Embed Size (px)
Citation preview

What are we trying to do?What are we trying to do?

Acute Acute Phase Phase Driver Driver
DiagramDiagram

An example from another An example from another settingsetting
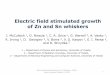
Acute MI Care in US
• Aspirin at discharge • ACEI for LVSD • Beta-blocker at arrival • Beta-blocker at discharge • Door to lytic • Door to PCI • Smoking cessation advice • Composite and all-or-none scores • Survival rate/index• Aspirin at arrival


ReliabilityReliability
Level 1 10-1 errors 90% right
Level 2 10-2 errors 99% right
Level 3 10-3 errors 99.9% right

Examples – most are level 2 or 3Examples – most are level 2 or 3but three are level 1but three are level 1
• Himalaya mountaineering • Fatal iatrogenic adverse events • Cardiac surgery (Patient ASA 3-5) • Road safety • Civil aviation • Railways • France Nuclear power industry • Anaesthesia ASA1 • Blood transfusion • A and E staff reading X-rays

Examples – most are level 2 or 3 Examples – most are level 2 or 3 but three are level 1but three are level 1
• Himalaya mountaineering • Fatal iatrogenic adverse events • Cardiac surgery (Patient ASA 3-5) • Road safety • Civil aviation • Railways • France Nuclear power industry • Anaesthesia ASA1 • Blood transfusion • A and E staff reading X-rays

Strategies –Level 1Strategies –Level 1“Intent, vigilance, hard work”
• Standardized protocols• Feedback• Training• Checklists

What they did at the MayoWhat they did at the Mayo• Expanded the Chest Pain Center hours to 24/7 with observation area for
23-hour evaluation. • Revised criteria for EKG screening in the ED to include atypical
presentations (e.g., non-STEMI, female, gastric). • Created buy-in to measures by reviewing the inclusion and exclusion
criteria for each indicator for CMS/ORYX, thereby accelerated the learning curve on the varying definitions compared to prior/other benchmarks.
• Overhauled ED and Cath Lab process flow including transmission of EKG results by the EMS, setting time threshold cutoffs, implementing a master clock system, centralizing the Cath Lab call-back system, fast-tracking Cath Lab set-up with ED transport and pre-set equipment/supplies, and availability of non-interventional or interventional cardiologist to start the case.
• Revised elective Cath Lab schedule to expand blocks, hours of service. • Added smoking history to admission assessment for all patients. • Trained acute MI care champions in each care area.

Strategies –Level 2Strategies –Level 2“Redesign the system –
don’t rely on checking”
• Decision aids and reminders built into the system
• Automation• Evidence as the default• Scheduling• Connection to habits

What they did at the MayoWhat they did at the Mayo• Activated Chest Pain Center default orders tailored to AMI type,
incorporated on ED record, with RN follows up with ER physician if variation.
• Inserted opportunity for ED MD to give the lytic if door-to-Cath Lab time predicted to exceed 90 minutes.
• Initiated concurrent redundant review in the Cath Lab to identify and mitigate fallouts (e.g., ASA or beta-blocker within 24 hours of arrival).
• Created brochure for first- and second-hand smoking cessation, made default care for all patients regardless of diagnosis.
• Implemented Quality Management review of all admitted patients for evidence-based indicators, with concurrent review with ED, cardiologist if fallout.
• Reviewed final fallouts routinely with ED, hospitalist and cardiology physicians and nursing staff, with drill-down data for PCI process as well as non-STEMIs, to create enhanced understanding of overall scoring and further PI opportunities.
• Next changes: Adding to manager/director/VP and hospitalist incentive goals.


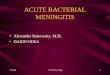
We can do this in Wales!We can do this in Wales!

Feb-07Dec-07Oct-07Aug-07J un-07Apr-07Feb-07Dec-06Oct-06Aug-06J un-06
100.00%
90.00%
80.00%
_X=97.82%
Feb-07Dec-07Oct-07Aug-07J un-07Apr-07Feb-07Dec-06Oct-06Aug-06J un-06
90.00%
60.00%
30.00%
_X=97.11%
Feb-07Dec-07Oct-07Aug-07J un-07Apr-07Feb-07Dec-06Oct-06Aug-06J un-06
102.00%
96.00%
90.00%
_X=94.71%
UCL=103.43%
LCL=85.99%
6
11
566
113
3
665
11
I Chart of Vent Bundle
I Chart of CVC bundle
I Chart of CVCI bundle


Action plansAction plans
• Local awareness• Ownership• Agree morbidity outcome measure• Ensure data collection• Drive for reliability• Understand special cases• Make hypotheses• PDSAs• June conference