Embed Size (px)
Citation preview
Wrap-Around Plan Document and Summary Plan Description
Southern Personnel Management, Inc. (SPMI)
This Wrap-Around Plan Document and Summary Plan Description (SPD) together with your most
recent insurance certificate of coverage, benefit summary, insurance booklet, amendments, and benefit
riders issued to you by MetLife and AFLAC (collectively referred to in this document as the "Certificate
of Coverage"), will constitute your complete ERISA Plan Document and Summary Plan Description
(SPD). If the certificate of coverage is not attached, then this wrap-around document is not complete
and the participant should contact SPMI for a complete copy. If you have not received your insurance
certificate of coverage you should contact SPMI at (800) 940-8706 to request a copy.
This Wrap-Around Plan Document was created in good faith to comply with the requirements of the
Patient Protection and Affordable Care Act (PPACA). However, some of the regulations and other
guidance under PPACA may be temporary or has not yet been issued. SPMI reserves the right to amend
this Wrap-Around Plan Document and SPD, retroactively if deemed necessary, to comply with the
requirements under PPACA.
Effective Date: 06/01/2015

PLEASE READ THIS DOCUMENT CAREFULLY AND KEEP FOR FUTURE REFERENCE
SPMI Plan
To request a copy of this Wrap-Around Plan Document and Summary Plan Description in a larger font, please contact SPMI Benefits Department at (800) 940-8706 or at [email protected]
Introduction SPMI maintains the Group Dental, Vision, and Supplemental Insurance Plan (the “Plan”) to provide Dental, Vision, and Supplemental benefits to its eligible employees, their eligible spouses and eligible dependents. Benefits of the Plan are provided under an insurance contract entered into between SPMI and MetLife and AFLAC (the “Insurance Company”). The terms, provisions and conditions under which you may be eligible for and receive benefits are set forth in the terms of each applicable insurance policy. The benefits are under this Plan are provided solely through insurance contracts. This document does not replace the provisions of the insurance policy (ies). Every effort has been made to make this Wrap-Around Plan Document and Summary Plan Description as complete and accurate as possible. In the event of any differences between this Wrap-Around Plan Document and Summary Plan Description and any of the insurance policies, the terms of the insurance contract/policy will prevail. You must complete an enroll application to receive benefits under this Plan. Benefits under the Plan are described in the insurance Certificate of Coverage governing your benefit program issued by the Insurance Company, which you should have received. You must read the Certificate of Coverage carefully to understand your benefit. SPMI is providing this document to give you an overview of the Plan and to address certain information that may not be addressed in the Certificate of Coverage. This SPMI document, together with the Certificate of Coverage issued by the Insurance Company, is the complete Wrap-Around Plan Document and Summary Plan Description (SPD) as required by the Employee Retirement Income Security Act of 1974 (ERISA), for the benefit programs to which ERISA applies. This Wrap-Around Plan Document and Summary Plan Description document is not intended to give you any substantive rights to benefits that are not already provided by the Certificate of Coverage. Information contained herein does not constitute or replace the Certificate of Coverage issued by the insurance company (ies) listed in this document.
General Plan Information The following information is information about the Plan that is required to be provided to you under ERISA. Plan Name: SPMI Health and Welfare Plan Type of Plan: Welfare Benefit Plan - Group Dental, Vision, and AFLAC
Plan Year: The 12 month period beginning each June 1 and ending each May 31 Plan Number: 501 Effective Date: The effective date of this document is 06/01/15. Funding of this plan: The plan is funded by the payment of premium under the group insurance policy(ies). The premium is paid partly from funds contributed by the employer and party from funds contributed by the employees, which may include pre-tax payroll deductions, at a rate determined by the employer. The Plan Administrator for the various benefit programs will provide a schedule of the applicable premiums during the initial and subsequent open enrollment periods and upon request for each of the benefit Programs, as applicable. Type of Plan Administration: This plan is fully insured. Benefits are provided under a group insurance contract entered into by SPMI and MetLife and AFLAC. Benefits are provided in accordance with the provision of the group insurance policy (ies) issued to the employer by the Insurance Carrier(s)shown below and throughout this document. While MetLife and AFLAC and SPMI share responsibility for administering the terms of the plan, MetLife and AFLAC is responsible for processing and paying benefit claims and for handling appeals of denied claims. Insurance Carrier Information and Claim Administrator: (Available coverage options and insurance carriers may be changed at any time by the Employer.) MetLife - Dental PO Box 981282 El Paso, TX 79998-1282 Phone: 800-275-4638 AFLAC - Supplemental 1932 Wynnton Road Columbus, Georgia 31999 Phone: 800-992-3522 Plan Sponsor: SPMI, 1701 Main St., Van Buren, AR 72956; Phone: 479-474-7752 Plan Sponsor’s Employer Identification Number (EIN): Available upon request
Plan Administrator: SPMI, 1701 Main St., Van Buren, AR 72956; Phone: 479-474-7752

PLEASE READ THIS DOCUMENT CAREFULLY AND KEEP FOR FUTURE REFERENCE
SPMI Plan
To request a copy of this Wrap-Around Plan Document and Summary Plan Description in a larger font, please contact SPMI Benefits Department at (800) 940-8706 or at [email protected]
Named Fiduciary: SPMI, 1701 Main St., Van Buren, AR 72956; Phone: 479-474-7752 Agent for Service of Legal Process: Clifford Lyon, 1701 Main St., Van Buren, AR 72956; Phone: 479-474-7752 Participating Employers: See Appendix 1 (available upon request)
Eligibility and Participation Requirements and Provisions (For complete conditions of eligibility read the Eligibility and Enrollment sections contained in the Certificate of Coverage for each insurance policy/benefit program in which you have enrolled in) Employee Eligibility: To be eligible for coverage under this plan, you must be classified by SPMI as a full-time employee regularly scheduled to work at least 30 hours per week.
Waiting Period: Your coverage will begin on the first day of the first month following the completion of your worksite eligibility waiting period. If your worksite employer does not have an eligibility waiting period, your coverage will begin on the first day of the first month following a 3 months waiting period.
Spouse and Dependent Eligibility: To determine whether your spouse and/or dependents are eligible to participate in the plan and for enrollment requirements, read the Eligibility and Enrollment sections contained in the Certificate of Coverage for each insurance policy in which you have enrolled in. The dependent age may defer for each insurance product you may have elected. Enrollment Time Limits: Eligible employees must complete an application form (available by contacting SPMI’s Benefit Department) to enroll themselves and/or their eligible spouses and dependents. New employees must enroll within certain time periods after being hired, as described in the certificate of coverage insurance booklet issued by MetLife, and AFLAC. Otherwise, enrollment generally is limited to the annual open enrollment period that occurs before June 1 of each year. If an employee does not enroll for coverage within the required period as indicated in Certificate of Coverage for each insurance carrier, the employee and/or any dependents may be considered a late entrant subject to coverage exclusion, limitations and coverage waiting periods. Open Enrollment Period: An “open enrollment period” is a time established by the Company when eligible employees and their eligible dependents have the option to enroll in the plan or make changes to current plan coverage. Each eligible employee may enroll for coverage (or enroll any eligible dependents) or may change the level of coverage during the
annual open enrollment period. The annual open enrollment period will be the month of April each plan year for a June 1 effective date. Special Enrollment Rights: In certain circumstances, enrollment may occur outside the open enrollment period. See the Special Enrollment in section of the Certificate of Coverage. The plan’s special enrollment rights notice also contains important information about the special enrollment rights that you may have, you can find a copy of the complete notice under the Employee Benefit Disclosure Notice section of this document. You may also contact SPMI’s Benefit Department to request a copy at any time. If the cost of benefits increases or decreases during a benefit period the Plan Administrator may automatically change the contribution amount. When a change in contribution is significant, a Participant may either increase the contributions or change to a less costly coverage election. When a new benefit option is added, a Participant may change to elect the new benefit option. When a significant overall reduction is made to a benefit option, a Participant may elect another available benefit option. Employee Premium Payment Requirement: Employees must pay a portion of the premium. SPMI provides a schedule of the applicable premiums; contact SPMI Benefit Department if you need another copy. If your employer maintains a Cafeteria Plan, your required premium contribution may be paid on a pre-tax basis. Termination of Coverage: Coverage shall terminate as described in the Termination of Coverage section in the Certificate of Coverage. Coverage will also terminate if you fail to pay your share of the premium, or if your hours drop below the required eligibility threshold, if you submit false claims, and for certain other reasons described in the certificate of coverage insurance booklet. Benefits will also cease for employees, spouses and dependents upon termination of the Plan. Continuation of Coverage: If vision or dental coverage for the Participant, the Participant’s eligible spouse, or eligible Dependents ceases because of certain “qualifying events” (e.g., termination of employment, reduction in hours, divorce, death, or a child’s ceasing to meet the Plan’s definition of Dependent) specified in a federal law called COBRA, then the Participant, the Participant’s eligible spouse, or eligible Dependents may have the right to purchase continuing coverage under the Plan for a limited period of time. COBRA applies to most employees (and most of their covered family Dependents) of most employers with 20 or more employees. An explanation of COBRA continuation coverage, including information concerning qualifying events

PLEASE READ THIS DOCUMENT CAREFULLY AND KEEP FOR FUTURE REFERENCE
SPMI Plan
To request a copy of this Wrap-Around Plan Document and Summary Plan Description in a larger font, please contact SPMI Benefits Department at (800) 940-8706 or at [email protected]
and qualified beneficiaries, premiums, notice and election requirements and procedures, and duration of coverage is contained in the Employee Benefit Disclosure Notice section of this document. Please refer to that section to determine if your group is subject to COBRA. Military Leave-USERRA Continuation Coverage: If COBRA or USERRA gives Covered Persons different rights or protections, the law that provides the greater benefit will apply. The Uniformed Services Employment and Reemployment Rights Act of 1994 (“USERRA”) established requirements that employers must meet for certain Employees who are involved in the Uniformed Services. In addition to the rights that Participant has under COBRA, Participant is entitled under USERRA to continue the coverage Covered Persons. If any of the provisions concerning USERRA within this document conflict with the USERRA federal law, USERRA federal law shall govern. You must submit a USERRA election to the plan within the required time. Please refer to each insurance carrier’s specific Certificate of Coverage governing your benefit program. Duration of USERRA Coverage: When a Participant takes a leave for service in the Uniformed Services, USERRA coverage for the Participant (and Covered Dependents for whom coverage is elected) begin the day after the Participant (and Covered Dependents) lose coverage under the Plan, and it may continue for up to 24 months. However, USERRA coverage will end earlier if one of the following events takes place: Participant fails to make a premium payment within the required time;
Participant fails to return to work within the time frame required under USERRA (see below) following the completion of Participant’s service in the Uniformed Services; or
Participant loses rights under USERRA as a result of a dishonorable discharge or other conduct specified in USERRA. Returning to Work: Participant’s right to continue coverage under USERRA will end if Participant does not notify the Employer of the intent to return to work within the time frame required under USERRA following the completion of Participant’s service in the Uniformed Services by either reporting to work (when absence was for less than 31 days) or applying for reemployment (if absence was for more than 30 days). If continuation is elected COBRA coverage and USERRA coverage begin at the same time and run concurrently. However, COBRA coverage can continue longer, depending on the qualifying event, and is subject to different early termination provisions. In contrast, USERRA coverage can continue for up to 24 months, as described earlier in this Section.
Family and Medical Leave: The Family and Medical Leave Act of 1993 (“FMLA”) applies to the Plan during any calendar year
when the Employer employs 50 or more employees (including part-time employees) each working day during 20 or more calendar weeks in the current or preceding calendar year. Further, the FMLA provisions apply only to eligible employees (i.e., participating employees who have been employed by the Employer for at least 12 months and who have worked at least 1,250 hours in the 12-month period immediately preceding the taking of the FMLA leave). A participant on an FMLA leave may continue health coverage during the leave on the same basis and at the same participant contribution rate as if the employee had continued in active employment continuously for the duration of the leave. The maximum period of an FMLA leave is generally 12 weeks per 12-month period (as that 12-month period is defined by the Employer). However, if an employee takes a leave under the FMLA to care for a qualifying military service member injured in the line of active duty, the maximum period of FMLA is 26 weeks per 12-month period. If health coverage ends at the end of an FMLA leave, COBRA continuation coverage is available.
If a Participant is on a leave of absence under the Family and Medical Leave Act (FMLA), the Participant may continue coverage under a Component Benefit Program that is a health plan. Such coverage is subject to the FMLA and to the terms of the Component Benefit Program. Such coverage is also subject to the following conditions:
The Participant must pay any required employee contribution; and
The Participant must obtain written approval of leave from the Company.
Coverage will be continued for up to the greater of:
The leave period required by the FMLA; or
The leave period required by a similar state law. Conversion Privileges: When you or one of your dependents are no longer eligible under the Plan (either as an active participant, the eligible dependent of an active participant, or as a qualified beneficiary receiving continuation coverage), you and/or your dependents may be eligible to obtain an
individual conversion policy for one or more of your insured benefits. The availability of this conversion coverage and the rules concerning your eligibility are set forth in the policy with each insurance carrier.
