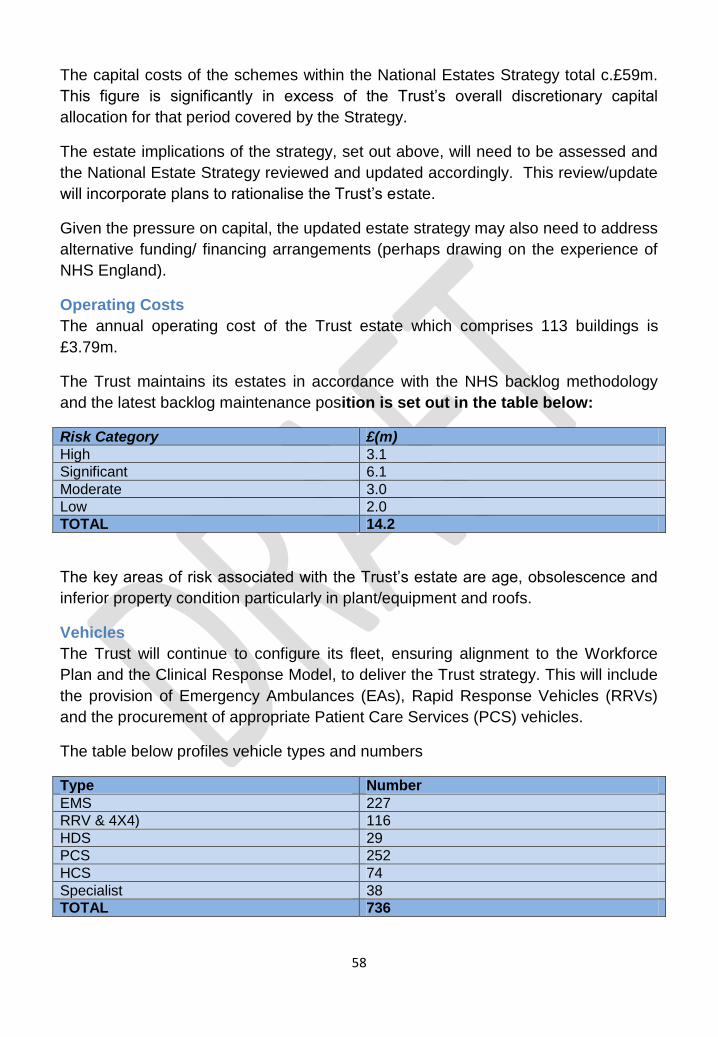
58
The capital costs of the schemes within the National Estates Strategy total c.£59m.
This figure is significantly in excess of the Trust‟s overall discretionary capital
allocation for that period covered by the Strategy.
The estate implications of the strategy, set out above, will need to be assessed and
the National Estate Strategy reviewed and updated accordingly. This review/update
will incorporate plans to rationalise the Trust‟s estate.
Given the pressure on capital, the updated estate strategy may also need to address
alternative funding/ financing arrangements (perhaps drawing on the experience of
NHS England).
Operating Costs
The annual operating cost of the Trust estate which comprises 113 buildings is
£3.79m.
The Trust maintains its estates in accordance with the NHS backlog methodology
and the latest backlog maintenance position is set out in the table below:
Risk Category £(m)
High 3.1
Significant 6.1
Moderate 3.0
Low 2.0
TOTAL 14.2
The key areas of risk associated with the Trust‟s estate are age, obsolescence and
inferior property condition particularly in plant/equipment and roofs.
Vehicles
The Trust will continue to configure its fleet, ensuring alignment to the Workforce
Plan and the Clinical Response Model, to deliver the Trust strategy. This will include
the provision of Emergency Ambulances (EAs), Rapid Response Vehicles (RRVs)
and the procurement of appropriate Patient Care Services (PCS) vehicles.
The table below profiles vehicle types and numbers
Type Number
EMS 227
RRV & 4X4) 116
HDS 29
PCS 252
HCS 74
Specialist 38
TOTAL 736
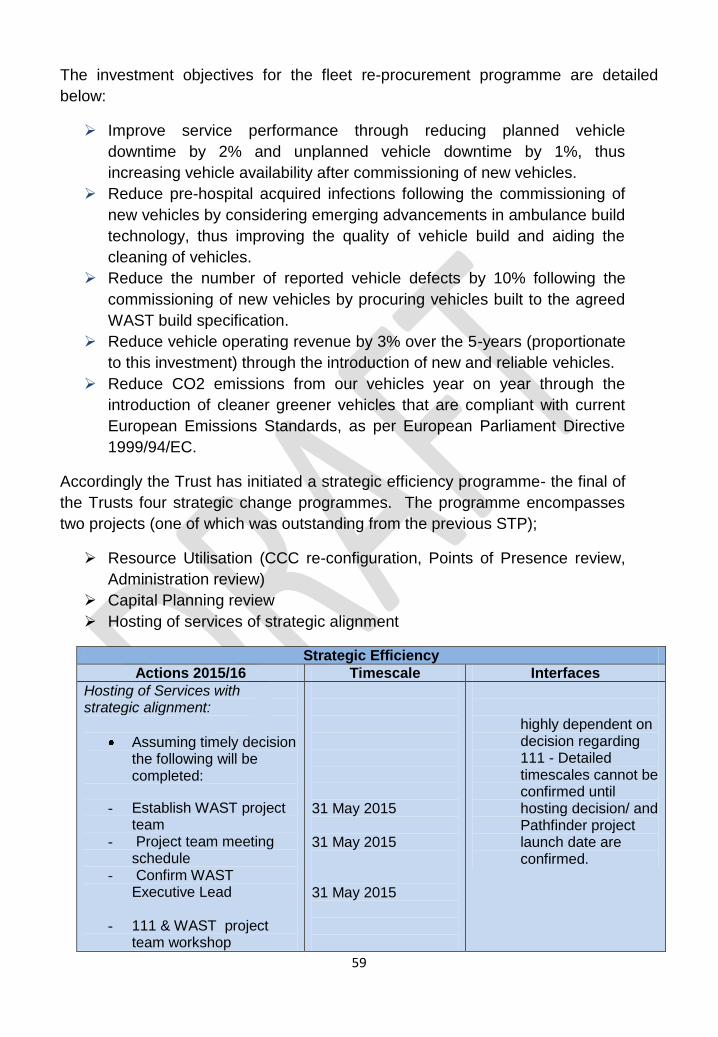
59
The investment objectives for the fleet re-procurement programme are detailed
below:
Improve service performance through reducing planned vehicle
downtime by 2% and unplanned vehicle downtime by 1%, thus
increasing vehicle availability after commissioning of new vehicles.
Reduce pre-hospital acquired infections following the commissioning of
new vehicles by considering emerging advancements in ambulance build
technology, thus improving the quality of vehicle build and aiding the
cleaning of vehicles.
Reduce the number of reported vehicle defects by 10% following the
commissioning of new vehicles by procuring vehicles built to the agreed
WAST build specification.
