Embed Size (px)
Citation preview

W O R K E R S ’ C O M P E N S A T I O NQ U I C K D E S K R E F E R E N C E F O R
Claims Management

Workers’ Compensation Quick Desk Reference For Claims Management Overview The OMA Workers’ Compensation Services Account Managers have compiled this Quick Desk Reference. It contains what we consider the top tools necessary to contain the costs of a workplace injury/illness and return your valuable employee safely to work. Lost time claims are the major cost driver of workers’ compensation insurance and can be complicated. Therefore, the Account Managers’ number one rule of thumb: notify us immediately when lost work days are a fact of an injury or illness. By communicating directly with your OMA Account Manager, you can coordinate claim management strategies that minimize financial impacts to your company and maximize your employee’s healthy return to work. Enclosed you will find information about these topics:
Investigate every incident: how to do it Claim adjudication and the hearing process, along with your rights to independent
medical exams (IMEs) and private investigations When to pay wages (salary continuation) in lieu of BWC temporary total disability
compensation Use Transitional Work to reduce costs and put your employee on a solid path to
healthy return to work Reduce the costs of existing claims with the Handicap Reimbursement program Eliminate the costs of existing claims using the Lump Sum Settlement procedure Evaluate additional Ohio Bureau of Workers’ Compensation (BWC) cost saving
programs No matter what, OMA Account Managers encourage you to call any time you have questions or concerns and are here to serve you.
Barbara Bender Lead Account Manager [email protected] (614) 629-6833
Georgia Booth Account Manager [email protected] (614) 629-6834
The Ohio Manufacturers' Association Workers’ Compensation Services Account Management Staff

Table of Contents Custom Data & Analyses to Help You Make the Best Decisions 4
Guidelines for Claim Investigation 5
Claim Adjudication and the Hearing Process 11
Salary Continuation 12
BWC $15,000 Medical Program 16
Light Duty 17
Transitional Work 23
Handicap Reimbursement 24
Lump Sum Settlement (LSS) 25

4
Custom Data & Analyses to Help You Make the Best Decisions
We organize your company’s data and provide customized analyses and reports to help inform and support your critical management decisions so you can:
• Predict and manage future workers’ comp costs • Understand and control your specific cost drivers
Each quarter when the BWC releases new claims experience data, we produce a whole new set of updated management reports for your company, including:
• Status of Claims with Handicap Reimbursement Action • Key Drivers of Rates and Premiums • Four-Year Roster of Claims History • Outstanding and Unsettled Claims • Claims Causality Report • And, at appropriate points in the year, we show you your company’s potential savings in
a variety of BWC programs, including deductible, Drug Free Safety Program, and more
This tool shows you which BWC cost-saving programs are compatible with one another.
Easy Access
We generate your company’s analyses and have them online, all the time.
Go to My OMA
1. Use your existing login, or create one 2. Follow online prompts to view reports and authorize others in your company to do so 3. Questions? Contact us at (800) 662-4463 or [email protected]
Due to the sensitive nature of workers’ compensation information, only the OMA’s key contact in your company can authorize your access. Please see him/her to request access. Not sure who the OMA’s key contact is for your company? Call us at (800) 662-4463.

5
Guidelines for Claim Investigation We’ve created a video that describes best practices in claims investigation. Search under Workers’ Compensation Management in the OMA Video Library. My OMA login required. 1. Obtain witness and non-witness statements from appropriate parties.
Witness statements should be obtained as soon as possible following an injury and from only those individuals that were eye witnesses. Collecting witness statements from actual eye witnesses increases the credibility of the statements in the event they are used to defend your position at an Industrial Commission administrative hearing.
Witness statements should include statements about:
WHO In addition to the injured worker, who else was present?
WHAT What did the witnesses see happen (include specific details i.e. weight
and height of objects, distance, machinery, etc.).
WHEN Date and time of injury. Include special circumstances, i.e., beginning of shift, after lunch or break.
WHERE The exact location of the accident, i.e. department, process line, vantage
point – standing, sitting, walking, etc.
HOW How did the incident happen? Be specific regarding events leading up to the incident or immediately following.
Non-witness statements can be just as valuable even if the workers in the vicinity know nothing about the incident; their statements can substantiate work place conditions that were or were not present. Statements can be taken from anyone in the area. Witness and non-witness statements can be handwritten on any piece of paper. If statements are verbal, they can be typed and then signed by the witness. If a claim is questionable, that is, might be contested by any party, original signatures should be notarized when possible. When all incidents and accidents are investigated in the same manner whether or not an injury or medical attention was required at the time, the process is less likely to create an adversarial situation. Keep in mind the injured worker has two years in which to file a claim following an incident.