Plan Benefits
SPMI has contracted with MetLife and AFLAC to provide you and your dependents with certain Dental, Vision, and Supplemental insurance benefits. The Plan provides Dental, Vision, and Supplemental insurance to eligible employees and their eligible spouses and dependents. A summary of the benefits provided under this Plan are set forth in the certificate of coverage insurance booklet issued by MetLife and AFLAC. You must read the booklet to understand your benefits. If you did not receive the certificate of coverage insurance booklet please contact MetLife and AFLAC or SPMI
PLEASE READ THIS DOCUMENT CAREFULLY AND KEEP FOR FUTURE REFERENCE
SPMI Plan
To request a copy of this Wrap-Around Plan Document and Summary Plan Description in a larger font, please contact SPMI Benefits Department at (800) 940-8706 or at [email protected]
Benefits Department to request a new copy. These benefits are outlined in the Certificate of Coverage issued to you by MetLife and AFLAC and may include the following information, if applicable:
A detailed schedule of benefits and cost-sharing provisions, to include deductibles, coinsurance or copayment amounts for which participants and/or beneficiary will be responsible
Any annual or lifetime caps or other limits on benefits
The extent to which preventive services are covered
Whether (and under what circumstances) existing and new drugs are covered
Details of coverage for medical tests, devices and procedures
Provisions regarding the use of network (if any) and out-of-network (if any) providers and services
Circumstances under which coverage is provided for out of network services
Conditions or limits on the selection of primary care providers (PCPs)
Conditions or limits on the selection of providers of specialty medical care
Conditions or limits applicable to obtaining emergency care
Requirements for pre-authorization and utilization review as a condition to obtaining a benefit of service under the plan
Circumstances that may result in disqualification or ineligibility under the plan, or in the denial, loss, forfeiture, suspension, offset, reduction, or recovery (e.g., by subrogation or reimbursement rights) of any benefits under the plan
The eligibility and participant conditions for any dependent coverage
A summary of the claim procedures
Claims Procedures: The Insurance Company is responsible for evaluating all benefit claims under the plan. The Insurance Company will decide your claim in accordance with its reasonable claims procedures, as required by ERISA. Claims procedures on how to file a claim and how claims are processed are fully described in the Certificate of Coverage. These include procedures for obtaining pre-authorizations, approvals, utilization review decisions, procedures for filing claims, notification of benefit determinations, grievance procedures for the review and appeal of denied claims. If your claim is denied, you may appeal to the Insurance Company for a review of the denied claim. The Insurance Company will decide your appeal in accordance with its reasonable claims procedures, as required by ERISA. See your certificate of coverage insurance booklet issued by MetLife and AFLAC for information about how to appeal a denied claim, the required timeframe to appeal a claim and
for complete details regarding the Insurance Company’s claims procedures. Listing of Provider Networks: To find the most up to date listing of network providers contact the insurance carrier at the phone number found in the back of your ID card and/or by visiting their website also found on the back of your ID card. You can also request printed copy free of charge by contacting SPMI Benefits Department. Termination and Amendment: Benefits under this plan are not vested. SPMI reserves the right to terminate the plan or amend or eliminate benefits under MetLife and AFLAC at any time in its discretion. The plan may be amended or terminated by a written instrument duly adopted by SPMI or any of its delegates.
Plan Administration: The Plan Administrator has delegated responsibility for determinations regarding covered benefits and the amount and manner of the payment of benefits, including the appeal of denied claims, to MetLife and AFLAC, the insurer of the plan.
No Contract of Employment: The plan is not intended to be, and may not be construed as constituting, a contract or other arrangement between you and your employer to the effect that you will be employed for any specific period of time.
Preexisting Conditions and Other Exclusions: Other circumstances that can result in the termination, reduction, loss or denial of benefits (including exclusions due to preexisting conditions and exclusions for certain medical procedures) are described in the certificate of coverage insurance booklet issued by MetLife and AFLAC. Please read the booklet carefully. The Plan’s Initial Preexisting conditions notice and the Plan’s Special Enrollment Notice contain important information about the exclusions due to preexisting conditions and special enrollment rights that you may have.
Power and Authority of Insurance Company: This Plan is fully insured. Benefits are provided under a group insurance contract entered into between SPMI and MetLife and AFLAC. Claims for benefits are sent to the Insurance Company. The Insurance Company, MetLife and AFLAC, is responsible for paying claims.
The Insurance Company is the Named Fiduciary for benefit appeals and is responsible for:
Determining eligibility for and the amount of any benefits payable under the Plan; and
Providing the claims procedures to be followed and the claims forms to be used by eligible individuals pursuant to the Plan.
PLEASE READ THIS DOCUMENT CAREFULLY AND KEEP FOR FUTURE REFERENCE
SPMI Plan
To request a copy of this Wrap-Around Plan Document and Summary Plan Description in a larger font, please contact SPMI Benefits Department at (800) 940-8706 or at [email protected]
The Insurance Company also has the authority to require eligible individuals to furnish it with such information as it determines is necessary for the proper administration of the Plan.
Certificate of Health Plan Coverage: If you have lost or misplaced your copy of your Certificate of Coverage and would like to request a copy you can contact SPMI, 1701 Main St. Van Buren, AR 72956; Phone: 479-474-7752
You may contact the carriers:
MetLife - Dental PO Box 981282 El Paso, TX 79998-1282 Phone: 800-275-4638 AFLAC - Supplemental 1932 Wynnton Road Columbus, Georgia 31999 Phone: 800-992-3522
You can also contact SPMI Benefits Department: 1701 Main St. Van Buren, AR 79265 Phone: (479) 474-7752 E-Mail: ; website: www.myhrprofessionals.com
Your Questions
If you have any general questions regarding the Plan, please contact SPMI, as Plan Administrator.
However, if you have questions regarding eligibility for and/or the amount of any benefits payable under the Plan, please contact MetLife and AFLAC.
Governing Law
The Plan is primarily subject to the Employee Retirement Income Security Act of 1974 (“ERISA”), as well as other various federal laws, including, but not limited to, the Newborns’ and Mothers’ Health Protection Act, the Women’s Health and Cancer Rights Act, HIPAA, Michelle’s Law, FMLA, COBRA, USERRA and Patient Protection and Affordable Care Act (PPACA), as well as certain state insurance laws. However, the Plan may include certain benefits (such as, but not limited to dependent care flexible spending account) that are not subject to ERISA.
Procedures for Requesting Certificates of Creditable Coverage You and your dependents may request a certificate at any time while you are covered under the group plan and up to
24 months after losing coverage under the Plan. You may contact MetLife and AFLAC to request one.
Statement of ERISA Rights
As a participant in the Dental, Vision, and/or Supplemental plans you are entitled to certain rights and protections under the Employee Retirement Income Security Act of 1974 (ERISA). ERISA provides that all plan participants shall be entitled to:
Receive Information About Your Plan and Benefits
Examine, without charge, at the Plan Administrator's office and at other specified locations, such as at a worksite, all documents governing the plan, including insurance contracts and, if the plan covers more than 100 participants at the beginning of the plan year, a copy of the latest annual report (Form 5500 Series) filed by the plan with the U.S. Department of Labor and available at the Public Disclosure Room of the Employee Benefits Security Administration.
Obtain, upon written request to the Plan Administrator, copies of documents governing the operation of the plan, including insurance contracts and copies of the latest annual report (Form 5500 Series), if any, and updated summary plan description. The administrator may make a reasonable charge for the copies.
Receive a summary of the plan's annual financial report, if one is required. The Plan Administrator is required by law to furnish each participant with a copy of this summary annual report.
HIPAA Rights
Reduction or elimination of exclusionary periods of coverage for pre-existing conditions under another group health plan, if you have creditable coverage from this plan. You should be provided a certificate of creditable coverage, free of charge, when you lose coverage under this plan, when you become entitled to elect COBRA continuation coverage, when your COBRA continuation coverage ceases, if you request it before losing coverage, or if you request it up to 24 months after losing coverage. This may reduce or eliminate exclusionary periods of coverage for pre-existing conditions if you join a plan that excludes or limits pre-existing conditions. Without evidence of creditable coverage, you may be subject to a pre-existing condition exclusion for 12 months (18 months for late enrollees) after your enrollment date in your coverage.
Plan Fiduciaries
In addition to creating rights for plan participants ERISA imposes duties upon the people who are responsible for the

PLEASE READ THIS DOCUMENT CAREFULLY AND KEEP FOR FUTURE REFERENCE
SPMI Plan
To request a copy of this Wrap-Around Plan Document and Summary Plan Description in a larger font, please contact SPMI Benefits Department at (800) 940-8706 or at [email protected]
operation of the plan. The people who operate your plan, called "fiduciaries" of the plan, have a duty to do so prudently and in the interest of you and other plan participants and beneficiaries. No one, including your employer or any other person, may fire you or otherwise discriminate against you in any way to prevent you from obtaining a welfare benefit or exercising your rights under ERISA.
Enforce Your Rights
If your claim for a welfare benefit is denied or ignored, in whole or in part, you have a right to know why this was done, to obtain copies of documents relating to the decision without charge, and to appeal any denial, all within certain time schedules.
Under ERISA, there are steps you can take to enforce the above rights. For instance, if you request a copy of plan documents or the latest annual report from the plan and do not receive them within 30 days, you may file suit in a Federal court. In such a case, the court may require the Plan Administrator to provide the materials and pay you up to $110 a day until you receive the materials, unless the materials were not sent because of reasons beyond the control of the administrator. If you have a claim for benefits that is denied or ignored, in whole or in part, you may file suit in a state or Federal court. In addition, if you disagree with the plan's decision or lack thereof concerning the qualified status of a domestic relations order or a medical child support order, you may file suit in Federal court. If it should happen that plan fiduciaries misuse the plan's money, or if you are discriminated against for asserting your rights, you may seek assistance from the U.S. Department of Labor, or you may file suit in a Federal court. The court will decide who should pay court costs and legal fees. If you are successful the court may order the person you have sued to pay these costs and fees. If you lose, the court may order you to pay these costs and fees, for example, if it finds your claim is frivolous.
Assistance with Your Questions
If you have any questions about your plan, you should contact the Plan Administrator. If you have any questions about this statement or about your rights under ERISA, or if you need assistance in obtaining documents from the Plan Administrator, you should contact the nearest office of the Employee Benefits Security Administration, U.S. Department of Labor, listed in your telephone directory or the Division of Technical Assistance and Inquiries, Employee Benefits Security Administration, U.S. Department of Labor, 200 Constitution Avenue N.W., Washington, D.C. 20210. You may also obtain certain publications about your rights and responsibilities under ERISA by calling the publications hotline of the Employee Benefits Security Administration or viewing its website at www.dol.gov/ebsa.
Employee Benefit Disclosure Notices Information contained herein does not constitute an insurance certificate or policy. Certificates will be issued to participants by the corresponding insurance carrier. If you would like to request an additional copy of your certificate of coverage please contact SPMI at (800) 940-8706 or benefits@myhrprofessionals. You can also contact the insurance carrier directly at the number listed on the back of your insurance card. DISCLAIMER INFORMATION The analysis of the following plans is a summary. You must refer to the insurance carriers’ contract and plan description for a full list of coverage and exclusions. Conditional Understanding: This document is intended to be a summary document only and is not intended to limit, enhance or supersede the provisions of your employer insurance carrier policies, procedures and contracts which are in place and are the controlling authorities over the plan(s). This form, any Summary of Benefits and/or enrollment forms do not guarantee payment or verify eligibility. Payment of benefits are subject to all terms, conditions, limitations, and exclusions of the member’s contract at time of service. It is assumed that the recipients of this request form will seek an explanation of any items that may be in question. Any existing plan with other carriers should not be cancelled until your request for enrollment has been reviewed and processed as approved by the insurance carriers. SPMI representatives may from time to time provide guidance regarding certain legal requirements affecting health plans, including the requirements of federal and state health care reform legislation. Such guidance is based on good-faith interpretation of laws and regulations currently in effect, and is not intended to be a substitute for legal advice. Employers should contact their own legal counsel for advice regarding legal requirements.
NOTICE OF HIPAA SPECIAL ENROLLMENT RIGHTS If you are declining enrollment for yourself or your dependents (including your spouse) because of other employer group health plan coverage, you may be able to enroll yourself and your dependents in this plan if you or your dependents lose eligibility for that other group coverage (involuntary loss of coverage) or if the employer stops contributing toward your or your dependents’ other group coverage. However, you must request enrollment within 30 days after your or your dependents’ other coverage ends or after the employer stops contributing toward the other coverage. NOTE: A waiver form must be completed when initially declining coverage stating the reason for waiving coverage.
PLEASE READ THIS DOCUMENT CAREFULLY AND KEEP FOR FUTURE REFERENCE
SPMI Plan
To request a copy of this Wrap-Around Plan Document and Summary Plan Description in a larger font, please contact SPMI Benefits Department at (800) 940-8706 or at [email protected]
In addition, if you have a new dependent as a result of marriage, birth, adoption, or placement for adoption, you may be able to enroll yourself and your dependents. However, you must request enrollment within 30 days after the marriage, birth, adoption, or placement for adoption. Effective April 1, 2009, the Children’s Health Insurance Program Reauthorization Act of 2009 creates two new special enrollment rights for employees and/or their dependents. In addition to the special enrollment rights set forth above, all group health plans must also permit eligible employees and their dependent(s) to enroll in an employer plan if the employee requests enrollment under the group health plan within 60 days of the occurrence of the following events:
1. Termination of Medicaid or State Children’s Health Insurance Program (SCHIP) as a result of loss of eligibility- If you or your dependent(s) lose coverage under Medicaid or a state child health plan, you may request to enroll yourself and/or your dependent(s) in our group health plan not later than 60 days after the date coverage ends under Medicaid or the state child health plan.