Reduce vehicle operating revenue by 3% over the 5-years (proportionate
to this investment) through the introduction of new and reliable vehicles.
Reduce CO2 emissions from our vehicles year on year through the
introduction of cleaner greener vehicles that are compliant with current
European Emissions Standards, as per European Parliament Directive
1999/94/EC.
Accordingly the Trust has initiated a strategic efficiency programme- the final of
the Trusts four strategic change programmes. The programme encompasses
two projects (one of which was outstanding from the previous STP);
Resource Utilisation (CCC re-configuration, Points of Presence review,
Administration review)
Capital Planning review
Hosting of services of strategic alignment
Strategic Efficiency
Actions 2015/16 Timescale Interfaces
Hosting of Services with strategic alignment:
Assuming timely decision the following will be completed:
- Establish WAST project team
- Project team meeting schedule
- Confirm WAST Executive Lead
- 111 & WAST project team workshop
31 May 2015 31 May 2015
31 May 2015
highly dependent on decision regarding 111 - Detailed timescales cannot be confirmed until hosting decision/ and Pathfinder project launch date are confirmed.
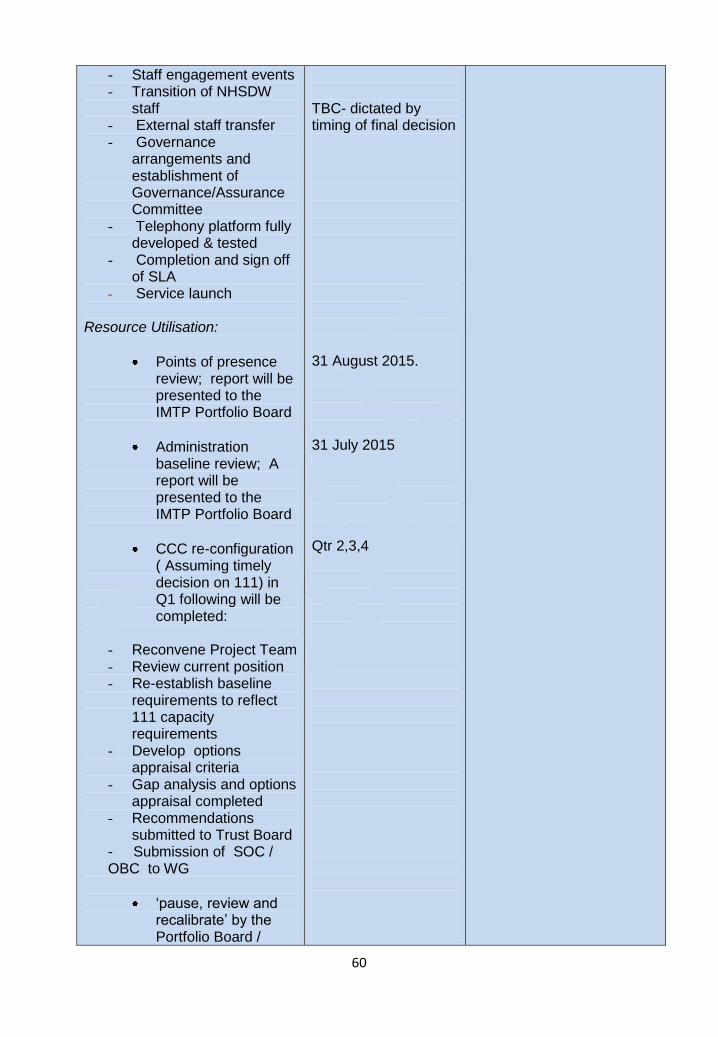
60
- Staff engagement events - Transition of NHSDW
staff - External staff transfer - Governance
arrangements and establishment of Governance/Assurance Committee
- Telephony platform fully developed & tested
- Completion and sign off of SLA
- Service launch
Resource Utilisation:
Points of presence review; report will be presented to the IMTP Portfolio Board
Administration baseline review; A report will be presented to the IMTP Portfolio Board
CCC re-configuration ( Assuming timely decision on 111) in Q1 following will be completed:
- Reconvene Project Team - Review current position - Re-establish baseline
requirements to reflect 111 capacity requirements
- Develop options appraisal criteria
- Gap analysis and options appraisal completed
- Recommendations submitted to Trust Board
- Submission of SOC / OBC to WG
„pause, review and recalibrate‟ by the Portfolio Board /
TBC- dictated by timing of final decision
31 August 2015. 31 July 2015 Qtr 2,3,4
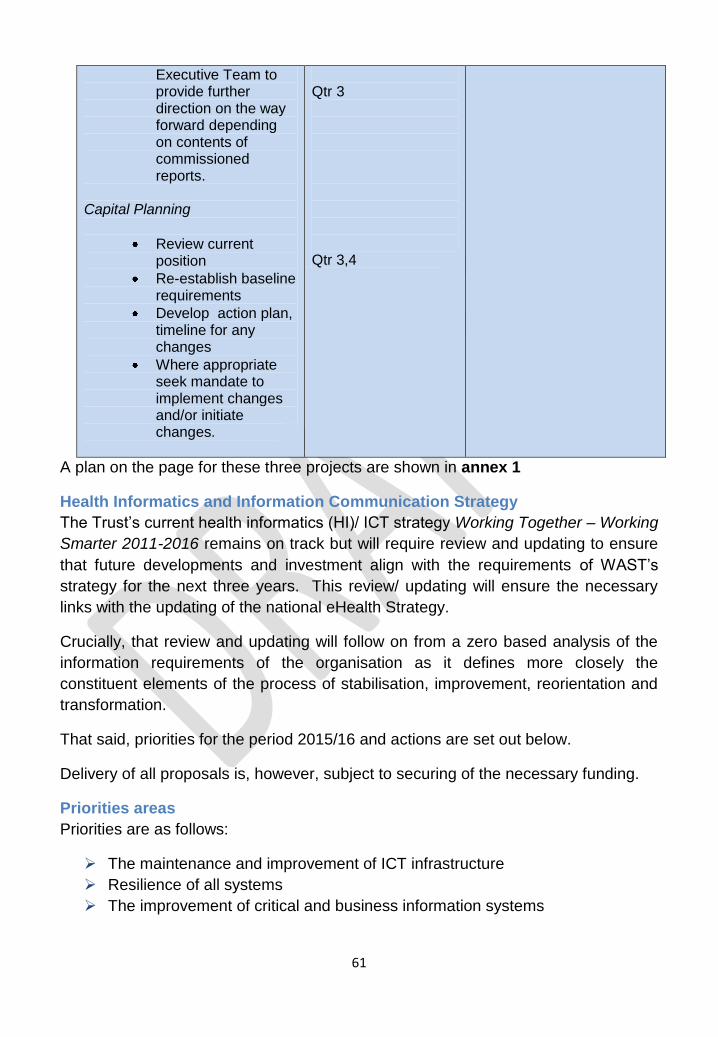
61
Executive Team to provide further direction on the way forward depending on contents of commissioned reports.
