Embed Size (px)
Citation preview

This article was downloaded by: [Pennsylvania State University]On: 12 August 2014, At: 03:14Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Journal of Workplace Behavioral HealthPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/wjwb20
Who Do We Serve?Rick Csiernik PhD, RSW a , Scott Macdonald PhD b , Pierre DurandPhD c , T. Cameron Wild PhD d & Margaret Rylett MA ea School of Social Work , King's University College at the Universityof Western Ontariob Universtity of Victoria, Centre for Addictions Researchc University of Montreald University of Alberta, Centre for Addiction and Mental Healthe Centre for Addiction and Mental HealthPublished online: 22 Sep 2008.
To cite this article: Rick Csiernik PhD, RSW , Scott Macdonald PhD , Pierre Durand PhD , T. CameronWild PhD & Margaret Rylett MA (2006) Who Do We Serve?, Journal of Workplace Behavioral Health,21:2, 15-29, DOI: 10.1300/J490v21n02_02
To link to this article: http://dx.doi.org/10.1300/J490v21n02_02
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoever orhowsoever caused arising directly or indirectly in connection with, in relation to or arisingout of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
Who Do We Serve?Worksite Characteristics,
Workforce Attributesand Occupational Assistance
Programming in Canada
Rick CsiernikScott MacdonaldPierre Durand
T. Cameron WildMargaret Rylett
ABSTRACT. One component of a 2003 national cross sector survey ofCanadian organizations with 100 or more employees was an assessmentof whether occupational assistance programs were mechanisms of socialcontrol or additional employee benefits of those already economicallyprivileged. Employee Assistance Programs (EAPs) were the most com-mon form of assistance provided, followed by health promotion initia-tives and drug testing programs, though only EAPs were found in themajority of workplaces studied. Organizations that scored higher inmanagement control and employee involvement were significantly
Rick Csiernik, PhD, RSW, is affiliated with the School of Social Work, King’s Uni-versity College at the University of Western Ontario. Scott Macdonald, PhD, isaffiliated with the Universtity of Victoria, Centre for Addictions Research. PierreDurand, PhD, is affiliated with the University of Montreal. T. Cameron Wild, PhD, isaffiliated with the University of Alberta and the Centre for Addiction and MentalHealth. Margaret Rylett, MA, is affiliated with the Centre for Addiction and MentalHealth.
Address correspondence to: Rick Csiernik, PhD, RSW, School of Social Work,King’s University College at the University of Western Ontario, c/o 125 East 8th Street,Hamilton, Ontario, L9A 4Y7 (E-mail: [email protected]).
Journal of Workplace Behavioral Health, Vol. 21(2) 2005Available online at http://www.haworthpress.com/web/JWBH
© 2005 by The Haworth Press, Inc. All rights reserved.doi:10.1300/J490v21n02_02 15
Dow
nloa
ded
by [
Penn
sylv
ania
Sta
te U
nive
rsity
] at
03:
14 1
2 A
ugus
t 201
4

(p < 0.001) less likely to have an EAP and health promotion programmingcompared with those companies with greater scores in employee involve-ment. An inverse relationship between employee involvement and theestablishment of a drug testing program was close to significant(p < 0.10). Organizations that employed a greater proportion of personsof colour and female employees were the least likely to have an EAP.[Article copies available for a fee from The Haworth Document Delivery Ser-vice: 1-800-HAWORTH. E-mail address: <[email protected]>Website: <http://www.HaworthPress.com> © 2005 by The Haworth Press, Inc.All rights reserved.]
KEYWORDS. Employee Assistance Programming (EAP), health pro-motion, drug testing, privilege, social control
INTRODUCTION
We have some knowledge of the prevalence and characteristics ofoccupational assistance programming, particularly Employee AssistancePrograms (EAPs) in Canada (Csiernik, 2002; Macdonald, 2005; Mac-donald et al., 1990, 1994), the United Kingdom (Arthur, 2002; Highley-Marchington et al., 1997; Marlow, 1991), South Africa (Du Plessis,1992; Harper, 1999; Maiden, 1992; Terblanche, 1992) and the UnitedStates (Hartwell et al., 1996) along with various analysis of the costs ofthese programs (Bray et al., 1996; French et al., 1997, 1998), and theiroutcomes (Csiernik, 1995a, 1998, 2004; Jerrell et al., 1982; Kurtz et al.,1984). However, another question of equal merit is: Who do these pro-grams actually serve?
There has been a long-standing argument that EAPs and related pro-grams are merely programs of social control (Corneil, 1984; Csiernik,1996; Pace, 1990; Roman, 1980). Those with this orientation view oc-cupational assistance as acting in the interest of the owners of the meansof production to influence workers towards conforming to establishedbehaviours and norms in order to maximize productivity and profit inthe workplace (Armitage, 1996). Some have suggested that occupa-tional assistance is, in fact, a privatized form of health care benefitingalready economically privileged workers and, thus, further eroding ac-cess to or development of universal health care initiatives (Tudiver,1993) while underserving marginalized populations (Howell et al., 1998;Jackson et al., 2002; Karuntzos et al., 1998; McKinney Jackson, 1994;Van Den Bergh, 1999). A third argument can be made that EAPs are
16 JOURNAL OF WORKPLACE BEHAVIORAL HEALTH
Dow
nloa
ded
by [
Penn
sylv
ania
Sta
te U
nive
rsity
] at
03:
14 1
2 A
ugus
t 201
4

benefits that employees endorse. If this later argument is true then wemight expect that worksites with EAPs are more likely to have a work-place culture with less management control over decisions and moreemployee involvement.