6
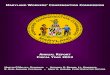
2. Complete an Incident Report.
See OMA’s model Incident Report. This form has been reviewed by legal counsel from Dinsmore & Shohl LLP.

© The Ohio Manufacturers’ Association 2012
Employee Name__________________________________________ SSN _______________________________________
Job Title ________________________________________________ Department _________________________________
Date of Accident _________________________________________ Time of Accident_____________________ AM / PM
What was your job assignment at time of injury? ________________________________________________________________
In the space below, please describe what happened. What were you doing? What equipment, machinery or substanceswere involved? How were you injured? ______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
State the nature of injury (i.e., cut, bruise, burn, sprain, etc.) and the specific part of body injured (i.e., right knee, left index finger, etc.)________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Mark part(s) of body injured with an “X”
Did you seek medical treatment? ❑ Y / ❑ N If yes, when/where? ________________________________________________________________________________________
Have you ever injured this body part(s) previously? ❑ Y / ❑ N If yes, give details (when/where/how/treating physician) __________________________________________________________________________________________________________
List all witnesses to the incident that you are aware of: __________________________________________________________________________________________________________
Did you report the incident to your supervisor ❑ Y / ❑ N If yes, who did you report to? _________________________________________________ Date reported______/______/______If no, why did you not report the incident? ________________________________________________________________________________________________________________________________________________________________________________
MEDICAL RELEASE:I hereby authorize any medical provider to release all medical records pertaining to this injury and/or any prior treatmentrecords to the areas of the body listed above, regardless of date of service.
Employee Signature ____________________________________________________________ Date _____________________
INCIDENT REPORT PART 1 TO BE COMPLETED BY EMPLOYEE
R RLL
FRONT BACK

Employee Name__________________________________________ SSN _____________________________________
Date of Accident _________________________________________ Date Reported ____________________________
Time of Accident _________________________________ AM / PM
Date of Hire______________________________________________ Years on current job ________________________
Last Day Worked _________________________________________ Return-To-Work Date _______________________
Are pictures, sketches or video available? ❑ Y / ❑ N (Attach)
Witnesses to the incident? ❑ Y / ❑ N (Attach statements)
Was first-aid treatment given at the scene? ❑ Y / ❑ N / Offered but refused
Did employee seek medical treatment at an outside facility? ❑ Y / ❑ N
Incident Type (Fall, Slip/Trip, Caught In/Under/Between, Struck Against, etc.):
_______________________________________________________________________________________________________
Nature of Incident (Bruise, Burn, Cut, Fracture, Sprain, etc.):
_______________________________________________________________________________________________________
Body Part (Head, Back, Internal, Lower Limb, Upper Limb, Torso, etc. – LEFT/RIGHT)
_______________________________________________________________________________________________________
Equipment Involved: _____________________________________________________________________________________
Other factors involved (Failure to follow procedures, skill ability deficiency, horseplay, housekeeping, equipment or tools, etc.)_____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Supervisor Signature ___________________________________________________________ Date __________________
What action have you taken and/or do you plan to take to prevent recurrence? Enumerate actions and star (*) those already taken: __________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
What further recommendations or additional comments do you have?_____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Safety Director Signature _______________________________________________________ Date __________________
© The Ohio Manufacturers’ Association 2012
INCIDENT REPORT PART 2 TO BE COMPLETED BY IMMEDIATE SUPERVISOR & SAFETY DIRECTOR
IMM
ED
IAT
E S
UP
ER
VIS
OR
TO
CO
MP
LE
TE
SA
FE
TY
DIR
EC
TO
R T
O C
OM
PL
ET
E

9
3. Obtain a Medical Release
As soon as possible after the incident, collect a medical release from the injured worker in the event we would need to solicit medical records to better understand the injury/illness. We recommend you routinely – on every injury/illness – obtain a Bureau of Workers’ Compensation Form C-101. Making this a standard operational procedure will help diminish any feelings about matters of privacy or harassment on behalf of the injured worker. Click here to obtain BWC Form C-101.