Capital Planning
Review current position
Re-establish baseline requirements
Develop action plan, timeline for any changes
Where appropriate seek mandate to implement changes and/or initiate changes.
Qtr 3 Qtr 3,4
A plan on the page for these three projects are shown in annex 1
Health Informatics and Information Communication Strategy The Trust‟s current health informatics (HI)/ ICT strategy Working Together – Working
Smarter 2011-2016 remains on track but will require review and updating to ensure
that future developments and investment align with the requirements of WAST‟s
strategy for the next three years. This review/ updating will ensure the necessary
links with the updating of the national eHealth Strategy.
Crucially, that review and updating will follow on from a zero based analysis of the
information requirements of the organisation as it defines more closely the
constituent elements of the process of stabilisation, improvement, reorientation and
transformation.
That said, priorities for the period 2015/16 and actions are set out below.
Delivery of all proposals is, however, subject to securing of the necessary funding.
Priorities areas
Priorities are as follows:
The maintenance and improvement of ICT infrastructure
Resilience of all systems
The improvement of critical and business information systems
62
Working with partner organisations in the health, other emergency services
and other sector(s) on the sharing of information and potentially sharing
facilities
Supporting improved staff access and patient engagement
Enhancing Business Continuity
Improving ICT operational service delivery
Developing the professional skills of ICT staff
Develop the organisation‟s commissioning dataset
Strengthen the Trust‟s Information Governance Standards to maintain our
information‟s confidentiality, integrity and availability
Increasing our range of internet-based and mobile services
Consolidating our information systems to provide internal and external-facing
portals for Trust statistics and management information
Further developing our data warehouse by incorporating clinical and
business-support data streams
Developing a Records Management framework which outlines how we treat
each type of information, ensuring classification, retention and disposal
guidelines are adhered to
Developing the approach and plan towards achieving ISO/IEC 15489-1 and
ISO9001.
The primary focus during the first part of 2015-2016 will be to consolidate all ongoing
works to build a resilient, robust and highly available ICT infrastructure which will
provide the foundation to support the vision for delivery of HI and ICT services for a
21st century ambulance services. This will also place the ICT department in a strong
position to support the IMTP projects proposed in the transformation programmes
such as Clinical Modernisation, as they develop.
Whilst very much out of sight for the majority of users, nonetheless the Trust will
continue with the maintenance of the network, server and storage infrastructure,
ensuring the Trust meets is legal obligation for licensing of servers and end user
devices (EUD), i.e. desktop, laptop, tablet computers and Smartphones.
The Trust will need to complete the work to replace computers that are incompatible
with Windows 7 in order to mitigate the security risk of Windows XP from June 2014.
In so doing, it is hoped to upgrade the heavily ageing computer population currently
in use within the Trust.
During this period we will also work with colleagues within the trust on
implementation of solutions namely, Digi Pens, a demand and capacity modelling
system, CFR application and a replacement CAD. We will also look to enhance the
capability of current systems. An early opportunity exists with PCS where, as a first
63
step, we can look to provide secured access to patients, thorough dedicated kiosks
at treatment centres to electronically book transport.
WAST will also work with NWIS to provide access to national information resources,
such as the Master Patient Index (eMPI) and Individual Health Records (IHR) as well
as investigating options to provide Trust information into national repositories, such
as Welch Clinical Records Service (WCRS). We will also look to work with
colleagues in LHBs on local initiatives to exploit ICT in order to improve the patient
experience.
The Trust will contribute to the work of national projects such as USC, 111, ARP and
Emergency Services Mobile Communication Programme (ESMCP) ensuring the
Trust requirements for these services are included and the Trust is well positioned to
take advantage of future developments delivered by these programmes and to adopt
them into its future operational model. An ESMCP project team will be established
as preparatory work will be required in 2016
The Trust will look to enhance our Wi-Fi service by extending it across our buildings.
This is an essential component to support an increase in mobile computing thereby
providing easier access to staff.
Improvement in ICT service delivery will continue as the current Service
Improvement Plan evolves with the introduction of the Information Technology
Infrastructure Library (ITIL) processes for problem, change and release
management. Further work on pro-active monitoring management of ICT
infrastructure will also be improved through the introduction of System Control and
Configuration Manager (SCCM) as a management tool for both Servers and EUD
In executing all these programmes of work, we will take account of information
security and business continuity requirements and build and develop these into the
delivery of the final solutions, thereby ensuring that the Trust not only meets its
legislative requirements but is well placed to minimise any service disruption through
technical failures.
In order to support the organisation there will be a requirement to ensure that new
models of care are suitably statistically modelled to support strategic decision-
making. This includes co-production modelling to support the South Wales
Programme, the Mid Wales Healthcare Collaboration and the ongoing review of
acute services in Betsi Cadwaladr University LHB, as well as supporting capacity
and service reviews.
64
A key development will be the production of our organisation commissioning dataset
and ongoing information analysis and support. As the roll-out of national and local
commissioning arrangements commence, how we share information with our
partners and regulators will need to change to reflect this.
The Trust will develop and update our plans for our SQL Server estate and our Data
Warehouse, ensuring that short term recommendations are addressed as a priority.
We will document a long-term plan to incorporate additional data streams such as
clinical, fleet, HR and risk management information. We will upgrade our information
portals such as Launchpad and ensure that our information systems have a modern
interface that people are used to in their private lives. Part of this upgrade will be
simplified access to our information systems through the use of a single sign-on
process.
Central to our informatics delivery will continue to be modern, fit for purpose
technological solutions in the form of internet and mobile technologies. Ensuring
that we use smart applications to support demand management and health
promotion will underpin our organisation‟s Quality plan. We will continue to develop
apps and self-assessment tools to support the self-care agenda in NHS Wales.
We will ensure that a robust records management framework and records retention
schedule is in place. We will undertake a complete records inventory and
information asset owners directory to create a departmental register of information.
We will develop an approach to deliver ISO15489-1 in Records Management for
implementation in the following years.
The Trust will strengthen the Trust‟s Information Governance Standards to maintain
our Information‟s confidentiality, integrity and availability by ensuring our policies and
procedures are fit for purpose. The Trust‟s Information Governance Training &
Awareness programme will be upgraded in-year which will provide further assurance
and protection of our data assets.
We will ensure that our data standards and statistical reporting systems, structures
and processes are continually reviewed by adopting ISO9001 data quality
standards. Immediately, we will upgrade our data dictionary and create information
release grading standards and an Information Classification protocol for the security
marking and subsequent handling of its information assets and documents.
The Trust will conduct a review of the current skills and abilities of ICT staff and
identify any gaps in key technology areas. We will then develop a structured
development programme for each member of staff to ensure they can support the
future developments and technologies while minimising the need to employ external
contractors.