2. Eligibility for state premium assistance under Medicaid or CHIP- If you and/or your dependent(s) become eligible for financial assistance from Medicaid or a state child health plan, you may request to enroll yourself and/or your dependent(s) under our group health plan, provided that your request is made not later than 60 days after the date that Medicaid or the state child health plan determines that you and/ or your dependent(s) are eligible for such financial assistance. If you and/or your dependent(s) are currently enrolled in our group health plan, you have the option of terminating your and/or your dependent’s (s’) enrollment in our group health plan and enroll in Medicaid or a state child health plan.
Please note that once you terminate your enrollment in our group health plan, your dependent’s (s’) enrollment will be also terminated. All special enrollment requests are processed at the discretion of the insurance carrier and the insurance carrier reserves the right to approve or deny a request after review. Insurance carrier enrollment form (s) must also be completed along with this request form and return to SPMI for further processing. The carrier also reserves the right to request proof of the qualifying event either at the time the special enrollment request is made or at any time thereafter. The carrier will not consider this request unless the carrier’s completed enrollment form is submitted to them for review. The insurance carrier must receive all completed forms within the timeframes specified within this document. Please contact the insurance carrier directly to find out their specific
timeframe requirements for the various special enrollment events. To request special enrollment or obtain more information, please contact the insurance carrier directly at the phone number found on the back of your insurance card or contact SPMI to obtain the carriers’ phone number. To request enrollment forms and to submit the forms please contact SPMI at SPMI Benefits Department P.O. BOX 6040, Van Buren, AR 72956 Phone: (479) 474-7752 or (800)940-8706 Fax: (479) 922-8006 Email:[email protected], Website: www.myhrprofessionals.com. Additional Information: Election can only be made when you are newly eligible (as long as enrollment is completed within the established timeframe allowed by the carriers) and once a year during the open enrollment period. The open enrollment period may be conducted up to 30 days prior to the start of each plan year. The employer reserves the right to modify the plan year or change carriers at any time. Therefore once you have submitted your election for this plan year you will not be able to make another election change until open enrollment. However, you may need to make an election change that is the result of a “qualifying event” that may trigger a special enrollment period for you and/or your dependents. You may have up to 30 days from the qualifying event date to request and submit your forms to request the change. Special enrollment changes may include: marriage, divorce, legal separation, birth or adoption of a child, change in child’s dependent status, death of spouse or other qualified dependent or involuntary loss of other employer group coverage or Medicaid (loss of eligibility) for you or your qualified dependent. The requested change must be consistent with the qualifying event. All qualifying events are processed at the discretion of the insurance carrier and the insurance carrier reserves the right to approve or deny a request after review. The carrier also reserves the right to request proof of the qualifying event either at the time the special enrollment request is made or at any time thereafter. See above for more information regarding special enrollment. ADDITIONAL INFORMATION-SPECIAL ENROLLMENT DUE TO LOSS OF COVERAGE REQUIREMENTS: Under a federal law known as HIPAA, special enrollment rights that allow you to enroll yourself or your eligible dependents in your employers’ group insurance plan may apply if you previously declined your employer’s enrollment for yourself or for an eligible dependent (including your spouse) while other employer group health insurance coverage was in effect for those individuals. In order for these special enrollment rights to apply, certain conditions must be met. In order to qualify for special enrollment rights because of loss of coverage, the employee or dependent must have had other group health plan coverage at the time your employer’s coverage was previously offered. The employee must have
PLEASE READ THIS DOCUMENT CAREFULLY AND KEEP FOR FUTURE REFERENCE
SPMI Plan
To request a copy of this Wrap-Around Plan Document and Summary Plan Description in a larger font, please contact SPMI Benefits Department at (800) 940-8706 or at [email protected]
also stated in writing at that time by completing the insurance carrier waiver form, that coverage was declined because of the other coverage utilizing the insurance carrier’s waiver form. Special Enrollment Events do not apply to plans that are not considered defined as group health plans. In order to qualify for special enrollment rights because of loss of other coverage (involuntary loss), the employee or dependent must have lost other group health plan coverage because:
The coverage was provided under COBRA, and the COBRA coverage was exhausted; or,
The coverage was non-COBRA employer coverage and (a) the coverage terminated due to loss of eligibility for coverage, or (b) the employer stopped contributing toward the other coverage for you or your family members.
For example, a “loss of eligibility” for special enrollment may include:
Loss of eligibility for coverage as a result of divorce Cessation of dependent status
Death of an employee Termination of employment
Reduction in the number of hours of employment that results in a loss of eligibility for plan participation in which you were enrolled.
An individual no longer resides, lives, or works in an HMO service area (whether or not within the choice of the individual), and no other benefit package is available to the individual through the other employer.
If Coverage Was Under COBRA, Entire COBRA Period Must Be Exhausted. If an eligible employee or dependent has COBRA coverage, the coverage must be exhausted in order to trigger a special enrollment right. Generally, this means that the entire 18-, 29-, or 36-month COBRA period must be completed in order to trigger a special enrollment for loss of other coverage. Loss of eligibility does not include a loss resulting from the employee or dependent failure to pay premiums. Note: An employee or dependent that is offered COBRA under the plan under which the coverage is lost (the old plan) is not required to elect COBRA to preserve his or her special enrollment rights under the new plan. But if the employee or dependent does elect COBRA coverage under the old plan, then the entire COBRA period must be exhausted in order for the individual to have another special enrollment right under the new plan. Situations That Do Not Qualify for Special Enrollment:
Reduction of Contributions or Level of Benefits Is Not Sufficient
The special enrollment right for loss of other employer coverage generally requires that coverage be lost involuntarily. A reduction in the level of
benefits under a plan will not trigger a special enrollment right. For example, if an employee loses eligibility for an option (such as an HMO alternative) under his or her spouse’s plan but is still eligible for another health insurance option under that same plan, then no special enrollment will be triggered—coverage was not lost under the plan. However, if no other health insurance option is available to the employee under the plan, then the employee has lost eligibility and would be entitled to special enrollment. The reason for the loss of eligibility does not matter.
Increase in Cost of Coverage Won’t Trigger Special Enrollment Rights. Increases in the cost of coverage do not trigger special enrollment rights unless the other employer completely stops contributing toward the cost of the other coverage for you or your family members.
Other Employer’s Open Enrollment Period Differs. Insurance carriers generally do not allow mid-year enrollment into the employer plans due to another employer’s open enrollment period. An employee may cancel their existing coverage through his/her employer mid-year and transfer to another employer’s plan but only if coverage under spouse’s plan is actually obtained. Request to cancel coverage must be made within 30 days of spouse’s open enrollment.
Changes to Health Care Flexible Spending Account: The special enrollment right for loss of other coverage may permit either an enrollment or increase in a Health Care Flexible Spending Account
USERRA Continuation and reinstatement rights may also be available if you are absent from employment due to service in the uniformed services pursuant to the Uniformed Services Employment and Reemployment Rights Act of 1994 (USERRA). More information about coverage under USERRA is available by contact SPMI at (800)940-8706 or [email protected]
PREMIUM ASSISTANCE UNDER MEDICAID AND THE CHILDREN’S HEALTH INSURANCE PROGRAM (CHIP)
If you or your children are eligible for Medicaid or CHIP and you’re eligible for health coverage from your employer, your state may have a premium assistance program that can help pay for coverage, using funds from their Medicaid or CHIP programs. If you or your children aren’t eligible for Medicaid or CHIP, you won’t be eligible for these premium assistance programs but you may be able to buy individual insurance coverage through the Health Insurance Marketplace. For more information, visit www.healthcare.gov.
PLEASE READ THIS DOCUMENT CAREFULLY AND KEEP FOR FUTURE REFERENCE
SPMI Plan
To request a copy of this Wrap-Around Plan Document and Summary Plan Description in a larger font, please contact SPMI Benefits Department at (800) 940-8706 or at [email protected]
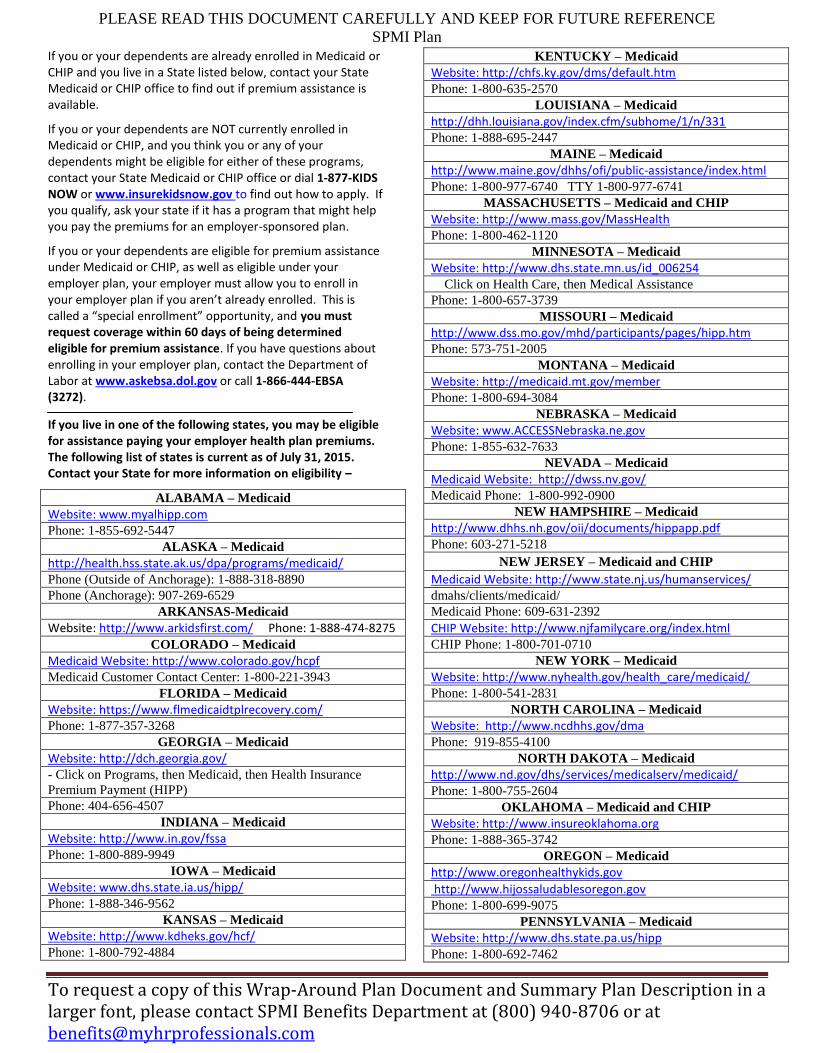
If you or your dependents are already enrolled in Medicaid or CHIP and you live in a State listed below, contact your State Medicaid or CHIP office to find out if premium assistance is available.
If you or your dependents are NOT currently enrolled in Medicaid or CHIP, and you think you or any of your dependents might be eligible for either of these programs, contact your State Medicaid or CHIP office or dial 1-877-KIDS NOW or www.insurekidsnow.gov to find out how to apply. If you qualify, ask your state if it has a program that might help you pay the premiums for an employer-sponsored plan.
If you or your dependents are eligible for premium assistance under Medicaid or CHIP, as well as eligible under your employer plan, your employer must allow you to enroll in your employer plan if you aren’t already enrolled. This is called a “special enrollment” opportunity, and you must request coverage within 60 days of being determined eligible for premium assistance. If you have questions about enrolling in your employer plan, contact the Department of Labor at www.askebsa.dol.gov or call 1-866-444-EBSA (3272).
