Embed Size (px)
Citation preview
facts and opinion What Do Nurses Know About Breastfeeding Problems? PATRICIA JENAWAY E S T O K , RN, BSN, MSN
A small sampling of nurses completed a questionnaire designed to ,determine a ) whether nurses can identify common problems mothers have wi th breast feeding after they are discharged f r o m the hospital and b) whether ability to identify the problems is affected b y the nurse’s date of graduation f r o m nursing school, age, direct or indirect experience wi th breastfeeding, or her attitude toward breastfeeding. T h e nurses were unable to identify the problems, and the variables tested did not influence their ability. T h i s points to a deficiency in nurses’ knowledge about breastfeeding problems and in the guidance offered t o mothers w h o chose to breastfeed.
Nurses often discuss the value of meeting the individual needs of the patient. To do this, the professional nurse must be able to identify the patient’s needs, discern what nursing intervention is necessary or desirable, initiate the necessary intervention, and evaluate the consequences. Dis- brow and others1s2 have suggested that nursing intervention is a factor in successful breastfeeding and that discussion with a mother of breastfeeding problems that may arise within six weeks following her discharge from the hospital could increase the probability of breastfeeding success. Many authors, however, point out the fact that the new mother does not receive the guidance she needs from the nursing ~ t a f f ’ . ~ * ~ and that, after discharge, bottle- feeding is all too often substituted for breast- feeding.
W h y don’t maternity nurses prepare patients to meet their problems? Disbrow asks if it “could be that the nurse does not know what happens during the first few weeks of breastfeeding after the mother leaves the hospital.”6 Brown et al. state that “one gains the impression that many nurses either entertain negative attitudes toward breast- feeding or are insufficiently trained to give help,
or both.”4 According to Salber, Stitt, and Babbitt, “medical and nursing students are getting very lit- tle practical training in breastfeeding techniques.”’
This study was designed to test whether these postulations are true-whether nurses can identify the common probIems mothers have with breast- feeding after discharge from the hospital and whether this ability is affected by the nurse’s date of graduation from nursing school, age, direct or indirect experience with breastfeeding, or attitude toward breastfeeding.
BREASTFEEDING PROBLEMS : REVIEW OF THE LITERATURE
Studies have been done to determine what prob- lems breastfeeding mothers encounter most often after hospital discharge. Burnett stated that the most frequent reasons for weaning babies, given by 254 women who were breastfeeding at dis- charge, were 1) insufficient milk, 2) social incon- vience, 3 ) milk was not good for the baby, and 4) mother was too tired to ~ o n t i n u e . ~ Branin studied 26 nursing mothers and stated that all of their breastfeeding problems could have been avoided or alleviated if the patients had received adequate information on 1) breast care, 2) breast changes, 3 ) changes in infant feeding habits, 4) sibling rivalry, 5) diet, 6) importance of adequate rest, 7 ) importance of adequate fluids, 8) relation of breast stimulation to milk supply, and 9 ) basic emotional reaction^.^ Branin’s sample included mul- tiparas as well as primiparas. Disbrow’s sample was made up of 1 7 5 primiparas-nearly the total population of primiparas at a particular hospital during a one-year period. T h e problems they en- countered most often after discharge from the hospital were’:
1. Length of time it took for milk supply to
2. Milk flowing too freely, 3 . Difficulty in determining when the baby was
hungry and whether or not he was getting enough to eat,
4. H o w to arrive at the most comfortable posi- tion for both mother and baby during nursing,
stabilize,
36 November/December 1973 JOGN Nursing
5. Mother’s feeling of being constantly tired
6. The occurrence of unexpected and uncon-
7. Mother being tied down much more than
and irritable,
trollable spells of crying by the mother,
she expected.
The common problems revealed in Disbrow’s study were used as the basis for this study because the list is more inclusive than Burnett’s and because the sample was larger and more well controlled than Branin’s.
THE SAMPLE A sample was drawn from the population of
Registered Nurses employed a t hospitals in a large metropolitan area in the Midwest. Hospitals with more than 2,000 births per year were listed alpha- betically and numbered. A table of random num- bers was used to select three hospitals from the list. The names of Registered Nurses who worked more than 30 hours per week on postpartum and/or nursery units of each hospital were listed and numbered. A table of random numbers was used to select 10 from each hospital. In one hospital where the total maternity nurse population was 9, the entire group was used. Only hospitals with large maternity units were chosen in order to obtain the desired sample number and facilitate data collection. It was assumed that nurses working in either small or large metropolitan hospitals would have a normal distribution with regard to recency of graduation and ability to identify Disbrow’s common problems.