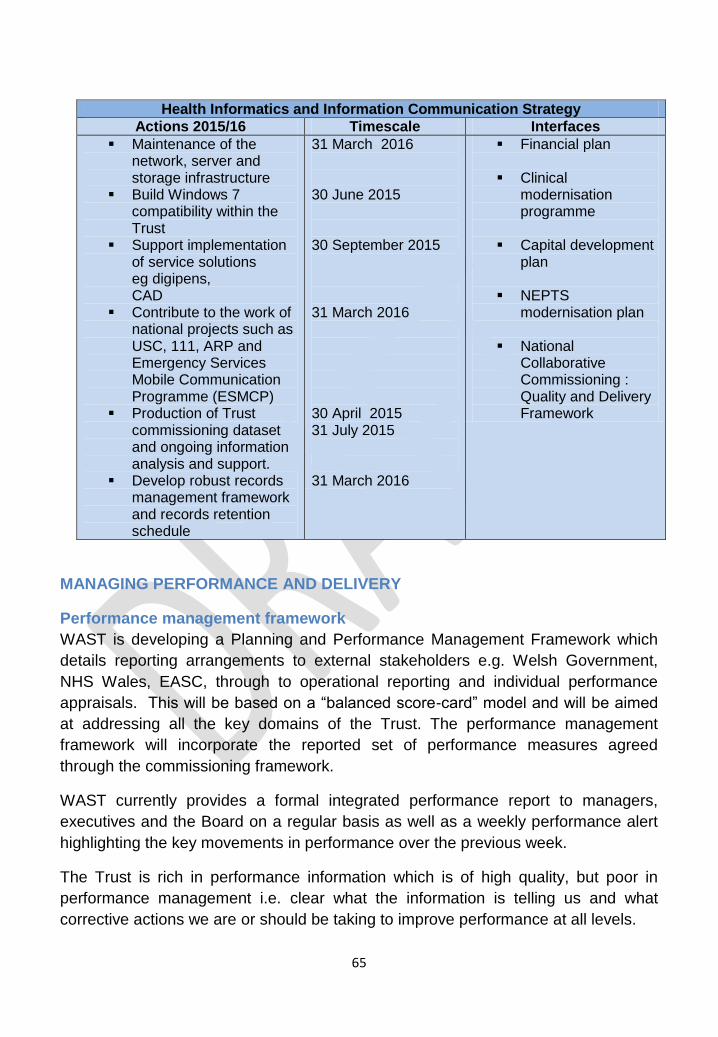
65
Health Informatics and Information Communication Strategy
Actions 2015/16 Timescale Interfaces
Maintenance of the network, server and storage infrastructure
Build Windows 7 compatibility within the Trust
Support implementation of service solutions eg digipens, CAD
Contribute to the work of national projects such as USC, 111, ARP and Emergency Services Mobile Communication Programme (ESMCP)
Production of Trust commissioning dataset and ongoing information analysis and support.
Develop robust records management framework and records retention schedule
31 March 2016 30 June 2015 30 September 2015
31 March 2016 30 April 2015 31 July 2015 31 March 2016
Financial plan
Clinical modernisation programme
Capital development plan
NEPTS modernisation plan
National Collaborative Commissioning : Quality and Delivery Framework
MANAGING PERFORMANCE AND DELIVERY
Performance management framework
WAST is developing a Planning and Performance Management Framework which
details reporting arrangements to external stakeholders e.g. Welsh Government,
NHS Wales, EASC, through to operational reporting and individual performance
appraisals. This will be based on a “balanced score-card” model and will be aimed
at addressing all the key domains of the Trust. The performance management
framework will incorporate the reported set of performance measures agreed
through the commissioning framework.
WAST currently provides a formal integrated performance report to managers,
executives and the Board on a regular basis as well as a weekly performance alert
highlighting the key movements in performance over the previous week.
The Trust is rich in performance information which is of high quality, but poor in
performance management i.e. clear what the information is telling us and what
corrective actions we are or should be taking to improve performance at all levels.
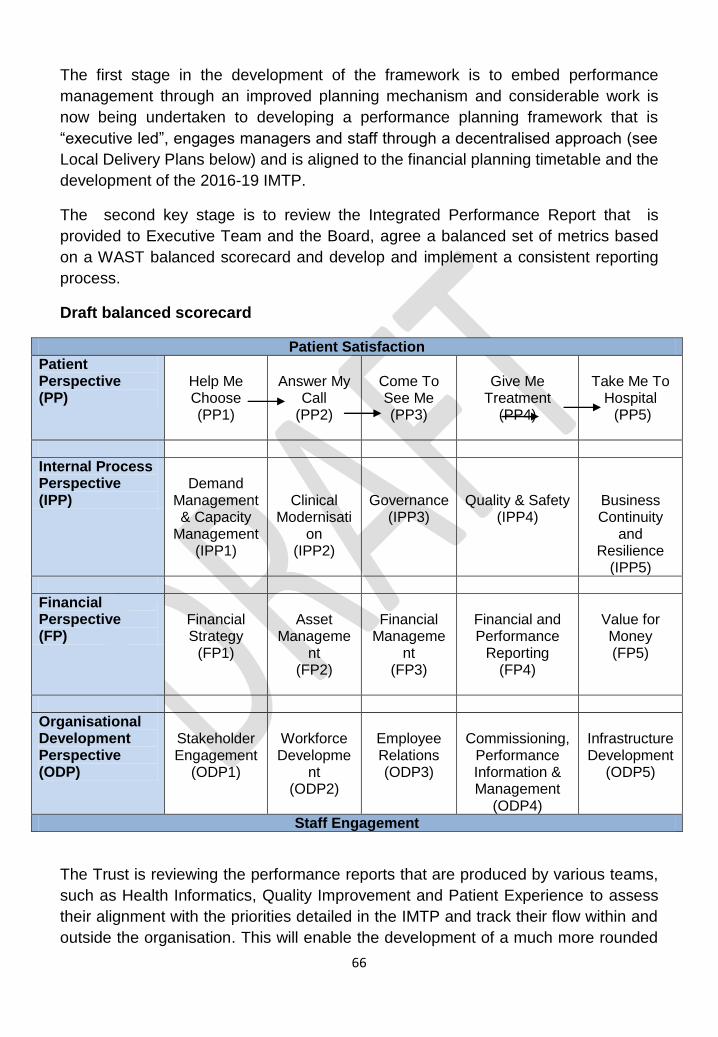
66
The first stage in the development of the framework is to embed performance
management through an improved planning mechanism and considerable work is
now being undertaken to developing a performance planning framework that is
“executive led”, engages managers and staff through a decentralised approach (see
Local Delivery Plans below) and is aligned to the financial planning timetable and the
development of the 2016-19 IMTP.
The second key stage is to review the Integrated Performance Report that is
provided to Executive Team and the Board, agree a balanced set of metrics based
on a WAST balanced scorecard and develop and implement a consistent reporting
process.