Authorization to ReleaseMedical Information
Address
Injured worker name (first, M.I., last)
Employer name
Date of injury
StateCity
Claim number
Nine-digit ZIP code
I, the above-named injured worker, understand I am allowing the Opportunities for Ohioans with Disabilities and the
providers (persons or facilities) named here (_________________________________________________________________
_____________________________________________________________________________________) that attend or examine me to release the following medical, psychological and/or psychiatric information (excluding psychotherapy notes) that are related causally or historically to physical or mental injuries relevant to my workers’ compensation claim:
• Pathologyslidesandimmunohistochemicalstainingresults,ifapplicable; • Hospitaladmissionhistoryandphysical;emergencyroomreports;hospitaldischargesummaries;physician
officenotes;physicaltherapist,occupationaltherapistorathletictrainerassessmentsandprogressnotes;consultationreports;labresults;medicalreports;surgicalreports;diagnosticreports;procedurereports;nurs-inghomeandskillednursingfacilitiesdocumentation;homenursingprogressnotes;orotherlistedbelow.
____________________________________________________________________________________________________
I understand I am authorizing the release of this information to the following: the Ohio Bureau of Workers’ Com-pensation (BWC), the Industrial Commission of Ohio, the above-named employer, the employer’s managed care organization or qualified health plan and any authorized representatives.
I understand this information is being released to the above-referenced persons and/or entities for use in administering my workers’ compensation claim.
This authorization to release medical, psychological and/or psychiatric information shall remain in effect for as long as my workers’ compensation claim remains open under Ohio law. I understand I have the right to revoke this authorization at any time. However, I must submit my revocation in writing and file it with BWC or my self-insured employer. My decision to revoke this authorization will be effective, except in the case that any provider referenced above already has relied on my authorization and released information.
I understand the provider(s) referenced above may not make my completing and signing this authorization a condition of my treatment.
I understand the parties I am authorizing the release of information to are exempted from the federal privacy require-ments of the Health Insurance Portability and Accountability Act of 1996 as they administer workers’ compensation programs. Information disclosed pursuant to this authorization may be redisclosed by them and may no longer be protected by the federal privacy requirements. I understand such redisclosures may include but are not limited to the following:
• AcopyofthemedicalinformationtheemployerreceivesmaybeforwardedtoBWCbytheemployer;• AcopyofthemedicalinformationwillbeavailabletomeormyphysicianofrecorduponrequesttoBWCor
to the employer.
If signed by the injured worker's guardian or personal representative, provide a description of the guardian
or personal representative’s authority to sign on behalf of the injured worker. ____________________________________________________________________ ___________________________________________________________________________________________________________BWC-1224 (Rev. 9/24/2013)C-101
Injured worker (or guardian or personal representative) signature Date
Employer MCO or QHP
.
Instructions•Pleaseprintortype.•Listtheprovider(s)youareauthorizingtoreleasemedicalrecordsinthespaceindicatedonthisform.•Pleasesignanddatetheform,andsendittothecustomerserviceofficewhereyourclaimislocatedortoyourself-insuredemployer.
You can obtain this form online at ohiobwc.com
.

11
Claim Adjudication and the Hearing Process We’ve created a video that describes the Industrial Commission process for appealed claims. Search under Workers’ Compensation Management in the OMA Video Library. My OMA login required. The Claims Service Specialist (CSS) at the Bureau of Workers’ Compensation is most often the first party to issue a BWC Order to set forth the initial allowance or denial of a claim. Both the injured worker and the employer have the right to appeal this decision, typically within 14 days from the receipt of the order. If appealed, the claim is set for a District Hearing where all parties have the opportunity to present evidence that is relevant to properly adjudicate pending issues. All administrative hearings are conducted “informally” by a hearing officer. The District Hearing Officer (DHO) issues a Record of Proceedings (a decision). If either party disagrees with the District level decision, either party has the right to appeal to the Staff Hearing level, again, generally within 14 days of receipt of the order. The Staff Hearing offers a second opportunity to present relevant information to a Staff Hearing Officer (SHO) and a Record of Proceedings is again issued. Either party has 14 days to appeal to the full Industrial Commission (IC). It is uncommon for the Industrial Commission, or a Deputy of the IC, to hear a third level appeal. The IC generally hears only precedent-setting claims. However, either party can file for Reconsideration of a refused appeal, which generally requires a legal brief to support the appeal. Following this reconsideration decision or the initial refusal, the parties may file most matters (but not extent of disability grievances) into Common Pleas Court within 60 days. All appeal deadlines specified on BWC Orders, Tentative Orders or Records of Proceeding are strictly observed. The District Hearing or the Staff Hearing present the best, and sometimes the only, opportunity to file evidence to support your position. As your TPA, we are required to have your (the employer) permission in order to file for an appeal. Following best practices in collecting witness and non-witness statements, authorizations for the release and solicitation of medical records, independent medical exams or private investigations will enable you to present the most complete evidence for the Hearing Officer’s consideration. Employers have specific rights concerning independent medical examinations (IMEs) and private investigations. Data from IMEs and private investigations are useful during the initial adjudication process, and can also be valuable on an on-going basis once a claim has been allowed to contain future claim costs. Both IMEs and private investigations are a direct expense to the employer. Therefore, careful consideration should be given to their use and usefulness. Your OMA Account Manager can advise you about, and assist you with, obtaining IMEs and private investigations.