Historically occupational assistance in North America, in the form ofWelfare Capitalism, began by ensuring that young single women wereliving in virtuous Christian environments through building separatedormitories for female employees and hiring welfare secretaries tooversee their activities. Occupational assistance also emerged in theform of company towns with dry zones so that employed male labourerswould not drink too much and as programs to properly acculturatenewly arrived immigrants to a new continent and to the North Americanindustrial work environment (Brandes, 1976; McGilly, 1985; Popple,1981; Trice et al., 1988, 1985; Thomlison, 1983). However, with theevolution of occupational assistance to broad brush EAPs, greater num-bers of white collar workers and professionals have gained increasingaccess to this form of assistance through the latter half of the 20th cen-tury (Csiernik et al., 2001; Gladstone et al., 1999; Sciegaj et al., 2001).Nonetheless, it is still argued by some that the primary focus of occupa-tional assistance programs remains on fixing individuals rather thanexamining larger organizational and structural issues that equally con-tribute to negatively affecting worker wellness (Csiernik, 1995b).
Workplace health promotion programming, a combination of educa-tional, organizational, economic and environmental activities was de-signed to support positive health maintenance behaviours conducive tothe well-being of employees and their families (Parkinson, 1982; Chu,1994). The motive behind this type of occupation assistance program-ming is to identify, prevent, reduce and control physiological and be-havioural health risks before they develop into disabilities or prematuremortality thus negatively affecting both employees and employers.Health promotion programs target employees who are generally func-tioning well but who engage in behaviours that are likely to result inserious illnesses or unproductive work contributions in the future if un-changed, creating additional costs for the organization. Risk avoidanceand risk reduction are the two prominent strategies with risk avoidancedirected towards low-risk populations to inhibit transition to high-riskbehaviours and thereby maintaining existing levels of physical health.Risk reduction is targeted at employees already at risk and is designedto foster a transition to a lower risk or safe status so that illness does notimpact upon organizational outcomes or profits (Erfurt et al., 1992;Goodstadt et al., 1987).
Csiernik et al. 17
Dow
nloa
ded
by [
Penn
sylv
ania
Sta
te U
nive
rsity
] at
03:
14 1
2 A
ugus
t 201
4
In contrast to health promotion is the newest addition to the realm ofoccupational assistance, drug testing. Drug testing is a simplistic andreactive response to the latest “War on Drugs” that was introduced tothe North American workplace during the mid-1980s. It is the programwith the most overt social control role with minimal employee-specificbenefits. Rather than having a preventative or rehabilitative component,the foremost intent of drug testing programs is to eradicate employeedrug use through fear of detection and subsequent employment reper-cussions for failing a test. In Canada, drug testing is rationalized on thebasis of improving work safety; however, in the United States, simplyreducing drug use is a viable purpose. Though there certainly are manycompanies in both countries that have not only drug testing initiativesbut also EAPs and health promotion programs in place. However, alldrug tests do is detect metabolites from psychoactive drugs, both licitand illicit. The testing method is typically conducted through urinalysisoften including visual inspection of sample provision. Most importantto note regarding drug tests is that they cannot indicate physical depend-ency let alone addiction; rather they only indicate use (Csiernik et al.,2003; Macdonald, 2005).
In examining the EAP field, and the subsequent occupational assis-tance options that have evolved, who actually has access to these pro-grams is relatively unknown. Additionally, the underlying philosophy ofan organization, whether it is more attuned to employee involvement incompany decisions or whether it is an organization with a focus on man-agement control, may be a significant contributor to the type and extent ofoccupational assistance programming provided. Thus, the intent of thisstudy is to explore the characteristics of worksites and the various attrib-utes of workforces from across Canada to determine who receives whatform of occupational assistance and in what circumstances.
METHODOLOGY
Sample
The sampling frame was obtained from Dun and Bradstreet of Canada,an international marketing firm, who provided a comprehensive list of allworksites in Canada with 100 or more employees. A stratified systematicsample of these worksites (n = 1110) was drawn from the list, organizedwithin work sectors and provinces to produce a representative sample.In addition, the transportation and communications sector was over-
18 JOURNAL OF WORKPLACE BEHAVIORAL HEALTH
Dow
nloa
ded
by [
Penn
sylv
ania
Sta
te U
nive
rsity
] at
03:
14 1
2 A
ugus
t 201
4

sampled for statistical purposes to increase the proportion of worksitesoffering with drug testing programs. As the study’s intent was to comparethe characteristics of worksites with and without certain occupationalprograms, oversampling in this particular work sector ensured that therewould be adequate cases for statistical analyses.