Draft balanced scorecard
Patient Satisfaction
Patient Perspective (PP)
Help Me Choose (PP1)
Answer My
Call (PP2)
Come To See Me (PP3)
Give Me
Treatment (PP4)
Take Me To
Hospital (PP5)
Internal Process Perspective (IPP)
Demand
Management & Capacity
Management (IPP1)
Clinical Modernisati
on (IPP2)
Governance (IPP3)
Quality & Safety (IPP4)
Business Continuity
and Resilience
(IPP5)
Financial Perspective (FP)
Financial Strategy
(FP1)
Asset
Management
(FP2)
Financial
Management
(FP3)
Financial and Performance
Reporting (FP4)
Value for Money (FP5)
Organisational Development Perspective (ODP)
Stakeholder Engagement
(ODP1)
Workforce Developme
nt (ODP2)
Employee Relations (ODP3)
Commissioning,
Performance Information & Management
(ODP4)
Infrastructure Development
(ODP5)
Staff Engagement
The Trust is reviewing the performance reports that are produced by various teams,
such as Health Informatics, Quality Improvement and Patient Experience to assess
their alignment with the priorities detailed in the IMTP and track their flow within and
outside the organisation. This will enable the development of a much more rounded
67
and integrated performance report and result in an agreed suite of reports with a
timetable for their production and reporting.
It will be important to ensure that the Local Delivery Plan process includes a clear
performance “diagnosis” for each operations area i.e. what the particular
performance issues are in each LHB area and the key solutions that then flow from
these.
The Trust is also considering the use of email alerts so that “live” information is
available to the right people, in WAST so that performance on the 5 step clinical
model can be monitored and managed in real time rather than historic information
being reviewed.
Finally, the development of a demand and capacity model, agreed with
commissioners, will inform the development of the performance management
framework and enable benchmarking with other comparable organisations. This is a
significant piece of work, but in the short term the Trust will build its performance
framework based on the principles outlined above.
Programme and project management arrangements
Delivery of the Trust strategy will build on the adoption of formal programme, project
and workstream management originally deployed in support of the Trusts Strategic
Transformation Programme (STP). In line with the activities identified in the original
IMTP a series of plans on a page (PoPs) have been written. This exercise required
officers to address a series of aspects of the work required, which included:
Purpose and Objectives
Background
Required resources
Timescales and key milestones
Scope
Governance structure
Risk and issues including any mitigating action taken
Dependencies
Expected outcomes
Expected benefits and measures of success
This allowed each of the proposed areas of work to be mapped to one of the eight
priorities which have subsequently emerged as part of this IMTP re-fresh to see if
there is continued alignment / justification for the work. Where there was not
alignment it was agreed the work be scheduled for years two or three. Annex 2
details the results of this mapping exercise.
68
The suite of PoPs was subsequently taken to the inaugural meeting of the IMTP
Portfolio Board where the robustness of information was scrutinised and an
assessment made as to whether the work in question was:
Routine / low risk / low contention / business development type activity and
could thus be progressed within the business as usual (BAU) environment of
the organisation e.g. handed to the relevant Director for execution within their
Directorate.
Discrete / „new‟ / high risk e.g. reputational / highly specialised type activity
and would thus benefit from being embedded within a dedicated programme
and project management environment.
Annex 3 presents the outcome of this assessment.
Just as when projects and programmes are complete and products are moved into
the business as usual environment of the business it is equally recognised that at
certain points of time some activities will need to move from business as usual into a
formal project and programme management (PPM) environment.
For example, there may be significant ICT and capital projects which once
developmental work (business case preparation, approval etc) has been undertaken
will require moving into a PPM environment in order to maximise the chances of
timely and high quality delivery.
Consequently, WAST has identified four strategic programmes comprising a number
of projects requiring a formal management approach:-
1. Workforce & OD - our people
2. Clinical Modernisation – our services
3. Non Emergency Patient Transport Services – our services
4. Strategic Efficiency & Effectiveness – our resources
The STP has been subsumed within the four programmes and its constituent
projects will be managed through the new programme and Portfolio Management
arrangements. Annex 1 documents the plans on a page for these projects.
Delivery of these four programmes will be through the IMTP Portfolio Board (chaired
by the Chief Executive). This Board will:
Ensure the Portfolio of programmes delivers within agreed parameters
Resolves strategic issues between programmes
Makes resource decisions in regards to delivery of the Portfolio
Gives approval (or not) of key milestone outputs.
69
In order for the organisation to retain confidence on the delivery of those activities
which have been deemed suitable for progression within the BAU part of the
business monthly „status reports‟ for these areas will also be required by the
Portfolio Board.
The Portfolio Board will be supported by an IMTP Implementation group which will
be chaired by the Associate Portfolio and Programme Director. The group will
constitute the respective programme leads and other key stakeholders. This group
will:
Manage delivery of the programmes on a day to day basis
Ensure key dependencies, barriers between programmes are identified and
managed.
Portfolio level risks and issues are identified and actively managed.
Allow the Portfolio Board to „manage by exception‟ whilst being able to retain
confidence and a clear line of sight regarding the Portfolio.
The Portfolio structure for delivery is reproduced in full at Annex 4.
Local Delivery Plans
It is recognised that the original IMTP was largely driven by the Executive Team on a
„top down‟ basis. However, this refreshed IMTP and the clear priorities agreed for
2015/16 is expected to help better engage and involve staff in creating an
understanding of the challenges faced by the Trust, the way these are being tackled
and how frontline staff and our partners can contribute to successful delivery over
the coming year. As part of the roll out of the Plan, each LHB based team (together
with other operational units such as HART and the Clinical Control Centres) will work
on the localisation of the IMTP through the development of Local Delivery Plans
(LDPs). These will not only describe the implementation of year one priorities but
will also establish a platform from which staff across the Trust can contribute and
drive the development of the 2016/2019IMTP.
Local Performance & Planning Cells
Delivering improvement in the performance of EMS and NEPTS will require
enhanced joint working with LHBs. This will be supported through the establishment
of Local Performance & Planning Cells (LPPCs) in each LHB area.
Developing the 2016/19 IMTP
Planning the development of the 2016/19 IMTP is a critical element of the continued
transformation of WAST and will signal a shift in emphasis to a “bottom-up”, creative
approach to strategic planning and delivery rather than a “top-down” executive level
document. The timetable for developing the 2016/19 IMTP is below.