12
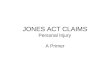
Salary Continuation The employer has the option at the onset of a lost time claim (a lost time claim is defined as a case involving 8 or more lost work days, not necessarily consecutive) to pay the worker’s salary in lieu of BWC temporary total disability compensation by completing a Salary Continuation Agreement (Bureau of Workers’ Compensation Form C-55). This allows the employer to pay regular full wages during periods of certified disability. You must notify the BWC within 7 days of filing a claim that you intend to pay wages in lieu of BWC compensation and the injured worker must not miss a pay check. Note: The C-55 form is to cover only the period of disability currently certified by the treating physician and is not to exceed a duration in excess of 45 days. As updates on the estimated return-to-work date are received, both parties should complete a new C-55 and forward to BWC in a timely manner (within 5 days of expiration of prior form). “Self-insuring” your lost time cost in lieu of BWC temporary total disability compensation will not prevent the establishment of a MIRA reserve on the claim. MIRA (Micro Insurance Reserving Analysis) is the method of calculating reserves that the BWC has adopted. A reserve is the estimated future cost of a claim at a point in time. There are pros and cons of using salary continuation; contact your OMA Account Manager for advice. It can be used selectively to create employee-employer goodwill. Employers are not authorized to pay any other types of compensation benefits (other than wages in lieu of temporary total) directly. Salary Continuation is not available to employers enrolled in the BWC deductible programs. See BWC Form C-55 and BWC Salary Continuation policy.

Salary Continuation AgreementThis form can be obtained online at: www.ohiobwc.com
Employee name Claim number
On the ________ day of _________________ , ______ , ____________________________ , the employer and
the employee named above executed the following terms and conditions pertaining to the payment of salary continuation.
The employer, since the inception of the employee’s disability resulting from an accident/occupational disease suffered by the
employee on ____ / ____ / ____ , while in course of their employment, has been or is paying regular (full) salary/wages in lieu
of temporary total or living maintenance compensation, to the employee during the period of disability as indicated below:
Continuation of regular (full) salary/wages and any benefits the injured worker would otherwise have been entitled to has been/will
be paid. Salary continuation will be paid at the rate of $ ________________ per ________________ (week, two weeks, etc.) for
the period of time from ____ / ____ / ____ to ____ / ____ / ____ (a period of time not to exceed 45 days per C-55 submission).
Does the amount paid include salary/wages from other employment? Yes No
Should salary continuation payment continue a new C-55 must be submitted within 5 days of the end date of this agreement. The employer must notify BWC immediately if salary continuation will be discontinued and/or if the injured worker returns to work.
Employer name
Employer name Employer telephone number
Instructions• This form is used to acknowledge an agreement to pay salary/wage continuation
in lieu of temporary total or living maintenance compensation.• Regular (full) salary/wages includes any benefits which the employee would
normally be entitled to if the employee was working.
• This form must be signed by the employee and the employer.• Fax or mail this completed agreement to your local BWC service office.
Employee signature
Employer signature and title
Date
Date
BWC-1174 (6/25/2008)C-55
Policy number