If you live in one of the following states, you may be eligible for assistance paying your employer health plan premiums. The following list of states is current as of July 31, 2015. Contact your State for more information on eligibility –
ALABAMA – Medicaid
Website: www.myalhipp.com
Phone: 1-855-692-5447
ALASKA – Medicaid
http://health.hss.state.ak.us/dpa/programs/medicaid/
Phone (Outside of Anchorage): 1-888-318-8890
Phone (Anchorage): 907-269-6529
ARKANSAS-Medicaid
Website: http://www.arkidsfirst.com/ Phone: 1-888-474-8275
COLORADO – Medicaid
Medicaid Website: http://www.colorado.gov/hcpf
Medicaid Customer Contact Center: 1-800-221-3943
FLORIDA – Medicaid
Website: https://www.flmedicaidtplrecovery.com/
Phone: 1-877-357-3268
GEORGIA – Medicaid
Website: http://dch.georgia.gov/
- Click on Programs, then Medicaid, then Health Insurance
Premium Payment (HIPP)
Phone: 404-656-4507
INDIANA – Medicaid
Website: http://www.in.gov/fssa Phone: 1-800-889-9949
IOWA – Medicaid
Website: www.dhs.state.ia.us/hipp/ Phone: 1-888-346-9562
KANSAS – Medicaid
Website: http://www.kdheks.gov/hcf/ Phone: 1-800-792-4884
KENTUCKY – Medicaid
Website: http://chfs.ky.gov/dms/default.htm Phone: 1-800-635-2570
LOUISIANA – Medicaid
http://dhh.louisiana.gov/index.cfm/subhome/1/n/331 Phone: 1-888-695-2447
MAINE – Medicaid
http://www.maine.gov/dhhs/ofi/public-assistance/index.html Phone: 1-800-977-6740 TTY 1-800-977-6741
MASSACHUSETTS – Medicaid and CHIP
Website: http://www.mass.gov/MassHealth Phone: 1-800-462-1120
MINNESOTA – Medicaid
Website: http://www.dhs.state.mn.us/id_006254 Click on Health Care, then Medical Assistance
Phone: 1-800-657-3739
MISSOURI – Medicaid
http://www.dss.mo.gov/mhd/participants/pages/hipp.htm Phone: 573-751-2005
MONTANA – Medicaid
Website: http://medicaid.mt.gov/member Phone: 1-800-694-3084
NEBRASKA – Medicaid
Website: www.ACCESSNebraska.ne.gov
Phone: 1-855-632-7633
NEVADA – Medicaid
Medicaid Website: http://dwss.nv.gov/
Medicaid Phone: 1-800-992-0900
NEW HAMPSHIRE – Medicaid
http://www.dhhs.nh.gov/oii/documents/hippapp.pdf Phone: 603-271-5218
NEW JERSEY – Medicaid and CHIP
Medicaid Website: http://www.state.nj.us/humanservices/ dmahs/clients/medicaid/
Medicaid Phone: 609-631-2392
CHIP Website: http://www.njfamilycare.org/index.html CHIP Phone: 1-800-701-0710
NEW YORK – Medicaid
Website: http://www.nyhealth.gov/health_care/medicaid/ Phone: 1-800-541-2831
NORTH CAROLINA – Medicaid
Website: http://www.ncdhhs.gov/dma Phone: 919-855-4100
NORTH DAKOTA – Medicaid
http://www.nd.gov/dhs/services/medicalserv/medicaid/ Phone: 1-800-755-2604
OKLAHOMA – Medicaid and CHIP
Website: http://www.insureoklahoma.org Phone: 1-888-365-3742
OREGON – Medicaid
http://www.oregonhealthykids.gov
http://www.hijossaludablesoregon.gov Phone: 1-800-699-9075
PENNSYLVANIA – Medicaid
Website: http://www.dhs.state.pa.us/hipp Phone: 1-800-692-7462
PLEASE READ THIS DOCUMENT CAREFULLY AND KEEP FOR FUTURE REFERENCE
SPMI Plan
To request a copy of this Wrap-Around Plan Document and Summary Plan Description in a larger font, please contact SPMI Benefits Department at (800) 940-8706 or at [email protected]
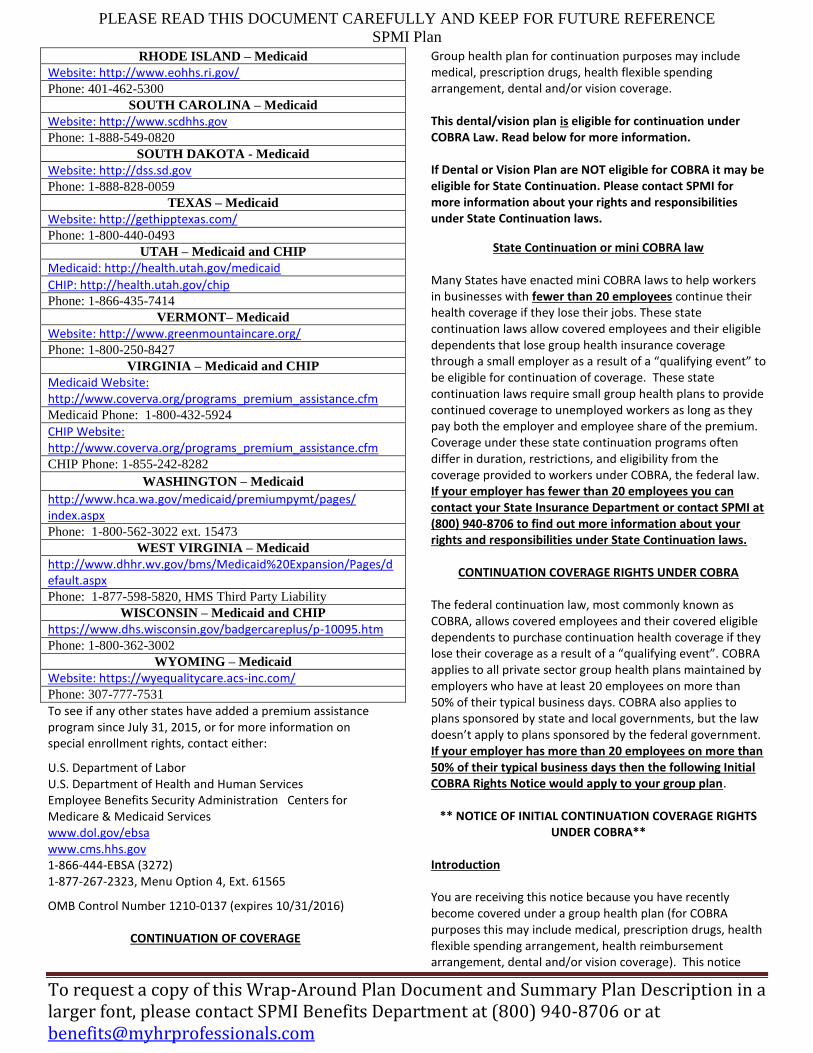
RHODE ISLAND – Medicaid
Website: http://www.eohhs.ri.gov/ Phone: 401-462-5300
SOUTH CAROLINA – Medicaid
Website: http://www.scdhhs.gov Phone: 1-888-549-0820
SOUTH DAKOTA - Medicaid
Website: http://dss.sd.gov Phone: 1-888-828-0059
TEXAS – Medicaid
Website: http://gethipptexas.com/ Phone: 1-800-440-0493
UTAH – Medicaid and CHIP
Medicaid: http://health.utah.gov/medicaid
CHIP: http://health.utah.gov/chip Phone: 1-866-435-7414
VERMONT– Medicaid
Website: http://www.greenmountaincare.org/ Phone: 1-800-250-8427
VIRGINIA – Medicaid and CHIP
Medicaid Website: http://www.coverva.org/programs_premium_assistance.cfm Medicaid Phone: 1-800-432-5924
CHIP Website: http://www.coverva.org/programs_premium_assistance.cfm CHIP Phone: 1-855-242-8282
WASHINGTON – Medicaid
http://www.hca.wa.gov/medicaid/premiumpymt/pages/ index.aspx
Phone: 1-800-562-3022 ext. 15473
WEST VIRGINIA – Medicaid
http://www.dhhr.wv.gov/bms/Medicaid%20Expansion/Pages/default.aspx Phone: 1-877-598-5820, HMS Third Party Liability
WISCONSIN – Medicaid and CHIP
https://www.dhs.wisconsin.gov/badgercareplus/p-10095.htm Phone: 1-800-362-3002
WYOMING – Medicaid
Website: https://wyequalitycare.acs-inc.com/ Phone: 307-777-7531
To see if any other states have added a premium assistance program since July 31, 2015, or for more information on special enrollment rights, contact either:
U.S. Department of Labor U.S. Department of Health and Human Services Employee Benefits Security Administration Centers for Medicare & Medicaid Services www.dol.gov/ebsa www.cms.hhs.gov 1-866-444-EBSA (3272) 1-877-267-2323, Menu Option 4, Ext. 61565
OMB Control Number 1210-0137 (expires 10/31/2016)
CONTINUATION OF COVERAGE
Group health plan for continuation purposes may include medical, prescription drugs, health flexible spending arrangement, dental and/or vision coverage. This dental/vision plan is eligible for continuation under COBRA Law. Read below for more information. If Dental or Vision Plan are NOT eligible for COBRA it may be eligible for State Continuation. Please contact SPMI for more information about your rights and responsibilities under State Continuation laws.
State Continuation or mini COBRA law Many States have enacted mini COBRA laws to help workers in businesses with fewer than 20 employees continue their health coverage if they lose their jobs. These state continuation laws allow covered employees and their eligible dependents that lose group health insurance coverage through a small employer as a result of a “qualifying event” to be eligible for continuation of coverage. These state continuation laws require small group health plans to provide continued coverage to unemployed workers as long as they pay both the employer and employee share of the premium. Coverage under these state continuation programs often differ in duration, restrictions, and eligibility from the coverage provided to workers under COBRA, the federal law. If your employer has fewer than 20 employees you can contact your State Insurance Department or contact SPMI at (800) 940-8706 to find out more information about your rights and responsibilities under State Continuation laws.
CONTINUATION COVERAGE RIGHTS UNDER COBRA
The federal continuation law, most commonly known as COBRA, allows covered employees and their covered eligible dependents to purchase continuation health coverage if they lose their coverage as a result of a “qualifying event”. COBRA applies to all private sector group health plans maintained by employers who have at least 20 employees on more than 50% of their typical business days. COBRA also applies to plans sponsored by state and local governments, but the law doesn’t apply to plans sponsored by the federal government. If your employer has more than 20 employees on more than 50% of their typical business days then the following Initial COBRA Rights Notice would apply to your group plan.
** NOTICE OF INITIAL CONTINUATION COVERAGE RIGHTS UNDER COBRA**
Introduction You are receiving this notice because you have recently become covered under a group health plan (for COBRA purposes this may include medical, prescription drugs, health flexible spending arrangement, health reimbursement arrangement, dental and/or vision coverage). This notice
PLEASE READ THIS DOCUMENT CAREFULLY AND KEEP FOR FUTURE REFERENCE
SPMI Plan
To request a copy of this Wrap-Around Plan Document and Summary Plan Description in a larger font, please contact SPMI Benefits Department at (800) 940-8706 or at [email protected]
contains important information about your right to COBRA continuation coverage, which is a temporary extension of coverage under the Plan. This notice generally explains COBRA continuation coverage, when it may become available to you and your family, and what you need to do to protect the right to receive it. When you become eligible for COBRA, you may also become eligible for other coverage options that may cost less than COBRA continuation coverage. The right to COBRA continuation coverage was created by a federal law, the Consolidated Omnibus Budget Reconciliation Act of 1985 (COBRA). COBRA continuation coverage can become available to you when you would otherwise lose your group health (for COBRA purposes this may include medical, prescription drugs, health flexible spending arrangement, health reimbursement arrangement, dental and/or vision coverage). It can also become available to other members of your family who are covered under the Plan when they would otherwise lose health coverage (for COBRA purposes this may include medical, prescription drugs, health flexible spending arrangement, health reimbursement arrangement, dental and/or vision coverage). This notice only gives a summary of your continuation coverage rights under the plan. For additional information about your rights and obligations under the Plan and under federal law, you should review the Plan’s Summary Plan Description or contact the Plan Administrator. You may have other options available to you when you lose group health coverage. For example, you may be eligible to buy an individual plan through the Health Insurance Marketplace. By enrolling in coverage through the Marketplace, you may qualify for lower costs on your monthly premiums and lower out-of-pocket costs. Additionally, you may qualify for a 30-day special enrollment period for another group health plan for which you are eligible (such as a spouse’s plan), even if that plan generally doesn’t accept late enrollees. Who is my COBRA Administrator? The COBRA administrator for your dental and/or vision plan is: SPMI PO Box 6040 Van Buren, AR 72956 Phone number: (800) 940-8706
What is COBRA Continuation Coverage? COBRA continuation coverage is a continuation of Plan coverage when coverage would otherwise end because of a life event known as a “qualifying event.” Specific qualifying events are listed later in this notice. After a qualifying event, COBRA continuation coverage must be offered to each
person who is a “qualified beneficiary.” You, your spouse, and your dependent children could become qualified beneficiaries if coverage under the Plan is lost because of the qualifying event. Under the Plan, qualified beneficiaries who elect COBRA continuation coverage must pay for COBRA continuation coverage.
If you are an employee, you will become a qualified beneficiary if you lose your coverage under the Plan because either one of the following qualifying events happens:
Your hours of employment are reduced, or
Your employment ends for any reason other than your gross misconduct.
If you are the spouse of an employee, you will become a qualified beneficiary if you lose your coverage under the Plan because any of the following qualifying events happens:
Your spouse dies;
Your spouse’s hours of employment are reduced;
Your spouse’s employment ends for any reason other than his or her gross misconduct;
Your spouse becomes entitled to Medicare benefits (under Part A, Part B, or both); or
You become divorced or legally separated from your spouse.
Your dependent children will become qualified beneficiaries if they lose coverage under the Plan because any of the following qualifying events happens:
The parent-employee dies;
The parent-employee’s hours of employment are reduced;
The parent-employee’s employment ends for any reason other than his or her gross misconduct;
The parent-employee becomes entitled to Medicare benefits (Part A, Part B, or both);
The parents become divorced or legally separated; or
The child stops being eligible for coverage under the plan as a “dependent child.”
Qualified beneficiaries also include a child born to or placed for adoption with the covered employee who satisfies the plan eligibility requirements and becomes covered under the plan during the period of COBRA coverage.
A child of the covered employee who is receiving benefits under the Plan pursuant to a Qualified Medical Support Order (QMCSO) received by the Plan Administrator during the covered employee’s period of employment with the employer is entitled to the same rights under COBRA as a dependent child of the covered employee, regardless of whether that child would otherwise be considered a dependent.