Data Collection Procedures
Data collection entailed five distinct stages. The first stage entailedcontacting each worksite by telephone to verify the address and obtainthe name of the current human resources manager or the name of themost appropriate alternative, to complete the questionnaire. The secondstage was the actual mailing of the questionnaire. The contact personwas sent a covering letter, a copy of the questionnaire and a stamped,self-addressed envelope. A copy of the cover letter was also forwardedto the president of the organization. This was followed by the first set offollow-up telephone calls, if the questionnaire was not returned afterthree weeks. The follow-up telephone call was made to verify receiptand to encourage the completion and return of the questionnaire. Insome cases, the human resources manager or alternative contact mayhave designated responsibility for completing the questionnaire tosomeone else within the organization such as the occupational healthnurse, EAP co-ordinator or occupational health and safety co-ordinator.In these cases, the name of the new contact was obtained and the personwas telephoned. When the person could not be directly contacted, amessage was left. A minimum of two calls was made in an attempt tomake personal contact. Then, if contact still had not occurred a secondletter was sent, along with another copy of the questionnaire. The letterreiterated the importance of worksite participation in this national sur-vey and assured anonymity. This was followed three weeks later by asecond follow-up telephone call in an effort to yet again make personalcontact. If contact was achieved, an attempt was made to obtain, at aminimum, responses to the three types of programs and the number ofemployees at the worksite. In some cases, respondents were asked allquestions from the questionnaire over the telephone.
Data Collection Instrument
A self-administered questionnaire based on an instrument originallydeveloped in 1989 and revised in 1993 to collect information onworksite health programs in Ontario, Canada (Macdonald et al., 1990,
Csiernik et al. 19
Dow
nloa
ded
by [
Penn
sylv
ania
Sta
te U
nive
rsity
] at
03:
14 1
2 A
ugus
t 201
4

1993) was the basis for the survey instrument. The 2003 questionnaireconsisted primarily of close-ended questions on the existence and char-acteristic of Employee Assistance Programs, drug testing, and healthpromotion activities at each work site. In it were included 49 items de-signed to capture characteristics of the worksite, attitudes about theworksite and attitudes of human resource managers about workplacehealth programs, as well as some data on absenteeism, size of worksiteand organization, use of workplace programs, and level of unionization.
Response Rate
Of the 1110 surveys that were distributed, 819 were eligible for thestudy. Those that were not eligible (n = 291) were no longer in business,had less than 100 employees or could not be reached by letter or tele-phone. Of the 819 eligible worksites, 638 completed the questionnairewhile 181 refused. Of the 638 who completed the questionnaire, 172 didso by telephone and gave, at a minimum, responses to only three majorprogram questions and the number of employees. This represents a re-sponse rate of 77.9% for the study.
Analysis
The goal of the analysis was to compare mean values on a variety oforganizational characteristics across worksites with and without occu-pational assistance programs. Frequencies were performed on the vari-ables related to the three different types of workplace programs. Assome of this information was obtained by telephone and was incompletefor the health promotion programs when the contact person indicatedthe worksite had health promotion programs but did not specify any, itwas necessary to impute responses for specific programs. Thus, for esti-mates of this group, the distribution of responses given by those whofully completed the question was used.
A factor analysis of the 20 items on the job characteristics of the worksite was conducted to determine which items were related to the threethemes of interest: (1) Level of management control, (2) amount of em-ployee involvement, and (3) worker drinking. Respondents, using afive- point Likert scale from 1 “strongly disagree,” to 5 “strongly agree,”rated each of the items. The factor analysis reduced the eight manage-ment control items to six, employee involvement items from eight tofour and worker drinking from four to three. Reliabilities were assessedon three factors. The items in each factor along with their corresponding
20 JOURNAL OF WORKPLACE BEHAVIORAL HEALTH
Dow
nloa
ded
by [
Penn
sylv
ania
Sta
te U
nive
rsity
] at
03:
14 1
2 A
ugus
t 201
4

Cronbach alphas are presented in Table 1 with employee involvementhaving the strongest reliability and worker drinking, the weakest.Frequencies, correlations, t-tests, and the chi-square statistic were per-formed using these three factors and several variables of interest.
The score range for the factor management control was from six tothirty with a higher score indicating a more authoritarian style of man-agement. The score range for the factor employee involvement wasfrom four to twenty and measured employee participation in companydecisions. The score range for the factor worker drinking was fromthree to fifteen and measured the extent to which use of alcohol, on oroff the worksite, was common. Employee involvement and manage-ment control were found to be negatively correlated (p < 0.001) as wasexpected, since authoritative and participatory styles of managementare antithetical. Three types of statistical analyses were conducted: chi-square tests for two categorical variables, t-tests to compare means oftwo groups, and correlations to compare two variables with continuousmeasures.
RESULTS
The participating worksites were proportionally distributed acrossCanada by work sector and province as illustrated in Tables 2 and 3.
Csiernik et al. 21
TABLE 1. Factor Items
Management control (alpha = .527) (5 items)
1. Most employees who work here are supervised closely.2. Management provides strong direction over employee’s work.3. Authority for decision-making rests with a few individuals.4. Employees cannot work flexible hours.5. Job sharing is not possible.
Employee involvement (alpha = .638) (4 items)1. At this worksite major rewards are based on performance effectiveness.2. Managers at this worksite make an effort to involve employees in decision-making.3. Communication between managers and employees is good.4. People who work here are very sensitive toward others.
Worker drinking (alpha = .298) (3 items)1. Employees are permitted to drink alcohol at some team meetings.2. Many team groups drink after work.3. Alcohol use among employees is a problem at this worksite.