An analysis of variance revealed that the three groups of nurses can be considered to come from the same population in regard to age, date of grad- uation, and the number of Disbrow’s common problems that they identified (see Table 1 ) .
RESULTS Ability to Identify Problems
The 29 nurses sampled varied little in their ability to identify common breastfeeding problems. Each nurse was asked to list 5 to 10 problems con- cerning breastfeeding that breastfeeding primiparas
November/December 1973 IOGN Nursing
are most likely to encounter during the first six weeks following hospital discharge. One point was given for each breastfeeding problem that was also included on Disbrow’s list. No points were given for breastfeeding problems that were not included on Disbrow’s list. The maximum possible score was 7 . The range of problems correctly identified by the nurses was 0 to 4. Only 2 nurses identified as many as 4 problems, 10 identified 1 problem, and 4 did not identify any of Disbrow’s common problems. In other words, 2 5 of the 29 nurses identified 2 or less of the 7 Disbrow prob- lems and approximately half of the nurses (14) identified 1 or 0 of the 7 problems.
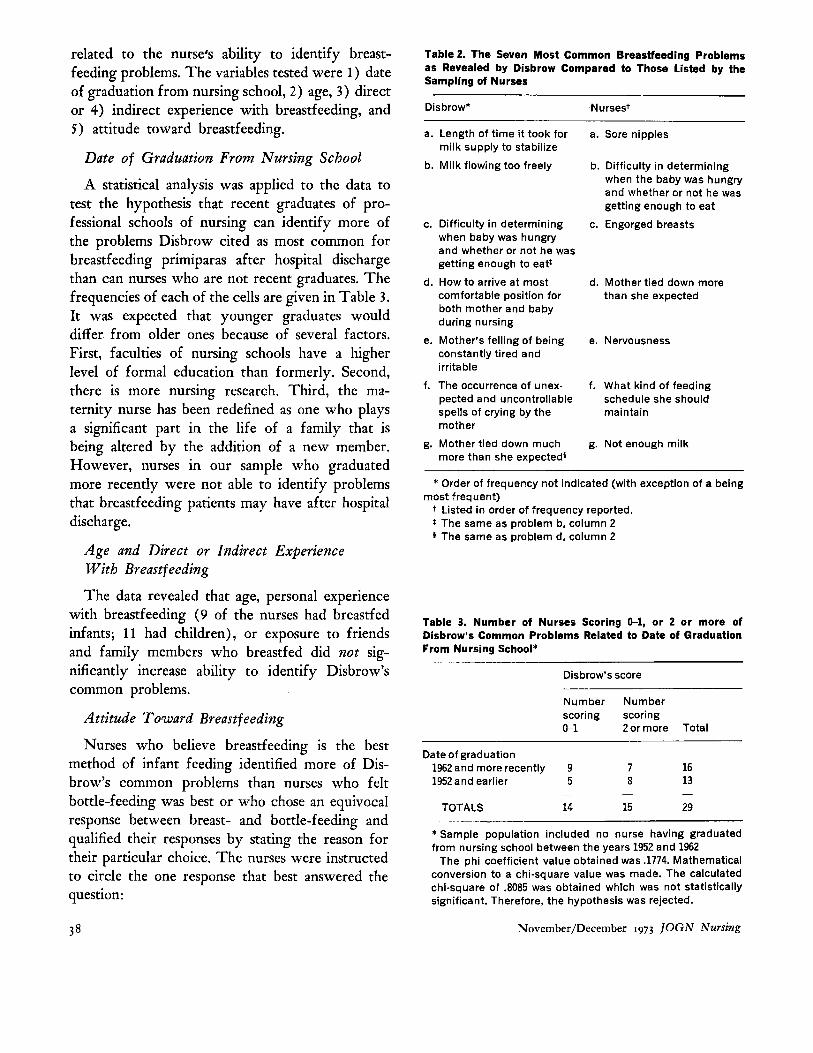
Seventy-two percent of the sample in this study listed sore nipples and 38% listed breast engorge- ment as common breastfeeding problems after dis- charge. These two problems ranked first and third in the frequency of breastfeeding problems as per- ceived by the nurses (Table 2 ) . Neither breast engorgement nor sore nipples were mentioned in Disbrow’s study. Newton has stated that nearly all women have some nipple tenderness until lacta- tion is well established,’ and anyone who has worked in a postpartum unit knows that nipple tenderness can be a problem. Since maternity nurses have little opportunity to evaluate patient needs after the patient is discharged, it seems reasonable that the nurse would believe the patient has the same problems while hospitalized and after dis- charge.