When is COBRA Coverage Available?

PLEASE READ THIS DOCUMENT CAREFULLY AND KEEP FOR FUTURE REFERENCE
SPMI Plan
To request a copy of this Wrap-Around Plan Document and Summary Plan Description in a larger font, please contact SPMI Benefits Department at (800) 940-8706 or at [email protected]
The Plan will offer COBRA continuation coverage to qualified beneficiaries only after the Plan Administrator has been notified that a qualifying event has occurred. When the qualifying event is the end of employment or reduction of hours of employment, death of the employee, commencement of a proceeding in bankruptcy with respect to the sponsoring employer, or the employee becoming entitled to Medicare benefits (under Part A, Part B, or both), the employer must notify the Plan Administrator of the qualifying event.
You Must Give Notice of Some Qualifying Events
For the other qualifying events (divorce or legal separation of the employee and spouse or a dependent child’s losing eligibility for coverage as a dependent child) causing a loss of coverage, you must notify the Plan within 60 days from whichever is later: the date after the qualifying event occurs or the date on which health plan coverage would be lost under the terms of the insurance contract because of the event. The employee or family member can provide notice on behalf of themselves as well as other family members affected by the qualifying event. You must provide notice to SPMI: The insurance carrier requires you provide a change form. Please contact SPMI Benefits department to obtain a Change form. Once you have completed a change form, this form will need to be returned to SPMI Benefits Department for submittal to the insurance carrier.
If you need help acting on behalf of an incompetent beneficiary, please contact SPMI Benefits department for assistance. If this notification is not completed according to the above procedures within the required notification period, then rights to continuation will be forfeited.
How is COBRA Coverage Provided?
Once the Plan Administrator receives notice that a qualifying event has occurred, COBRA continuation coverage will be offered to each of the qualified beneficiaries. Each qualified beneficiary will have an independent right to elect COBRA continuation coverage and will have 60 days to elect continuation coverage. Covered employees may elect COBRA continuation coverage on behalf of their spouses, and parents may elect COBRA continuation coverage on behalf of their children. The 60 day election period is measured from the later of the date of the health plan coverage is lost due to the qualifying event or from the date of COBRA notification. If a qualified beneficiary does not elect continuation coverage within this election period, then rights to continue health insurance will end.
A qualified beneficiary will have to pay the entire applicable premium plus an administrative charge for continuation coverage as allowed by law, currently 2% of the total premiums. These premiums will be adjusted in the future if
the applicable premium amount changes. In addition, if continuation coverage is extended from 18 months to 29 months due to a Social Security disability, your employer can charge up to 150% of applicable premium during the extended coverage period. Premiums are due on the first of every month of continuation of coverage. In addition there will be a maximum grace period of 30 days for the regularly scheduled monthly premiums. Upon expiration of the continuation coverage period, a qualified beneficiary must be allowed to enroll in an individual conversion health plan provided under the employer’s group health plan if an individual conversion plan is available at that time.
Qualified beneficiaries do not have to show they are insurable to elect continuation coverage; however, they must have been covered by the plan for at least one day prior to the qualifying event to be eligible for COBRA continuation coverage. Although a qualified beneficiary participating in COBRA continuation coverage has the same rights as an active participant to add dependents to the plan, those additional dependents may not be qualified beneficiaries. An exception to this rule is if, while on continuation coverage, a baby is born to or adopted by an employee/former employee. Procedures and deadlines for adding these individuals can be found in your summary plan description (benefits booklets-If you need a copy of your summary plan description please contact SPMI Benefits department) and must be followed. Your employer reserves the right to verify COBRA eligibility status and terminate continuation coverage retroactively if you are determined to be ineligible or if there has been a material misrepresentation of the facts.
COBRA continuation coverage is a temporary continuation of coverage. When the qualifying event is the death of the employee, the employee's becoming entitled to Medicare benefits (under Part A, Part B, or both), your divorce or legal separation, or a dependent child's losing eligibility as a dependent child, COBRA continuation coverage lasts for up to a total of 36 months. When the qualifying event is the end of employment or reduction of the employee's hours of employment, and the employee became entitled to Medicare benefits less than 18 months before the qualifying event, COBRA continuation coverage for qualified beneficiaries other than the employee lasts until 36 months after the date of Medicare entitlement. For example, if a covered employee becomes entitled to Medicare 8 months before the date on which his employment terminates, COBRA continuation coverage for his spouse and children can last up to 36 months after the date of Medicare entitlement, which is equal to 28 months after the date of the qualifying event (36 months minus 8 months). If you or anyone in your family becomes entitled to Medicare prior to end of employment or reduction of the employee's hours of employment, it is your responsibility to notify SPMI of the effective date of this entitlement. Otherwise, when the qualifying event is the end of employment or reduction of the employee’s hours of

PLEASE READ THIS DOCUMENT CAREFULLY AND KEEP FOR FUTURE REFERENCE
SPMI Plan
To request a copy of this Wrap-Around Plan Document and Summary Plan Description in a larger font, please contact SPMI Benefits Department at (800) 940-8706 or at [email protected]
employment, COBRA continuation coverage generally lasts for only up to a total of 18 months. There are two ways in which this 18-month period of COBRA continuation coverage can be extended:
1) Disability extension of 18-month period of continuation
coverage If you or anyone in your family covered under the Plan is determined by the Social Security Administration to be disabled and you notify your COBRA Administrator in a timely fashion, you and your entire family may be entitled to receive up to an additional 11 months of COBRA continuation coverage, for a total maximum of 29 months. The disability would have to have started at some time before the 60th day of COBRA continuation coverage; and the qualified beneficiary must notify their COBRA Administrator found on the first page of this notice within 60 days after the determination of disability made by the Social Security Administration. And the disability must last at least until the end of the 18-month period of continuation coverage. It is the qualified beneficiary’s responsibility to obtain this disability determination from the Social Security Administration. It is also the qualified beneficiary’s responsibility to provide a copy of the written determination to SPMI Benefits department within 60 days of the latest of the following occurrences: the date of disability determination by Social Security Administration, the date of the qualifying event or the benefit termination date due to the qualifying event; and before the original 18 months expires. It is also the qualified beneficiary’s responsibility to notify their COBRA Administrator found on the first page of this notice, within 30 days if a final determination has been made that they are no longer disabled. You could be required to pay up to 150 percent of the group rate during the 11
th month extension.
2) Second qualifying event extension of 18-month period of
continuation coverage If your family experiences another qualifying event while receiving 18 months of COBRA continuation coverage, the spouse and dependent children in your family can get up to 18 additional months of COBRA continuation coverage, for a maximum of 36 months, if notice of the second qualifying event is properly given to the COBRA Administrator. This extension may be available to the spouse and any dependent children receiving continuation coverage if the employee or former employee dies, becomes entitled to Medicare benefits (under Part A, Part B, or both), or gets divorced or legally separated, or if the dependent child stops being eligible under the Plan as a dependent child, but only if the event would have caused the spouse or dependent child to lose coverage under the Plan had the first qualifying event not occurred. If a second qualifying event occurs, it is the
qualified beneficiary’s responsibility to notify their COBRA Administrator found on the first page of this notice in writing within 60 days of either the second qualifying event date or the date the qualified beneficiary loses (would lose) coverage under the Plan as a result of the event and within the original 18 month continuation period. In no event, however, will continuation coverage last beyond the 36 months from the date of the event that originally made the qualified beneficiary eligible for continuation of coverage. Are there other coverage options besides COBRA Continuation Coverage?
Yes. Instead of enrolling in COBRA continuation coverage, there may be other coverage options for you and your family through the Health Insurance Marketplace, Medicaid, or other group health plan coverage options (such as a spouse’s plan) through what is called a “special enrollment period.” Some of these options may cost less than COBRA continuation coverage. You can learn more about many of these options at www.healthcare.gov.
If You Have Questions
Questions concerning your Plan or your COBRA continuation coverage rights should be addressed to the contact or contacts identified below. For more information about your rights under ERISA, including COBRA, the Health Insurance Portability and Accountability Act (HIPAA), and other laws affecting group plans, contact the nearest Regional or District Office of the U.S. Department of Labor’s Employee Benefits Security Administration (EBSA) in your area or visit the EBSA website at www.dol.gov/ebsa. (Addresses and phone numbers of Regional and District EBSA Offices are available through EBSA’s website.) For more information about the Marketplace, visit www.HealthCare.gov.
Keep Your Plan Informed of Address Changes
In order to protect your family’s rights, you should keep the Plan Administrator and SPMI Benefits department informed of any changes in the addresses of family members (including yourself) and change in marital status as soon as possible. Failure on your part to do will result in delayed COBRA notifications or a loss of continuation coverage options. If you do not understand any part of this summary notice or have questions the information, please contact your employer or SPMI Benefits department toll free at 1-800-940-8706. You should also keep a copy, for your records, of any notices you send to the Plan Administrator or SPMI Benefits department. Plan Contact Information SPMI Benefits Department P.O. Box 6040 Van Buren, AR 72956
PLEASE READ THIS DOCUMENT CAREFULLY AND KEEP FOR FUTURE REFERENCE
SPMI Plan
To request a copy of this Wrap-Around Plan Document and Summary Plan Description in a larger font, please contact SPMI Benefits Department at (800) 940-8706 or at [email protected]
(p) 1-800-940-8706 (f) 479-922-8006 Email: [email protected]
QUALIFIED MEDICAL CHILD SUPPORT ORDER The components of this Plan that are group health plans extend benefits to a participant’s noncustodial child, as required by any qualified medical child support order (QMCSO), as defined in ERISA section 609(a). The Plan has detailed procedures for determining whether an order qualified as a QMCSO. Participants and beneficiaries can obtain, without charge, a copy of such procedures from the Administrator.
HIPAA NOTICE OF PRIVACY PRACTICES FOR PERSONAL HEALTH INFORMATION
THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. Dear Employee: This is your Notice of Privacy Practices from SPMI. Please read it carefully. You have received this notice because of your employee benefits. SPMI strongly believes in protecting the confidentiality and security of information we collect about you. This notice refers to SPMI as “us”, “we”, or “our”. This notice describes how we protect the protected health information we have about you which relates to your employee benefits and how we may use and disclose this information. Protected Health Information includes individually identifiable information which relates to your past, present or future health, treatment or payment for health care services. This notice also describes your rights with respect to your Protected Health Information and how you can exercise those rights. We are required to provide this Notice to you by the Health Insurance Portability and Accountability Act (HIPAA). For additional information regarding our HIPAA Medical Information Privacy Policy or our general privacy policies, please contact the SPMI Benefits Department, or you may submit questions in writing directly to: SPMI Benefits Department via email at [email protected], via fax: (479) 922-8006 or mail: P.O. Box 6040 Van Buren AR 72956 We are required by law to:
Maintain the privacy of your Protected Health Information (PHI);
Provide you this notice of our legal duties and privacy practices with respect to your PHI, and;
Follow the terms of this notice.
We protect your PHI from inappropriate use or disclosure. Our employees, and those companies that help us service your employee benefits, are required to comply with our requirements that protect the confidentiality of PHI. They may look at your PHI only when there is an appropriate reason to do so, such as to administer the plans. We will not disclose your PHI to any other company for their use in marketing their products to you. However, as described below, we will use and disclose PHI about you for business purposes relating to your employee benefits. The main reasons for which we may use or disclose your PHI are: 1) to assist you in researching medical, dental, flexible spending account, and/or COBRA claims problems; 2) for benefit enrollment purposes and/or 3) for employee benefit plan administration. The following describes these and other possible uses and/or disclosures, together with some examples.
For Payment: We may use and disclose PHI to assist you in researching claims disputes. For example, we may review PHI, at the employee’s request, which is contained on claims submitted by medical or dental providers in an effort to verify that the claims were paid correctly.
For Health Care Operations: We may also use and disclose PHI for benefit plan operations. These purposes include evaluating an employee’s eligibility and administering the employee benefit plans. We may also disclose PHI to a business associate for benefit plan enrollment purposes. PHI may also be disclosed as part of the benefit plan renewal process so that we can make an informed decision regarding any such prospective changes to benefit plans.
Where Required by Law or for Public Health Activities: We disclose PHI when required by federal, state or local law. Examples of such mandatory disclosures include notifying state or local health authorities regarding particular communicable diseases, or providing PHI to a governmental agency or regulator with health care oversight responsibilities. We may also release PHI to a coroner or medical examiner to assist in identifying a deceased individual or to determine the cause of death.
To Avert a Serious Threat to Health or Safety: We may disclose PHI to avert a serious threat to someone’s health or safety. We may also disclose PHI to federal, state or local agencies engaged in disaster relief as well as to private disaster relief or disaster assistance agencies to allow such entities to carry out their responsibilities in specific disaster situations.
PLEASE READ THIS DOCUMENT CAREFULLY AND KEEP FOR FUTURE REFERENCE
SPMI Plan
To request a copy of this Wrap-Around Plan Document and Summary Plan Description in a larger font, please contact SPMI Benefits Department at (800) 940-8706 or at [email protected]
For Health-Related Benefits or Services: We may use PHI to provide you with information about benefits available to you under your current benefits plans.