Dow
nloa
ded
by [
Penn
sylv
ania
Sta
te U
nive
rsity
] at
03:
14 1
2 A
ugus
t 201
4
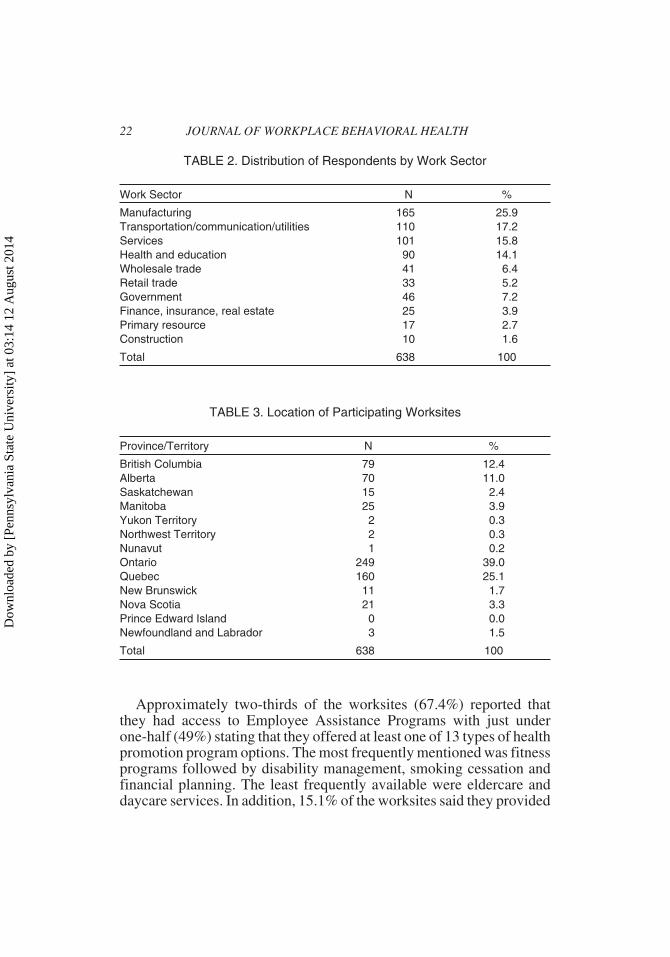
Approximately two-thirds of the worksites (67.4%) reported thatthey had access to Employee Assistance Programs with just underone-half (49%) stating that they offered at least one of 13 types of healthpromotion program options. The most frequently mentioned was fitnessprograms followed by disability management, smoking cessation andfinancial planning. The least frequently available were eldercare anddaycare services. In addition, 15.1% of the worksites said they provided
22 JOURNAL OF WORKPLACE BEHAVIORAL HEALTH
TABLE 2. Distribution of Respondents by Work Sector
Work Sector N %
Manufacturing 165 25.9Transportation/communication/utilities 110 17.2Services 101 15.8Health and education 90 14.1Wholesale trade 41 6.4Retail trade 33 5.2Government 46 7.2Finance, insurance, real estate 25 3.9Primary resource 17 2.7Construction 10 1.6
Total 638 100
TABLE 3. Location of Participating Worksites
Province/Territory N %
British Columbia 79 12.4Alberta 70 11.0Saskatchewan 15 2.4Manitoba 25 3.9Yukon Territory 2 0.3Northwest Territory 2 0.3Nunavut 1 0.2Ontario 249 39.0Quebec 160 25.1New Brunswick 11 1.7Nova Scotia 21 3.3Prince Edward Island 0 0.0Newfoundland and Labrador 3 1.5
Total 638 100
Dow
nloa
ded
by [
Penn
sylv
ania
Sta
te U
nive
rsity
] at
03:
14 1
2 A
ugus
t 201
4
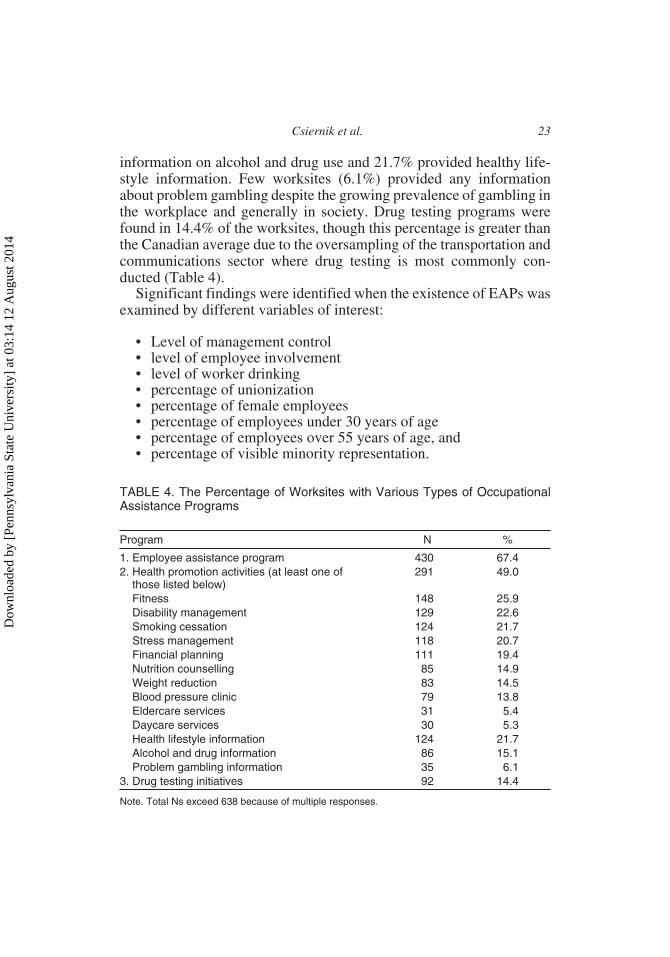
information on alcohol and drug use and 21.7% provided healthy life-style information. Few worksites (6.1%) provided any informationabout problem gambling despite the growing prevalence of gambling inthe workplace and generally in society. Drug testing programs werefound in 14.4% of the worksites, though this percentage is greater thanthe Canadian average due to the oversampling of the transportation andcommunications sector where drug testing is most commonly con-ducted (Table 4).