Date Forum Purpose End June 2015 Senior Management Team Tier 3 initial engagement in
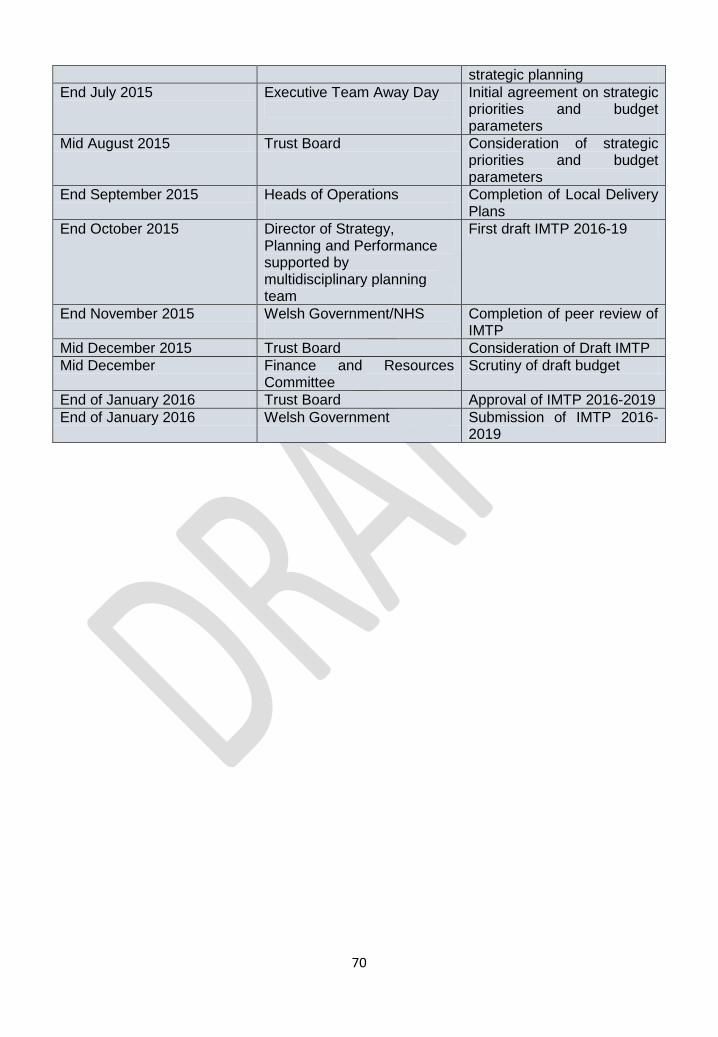
70
strategic planning
End July 2015 Executive Team Away Day
Initial agreement on strategic priorities and budget parameters
Mid August 2015 Trust Board Consideration of strategic priorities and budget parameters
End September 2015 Heads of Operations
Completion of Local Delivery Plans
End October 2015 Director of Strategy, Planning and Performance supported by multidisciplinary planning team
First draft IMTP 2016-19
End November 2015 Welsh Government/NHS
Completion of peer review of IMTP
Mid December 2015 Trust Board Consideration of Draft IMTP
Mid December Finance and Resources Committee
Scrutiny of draft budget
End of January 2016 Trust Board Approval of IMTP 2016-2019
End of January 2016 Welsh Government Submission of IMTP 2016-2019
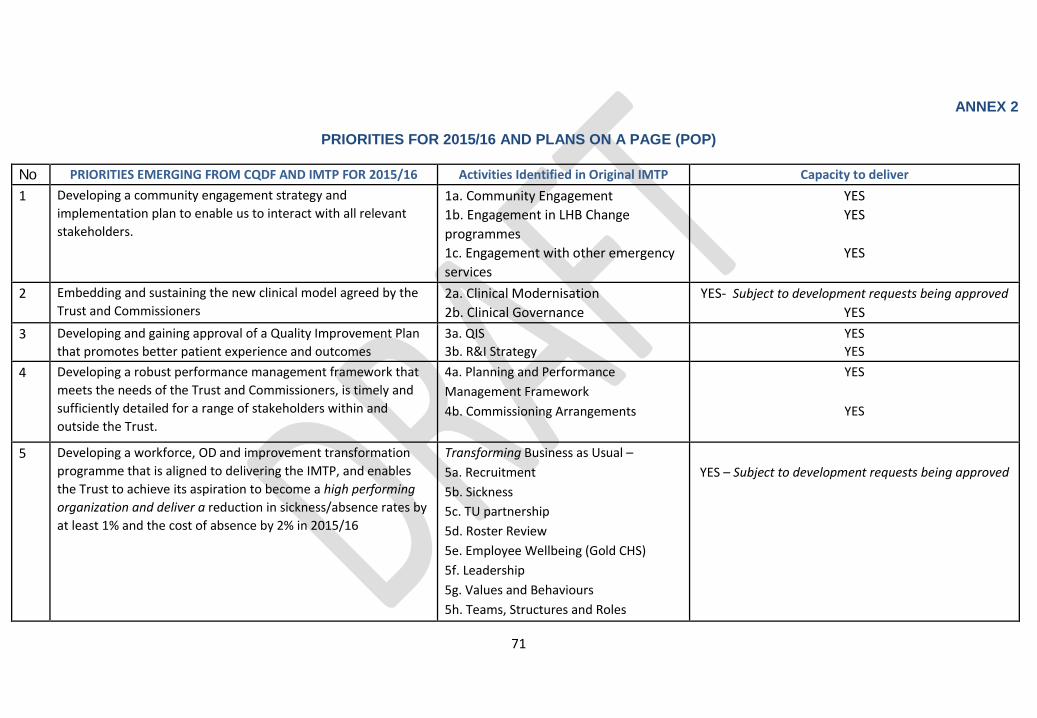
71
ANNEX 2
PRIORITIES FOR 2015/16 AND PLANS ON A PAGE (POP)
No PRIORITIES EMERGING FROM CQDF AND IMTP FOR 2015/16 Activities Identified in Original IMTP Capacity to deliver
1 Developing a community engagement strategy and
implementation plan to enable us to interact with all relevant
stakeholders.
1a. Community Engagement 1b. Engagement in LHB Change
programmes 1c. Engagement with other emergency
services
YES
YES
YES
2 Embedding and sustaining the new clinical model agreed by the
Trust and Commissioners 2a. Clinical Modernisation 2b. Clinical Governance
YES- Subject to development requests being approved
YES
3 Developing and gaining approval of a Quality Improvement Plan
that promotes better patient experience and outcomes
3a. QIS 3b. R&I Strategy
YES
YES
4 Developing a robust performance management framework that
meets the needs of the Trust and Commissioners, is timely and
sufficiently detailed for a range of stakeholders within and
outside the Trust.