For Law Enforcement or Specific Government Functions: We may disclose PHI in response to a request by a law enforcement official made through a court order, subpoena, warrant, summons or similar process. We may disclose PHI about you to federal officials for intelligence, counterintelligence, and other national security activities authorized by law.
When Required as Part of a Regulatory or Legal Proceeding: If you or your estates are involved in a lawsuit or a dispute, we may disclose PHI about you in response to a court or administrative order. We may also disclose PHI about you in response to a subpoena, discovery request, or other lawful process by someone else involved in the dispute, but only if efforts have been made to tell you about the request or to obtain an order protecting the PHI requested. We may disclose PHI to any governmental agency or regulator with whom you have filed a complaint or as part of a regulatory agency examination.
Other Uses of PHI: Other uses and disclosures of PHI not covered by this notice and permitted by the laws that apply to us will be made only with your written authorization or that of your legal representative. If we are authorized to use or disclose PHI about you, you or your legally authorized representative may revoke that authorization, in writing, at any time, except to the extent that we have taken action relying on the authorization. You should understand that we will not be able to take back any disclosures we have already made with authorization.
EXAMPLES FOR USES AND DISCLOSURES OF PROTECTED HEALTH INFORMATION We may use or disclosure PHI as permitted or required by law, including, for example: To public health authorities for the purposes of
preventing or controlling disease or other public health purposes;
To appropriate government authorities to report about victims of suspected abuse, neglect, or domestic violence;
In response to subpoenas, discovery requests, or other lawful legal processes in the course of a judicial or administrative proceeding;
To law enforcement authorities as required or permitted by law such as, for example, to report a death, to report a crime on our premises, or if it appears necessary to alert law enforcement to respond to an emergency;
We may disclose PHI if we believe, in good faith, that it is necessary to prevent or lessen a serious and imminent threat to the health or safety of a person or the public;
Other uses and disclosures will be made only with written authorization, which may revoked by notifying our Privacy Officer. We may not sell protected health information.
Your Rights Regarding Personal Health Information We
Maintain About You The following are your various rights as a consumer under HIPAA concerning your PHI. Should you have questions about a specific right, please write to us at the location listed in our discussion of that right.
Right to Inspect and Copy Your Personal Health Information: In most cases, you have the right to inspect and obtain a copy of the PHI that we maintain about you. To inspect and copy PHI, you must submit your request in writing to SPMI Benefits Department. To receive a copy of your PHI, you may be charged a fee for the costs of copying, mailing or other supplies associated with your request. However, certain types of PHI will not be made available for inspection and copying. This includes PHI collected by us in connection with, or in reasonable anticipation of any claim or legal proceeding. In very limited circumstances we may deny your request to inspect and obtain a copy of your PHI. If we do, you may request that the denial be reviewed. An individual chosen by us who was not involved in the original decision to deny your request will conduct the review. We will comply with the outcome of that review.
Right to Amend Your Personal Health Information: If you believe that your PHI is incorrect or that an important part of it is missing, you have the right to ask us to amend your PHI while it is kept by or for us. You must provide your request and your reason for the request in writing, and submit it to SPMI Benefits Department. We may deny your request if it is not in writing or does not include a reason that supports the request. In addition, we may deny your request if you ask us to amend PHI that:
Is accurate and complete;
Was not created by us, unless the person or entity that created the PHI is no longer available to make the amendment;
Is not part of the PHI kept by or for us; or
Is not part of the PHI that you would be permitted to inspect and copy
PLEASE READ THIS DOCUMENT CAREFULLY AND KEEP FOR FUTURE REFERENCE
SPMI Plan
To request a copy of this Wrap-Around Plan Document and Summary Plan Description in a larger font, please contact SPMI Benefits Department at (800) 940-8706 or at [email protected]
Right to a List of Disclosures: You have the right to request a list of the disclosures we have made of PHI about you. This list will not include disclosures made for treatment, payment, health care operations, for purposes or national security, made to law enforcement or to corrections personnel or made pursuant to your authorization or made directly to you. To request this list, you must submit your request in writing to SPMI Benefits Department. Your request must state the time period from which you want to receive a list of disclosures. The time period may not be longer than six years and may not include dates before April 14, 2004. Your request should indicate in what form you want the list (for example, on paper or electronically). The first list you request within a 12-month period will be free. We may charge you for responding to any additional requests. We will notify you of the cost involved and you may choose to withdraw or modify your request at that time before any costs are incurred.
Right to Request Restrictions: You have the right to request a restriction or limitation on PHI we use or disclose about you for treatment, payment or health care operations, or that we disclose to someone who may be involved in your care of payment for your care, like a family member or friend. While we will consider your request, we are not required to agree to it. To request a restriction, you must make your request in writing to SPMI Benefits Department. In your request, you must tell us what information you want to limit, whether you want to limit our use, disclosure or both and to whom you want the limits to apply. We will not agree to restrictions on PHI uses or disclosures that are legally required, or which are necessary to administer our business.
Right to Request Confidential Communications: You have the right to request that we communicate with you about PHI in a certain way or at a certain location if you tell us that communication in another manner may endanger you. For example, you can ask that we only contact you at work or by mail. To request confidential communications, you must make your request in writing to SPMI Benefits Department and specify how or where you wish to be contacted. We will accommodate all reasonable requests.
Right to File a Complaint: If you believe your privacy rights have been violated, you may file a complaint with the Secretary of the Department of Health and Human Services. To file a complaint, please forward all correspondence to SPMI Benefits Department. All complaints must be submitted in writing. You will not be penalized for filing a complaint. If you have
questions about how to file a complaint, please contact:
SPMI Benefits Department P.O. BOX 6040, Van Buren, AR 72956 Phone: (479) 474-7752 or (800)940-8706 Fax: (479) 922-8006 Email:[email protected] Website: www.myhrprofessionals.com
SUMMARY PLAN DESCRIPTION-CAFETERIA PLAN POP PLAN The Employer named below establishes a Premium Only Plan (the “Plan”) as set forth in this Summary Plan Description (“SPD”) as of the Effective Date set forth below. The purpose of the Plan is to provide eligible Employees a choice to pay for his or her share of contribution under one or more insurance plans described in this Plan Information Summary (see “Benefits provided under the Plan”) on a pre-tax salary reduction basis. Pre-tax contribution elections under the Plan are intended to qualify for the exclusion from income provided in Section 125 of the Internal Revenue code of 1986. The Plan Administrator has the exclusive right to interpret the Plan and to decide all matter arising under the Plan, including the right to make determinations of fact and to construe and interpret possible ambiguities, inconsistencies, or omissions in the Plan and this SPD.
Plan Name: Southern Personnel Management, Inc. Cafeteria Plan
Plan Administrator/Agent for Legal Services: SPMI’s CEO
1701 Main St. Van Buren, AR 72956 Telephone Number: Contact SPMI at 479-474-7752 if you have any questions Federal Tax Identification Number: available upon request Plan Number: 501 Effective Date of this Plan: 06/01/1998 Plan Year: 06/01-05/31 Affiliated Employers that will participate in the Plan: See Appendix 1 (available upon request) BENEFITS PROVIDED UNDER THE PLAN The following benefit plans subject (to the terms and conditions of the Plan) are available for eligible employees to elect to pay for with pre-tax dollars. It is intended that such pre-tax contribution amounts shall, for tax purposes, constitute an Employer contribution, but may constitute Employee contributions for state insurance law purposes.
Medical Vision Disability Income Cancer Dental Group Term Basic Life (part of medical policy & under
$50,000 in coverage) Group Term Basic Life (not part of medical policy) Voluntary Life Intensive Care Accident Critical Illness Hospital Indemnity
PLEASE READ THIS DOCUMENT CAREFULLY AND KEEP FOR FUTURE REFERENCE
SPMI Plan
To request a copy of this Wrap-Around Plan Document and Summary Plan Description in a larger font, please contact SPMI Benefits Department at (800) 940-8706 or at [email protected]
Insurance for Specific Disease or Condition Personal Sickness Indemnity
Health Savings Account (as defined in Code Section 223) established with the following Custodian/Trustee:__________________________
Medical Care Expense Reimbursement- $___________ Dependent Care Assistance Program
Administrators of Medical Care Reimbursement Plan and Dependent Care Assistance Program: If medical Care Expense Reimbursement and/or Dependent Care Assistance Program have been marked above, these benefits will be listed in this Plan Information Summary as “Benefits Provided under the Plan” and the SPD for each of these plans adopted by the employer will be set forth in a separate Plan document provided by:________________________ All Employees employed by the Employer shall be eligible to participate under the Plan except the following: PART-TIME LESS THAN 30 HOURS PER WEEK. An eligible Employee may become a Participant in the Plan on the first day of the month following the completion of your worksite employer waiting period. If your worksite employer does not have a waiting period, you may become a participant in the Plan on the first day of the month following a 3 month waiting period. Your employer (the "Employer") is pleased to sponsor an employee benefit program known as a "Premium Only Plan" (the "Plan") for you and your fellow employees. Under federal tax laws, it is also known as a "cafeteria plan". It is so called because it lets you choose from several different insurance and fringe benefit programs according to your individual needs. The Employer provides you with the opportunity to use pre-tax dollars to pay for them by entering into a salary redirection arrangement instead of receiving a corresponding amount of your regular pay. This arrangement helps you because the benefits you elect are nontaxable; you save Social Security and income taxes on the amount of your salary redirection. Alternatively, your Employer may allow you to pay for any of the available benefits with after-tax contributions on a salary deduction basis. This Summary Plan Description (“SPD”) describes the basic features of the Plan, how it operates, and how you can get the maximum advantage from it. Information relating to the Plan that is specific to your Employer is described in the Plan Information Summary attached to the front of this SPD. You will be referred to the Plan Information Summary throughout the SPD. The Plan is also established pursuant to a plan document into which this SPD has been incorporated. If there is a conflict between the official plan document and the SPD, the plan document will govern.
You may also be able to make pre-tax contributions to a Health Savings Account (as defined in Code Section 223) through this Plan if Health Savings Accounts are identified as an included benefit under “Benefits Provided under the Plan” in the Plan Information Summary. If Health Savings Accounts are identified as a benefit plan option offered under the Plan, your rights and obligations in regard to such contributions will be set forth in the Health Savings Account Contribution Appendix attached hereto. What Do I need to Know about the Plan?
