Embed Size (px)
Citation preview

Worth a Thousand Words:Telling a Story with Data
Ari Robicsek, MD
Chief Medical Analytics Officer
Providence St. Joseph Health
A5/B5

Session Objectives
• Consider the challenges of representing patient safety data
• Develop an approach to designing strong data visualizations
These presenters have nothing to disclose
2










7 ‘A’s of actionable data
• Accurate

Accurate
Acc
ura
cy
Effort
Bidirectionalvalidation
1. 2.

7 ‘A’s of actionable data
• Accurate
• Argumentative (i.e. Advances a hypothesis)





7 ‘A’s of actionable data
• Accurate
• Argumentative (i.e. Advances a hypothesis)
• Appealing (good looks draw in users)

© Jorge Gonzalezhttps://www.interaction-design.org/literature/article/bad-design-vs-good-design-5-examples-we-can-learn-frombad-design-vs-good-design-5-examples-we-can-learn-from-130706

© Nikki Syliantenghttps://www.interaction-design.org/literature/article/bad-design-vs-good-design-5-examples-we-can-learn-frombad-design-vs-good-design-5-examples-we-can-learn-from-130706


7 ‘A’s of actionable data
• Accurate
• Argumentative (i.e. Advances a hypothesis)
• Appealing (good looks draw in users)
• Aimed at the right person (no point creating a chief executive dashboard for a nursing unit leader, and vice versa)


7 ‘A’s of actionable data
• Accurate
• Argumentative (i.e. Advances a hypothesis)
• Appealing (good looks draw in users)
• Aimed at the right person (no point creating a chief executive dashboard for a nursing unit leader, and vice versa)
• Atomic (contains the deepest level of detail absolutely necessary for decision-making)

Where is my problem?What can I do about it?

7 ‘A’s of actionable data
• Accurate
• Argumentative (i.e. Advances a hypothesis)
• Appealing (good looks draw in users)
• Aimed at the right person (no point creating a chief executive dashboard for a nursing unit leader, and vice versa)
• Atomic (contains the deepest level of detail absolutely necessary for decision-making)
• Accessible (the four worst words in the English language…)

Carl Reinhold AugustWunderlich
https://en.wikipedia.org/wiki/Carl_Reinhold_August_Wunderlich#/media/File:Carl_August_Wunderlich.jpg







7 ‘A’s of actionable data
• Accurate
• Argumentative (i.e. Advances a hypothesis)
• Appealing (good looks draw in users)
• Aimed at the right person (no point creating a chief executive dashboard for a nursing unit leader, and vice versa)
• Atomic (contains the deepest level of detail absolutely necessary for decision-making)
• Accessible (the four worst words in the English language…)
• Arrives in time to do something about it

Big ideas for the system Inpatient Quality Dashboard
1. Employs data accuracy best practices (e.g. validation)
2. Clear visualizations with statistical discipline
3. Rapid comparison of different hospitals
4. Usable at system, market and hospital levels
5. Allows outcome and process metrics to be consumed together
6. Available ‘where users work’


Q2
A FRENCH PLOT
Current performance

A FRENCH PLOT
Trend
Q2

0
50
100
150
200
250
300
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
Dec
-15
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
May
-16
Jun
-16
Jul-
16
Au
g-1
6
Sep
-16
Oct
-16
No
v-1
6
Dec
-16
Jan
-17
Feb
-17
Mar
-17
Ap
r-1
7
May
-17
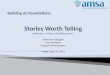
Statistical Process Control Chart

0
50
100
150
200
250
300
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
Dec
-15
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
May
-16
Jun
-16
Jul-
16
Au
g-1
6
Sep
-16
Oct
-16
No
v-1
6
Dec
-16
Jan
-17
Feb
-17
Mar
-17
Ap
r-1
7
May
-17
Statistical Process Control Chart
UCL
Avg
LCL

0
50
100
150
200
250
300
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
Dec
-15
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
May
-16
Jun
-16
Jul-
16
Au
g-1
6
Sep
-16
Oct
-16
No
v-1
6
Dec
-16
Jan
-17
Feb
-17
Mar
-17
Ap
r-1
7
May
-17
Statistical Process Control Chart
7 in a row moving in the same direction
UCL
Avg
LCL
2 out of 3 on same side of centerline and 2 SD away
4 out of 5 on same side of centerline and 1 SD away
Beyond 3 SD (control limits)
8 in a row on the same side of the centerline




https://industryvisuals.w2pstore.com/product/safety-cross-mounted-on-magnetic-dry-erase-board/


Q2

Q2


















Issues
• Look and feel
• Navigation hard
• Training
• Can’t see all nursing units at once
• Can’t see all metrics at once



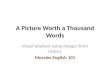
Multiple Metrics View
• Multiple metrics, multiple hospitals
• “Stoplight”
• Current performance
• Performance over time
• Performance relative to target