4a. Planning and Performance
Management Framework 4b. Commissioning Arrangements
YES
YES
5 Developing a workforce, OD and improvement transformation
programme that is aligned to delivering the IMTP, and enables
the Trust to achieve its aspiration to become a high performing
organization and deliver a reduction in sickness/absence rates by
at least 1% and the cost of absence by 2% in 2015/16
Transforming Business as Usual –
5a. Recruitment 5b. Sickness 5c. TU partnership 5d. Roster Review 5e. Employee Wellbeing (Gold CHS)
5f. Leadership
5g. Values and Behaviours
5h. Teams, Structures and Roles
YES – Subject to development requests being approved
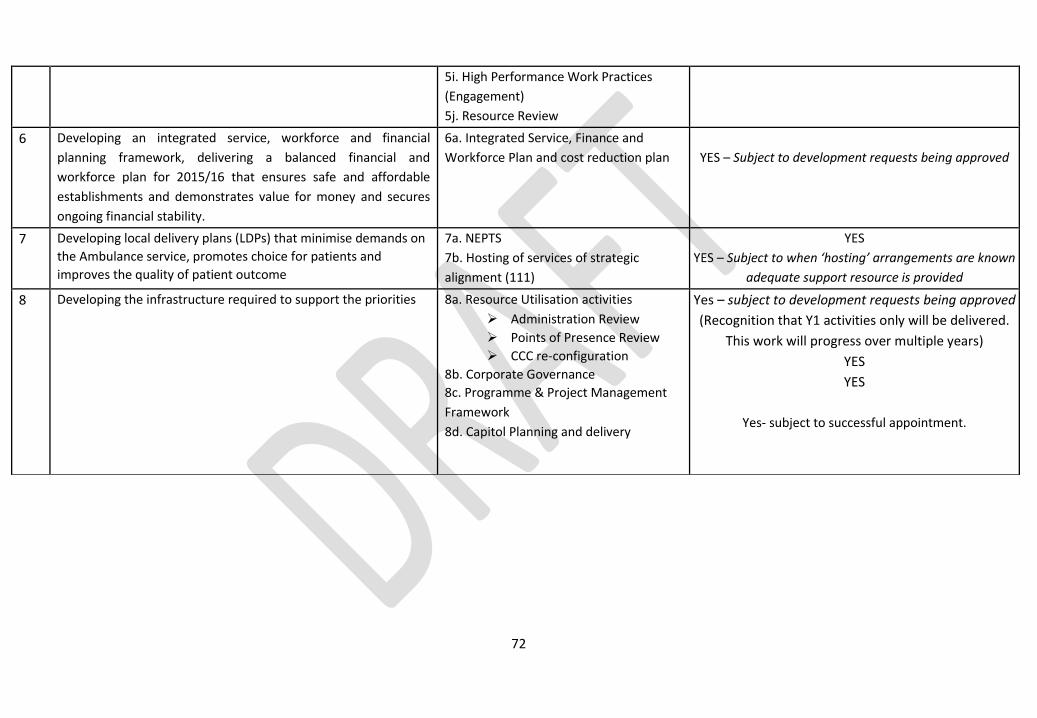
72
5i. High Performance Work Practices
(Engagement)
5j. Resource Review
6 Developing an integrated service, workforce and financial
planning framework, delivering a balanced financial and
workforce plan for 2015/16 that ensures safe and affordable
establishments and demonstrates value for money and secures
ongoing financial stability.
6a. Integrated Service, Finance and
Workforce Plan and cost reduction plan
YES – Subject to development requests being approved
7 Developing local delivery plans (LDPs) that minimise demands on
the Ambulance service, promotes choice for patients and
improves the quality of patient outcome
7a. NEPTS 7b. Hosting of services of strategic
alignment (111)
YES
YES – Subject to when ‘hosting’ arrangements are known
adequate support resource is provided
8 Developing the infrastructure required to support the priorities 8a. Resource Utilisation activities
Administration Review
Points of Presence Review
CCC re-configuration
8b. Corporate Governance 8c. Programme & Project Management
Framework
8d. Capitol Planning and delivery
Yes – subject to development requests being approved
(Recognition that Y1 activities only will be delivered.
This work will progress over multiple years)
YES
YES
Yes- subject to successful appointment.
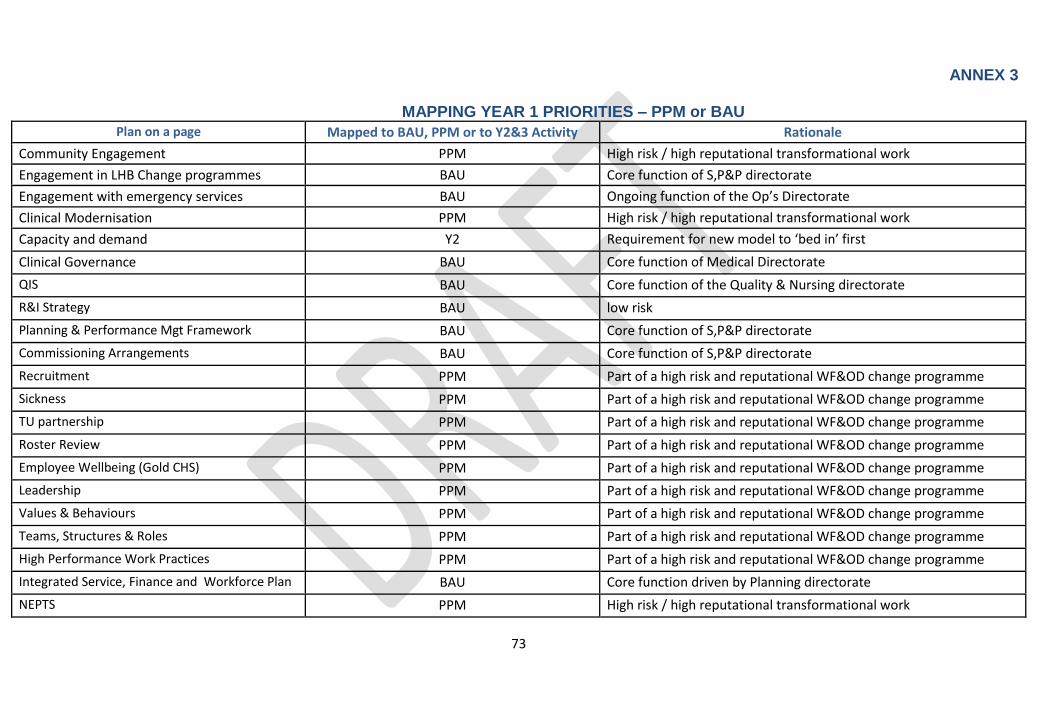
73
ANNEX 3 MAPPING YEAR 1 PRIORITIES – PPM or BAU
Plan on a page Mapped to BAU, PPM or to Y2&3 Activity Rationale
Community Engagement PPM High risk / high reputational transformational work
Engagement in LHB Change programmes BAU Core function of S,P&P directorate
Engagement with emergency services BAU Ongoing function of the Op’s Directorate
Clinical Modernisation PPM High risk / high reputational transformational work
Capacity and demand Y2 Requirement for new model to ‘bed in’ first
Clinical Governance BAU Core function of Medical Directorate
QIS BAU Core function of the Quality & Nursing directorate
R&I Strategy BAU low risk
Planning & Performance Mgt Framework BAU Core function of S,P&P directorate