1. What is the purpose of the Plan? The purpose of the Plan is to allow eligible employees to pay for certain benefits offered under the Plan (called “Benefit Plans or Policies”) with pre-tax dollars called “Pre-tax Contributions”. Pre-tax Contributions are described in more detail in Q-8 of this SPD. 2. What benefits can I purchase on a pre-tax basis through the Plan? You will be able to choose to participate in the Plan's various pre-tax options by filling out any required enrollment form(s) for the component Benefit Plans or Policies offered under the Plan. The complete list of Benefit Plans or Policies offered under the Plan is located in the Plan Information Summary under “Benefits Offered Under the Plan.” NOTE: You may only contribute with Pre-tax Contributions towards the cost of Benefit Plans or Policies that cover you, your legal Spouse, and/or your tax Dependents defined under Internal Revenue Code Section 152. Each Benefit Plan or Policy may define eligible Dependents more narrowly for purposes of coverage under the particular Benefit Plan or Policy. 3. Who can participate in the Plan? Each employee of the Employer (or an Affiliated Employer identified in the Plan Information Summary) who satisfies the eligibility requirements described in the Plan Information Summary and who is eligible to participate in any of the Benefit Plans or Policies offered under the Plan will be eligible to participate in this Plan as of the date described in the Plan Information Summary (see Q-5 of this SPD for instructions on how to become a Participant). Those employees who actually participate in the Plan are called "Participants." The terms of eligibility of this Plan do not override the terms of eligibility of each of the Benefit Plans or Policies offered under the Plan. For the details regarding eligibility provisions, benefit amounts, and premium schedules for each of the Benefit Plans or Policies, please refer to the plan summary for each of the Benefit Plans or Policies listed in the Plan Information Summary. Only coverage for an Employee and the Employee's Dependents may be paid for under this Plan. 4. When does my participation in the Plan end? You can
PLEASE READ THIS DOCUMENT CAREFULLY AND KEEP FOR FUTURE REFERENCE
SPMI Plan
To request a copy of this Wrap-Around Plan Document and Summary Plan Description in a larger font, please contact SPMI Benefits Department at (800) 940-8706 or at [email protected]
continue to participate in the Plan until (i) you elect not to participate in accordance with Q-9 of this SPD; (ii) you no longer satisfy the eligibility requirements described in the Plan Information Summary; (iii) you terminate employment with the Employer; or (iv) the Plan is terminated or amended to exclude you or the class of employees of which you are a member. If your employment with the Employer is terminated during the Plan Year or you otherwise cease to be eligible, your active participation in the Plan will automatically cease, and you will not be able to make any more Pre-tax Contributions under the Plan. If you are rehired within the same Plan Year or you become eligible again, you may make SPD new elections, provided that you are rehired or become eligible again more than 30 days after you terminated employment or lost eligibility. If you are rehired or again become eligible within 30 days or less, your prior elections will be reinstated and remain in effect for the remainder of the Plan Year unless you again lose eligibility. 5. How do I become a Participant? You become a Participant by signing an individual Salary Redirection Agreement (“SRA”) on which you elect one or more of the Benefit Plans or Policies available under the Plan, as well as agree to a salary redirection to pay for those benefits so elected. You will be provided an SRA when you first become eligible to participate in this Plan. You must complete the form and turn it in to the Personnel Office during the applicable enrollment period described in Q-6 below. 6. What are the enrollment periods for entering the Plan? If you are eligible on the effective date of the Plan, you must enroll during the enrollment period immediately preceding the effective date of the Plan. Otherwise, you must enroll during either the “Initial Enrollment Period” or the “Annual Enrollment Period”. You will be notified of the dates that each enrollment period begins and ends in the enrollment material provided to you prior to each enrollment period. If you make an election during the Initial Enrollment Period, your participation in this Plan will begin on the later of your eligibility date described in the Plan Information Summary, the first pay period coinciding with or next following the date that your election is received by the Plan Administrator (or its designated claims administrator) or the date coverage under a Benefit Plan or policy that you elect begins. The effective date of coverage under the applicable Benefit Plan(s) or Policy(ies) is governed by the terms of each Benefit Plan or Policy, as set forth in the governing documents for each Benefit Plan or Policy. The election that you make during the Initial Enrollment Period is effective for the remainder of the Plan Year and generally cannot be revoked during the Plan Year unless you have a Change in Status event as described in Q-9 below. If you do not make an election during the Initial Enrollment Period, you will be deemed to have elected not to participate in this Plan for the remainder of the Plan Year. You may, however, be covered by certain Benefit Plans or Policies automatically (and be required to contribute with
pre-tax dollars) even if you fail to make an election. These automatic Benefit Plans or Policies are called “Default Benefits” and will be identified in the enrollment material that you receive. The election that you make during the Annual Enrollment Period is effective the first day of the next Plan Year and is irrevocable for the entire Plan Year unless you have a Change in Status event described in Q-9 below. A Participant who fails to complete, sign, and file an SRA during the Annual Enrollment Period as required shall be deemed to have elected to continue participation in the Plan with the same benefit elections as during the prior Plan Year (adjusted to reflect any increase/decrease in applicable premiums), and except for a Change in Status, will not be permitted to modify his election until the next Annual Enrollment Period. Notwithstanding the foregoing, annual elections for participation in the Medical Care and Dependent Care Expense Reimbursement Plans, if offered under the Plan, must be made by submitting an SRA prior to the beginning of each Plan Year -- no deemed elections shall occur with respect to such benefits. The Plan Year is generally a 12-month period (except during the initial or last Plan Year of the Plan). The beginning and ending dates of the Plan Year are described in the Plan Information Summary. 7. What tax savings are available through the Cafeteria Plan? For example your semi-monthly gross pay is $1,500 and your semi-monthly premium for health coverage is $100 per check. In addition, your total withholdings (federal income taxes, state income taxes, Social Security and Medicare) are $302.67. After paying for coverage from your after-tax pay, your take home pay is $1,097.33. On the other hand, if you elect to have your premium paid through a pre-tax arrangement you will be considered to have received a semi-monthly gross pay of $1,400 gross pay rather than $1,500 for tax purposes with $100 contributed for health insurance coverage. As a result your take-home pay is increased to $1,126.98 and reducing your total withholdings to $273.02 per pay period. This means you increased your tax-home pay by $29.65 per pay period. 8. How are my contributions made? When you become a Participant, your share of the contributions for the elected Benefit Plan or Policy(ies) will be paid with Pre-tax Contributions elected on the SRA. Pre-tax Contributions are amounts withheld from your gross income before any applicable federal and state taxes have been deducted (some state tax laws do not recognize Pre-tax Contributions). In addition, all or a portion of the cost of the Benefit Plans or Policies may, in the Employer's discretion, be paid with contributions made by the Employer on behalf of each Participant (these are called “Non-elective Contributions”). The amount of Non-elective Contribution that is applied towards the cost of the Benefit Plan(s) or Policy(ies) for each Participant and/or level of coverage is subject to the sole

PLEASE READ THIS DOCUMENT CAREFULLY AND KEEP FOR FUTURE REFERENCE
SPMI Plan
To request a copy of this Wrap-Around Plan Document and Summary Plan Description in a larger font, please contact SPMI Benefits Department at (800) 940-8706 or at [email protected]
discretion of the Employer, and it may be adjusted upward or downward in the Employer's sole discretion. The Non-elective Contribution amount will be calculated for each Plan Year in a uniform and SPD nondiscriminatory manner and may be based upon your Dependent status, commencement or termination date of your employment during the Plan Year, and such other factors that the Employer deems relevant. In no event will any Non-elective Contribution be disbursed to you in the form of additional, taxable Compensation except as otherwise provided in the enrollment material. To the extent set forth in the enrollment material, the Employer may make available a certain amount of Non-elective Contributions and then allow you to allocate the Non-elective Contributions among the various Benefit Plan(s) or Policy(ies) that you choose (subject to restrictions described in the enrollment material). 9. Can I ever change my election during the Plan Year? Generally, you cannot change your election to participate in the Plan or vary the Pre-tax Contribution amounts although your election will terminate if you are no longer working for the Employer or no longer eligible under the terms of the Plan. Otherwise, you may change your elections for Pre-Tax Contributions only during the Annual Enrollment Period, and then, only for the coming Plan Year. There are several important exceptions to this general rule: You may change or revoke your previous election during the Plan Year if you file a written request for change with the Plan Administrator (or its designated claims administrator) within 30 days of any of the following events: 1. Change in Status. If one or more of the following
“Changes in Status” occur, you may revoke your old election and make a new election, provided that both the revocation and new election are on account of and correspond with the Change in Status (as described below). Those occurrences that qualify as a Change in Status include the events described below, as well as any other events that the Plan Administrator determines are permitted under subsequent IRS regulations:
• a change in your legal marital status (such as marriage,
legal separation, annulment, or divorce or death of your Spouse);
• a change in the number of your Dependents (such as the birth of a child, adoption or placement for adoption of a Dependent, or death of a Dependent);
• any of the following events that change the employment status of you, your Spouse, your Dependents, that affect benefit eligibility under a cafeteria plan (including this Plan and the Plan of another employer) or other employee benefit plan of yours, your Spouse, your Dependents. Such events include any of the following changes in employment status: termination or commencement of employment, a strike or lockout, a commencement of or return from an unpaid leave of
absence, a change in worksite, switching from salaried to hourly-paid, union to non-union, or part-time to full-time; incurring a reduction or increase in hours of employment; or any other similar change which makes the individual become (or cease to be) eligible for a particular employee benefit (NOTE: The specific rules governing election changes when you take a leave of absence are described in Q-13 of this SPD);
• an event that causes your Dependent to satisfy or cease to satisfy an eligibility requirement for a particular benefit;
• a change in your, your Spouse's, your Dependent's place of residence.
If a Change in Status occurs and you want to make a corresponding election change, you must inform the Plan Administrator and complete a new election within 30 days from the date of the event. The election change must be on account of and correspond with the Change in Status event as determined by the Plan Administrator with the exception of special enrollment resulting from birth, placement for adoption or adoption, all election changes are prospective. As a general rule, a desired election change will be found to be consistent with a Change in Status event if the event affects eligibility for coverage. A Change in Status affects eligibility for coverage if it results in an increase or decrease in the number of Dependents who may benefit under the plan. In addition, you must also satisfy the following specific requirements in order to alter your election based on that Change in Status: Loss of Spouse or Dependent Eligibility-For accident and health benefits (e.g., health, dental and vision coverage, and Medical Care Reimbursement Plan), a special rule governs which types of election changes are consistent with the Change in Status. For a Change in Status involving your divorce, annulment or legal separation from your Spouse, the death of your Spouse or your Dependent, or your Dependent ceasing to satisfy the eligibility requirements for coverage, your election to cancel accident or health benefits for any individual other than your Spouse involved in the divorce, annulment, or legal separation, your deceased Spouse or Dependent, or your Dependent that ceased to satisfy the eligibility requirements, would fail to correspond with that Change in Status. Hence, you may only cancel accident or health coverage for the affected Spouse or Dependent. Gain of Coverage Eligibility Under Another Employer’s Plan-For a Change in Status in which a Participant or his or her Spouse or Dependent gains eligibility for coverage under a cafeteria plan or qualified benefit plan of the employer of the Participant’s Spouse or Dependent as a result of a change in marital status or a change in employment status, a Participant may elect to cease or decrease coverage for that individual only if coverage for that individual becomes effective or is increased under the Spouse’s or Dependent’s employer’s plan. The Plan Administrator may rely on a
PLEASE READ THIS DOCUMENT CAREFULLY AND KEEP FOR FUTURE REFERENCE
SPMI Plan
To request a copy of this Wrap-Around Plan Document and Summary Plan Description in a larger font, please contact SPMI Benefits Department at (800) 940-8706 or at [email protected]
Participant’s certification that the Participant has obtained or will obtain coverage under the Spouse’s or Dependent’s employer’s plan, unless the Plan Administrator has reason to believe that the Participant’s certification is incorrect. Group Term Life Insurance, Disability Income, or Dismemberment Benefits (if offered under the Plan. See the list of Benefit Plans or Policies offered under the Plan in the Plan Information Summary). For group term life insurance, disability income, and accidental death and dismemberment benefits, if you experience any Change in Status (as described above), you may elect either to increase or decrease coverage. 2. Special Enrollment Rights. If you, your Spouse, and/or a
Dependent are entitled to special enrollment rights under a Benefit Plan or Policy that is a group health plan, you may change your election to correspond with the special enrollment right. Thus, for example, if you declined enrollment in medical coverage for yourself or your eligible Dependents because of outside medical coverage and eligibility for such coverage is subsequently lost due to certain reasons (i.e., due to legal separation, divorce, death, termination of employment, reductions in hours, or exhaustion of COBRA period), you may be able to elect medical coverage under the Plan for yourself and your eligible Dependents who lost such coverage. Furthermore, if you have a new Dependent as a result of marriage, birth, adoption, or placement for adoption, you may also be able to enroll yourself, your Spouse, and your newly acquired Dependents, provided that you request enrollment within the Election Change Period. An election change that corresponds with a special enrollment must be prospective, unless the special enrollment is attributable to the birth, adoption, or placement for adoption of a child, which may be retroactive up to 30 days. Effective April 1, 2009, group health plans will recognize the following as additional special enrollment opportunities for employees and dependents:
Termination of Medicaid or Children’s Health Insurance Program (CHIP) due to loss of eligibility.
Eligibility for state premium assistance under Medicaid or CHIP.
However, you must request enrollment within 60 days after the date of termination of Medicaid or CHIP; or the date the employee or dependent is determined eligible for premium assistance under Medicaid or CHIP. Please refer to the group health plan description for an explanation of special enrollment rights. 3. Certain Judgments, Decrees and Orders. If a judgment,
decree or order from a divorce, separation, annulment, or custody (including a QMCSO) change requires your
Dependent to be covered under this Plan, you may change your election to provide coverage for the Dependent identified in the order(including a foster child who is a dependent of the participant). If the order requires that another individual (such as your former Spouse) cover the Dependent child, and such coverage is actually provided, you may change your election to revoke coverage for the Dependent child.
4. Entitlement to Medicare or Medicaid. If you, your
Spouse, or a Dependent becomes entitled to Medicare or Medicaid, you may cancel that person’s accident or health coverage. Similarly, if you, your Spouse, or a Dependent who has been entitled to Medicare or Medicaid loses eligibility for such, you may, subject to the terms of the underlying plan, elect to begin or increase that person’s accident or health coverage.
5. Change in Cost. If you are notified that the cost of your
Benefit Plan or Policy coverage under the Plan significantly increases or decreases during the Plan Year, you may make certain election changes. If the cost significantly increases, you may choose either to make an increase in your contributions, revoke your election and receive coverage under another Benefit Plan or Policy that provides similar coverage, or drop altogether if no similar coverage exists. If the cost significantly decreases, you may revoke your election and elect to receive coverage provided under the option that decreased in cost. For insignificant increases or decreases in the cost of Benefits Plans or Policies, however, your Pre-tax Contributions will automatically be adjusted to reflect the minor change in cost. The Plan Administrator will have final authority to determine whether the requirements of this section are met. (Please note that none of the above “Change in Cost” exceptions are applicable to a Medical Care Reimbursement Plan, to the extent offered under the Plan.)
6. Change in Coverage. If you are notified that your
Benefit Plan or Policy coverage under the Plan is significantly curtailed, you may revoke your election and elect coverage under another Benefit Plan or Policy that provides similar coverage. If the significant curtailment amounts to a complete loss of coverage, you may also drop coverage if no other similar coverage is available. Further, if the Plan adds or significantly improves a benefit option during the Plan Year, you may revoke your election and elect to receive on a prospective basis coverage provided by the newly added or significantly improved option, so long as the newly added or significantly improved option provides similar coverage. Also, you may make an election change that is on account of and corresponds with a change made under another employer plan (including a plan of the Employer or another employer), so long as: (a) the other
PLEASE READ THIS DOCUMENT CAREFULLY AND KEEP FOR FUTURE REFERENCE
SPMI Plan
To request a copy of this Wrap-Around Plan Document and Summary Plan Description in a larger font, please contact SPMI Benefits Department at (800) 940-8706 or at [email protected]
employer plan permits its participants to make an election change permitted under the IRS regulations; or (b) the Plan Year for this Plan is different from the Plan Year of the other employer plan. Finally, you may change your election to add coverage under this Plan for yourself, your Spouse, or your Dependent if such individual(s) loses coverage under any group health coverage sponsored by a governmental or educational institution. The Plan Administrator will have final discretion to determine whether the requirements of this section are met. (Please note that none of the above “Change in Coverage” exceptions are applicable to the Medical Care Reimbursement Plan, to the extent offered under the Plan.) Additionally, your election(s), may be modified downward during the Plan Year if you are a Key Employee or Highly Compensated Individual (as defined by the Internal Revenue Code), if necessary to prevent the Plan from becoming discriminatory within the meaning of the federal income tax law.