Revised June 2012
Continued on next page
What is salary continuation?Salary continuation (wages in lieu of temporary total com-pensation) allows an employer to pay an employee his or her regular wages after a workplace injury or illness occurs.
The injured worker has the option to accept salary continu-ation if he or she so chooses unless there is a collective bar-gaining contract that states otherwise. The employer may pay the injured worker salary continuation until either party termi-nates payment. At that time, workers’ compensation benefits may take effect, if appropriate.
If we find, at any time, the employer is not paying the injured worker’s regular wages, we will begin paying temporary total compensation with supporting medical evidence and a signed request by the injured worker.
This fact sheet provides an overview of injured worker and employer responsibilities and rights related to salary continu-ation. This list is not all inclusive.
The injured worker’s responsibilities and rightsOYou are not required to accept salary continuation in
lieu of temporary total compensation. However, a col-lective bargaining contract may supersede this policy.
OYou should not experience a break in service that impacts seniority or other benefits when your employer pays salary continuation.
OYour employer cannot force you to use sick time, unless there is a collective bargaining contract that states oth-erwise.
The employer’s responsibilities and rightsOYour injured worker must receive a full check at the
next scheduled time after the injury or illness occurs. You cannot wait until we or the Industrial Commission of Ohio (IC) makes a determination. If you miss paying an injured worker at a scheduled time, you forfeit salary continuation rights on the claim and temporary total will begin with supporting medical evidence and a signed request by the injured worker.
OYou may not wait until the injured worker has missed 14 days to pay the first seven days. You must pay salary continuation when it is apparent the injured worker will
miss eight or more days due to the work-related injury or illness. Payment of eight or more days of salary continuation indicates a lost-time claim.
OYou are not required to pay salary continuation if the claim appears to be a medical-only claim. If you pay salary continuation for less than eight days, the claim remains medical only. If a medical-only claim subse-quently becomes lost time and you wish to pay salary continuation, you must pay all days at that time.
OIf you wish to pay salary continuation, you must notify us before we issue the initial determination decision.
OYou cannot pay salary continuation once we have ordered temporary total compensation, unless required by a collective bargaining contract.
OYou must report in writing the injured worker’s earn-ings. This earnings report must be for the 52-week period prior to the date of injury – or whatever portion of that time the injured worker worked for your com-pany. We use this information to determine the full and average weekly wage in the claim.
OYou must submit a Salary Continuation Agreement (C-55), signed by a representative of your company and the injured worker, for each period of salary con-tinuation to be paid. This does not mean for each pay period, but for each period of disability as identified on the C-55. You should base the end date on the expected period of disability as supported by medical documen-tation, not to exceed 45 days. Do not list “until return to work” or a vague future date on the form to avoid submitting additional C-55s.
OYou should pay salary continuation only for periods of disability related to the allowed conditions in the claim. we encourage you to review medical documen-tation to confirm that the injured worker remains off work for the allowed conditions and to determine if return to work (light duty) is possible.
OImportant note – If we discover the injured worker con-tinues to work other jobs, we will notify the employer.
OYou may choose to only cover your company’s por-tion of the injured worker’s lost wages if the employee had more than one job at the time of the accident. We would cover the difference for the injured worker.
Salary Continuation Policy

OHowever, you may choose to pay wages from the injured worker’s other job(s). The injured worker would not suffer any loss of wages. This would suppress reserves for claims with dates of injury prior to Jan. 1, 2011.
OYou may pay an injured worker the wage he or she earned prior to the injury even if the worker returns to work and is in a different position due to work restric-tions.
OYou must notify us within 72 hours when you have dis-continued the payment of salary continuation and/or when the injured worker returns to work. Failure to do so may impact your eligibility to participate in the salary continuation program.
OUnder salary continuation, you, BWC or the IC may schedule an independent medical exam (IME). The IME is scheduled to address issues such as return-to-work capability, functional limitations/restrictions, vocational rehabilitation potential, maximum medical improve-ment (MMI) and appropriateness of current treatment. However, an IME is not scheduled for the sole purpose of determining the issue of MMI. A finding of MMI has no impact on payment of salary continuation. Also, we do not view salary continuation as temporary total compen-sation for the purpose of scheduling a 90-day exam.
OWe do not authorize you to award wage loss, perma-nent partial, permanent total, death awards or any other awards.
OYou cannot pay salary continuation to an injured worker who no longer works for your company.
OThe payment of salary continuation will no longer sup-press the claim reserve for claims with a date of injury on or after Jan. 1, 2011.
If you have questions regarding our salary continuation policy, please contact your claims service specialist or employer ser-vices specialist at your local customer service office, or call 1-800-OHIOBWC.
Revised June 2012

16
BWC $15,000 Medical Program The BWC allows an employer to self-insure the first $15,000 of medical expenses on any claim. The employer may be able to improve its BWC claims experience (and therefore contain its premiums) by paying the first $15,000 in a claim’s medical costs. Generally speaking, this program is of limited value and requires coordination with Medicare/Medicaid for employees eligible for those programs. Contact us to see if this program can benefit your company. The employer can choose to pay out-of-its-pocket medical expenses on a claim by claim basis. Your OMA Account Manager can assist you in making this determination. You must notify the injured worker, the medical provider and your managed care organization (MCO) that you will be paying the fee bills directly, thus avoiding charges to your workers’ compensation experience. Payment of medical bills under this program does not waive the BWC’s right to decide a claim if filed, and it does not negate the injured worker’s right to file a claim. To enroll, you should contact your BWC Employer Service Specialist or call your OMA Account Manager for guidance. The $15,000 Medical Program is not available to employers enrolled in the BWC deductible or group retrospective rating programs.