Commissioning Arrangements BAU Core function of S,P&P directorate
Recruitment PPM Part of a high risk and reputational WF&OD change programme
Sickness PPM Part of a high risk and reputational WF&OD change programme
TU partnership PPM Part of a high risk and reputational WF&OD change programme
Roster Review PPM Part of a high risk and reputational WF&OD change programme
Employee Wellbeing (Gold CHS) PPM Part of a high risk and reputational WF&OD change programme
Leadership PPM Part of a high risk and reputational WF&OD change programme
Values & Behaviours PPM Part of a high risk and reputational WF&OD change programme
Teams, Structures & Roles PPM Part of a high risk and reputational WF&OD change programme
High Performance Work Practices PPM Part of a high risk and reputational WF&OD change programme
Integrated Service, Finance and Workforce Plan BAU Core function driven by Planning directorate
NEPTS PPM High risk / high reputational transformational work
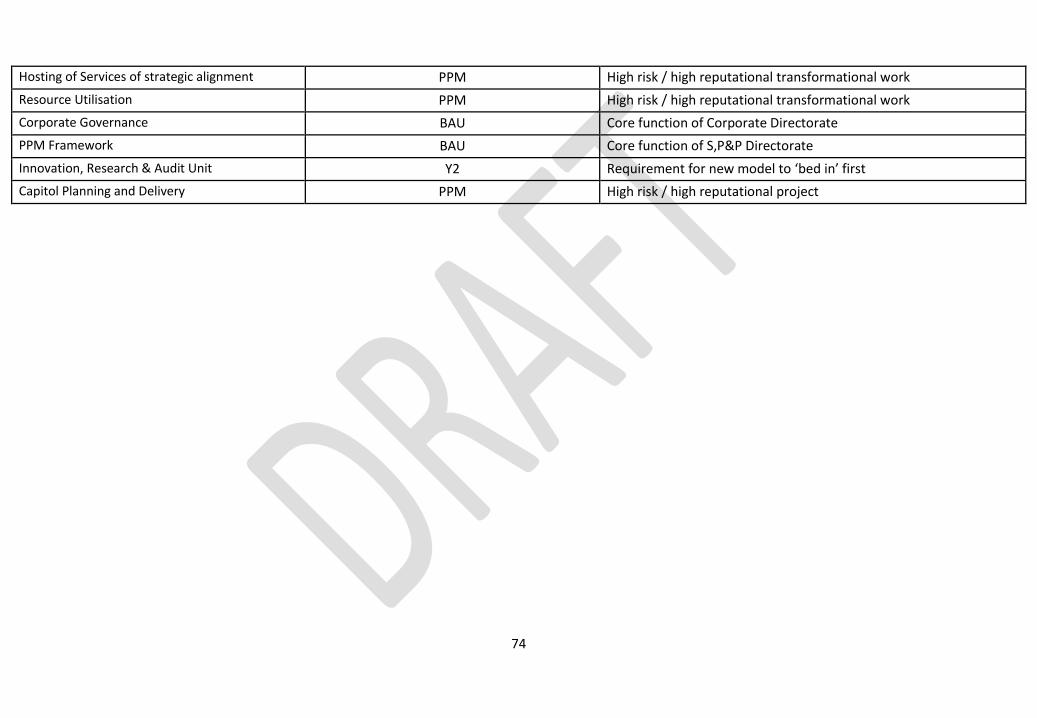
74
Hosting of Services of strategic alignment PPM High risk / high reputational transformational work
Resource Utilisation PPM High risk / high reputational transformational work
Corporate Governance BAU Core function of Corporate Directorate
PPM Framework BAU Core function of S,P&P Directorate
Innovation, Research & Audit Unit Y2 Requirement for new model to ‘bed in’ first
Capitol Planning and Delivery PPM High risk / high reputational project
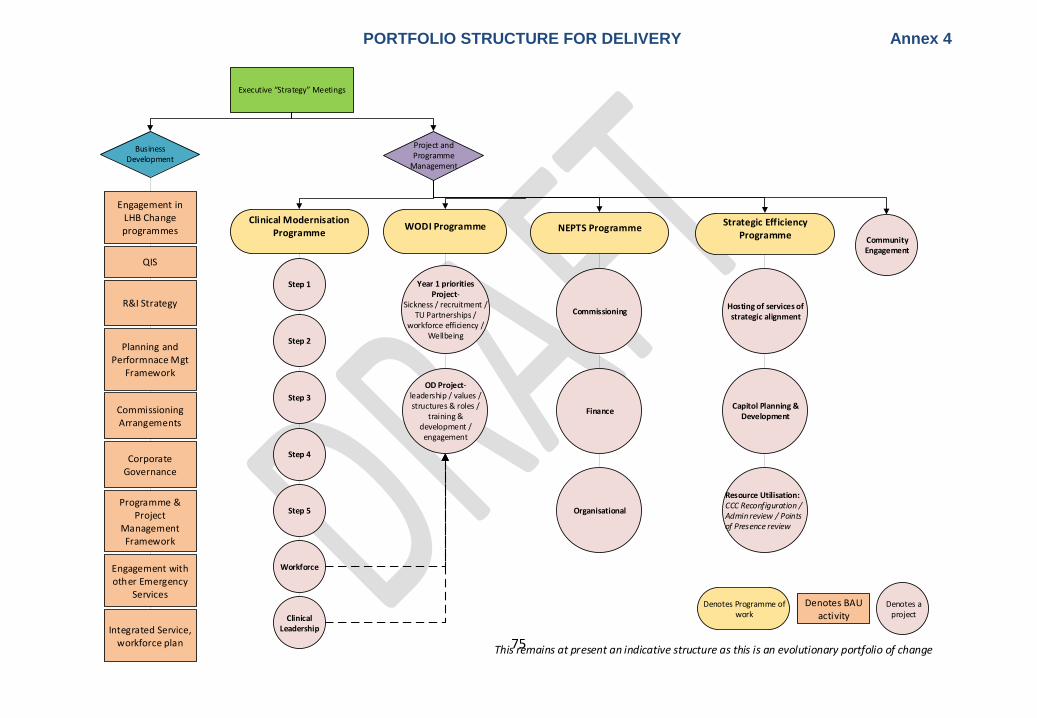
75
Executive “Strategy” Meetings
Business Development
Project and Programme
Management
Clinical Modernisation Programme
WODI Programme NEPTS ProgrammeStrategic Efficiency
Programme
Step 1
Step 2
Step 3
Commissioning
Finance
Resource Utilisation:CCC Reconfiguration / Admin review / Points of Presence review
Organisational
Step 4
Step 5
Workforce
Clinical Leadership
Hosting of services of strategic alignment
Community Engagement
Engagement in LHB Change programmes
QIS
R&I Strategy
Planning and Performnace Mgt
Framework
Commissioning Arrangements
Corporate Governance
Programme & Project
Management Framework
Engagement with other Emergency
Services
Capitol Planning & Development
Denotes Programme of work
Denotes a project
Denotes BAU activity
This remains at present an indicative structure as this is an evolutionary portfolio of change
Year 1 priorities Project-
Sickness / recruitment / TU Partnerships /
workforce efficiency / Wellbeing
OD Project- leadership / values / structures & roles /
training & development / engagement
Integrated Service, workforce plan
PORTFOLIO STRUCTURE FOR DELIVERY Annex 4





