10. How long will the Plan remain in effect? Although the Employer expects to maintain the Plan indefinitely, it has the right to modify or terminate the program at any time for any reason. It is also possible that future changes in state or federal tax .laws may require that the Plan be amended accordingly. 11. What happens if my claim for benefits under this Plan is denied? This SPD describes the basic features of the Plan. If your claim is for a benefit under one of the component Benefit Plans or Policies, you will generally proceed under the claims procedures applicable under the component Benefit Plan or Policy (see the plan summary for each of the Benefit Plans or Policies that you elect); However, if you are denied a benefit under this Plan, the claims procedure under this Plan will apply. You will be notified if your claim under the Plan is denied. The notice of denial will be furnished to you within 30 days after receiving your claim. However, if additional time is needed to process your claim you will be notified before the initial 30-day period has expired. The notice will explain why an extension is necessary and the date a decision is expected to be rendered. In no event will an extension go beyond 15 days after the end of the initial 30-day period. The notice of the denial will include the specific reasons for the denial and the relevant plan provisions on which the denial was based. If your claim is denied in whole or in part, you may appeal by requesting a review of the denied claim, as set forth in the notice of denial, within 180 days after you receive notice of the denial. If there are two levels of appeal (as indicated in the notice of denial), you will have a reasonable amount of time in which to request a second review and such time period will be identified in the notice of denial. As part of the appeal process (whether there is one or two appeals), you or your authorized representative may examine documents, records, and other information relevant to your claim and
submit issues, documents and comments in writing. Within 60 days after the request for review is received, you will be notified in writing of the decision on review. The notice of denial will indicate whether there are one or two levels of appeals and will contain the same type of information provided to you in the first notice of denial. If there are two levels of Plan appeals, the decisions on appeal will be made within 30 days after the request for each review is received. The Plan Administrator is the claims fiduciary for making the final decision under the plan. In the event of your death, your beneficiary has the same rights and is subject to the same time limits and other restrictions that would otherwise apply to you under the claims procedures explained above. 12. What happens if I take a leave of absence?
If you go on a qualifying unpaid leave under the Family and Medical Leave Act of 1993 (FMLA), to the extent required by the FMLA, the Employer will continue to maintain your Benefit Plans or Policies providing health coverage on the same terms and conditions as though you were still active (e.g., the Employer will continue to pay its share of the contribution to the extent you opt to continue coverage.)
Your Employer may elect to continue all coverage for Participants while they are on paid leave (provided Participants on non-FMLA paid leave are required to continue coverage). If so, you will pay your share of the contributions by the method normally used during any paid leave (for example, with Pre-tax Contributions if that is what was used before the FMLA leave began).
In the event of unpaid FMLA leave (or paid leave where coverage is not required to be continued), if you opt to continue your group health coverage you may pay your share of the contribution with after-tax dollars while on leave, or you may be given the option to pre-pay all or a portion of your share of the contribution for the expected duration of the leave with Pre-tax Contributions from your pre-leave compensation by making a special election to that effect before the date such compensation would normally be made available to you provided, however, that pre-payments of Pre-tax Contributions may not be utilized to fund coverage during the next Plan Year, or by other arrangements agreed upon between you and the Plan Administrator (for example, the Plan Administrator may fund coverage during leave and withhold amount from your compensation upon return from leave). The payment options provided by the Employer will be established in accordance with Code Section 125, FMLA and the Employer’s internal policies and procedures regarding leaves of absence. Alternatively, the Employer may require all Participants to continue coverage during the leave. If so, you may elect to discontinue your share of
PLEASE READ THIS DOCUMENT CAREFULLY AND KEEP FOR FUTURE REFERENCE
SPMI Plan
To request a copy of this Wrap-Around Plan Document and Summary Plan Description in a larger font, please contact SPMI Benefits Department at (800) 940-8706 or at [email protected]
the required contributions until you return from leave. Upon return from leave you will be required to repay the contribution not paid during the leave in a manner agreed upon with the Administrator.
If your coverage ceases while on FMLA leave (e.g., for non-payment of required contributions), you will be permitted to re-enter the Plan upon return from such leave on the same basis as you were participating in the Plan prior to the leave, or as otherwise required by the FMLA. Your coverage under the Benefit Plans or Policies providing health coverage may be automatically reinstated provided that coverage for Employees on non-FMLA leave is automatically reinstated upon return from leave.
The Employer may, on a uniform and consistent basis, continue your group health coverage for the duration of the leave following your failure to pay the required contribution. Upon return from leave, you will be required to repay the contribution in a manner agreed upon by you and Employer.
If you are commencing or returning from unpaid FMLA leave, your election under this Plan for Benefit Plans or Policies providing non-health benefits shall be treated in the same manner that elections for non-health Benefit Plans or Policies are treated with respect to Participants commencing and returning from unpaid non-FMLA leave.
If you go on an unpaid non-FMLA leave of absence that does not affect Eligibility offered under this plan, then you will continue to participate and the contribution due will be paid with a pre-payment before going on leave, by after-tax contributions while on leave, or with catch-up contributions after the leave ends, as may be determined by the Plan. If you go on an unpaid leave that affects eligibility the election change rules in Q-9 of this SPD will apply. The Plan Administrator will have discretion to determine whether taking an unpaid non-FMLA leave of absence affects eligibility.
13. Is there any other information that I should know about the Plan? Participation in the Plan does not give any Participant the right to be retained in the employ of his or her Employer or any other right not specified in the Plan. The Plan Administrator’s name, address, and telephone number appear in the Plan Information Summary attached to the front of the SPD. The Plan Administrator has the exclusive right to interpret the Plan and to decide all matter arising under the Plan, including the right to make determinations of fact, and construe and interpret possible ambiguities, inconsistencies, or omissions in the Plan and this SPD. Other important information such as the Plan Number and Plan Sponsor’s name and address has also been provided in the
Plan Information Summary. 14. What are my rights under ERISA? As a participant in this Plan you are entitled to certain rights and protections under the Employee Retirement Income Security Act of 1974. ERISA provides that all plan participants shall be entitled to examine, without charge, at the plan administrator’s office and at other specified location, such as worksites all plan documents, including insurance contracts, copies of the latest Form 5500, if applicable, updated summary plan description, collective bargaining agreements and copies of all documents filed by the plan with the Department of Labor, such as detailed annual reports and plan descriptions. In addition, ERISA imposes duties upon the people who are responsible for the operation of the employee benefit plan. The people who operate the plan, called “fiduciaries" of the plan have a duty to do so prudently and in the interest of you and other participants and beneficiaries. No one, including your employer, union or any other person, may fire you or otherwise discriminate against you in any way to prevent you from obtaining a welfare benefit or exercising your rights under ERISA. If your claim for a welfare benefit is denied in whole or in part you must receive a written explanation of the reason of denial. You have the right to have the plan review and reconsider your claim. Under ERISA, there are steps you can take to enforce the above rights. If you have any questions about this statement or about your rights under ERISA, you should contact the nearest office of the Pension and Welfare Benefits Administration, U.S. Department of Labor, listed in your telephone directory or the Division of Technical Assistance and Inquiries, Pension and Welfare Benefit Administration, U.S. Department, 200 Constitution Ave N.W., Washington, D.C. 20210. 15. Health Savings Accounts (HSA):
What are “HSA Benefits”? An HSA permits Employees to make pre-tax contributions to an HSA established and maintained outside the Plan with the Employee’s HSA trustee/custodian. For purposes of this Cafeteria Plan, HSA Benefits consist solely of the ability to make such pre-tax contributions under this Cafeteria Plan. If you elect HSA Benefits, then you will be able to provide a source of pre-tax contributions by entering into a Salary Reduction Agreement with your Employer. Because the share of the contributions that you pay will be with pre-tax funds, you may save both federal income taxes and FICA taxes. To participate in the HSA Benefits, you must be an “HSA-Eligible Individual.” This means that you are eligible to contribute to an HSA under the requirements of Code § 223 and that you have elected qualifying High Deductible Health Plan coverage offered by the Employer and have not elected any disqualifying Non- High Deductible Health Plan coverage offered by the Employer. (“High Deductible Health Plan” means the high deductible health plan offered by your Employer that is intended to qualify as a high deductible health plan under Code § 223(c)(2), as described in materials
PLEASE READ THIS DOCUMENT CAREFULLY AND KEEP FOR FUTURE REFERENCE
SPMI Plan
To request a copy of this Wrap-Around Plan Document and Summary Plan Description in a larger font, please contact SPMI Benefits Department at (800) 940-8706 or at [email protected]
that will be provided separately to you by the Employer.) If you elect HSA Benefits, you will be required to certify that you meet all of the requirements under Code § 223 to be eligible to contribute to an HSA. These requirements include such things as not having any disqualifying coverage—and you should be aware that coverage under a Spouse’s plan could make you ineligible to contribute to an HSA. In order to elect HSA Benefits under the Plan, you must establish and maintain an HSA outside of the Plan with an HSA trustee/custodian and you must provide sufficient identifying information about your HSA to facilitate the forwarding of your pre-tax Salary Reductions through the Employer’s payroll system to your designated HSA trustee/custodian. You may also want to review IRS Publication 969 (“Health Savings Accounts and Other Tax-Favored Health Plans”).
What is my “HSA”? The HSA is not an employer-sponsored employee benefit plan—it is an individual trust or custodial account that you open with an HSA trustee/custodian to be used primarily for reimbursement of “eligible medical expenses” as set forth in Code § 223. Your HSA is administered by your HSA trustee/custodian. Consequently, an HSA trustee/custodian, not the Employer, will establish and maintain your HSA. Your Employer’s role is limited to allowing you to contribute to your HSA on a pre-tax Salary-Reduction basis. The HSA trustee/custodian will be chosen by you, as the Participant, and not by the Employer. Your Employer may, however, limit the number of HSA providers to whom it will forward pretax Salary Reductions, a list of whom will be provided upon request. Any such list of HSA trustees/custodians, however, shall be maintained for administrative simplification and shall not be an endorsement of any particular HSA trustee/custodian. Your Employer has no authority or control over the funds deposited in your HSA. The Plan Administrator will maintain records to keep track of HSA contributions that you make via pre-tax Salary Reductions, but it will not create a separate fund or otherwise segregate assets for this purpose.
What are the maximum HSA Benefits that I may elect under the Cafeteria Plan?
Your annual contribution you elect must not exceed the statutory maximum amount for HSA contributions applicable to your High Deductible Health Plan coverage option (i.e., single or family) for the calendar year in which the contribution is made. For 2013 the statutory limit is $3,250 for single coverage and $6,450 for family (This limit may be adjusted each year by the IRS). An additional catch-up contribution of up to $1,000 may be made if you are age 55 or older. In addition, the maximum annual contribution shall be: (a) reduced by any matching (or other) Employer contribution made on your behalf and (b) pro-rated for the number of months in which you are an HSA-Eligible Individual. Note that if you are an HSA-Eligible Individual for only part of the year but you meet all of the requirements under Code § 223 to be eligible to contribute to an HSA on December 1, you may be able to contribute up to the full
statutory maximum amount for HSA contributions applicable to your coverage option (i.e., single or family). However, any contributions in excess of your annual contribution under the Plan for HSA benefits (as described above), but not in excess of the applicable full statutory maximum amount, must be made outside the Plan. In addition, if you do not remain eligible to contribute to an HSA under the requirements of Code § 223 during the following year, the portion of HSA contributions attributable to months that you were not actually eligible to contribute to an HSA will be includible in your gross income and subject to a 10% penalty (exceptions apply in the event of death or disability).
How are my HSA Benefits paid for under the Cafeteria Plan?
When you complete the Salary Reduction Agreement, you specify the amount of HSA Benefits that you wish to pay for with your salary reduction. From then on, you make a contribution for such coverage by having that portion deducted from each paycheck on a pre-tax basis (generally an equal portion from each paycheck or an amount otherwise agreed to or as deemed appropriate by the Plan Administrator). Such contributions will be forwarded to the HSA trustee/custodian (or its designee) within a reasonable time after being withheld. Your Employer has no authority or control over the funds deposited in your HSA.
Can I change my HSA Contribution under the Cafeteria Plan?
Unlike the other benefits offered under the Cafeteria Plan, you may increase, decrease, or revoke your HSA contribution election at any time during the plan year for any reason by submitting an election change form to the Plan Administrator (or to its designee). Your election change will be prospectively effective on the first day of the month following the month in which you properly submitted your election change. Your ability to make pre-tax contributions under this Plan to the HSA identified above ends on the date that you cease to meet the eligibility requirements

To request a copy of this Wrap-Around Plan Document and Summary Plan Description in a larger font, please contact SPMI Benefits Department at (800) 940-8706 or at [email protected]