17
Light Duty The following guidance is provided to help you return your employee to light duty work and to advise you how to document your process. In the process, you will send a series of communications to the treating physician, and then to the injured worker. We recommend that you maintain a written record of your correspondence in the unlikely event that the return-to-work is opposed and referred to the Industrial Commission for hearing. Step 1 – Contact the nurse at treating physician’s office
Introduce yourself Tell the nurse that you would like the physician to review options for a possible light duty
release Obtain a fax number or email address where you can direct documents to the physician
Step 2 – Send your request to the physician for the employee’s up-to-date work restrictions (sample letter 1 follows) with a blank BWC MEDCO-14 – Physician’s Report of Work Ability form (also available from your OMA account manager) This letter introduces you to the physician and informs him or her that your company is willing to offer light duty work to the injured worker. The letter requests that the doctor provide you with the employee’s up-to-date work restrictions. Step 3 – Request the physician to compare work restrictions to your job description Only proceed to this step if you have obtained up-to-date work restrictions (see above) and if you can accommodate the restrictions. Send a letter (sample letter 2 follows) informing the doctor that you have light duty work available that you believe meets the restrictions. This request asks the doctor to review your job description (with job title) and approve the return-to-work in this transitional capacity. We have created model Jobs/Duties Description form, approved by the BWC, for your use. Step 4 – Advise your employee of the return to work authorization provided by the physician Once the physician of record approves your job description in light of the employee’s work restrictions, you are ready to instruct the employee to return to work. Send a letter (sample letter 3 follows) to the employee to inform him or her the date and time he or she is expected to return to work. We recommend sending this letter both regular and certified mail. Also, place a courtesy call to the employee. It is always in everyone’s best interests to help an employee feel welcome to return to work.

18
Light Duty - Sample letter 1 Place on your letterhead To: physician of record Attach: BWC MEDCO-14 Physician’s Report of Work Ability form To: [Physician] Re: Employee Return-To-Work
[IW first name] [IW last name] Date of injury [month] [date] [year]
We are the employer in the above referenced workers’ compensation claim. As such, we would like to make you aware that we do have modified/light duty positions available that may provide an opportunity for this injured worker to safely return to work in a light duty/transitional capacity. If you decide that the injured worker is capable of returning to work with restrictions, please forward a list or description of those restrictions. After we review the restrictions, we will, if appropriate, forward to you a job description for your review. We look forward to working with you to safely return our employee to work. Should you have any questions, please do not hesitate to contact me at [contact information]. Respectfully, [name] [title] enclosure: BWC MEDCO-14

19
Light Duty - Sample letter 2 Place on your letterhead To: physician of record Attach: light duty job title and description To: [Physician] Re: Employee Return-To-Work
[IW first name] [IW last name] Date of injury [month] [date] [year]
We are the employer in the above referenced workers’ compensation claim. As such, we have received a copy of the restrictions you have established for our employee. At your earliest convenience, please review the attached job description and advise us if the employee can safely perform these job duties in light of the restrictions you have specified. Please advise if there are any duties which the employee should not perform. Finally, please indicate the specific date the employee could assume the duties of the attached job description. So that we can have a complete record, please sign and date your response. Should you have any questions, please do not hesitate to contact me at [contact information]. Respectfully, [name] [title] enclosure: job description

20
Light Duty - Sample letter 3 Place on your letterhead To: injured worker Attach: copy of physician’s restrictions and physician-approved light duty job title and description Send regular and certified mail To: [Employee] Re: Your Return-To-Work We have been working with your attending physician to determine if we have a position available for you that will accommodate your current physical restrictions and afford a safe return to work. Dr. [physician name] has reviewed the attached job description and has decided that you are capable of performing this job with restrictions as documented. At this time, we would like to offer you this modified duty position which accommodates your restrictions. Please report to work on [day of week], [month] [date] at [time] [a.m. or p.m.]. Your regular hours will be [beginning and ending time] and you will receive your former wage of [$/hour]. This is a temporary position and will be reevaluated should your restrictions change or until you can return to regular duty. Should you have any questions, please do not hesitate to contact me at [contact information]. Respectfully, [name] [title] enclosures: Physician’s restrictions Physician-approved light duty job title and job description