Safe
C. diff 56 75 !
CAUTI 76 75
CLABSI 65 75 ●
SSI-Hyst 80 75
SSI-Colon 46 75
Falls w injury 71 75
Option 1

System Performance – Safe 4 / 5Option 2

System Performance – Safe 4 / 5
Trend
Option 3

System Performance – Safe
3 / 5target: 75
target: 66
target: 63
target: 58
target: 71
Option 4










Example: Accelerating improvement in hospital-acquired Clostridium difficile
85
After
Q4 2016 – Q3 2017
Before
Q2 2016 – Q1 2017



Locations
Vantage
Epic
A Tableau linkhttp://tableauserver.providence.org/#/views/SystemQualityScorecard/Overview?:iid=1

More Issues
• C-suites don’t go searching for data
• Data issues arise regularly
• Framing in the context of the goals of the organization



Toolbox for EveryonePay Attention to Detail (STAR, peer check)
Communicate Clearly (SBAR, repeat back, clarifying questions)
Have a Questioning Attitude (know why and comply, validate and verify)
Operate as a Team (brief, execute and debrief)
Speak Up for Safety (CUS, event reporting systems)
Tones for RespectSmile and greet others; sayhello
Introduce using preferred names and explain roles Listen with
empathy and intent to understand Communicate positive intent
of our actions Provide an opportunity for others to ask
questions
Prevent InfectionsExpect scrupulous hand hygiene
Use standard precautions and appropriate PPE for isolation
Conduct case reviews immediately when infections occur
Assist patient in maintaining personal and hand hygiene
Ensure comprehensive environmental cleaning
Eliminate CAUTIKnow the evidence-based indications for catheter use and only use when met
Insert catheter aseptically
Ensure catheter is secured
Perform appropriate catheter hygiene daily, and following fecal incontinence
Remove at earliest opportunity, no later than 48 hours unless otherwise indicated
Eliminate C. DifficileAvoid excess and inappropriate antibiotic use
Isolate and test early on suspicion of infection
Only test symptomatic patients where infection is suspected
Terminally clean room with sporicidal disinfectant at discharge
Eliminate CLABSIVerify appropriate indications for placement
At insertion, utilize maximal barrier precautions & sterile technique
Change dressing/tubing every 7 days or when integrity is breached
Flush the central line at least once every 12 hours
Verify justification for continuing central line daily
Eliminate Surgical Site InfectionsEstablish and maintain glycemic control targets (pre, peri, post)
Maintain temperature at 36 degrees C or above (pre, peri, post)
Conduct post-procedure pause to document wound class and skin closure
Ensure weight-based, appropriate dosing of antibiotics
Counsel for smoking cessation, at least for duration of wound healing
Reduce Sepsis MortalityDraw lactate level on suspicion of sepsis
Draw immediate blood cultures on suspicion of sepsis
Resuscitate with fluids 30 mL/kg over 1 hour
Administer antibiotics within 3 hours
Repeat lactate at 6 hours
Eliminate Falls with InjuryUtilize universal assessment & safety protocol for all patients
Implement interventions based on risk assessment
Share plans with patients, family and care team
Debrief with team immediately after every fall
Review medication regimen after every fall (pharmacy)
Prevent ReadmissionsComplete medication reconciliation at discharge and follow up
Ensure safe discharge with concise instructions and f/u hotline
Schedule f/u w/in 5 days (high risk) or 14 days (moderate risk)
Conduct follow-up call within 48 hours (high risk)
Provide d/c summary for transitions, warm handoff in high risk
Make Hospitals HealthierProvide goal-aligned care (focus on what matters to the patient)
Assess and support nutritional status
Minimize night-time noise, enable undisturbed sleep
Encourage exercise & staying out of bed
Ensure 24-7 family access and support for patients
Care CompassionatelyConduct hourly nurse rounding using specific compassion-based
behaviors Conduct leader rounding and immediate intervention with
patients
Make post-discharge calls with compassion-based behaviors
Implement clinician-led forums aimed at compassion-based support/burnout prevention
Use compassion and resiliency-focused interventions with clinicians at high burnout risk
Toolbox for LeadersMessage on the Mission (reflection/safety message, safety first in every
decision, stand up for those who speak up for safety)
Lead Reliable Operations (daily huddles including experience, top 10 lists)
Build Engagement, Accountability (5:1 feedback, fair and just accountability, round to influence)
Foster Teamwork (display unit-based results, learning boards, action plans)
CARING RELIABLY: IMPROVINGOUTCOMES AND MAKING IT STICK
CORE BEHAVIORS OF CARING RELIABLY
IMPATIENT HEALTH: CARE BUNDLES
INPATIENT SAFETY: CARE BUNDLES