Significant findings were identified when the existence of EAPs wasexamined by different variables of interest:
• Level of management control• level of employee involvement• level of worker drinking• percentage of unionization• percentage of female employees• percentage of employees under 30 years of age• percentage of employees over 55 years of age, and• percentage of visible minority representation.
Csiernik et al. 23
TABLE 4. The Percentage of Worksites with Various Types of OccupationalAssistance Programs
Program N %
1. Employee assistance program 430 67.42. Health promotion activities (at least one of
those listed below)291 49.0
Fitness 148 25.9Disability management 129 22.6Smoking cessation 124 21.7Stress management 118 20.7Financial planning 111 19.4Nutrition counselling 85 14.9Weight reduction 83 14.5Blood pressure clinic 79 13.8Eldercare services 31 5.4Daycare services 30 5.3Health lifestyle information 124 21.7Alcohol and drug information 86 15.1Problem gambling information 35 6.1
3. Drug testing initiatives 92 14.4
Note. Total Ns exceed 638 because of multiple responses.
Dow
nloa
ded
by [
Penn
sylv
ania
Sta
te U
nive
rsity
] at
03:
14 1
2 A
ugus
t 201
4
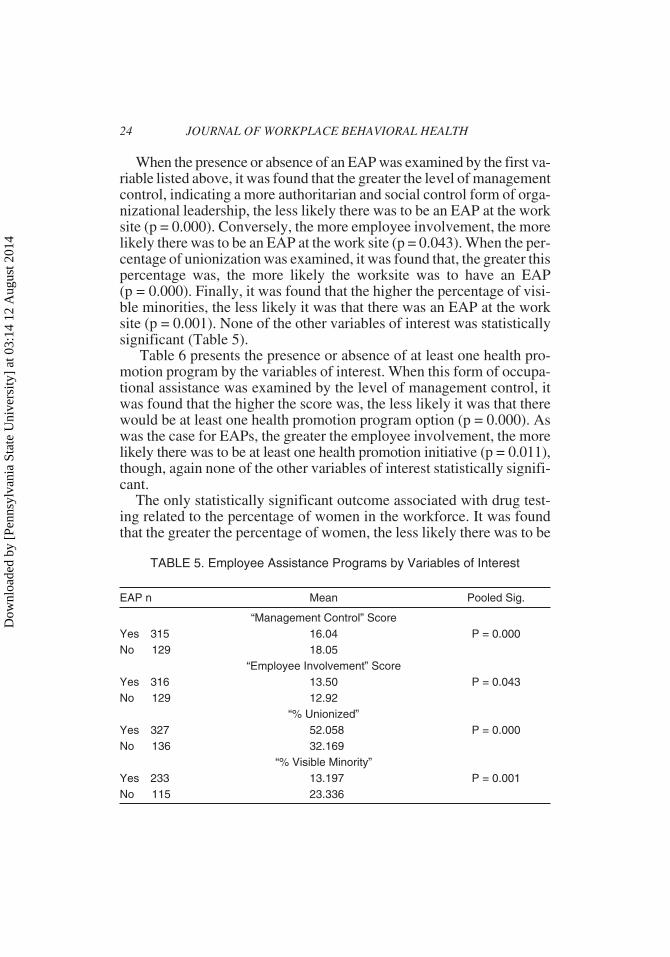
When the presence or absence of an EAP was examined by the first va-riable listed above, it was found that the greater the level of managementcontrol, indicating a more authoritarian and social control form of orga-nizational leadership, the less likely there was to be an EAP at the worksite (p = 0.000). Conversely, the more employee involvement, the morelikely there was to be an EAP at the work site (p = 0.043). When the per-centage of unionization was examined, it was found that, the greater thispercentage was, the more likely the worksite was to have an EAP(p = 0.000). Finally, it was found that the higher the percentage of visi-ble minorities, the less likely it was that there was an EAP at the worksite (p = 0.001). None of the other variables of interest was statisticallysignificant (Table 5).
Table 6 presents the presence or absence of at least one health pro-motion program by the variables of interest. When this form of occupa-tional assistance was examined by the level of management control, itwas found that the higher the score was, the less likely it was that therewould be at least one health promotion program option (p = 0.000). Aswas the case for EAPs, the greater the employee involvement, the morelikely there was to be at least one health promotion initiative (p = 0.011),though, again none of the other variables of interest statistically signifi-cant.