JOB/DUTIES DESCRIPTION PAGE 1 of 2 EMPLOYER TO COMPLETE AND SUBMIT TO PHYSICIAN
Injured worker name: _________________________________________ Claim no.: ____________________________________
Occupation/Job title: ________________________________________________________________________________________
General description of the injured worker’s usual job duties:________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
Describe other job duties the injured worker may perform: _________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
We can provide modified duty for this injured worker: (circle one) Yes No Possibly
Does the injured worker drive or operate heavy machinery? (circle one) Yes No
If yes, please describe, including the use of hand and/or foot controls.
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
Please circle the physical requirements of the injured worker's job.
Lifting/carrying requirements (circle one for each weight group)
0 to 10 lbs Never Occasionally Frequently Continuously
11 to 20 lbs Never Occasionally Frequently Continuously
21 to 40 lbs Never Occasionally Frequently Continuously
41 to 60 lbs Never Occasionally Frequently Continuously
61 to 100 lbs Never Occasionally Frequently Continuously
Pushing/pulling requirements (circle one for each weight group)
0 to 25lbs Never Occasionally Frequently Continuously
26 to 40 lbs Never Occasionally Frequently Continuously
41 to 60 lbs Never Occasionally Frequently Continuously
61 to 100 lbs Never Occasionally Frequently Continuously
26 to 50 lbs Never Occasionally Frequently Continuously
100 plus lbs Never Occasionally Frequently Continuously
Use of hands for simple grasping (circle one for each hand)
Right hand Never Occasionally Frequently Continuously
Left hand Never Occasionally Frequently Continuously
Use of hands for fine manipulation (circle one for each hand)
Right hand Never Occasionally Frequently Continuously
Left hand Never Occasionally Frequently Continuously
Use of feet/legs for controls (circle one for each foot/leg)
Right foot/leg Never Occasionally Frequently Continuously
Left foot/leg Never Occasionally Frequently Continuously
Other requirements (circle one for each motion)
Bending Never Occasionally Frequently Continuously
Squat/Kneel/Crawl Never Occasionally Frequently Continuously
Twist/turn Never Occasionally Frequently Continuously
Climb Never Occasionally Frequently Continuously
Reach above the shoulder Never Occasionally Frequently Continuously
Work with cold substances Never Occasionally Frequently Continuously
Work with hot substances Never Occasionally Frequently Continuously
Sitting ____ hours per day
Standing ____ hours per day
Walking ____ hours per day
CONTINUED

JOB/DUTIES DESCRIPTION PAGE 2 of 2 EMPLOYER TO COMPLETE AND SUBMIT TO PHYSICIAN
Injured worker name: _________________________________________ Claim no.: ____________________________________
Occupation/Job title: ________________________________________________________________________________________
General description of the injured worker’s usual job duties:________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
Describe other job duties the injured worker may perform: _________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
We can provide modified duty for this injured worker: (circle one) Yes No Possibly
Does the injured worker drive or operate heavy machinery? (circle one) Yes No
If yes, please describe, including the use of hand and/or foot controls.
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
Please circle the physical requirements of the injured worker's job.
Lifting/carrying requirements (circle one for each weight group)
0 to 10 lbs Never Occasionally Frequently Continuously
11 to 20 lbs Never Occasionally Frequently Continuously
21 to 40 lbs Never Occasionally Frequently Continuously
41 to 60 lbs Never Occasionally Frequently Continuously
61 to 100 lbs Never Occasionally Frequently Continuously
Pushing/pulling requirements (circle one for each weight group)
0 to 25lbs Never Occasionally Frequently Continuously
26 to 40 lbs Never Occasionally Frequently Continuously
41 to 60 lbs Never Occasionally Frequently Continuously
61 to 100 lbs Never Occasionally Frequently Continuously
26 to 50 lbs Never Occasionally Frequently Continuously
100 plus lbs Never Occasionally Frequently Continuously
Use of hands for simple grasping (circle one for each hand)
Right hand Never Occasionally Frequently Continuously
Left hand Never Occasionally Frequently Continuously
Use of hands for fine manipulation (circle one for each hand)
Right hand Never Occasionally Frequently Continuously
Left hand Never Occasionally Frequently Continuously
Use of feet/legs for controls (circle one for each foot/leg)
Right foot/leg Never Occasionally Frequently Continuously
Left foot/leg Never Occasionally Frequently Continuously
Other requirements (circle one for each motion)
Bending Never Occasionally Frequently Continuously
Squat/Kneel/Crawl Never Occasionally Frequently Continuously
Twist/turn Never Occasionally Frequently Continuously
Climb Never Occasionally Frequently Continuously
Reach above the shoulder Never Occasionally Frequently Continuously
Work with cold substances Never Occasionally Frequently Continuously
Work with hot substances Never Occasionally Frequently Continuously
Sitting ____ hours per day
Standing ____ hours per day
Walking ____ hours per day
Completed by:_________________________________________________________________ Date: ________________
Title: _______________________________________________________________________________________________
Phone: ______________________________________ Email: _________________________________________________