Variables
Part of the questionnaire was designed to deter- mine whether selected variables may be strongly
Table 1. Significance of Difference Between Means of Three Selected Variables for the Three Groups of Nurses
Mean scores
Group A Group B Group C Variables N = l O N = l O N = 9 F*
Disbrow common problem score 1.40 1.50 1.88 0.5435
Date of birth 1930.0 1936.4 1928.6 0.7772 Date of graduation 1951.8 1958.8 1950.0 0.9485
*F .05, 25 = 2.99.
37
related to the nurse’s ability to identify breast- feeding problems. The variables tested were 1 ) date of graduation from nursing school, 2 ) age, 3 ) direct or 4) indirect experience with breastfeeding, and 5) attitude toward breastfeeding.
Date of Graduation From Nursing School
A statistical analysis was applied to the data to test the hypothesis that recent graduates of pro- fessional schools of nursing can identify more of the problems Disbrow cited as most common for breastfeeding primiparas after hospital discharge than can nurses who are not recent graduates. The frequencies of each of the cells are given in Table 3. It was expected that younger graduates would differ from older ones because of several factors. First, faculties of nursing schools have a higher level of formal education than formerly. Second, there is more nursing research. Third, the ma- ternity nurse has been redefined as one who plays a significant part in the life of a family that is being altered by the addition of a new member. However, nurses in our sample who graduated more recently were not able to identify problems that breastfeeding patients may have after hospital discharge.
Age and Direct or Indirect Experience W i t h Breastfeeding
The data revealed that age, personal experience with breastfeeding (9 of the nurses had breastfed infants; 1 1 had children), or exposure to friends and family members who breastfed did not sig- nificantly increase ability to identify Disbrow’s common problems.
Attitude Toward Breastfeeding
Nurses who believe breastfeeding is the best method of infant feeding identified more of Dis- brow’s common problems than nurses who felt bottle-feeding was best or who chose an equivocal response between breast- and bottle-feeding and qualified their responses by stating the reason for their particular choice. The nurses were instructed to circle the one response that best answered the question:
Table 2. The Seven Most Common Breastfeeding Problems as Revealed by Disbrow Compared to Those Listed by the Sampling of Nurses
Dis brow*
a. Length of time it took for milk supply to stabilize
b. Milk flowing too freely
c. Difficulty in determining when baby was hungry and whether or not he was getting enough to eat:
d. How to arrive at most comfortable position for both mother and baby during nursing
e. Mother’s felling of being constantly tired and irritable
f. The occurrence of unex- pected and uncontrollable spells of crying by the mother
g. Mother tied down much more than she expected$
.Nursest
a. Sore nipples
b. Difficulty in determining when the baby was hungry and whether or not he was getting enough to eat
c. Engorged breasts
d. Mother tied down more than she expected
e. Nervousness
f. What kind of feeding schedule she should maintain
g. Not enough milk
* Order of frequency not indicated (with exception of a being
t Listed in order of frequency reported. * The same as problem b, column 2
The same as problem d, column 2
most frequent)
Table 3. Number of Nurses Scoring 0-1, or 2 or more of Disbrow’s Common Problems Related to Date of Graduation From Nursing School*
Disbrow’s score
Number Number scoring scoring 0-1 2 or more Total
Date of graduation 1962 and more recently 9 7 16 1952 and earlier 5 8 13
TOTALS 14 15 29 - _-__
* Sample population included no nurse having graduated from nursing school between the years 1952 and 1962
The phi coefficient value obtained was .1774. Mathematical conversion to a chi-square value was made. The calculated chi-square of .8085 was obtained whlch was not statistically significant. Therefore, the hypothesis was rejected.