The only statistically significant outcome associated with drug test-ing related to the percentage of women in the workforce. It was foundthat the greater the percentage of women, the less likely there was to be
24 JOURNAL OF WORKPLACE BEHAVIORAL HEALTH
TABLE 5. Employee Assistance Programs by Variables of Interest
EAP n Mean Pooled Sig.
“Management Control” ScoreYes 315 16.04 P = 0.000No 129 18.05
“Employee Involvement” ScoreYes 316 13.50 P = 0.043No 129 12.92
“% Unionized”Yes 327 52.058 P = 0.000No 136 32.169
“% Visible Minority”Yes 233 13.197 P = 0.001No 115 23.336
Dow
nloa
ded
by [
Penn
sylv
ania
Sta
te U
nive
rsity
] at
03:
14 1
2 A
ugus
t 201
4
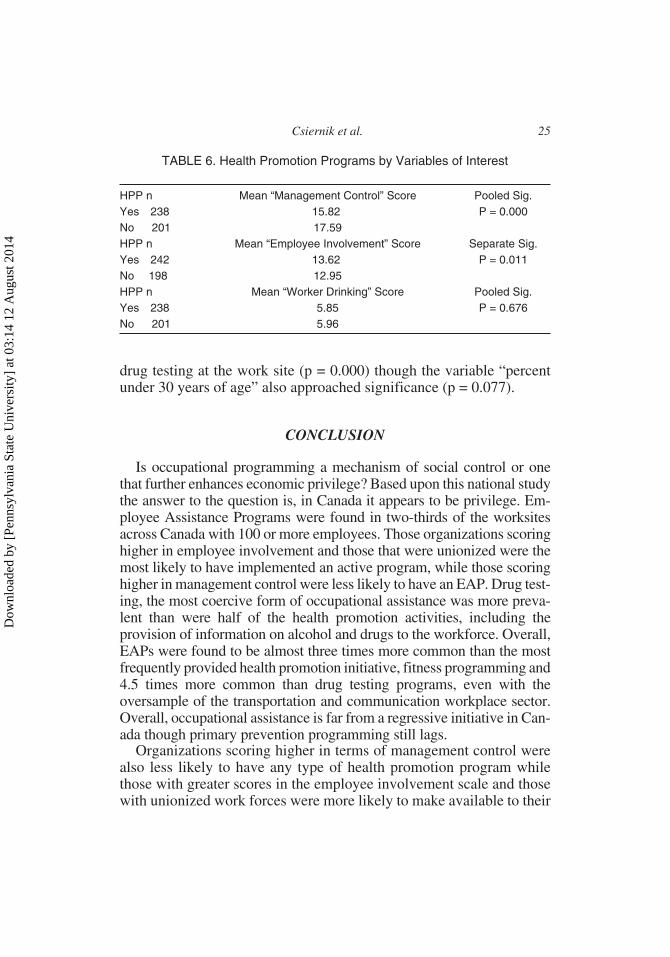
drug testing at the work site (p = 0.000) though the variable “percentunder 30 years of age” also approached significance (p = 0.077).
CONCLUSION
Is occupational programming a mechanism of social control or onethat further enhances economic privilege? Based upon this national studythe answer to the question is, in Canada it appears to be privilege. Em-ployee Assistance Programs were found in two-thirds of the worksitesacross Canada with 100 or more employees. Those organizations scoringhigher in employee involvement and those that were unionized were themost likely to have implemented an active program, while those scoringhigher in management control were less likely to have an EAP. Drug test-ing, the most coercive form of occupational assistance was more preva-lent than were half of the health promotion activities, including theprovision of information on alcohol and drugs to the workforce. Overall,EAPs were found to be almost three times more common than the mostfrequently provided health promotion initiative, fitness programming and4.5 times more common than drug testing programs, even with theoversample of the transportation and communication workplace sector.Overall, occupational assistance is far from a regressive initiative in Can-ada though primary prevention programming still lags.
Organizations scoring higher in terms of management control werealso less likely to have any type of health promotion program whilethose with greater scores in the employee involvement scale and thosewith unionized work forces were more likely to make available to their
Csiernik et al. 25
TABLE 6. Health Promotion Programs by Variables of Interest
HPP n Mean “Management Control” Score Pooled Sig.Yes 238 15.82 P = 0.000No 201 17.59HPP n Mean “Employee Involvement” Score Separate Sig.Yes 242 13.62 P = 0.011No 198 12.95HPP n Mean “Worker Drinking” Score Pooled Sig.Yes 238 5.85 P = 0.676No 201 5.96
Dow
nloa
ded
by [
Penn
sylv
ania
Sta
te U
nive
rsity
] at
03:
14 1
2 A
ugus
t 201
4

employees health promotion options. Workplaces with younger work-ers and with a greater emphasis on management control were margin-ally more likely to have a drug testing program (p < 0.10).