23
Transitional Work Transitional work is a BWC program that allows an injured worker to return to - or remain - at work, performing physically appropriate modified duties while he or she is recovering. This is an excellent alternative to BWC Temporary Total disability compensation and can minimize actual charges and reserve assessments to your experience; having a Transitional Work plan communicates to your employees how much you value their involvement in your organization. Job descriptions for transitional work must be specific and current. Procedural matters and documentation are extremely important in making an appropriate job offer and maintaining the integrity of the program. We can guide you through the process. We have created model Jobs/Duties Description form, approved by the BWC, for your use. The BWC’s Transitional Work program can pay premium bonuses for returning your employees to work. Enrollment in the program is necessary and assistance in implementing a transitional work program is available. The employer works with a BWC-accredited transitional work developer to qualify for this program. For additional information, contact your BWC Employer Service Representative or contact us.

24
Handicap Reimbursement The State of Ohio encourages the hiring and retention of employees with identified “handicap conditions.” As an incentive under the Handicap Workers’ Provision, the state will share the cost of a lost time claim (a lost time claim is defined as a case involving 8 or more lost work days, not necessarily consecutive) with the employer by charging a portion of the cost to the BWC Surplus Fund.
The request must be supported by evidence (medical records or physician statements) that the injured worker suffered from one or more of the qualifying handicap conditions prior to the date of injury and that the handicap condition either caused the injury, contributed to the cost of the claim, was aggravated by the claim, or delayed recovery. Please notify us should you have knowledge (verbal or written) that an injured worker suffers from one of the following conditions. We will initiate the appropriate process to secure financial relief to your claims experience should we be able to substantiate a handicap situation.
(01) Epilepsy (02) Diabetes (03) Cardiac disease (04) Arthritis (05) Amputated foot, leg, arm, or hand (06) Loss of sight of one or both eyes or a partial loss of uncorrected vision of more than seventy-five percent bilaterally (07) Residual disability from poliomyelitis (08) Cerebral palsy (09) Multiple sclerosis (10) Parkinson's disease (11) Cerebral vascular accident (12) Tuberculosis (13) Silicosis (14) Psycho-neurotic disability following treatment in a recognized medical or mental institution (15) Hemophilia (16) Chronic osteomyelitis (17) Ankylosis of joints (18) Hyper insulinism (19) Muscular dystrophies (20) Arterio-sclerosis (21) Thrombo-phlebitis (22) Varicose veins (23) Cardiovascular, pulmonary, or respiratory diseases of a fire fighter or police officer employed by a municipal corporation or township as a regular member of a lawfully constituted police department or fire department (24) Coal miners' pneumoconiosis, commonly referred to as "black lung disease" (25) Disability with respect to which an individual has completed a rehabilitation program approved by BWC.

25
Lump Sum Settlement (LSS)
Lump Sum Settlement (LSS) pays the injured worker a full and final settlement amount and removes all MIRA reserve costs of the claim from the employer’s claims experience. It is a useful tool in containing costs under appropriate circumstances.
Best Practice: We generally do not recommend settlement of a claim when the injured worker is still under your employment. However, you may know of special circumstances where settlement may be deemed appropriate regardless of employment status. We strongly recommend that you consult us regarding settlement opportunities any time an employee with a claim leaves your employment.
The settlement is paid to the injured worker by the Bureau of Workers’ Compensation. Once a claim is settled, the amount of the settlement is charged to the employer’s experience rating, eliminating all future MIRA reserve assessments, thus potentially reducing the employer’s workers’ compensation premiums.
A claim settlement can be initiated only by the injured worker/injured worker representative and employer/employer representative or BWC. The managed care organization (MCO) is not a party to the settlement; therefore, the MCO may not initiate nor advise an injured worker to settle his or her claim. Your OMA Account Manager also monitors your claims for settlement potential and has created a report for you that tracks OMA settlement activity on your behalf.
To see your Settlement Report and all other OMA workers’ compensation management reports we generate for you, log into My OMA. Learn more about this service here.
The Settlement Agreement and Application of Settlement Agreement, documents the agreement regarding the terms and conditions of the settlement. Your OMA Account Manager guides the process.
BWC administers and approves all claim settlements and reviews the agreement to ensure that the settlement is fair to all parties.