Novernber/Decernber 1973 ]OGN Nursing 38

What do you believe is the best kind of infant feeding? breast bottle other (explain)
Nineteen of the 29 nurses selected breastfeeding, 3 selected bottle-feeding, and the other 7 chose the “other” response. Statistical analysis revealed that the 19 who selected breastfeeding were statistically different in relation to Disbrow’s score. Nurses who definitely favor breastfeeding as the method of choice for infant feeding are more able to identify Disbrow’s common problems than nurses who do not definitely favor breastfeeding.
DISCUSSION Three major limitations of this study make it
necessary to view some findings with caution. First, the sampling was small. Second, it was limited to maternity nurses who were employed in the hospital at least three months, but the total time of employment in maternity nursing was not ascer- tained. A third limitation is the assumption that Disbrow’s common problems were valid for all primiparas.
Approximately half of the nurses in our sampling expressed concern because they did not know, or had not thought about, breastfeeding problems that mothers may have after hospital discharge. Among their comments were:
“We never see patients after they are discharged.” “I should have read more books on breast-
feeding.” “I just never thought about this. It’s something
that is important for nurses to know.” “A couple of my friends have breastfed but it’s
hard to remember what kind of problems they had.”
These comments and the data collected from our small sampling point to a deficiency in nursing education.
There is little information about common breast- feeding problems in textbooks on maternity nurs- ing,!’-13 and the authors usually focus on compli- cations such as sore nipples and breast engorgement. These were included in the problems the nurses listed as “most common” (Table 2 ) , so they are probably familiar with the information in the texts.
Information on identification of breastfeeding problems which are likely to occur after discharge and appropriate anticipatory guidance by the nurse should be included in the texts or otherwise pre- sented a t some time during the nurse’s formal education.
REFERENCES 1. Disbrow, M.: “Nursing Intervention as a Factor in
Successful Breast-Feeding,” Evaluation of Nursing Intervention. Convention Clinical Sessions, American Nurses Association, Monograph 4:5-12, 1964
2. Wessel, M. A.: “Maternal and Child Nursing-As a Pediatrician Sees It.” NUTS Outlook 11:207-210, 1963
3. Branin, V.: “A Study of Problems Encountered by Twenty-Six Nursing Mothers Following Hospital Discharge,” Evaluation of Nursing Intervention. Convention Clinical Sessions, American Nurses Association, Monograph 4: 13-1 8, 1964
by Primiparas: Attitudinal Factors and Extraneous Influences.” Psychosom Med 22:421-429, 1960
61:554-556, 1965
Regarding Infant Care Activities.” Nurs Res 12 (2) :72-77, 1963
Feeding.” Child and Family 2:4-12, 1963
Management of Lactation.” Clin Obstet Gynecol 5:49-63, 1962. (Reprinted in Maternal Health Nursing. Edited by N. Lytle. Dubuque, Iowa, Wm. C. Brown Company Publishers, 1967, pp. 108-125)
9. Bookmiller, M., G. Bowen, and D. Carpenter: Textbook of Obstetrics and Obstetric Nursing. Fifth edition. Philadelphia, W. B. Saunders Co., 1967
10. Davis, E., and R. Rubin: DeLee’s Obstetrics For Nurses. 17th edition. Philadelphia, W. B. Saunders Co., 1963
11. Fitzpatrick, E., N. Eastman, and S. Reeder: Maternity Nursing. Philadelphia, J. B. Lippincott Co., 1964
12. Wiedenbach, E.: Family Centered Maternity Nursing. Second edition. New York, G. P. Putnam’s Sons, 1967
13. Ziegel, E., and C. Van Blarcom: Obstetric Nursing. Fifth edition. New York, T h e Macmillan Co., 1964
4. Brown, F., et al.: “Studies in Choice of Infant Feeding
5. Burnett, C. W. F.: “Breast Feeding Today.” NUTS Times
6. Adams, M.: Early Concerns of Primigravida Mothers
7. Salber, E., P. Stitt, and J. Babbitt: “Patterns of Breast
8. Newton, M., and N. Newton: “The Normal Course and
Address reprint requests to Patricia Estok, RN, Assistant Professor, School of Nursing, Kent State University, Kent, OH 44240.
Patricia Estok, RN, is an Assistant Professor in the School of Nursing of Kent State University, Kent , Ohio; T h e N A A C O G member graduated from Washington (Pennsylvania) Hospital School of Nursing and holds BSN and MSN degrees in Maternity Nursing from Case Western Reserve University in Cleveland, Ohio.
November/December 1973 JOGN Nursing 39