While there is an extensive history and anecdotal evidence to supportthe hypothesis that occupational assistance is a form of social controlthis was not found in this study of Canadian EAPs. There is moreevidence provided by the research that occupational assistance is a priv-ileged benefit including the finding that historically marginalizedgroups, visible minorities, were still, in 2003, less likely to work in anorganized work environment and have access to these occupational pro-grams. A definite unequal distribution of resources based upon demo-graphic characteristics of workplace populations was found. If you arean employed person of colour or do not belong to a union in Canadathere is less likelihood that your workplace would have established anEAP. This perhaps is the most ironic finding of the research as two tar-get groups for whom the initial occupational assistance programming inNorth America, Welfare Capitalism, was intended were young femaleworkers and new immigrants.
The study has provided some empirical clarity regarding whomoccupational assistance programs are benefiting and under what cir-cumstances. Canadian EAPs of the 21st century are more likely to bevoluntary with less direct management involvement and overt control.However, perhaps the most disappointing finding of the entire study re-mains that of frequency. Entering the third century of the provision ofoccupational assistance in Canada it is unfortunate that not all employedCanadians and their dependants have access to the entire range of posi-tive occupational programming initiatives. EAP and related occupa-tional programming in Canada have moved away from being or at leastbeing perceived as a mechanism of social control. The next goal shouldbe to move occupational assistance away from being or at least beingperceived as being a privilege and making it more integrated into work-place life and thus more aligned with the philosophy of the Canadianhealth care system, that of a universal benefit.
REFERENCES
Armitage, A. (1996). Social welfare in Canada revisited: facing up to the future. DonMills, Ontario: Oxford University Press.
Arthur, R. (2002). Mental health problems and British workers: a survey of mentalhealth problems in employees who receive counselling from Employee AssistanceWorkers. Stress and Health, 18(2), 69-74.
26 JOURNAL OF WORKPLACE BEHAVIORAL HEALTH
Dow
nloa
ded
by [
Penn
sylv
ania
Sta
te U
nive
rsity
] at
03:
14 1
2 A
ugus
t 201
4

Brandes, S. (1976). American Welfare Capitalism, 1880-1940. Chicago: University ofChicago Press.
Bray, J., French, M., Bowland, B. & Dunlap, J. (1996). The cost of Employee Assis-tance Programs (EAPs): findings from seven case studies. Employee AssistanceQuarterly, 11(4), 1-19.
Chu, C. (1994). An integrated approach to workplace health promotion. In C. Chu &R. Simpson (Eds.). Ecological public health: from vision to practice. Toronto:ParticipACTION.
Corneil, W. (1984). History, philosophy and objectives of an employee recoveryprogram. In W. Albert, B. Boyle, & C. Ponee (Eds.). EAP Orientation: Volume II–Important Concepts. Toronto: Addiction Research Foundation.
Csiernik, R. (1995a). A review of research methods used to examine Employee Assis-tance Program delivery options. Evaluation and Program Planning, 18(1), 25-36.
Csiernik, R. (1995b). Wellness, work and Employee Assistance Programming. Em-ployee Assistance Quarterly, 11(2), 1-13.
Csiernik, R. (1996). Occupational social work: from social control to social assistance?The Social Worker, 64(3), 67-74.
Csiernik, R. (1998). A profile of Canadian Employee Assistance Programs. EmployeeAssistance Research Supplement, 2(1), 1-8.
Csiernik, R. (2002). An overview of Employee and Family Assistance Programming inCanada. Employee Assistance Quarterly, 18(1), 17-34.
Csiernik, R. (2004). A review of EAP evaluation in the 1990s. Employee AssistanceQuarterly, 19(4), 21-38.
Csiernik, R., Atkinson, B., Cooper, R., Devereux, J. & Young, M. (2001) An examina-tion of a combined internal-external program: the St. Joseph’s health centre em-ployee counselling service. Employee Assistance Quarterly, 16(3), 37-48.
Csiernik, R. & Gorlick, C. (2003). Drug testing, employability and welfare,pp. 293-309. In R. Csiernik & W.S. Rowe (Eds.). Responding to the Oppression ofAddiction: Canadian Social Work Perspectives. Toronto: Canadian Scholars Press.
Du Plessis, A. (1992). EAPs in South Africa: a macro model. Employee AssistanceQuarterly, 7(3), 29-43.
Erfurt, J., Foote, A. & Heirich, M. (1992). Integrating Employee Assistance andwellness: current and future core technologies of a megabrush program. Journal ofEmployee Assistance Research, 1(1), 1-31.
French, M., Dunlap, L., Zarkin, G. & Karuntzos, G. (1998). The costs of an enhancedEmployee Assistance Program (EAP) intervention. Evaluation and Program Plan-ning, 21(4), 227-236.
French, M., Zarkin, G., Bray, J. & Hartwell, T. (1997). Costs of Employee AssistancePrograms: findings from a national survey. American Journal of Health Promotion,11(3), 219-222.
Gladstone, J. & Reynolds, T. (1999). Responding to changing corporate paradigms: therole of EAP group work in promoting self-reliant clients. Employee AssistanceQuarterly, 14(4), 53-63.
Goodstadt, M., Simpson, R. & Loranger, P. (1987). Health promotion: a conceptualintegration. American Journal of Health Promotion, 1(1), 58-63.
Csiernik et al. 27
Dow
nloa
ded
by [
Penn
sylv
ania
Sta
te U
nive
rsity
] at
03:
14 1
2 A
ugus
t 201
4

Harper, T. (1999). Employee Assistance Programming and professional developmentsin South Africa. Employee Assistance Quarterly, 14(3), 1-18.
Hartwell, T., Steele, P., French, M., Potter, F., Rodman, N. & Zarkin, G. (1996). Aidingtroubled employees: the prevalence, cost and characteristics of Employee Assis-tance Programs in the United States. American Journal of Public Health, 86(6),804-808.
Highley-Marchington, C. & Cooper, C. (1997). An evaluation of Employee Assistanceand workplace counselling programs in the United Kingdom. In M. Carroll andM. Walton (Eds.). Handbook of counselling in organizations. London: SagePublications.
Howell, B., Ivy Fiene, J. & Pinchot Woychik, J. (1998). Employee Assistance implica-tions for Appalachian working-class women from the alcohol and stress researchproject. Employee Assistance Quarterly, 13(4), 55-60.
Jackson, L. & Greene, A. (2002). An EAP treatment paradigm for African Americanwomen. Employee Assistance Quarterly, 18(1), 35-45.
Jerrell, J. & Rightmyer, J. (1982). Evaluating Employee Assistance Programs: a reviewof methods, outcomes, and future directions. Evaluation and Program Planning,5(3), 255-267.
Karuntzos, G., Dunlap, L., Zarkin, G. & French, M. (1998). Designing an EmployeeAssistance Program intervention for women and minorities: lessons from theRockford EAP study. Employee Assistance Quarterly, 14(1), 49-67.
Kurtz, N., Googins, B. & Howard, W. (1984). Measuring the success of occupationalalcoholism programs. Journal of Studies on Alcohol, 45(1), 33-45.
Macdonald, S. (2005). Drug testing in the workplace: issues, answers and the Canadianperspective. In R. Csiernik (Ed.). Wellness and Work. Toronto: Canadian ScholarsPress.
Macdonald, S., Csiernik, R., Durand, P., Rylett, M. & Wild, C. (under review). Cana-dian worksite programs to address employee health.
Macdonald, S. & Dooley, S. (1990). Employee Assistance Programs: emerging trends.Canadian Journal of Community Health, 9(1), 97-106.
Macdonald, S. & Wells, S. (1994). The prevalence and characteristics of EAPs, healthpromotion and drug testing programs in Ontario. Employee Assistance Quarterly,10(1), 25-60.
Maiden, R. P. (1992). First world EAPs serving third world clients: A U.S. Perspectiveof the South Africa experience. Employee Assistance Quarterly, 7(3), 1-15.
Marlow, C. (1991). Occupational social work and Employee Assistance Programs inGreat Britain. Employee Assistance Quarterly, 7(1), 19-24.
McGilly, F. (1985). American historical antecedents to industrial social work. SocialWork Papers of the School of Social Work, University of Southern California, 19,1-13.
McKinney Jackson, B. (1994). African-American women in the workplace: A personalperspective from African-American female EAPs. Employee Assistance Quarterly,9(3/4), 11-19.
Pace, E. (1990). Peer Employee Assistance Programs for nurses. Perspectives on Ad-dictions Nursing, 1(4), 3-7.
28 JOURNAL OF WORKPLACE BEHAVIORAL HEALTH
Dow
nloa
ded
by [
Penn
sylv
ania
Sta
te U
nive
rsity
] at
03:
14 1
2 A
ugus
t 201
4

Parkinson, R.S. (1982). Managing health promotion in the workplace. Palo Alto, Ca.:Mayfield.
Popple, P. (1981). Social work practice in business and industry, 1875-1930. SocialService Review, 55, 257-269.
Roman, P. (1980). Medicalization and social control in the workplace: prospects forthe 1980s. Journal of Applied Behavioural Science, 16(3), 407-422.
Sciegaj, M., Garnick, D., Horgan, C., Merrick, E., Goldin, D., Urato, M. & Hodgkin, D.(2001). Employee Assistance Programs among Fortune 500 companies. EmployeeAssistance Quarterly, 16(3), 25-35.
Terblanche, L. (1992). The state of the art of EAPs in South Africa: a critical analysis.(1992). Employee Assistance Quarterly, 7(3), 17-28.
Thomlison, R. (1983). Industrial social work: perspectives and issues. Perspectives onIndustrial Social Work. Toronto: Family Service Canada.
Trice, H. & Schonbrunn, M. (1988). A history of job-based alcoholism programs,1900-1955. In F. Dickman, B.R. Challenger, W. Emener & W. Hutchinson, Jr.(Eds.). Employee Assistance Programs: A basic text. Springfield Illinois: CharlesC. Thomas Publisher.
Trice, H. & Sonnenstuhl, W. (1985). Contributions of AA to Employee Assistance Pro-grams. Employee Assistance Quarterly, 1(1), 7-31.
Tudiver, N. (1993). Employee Assistance plans: who benefits? Canadian Review ofSocial Policy, 32 (winter), 74-81.
Van Den Bergh, N. (1999). Workplace problems and needs for lesbian and gay maleemployees: implications for EAPs. Employee Assistance Quarterly, 15(1), 21-60.
Csiernik et al. 29
Dow
nloa
ded
by [
Penn
sylv
ania
Sta
te U
nive
rsity
] at
03:
14 1
2 A
ugus
t 201
4