Embed Size (px)
Citation preview

Wrist Disorders: What Should We Be Looking for with Imaging Techniques?
Thomas H. Berquist, MD, FACR Professor of Diagnostic Radiology, Mayo Medical School; Chair, Department of Diagnostic Radiology, Mayo Clinic Jacksonville, Jacksonville, Florida
I maging techniques play an important role in evaluating the complex bone and soft-tissue
anatomy of the wristY Routine radiographs are obtained for initial screening. Additional radiographic techniques or procedures are performed based upon clinical features and findings found on radiographs. Computed tomography (CT), magnetic resonance imaging (MRI), radionuclide scintigraphy, ultrasonography, and arthrography / tenography also play important roles in diagnosing disorders of the wrist. 1-9
This review discusses the role of imaging for anatomic display and detection of disorders of the wrist. Routine radiographs and MRI are emphasized, because of their current importance in wrist imaging. However, other techniques . and their indications are also addressed.
ROUTINE RADIOGRAPHY
There are numerous routine radiographic views of the wrist. We also include motion studies and fluoroscopically positioned spot views in our list of routine radiographic procedures.l,4,1(}-12 Osseous anatomy and articular relationships can be easily appreciated on radiographs obtained with the wrist in different positions. Multiple views in different positions (posteroanterior, oblique, etc.) are necessary to demonstrate anatomy, which is frequently obscured by overlying osseous structures on any single radiograph. Changes in bony relationships provide valuable signs of unsuspected ligament injury. In addition, soft-tissue anatomy can be evaluated. Fat planes provide valuable clues for detection of subtle fractures. l.1(}-13
Common radiographic views of the wrist are described to enhance the understanding of their SIgnificance for demonstrating anatomy and abnormalities.
Posteroanterior View
The posteroanterior (PA) view of the wrist is obtained with the patient sitting, with the elbow
Correspondence and reprint requests to Thomas H. Berquist, MD, Department of Diagnostic Radiology, Mayo Clinic, Jacksonville, Jacksonville, FL 32224.
108 JOURNAL OF HAND THERAPY
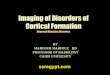
FIGURE 1. PA view of the wrist of a patient with recent trauma and pain over the scaphoid(s). Soft-tissue swelling (white open arrows) and obliteration of the navicular fat stripe (white broken line demonstrates normal location) are evident. This finding makes the diagnosis of the subtle scaphoid fracture (black arrow) much easier to accomplish. The other bony relationship are also appreciated and · the normal articular relationships easily defined. S = scaphoid, L = lunate, T = triquetrum, P = pisiform seen through the triquetrum, H = hampte, h = hook of hamate, C = capitate, tr = trapezium, tp = trapezoid, rs = radial stylpid, us = ulnar styloid, DRUJ = distal radioulnar joint (arrowhead).
flexed and the upper extremity at table level so that the forearm is in neutral rotation. The wrist is placed with the hand palm-down on a radiographic cassette. A light source on the x-ray table allows the technologist to reduce the area exposed to include the distal radius and ulna, carpal bones, and metacarpals (Fig. 1). The x-ray beam is centered over the carpal bones.l,lO Figure 1 demonstrates a PA view of the wrist. The normal bony relationships are demonstrated. However, some of the bones, specifically the trapezium and trapezoid, overlap so they cannot be completely evaluated. This emphasizes the importance of multiple views to more clearly demonstrate all osseous structures.
Careful evaluation of the bony relationships and soft-tissue anatomy can provide valuable in-

formation with regard to abnormalities and which additional imaging studies may be indicated. The articular surfaces of the carpal bones (Fig. 1) should be parallel and the joint spaces should be about 2 mm wideYO-12 Any change in a joint space or the shape of a cargal bone may indicate dislocation or subluxation.ll, Also, arcs can normally be configured along the carpal bones, The first arc is formed by the proximal articular surfaces of the scaphoid, lunate, and triquetrum. The second arc is formed by the distal articular surfaces of the same group of carpal bones. The third arc is formed by the proximal articular surfaces of the capitate and hamate.1,ll,12 The trapezium, trapezoid, and pisiform are overlapping structures on the PA view. Therefore, the arcs do not apply to these structures.
The relationship of the distal articular surfaces of the radius and ulna is also important to assess. Positive ulnar variance occurs when the ulnar articular surface is distal to the radial articular surface. Negative ulnar variance is described when the ulnar articular surface occurs proximal to the radial surface (ulna shorter). The positions of the ulnar styloid and articular surfaces vary as the forearm moves from pronation to supination.1,12
Ulnar positive variance has been associated with ulnar impaction syndrome and ulnar minus variance with Kienbock's disease. 1
Subtle fractures (Fig. 1) can be easily overlooked. Therefore, careful attention to the navicular fat stripe is important. This fat plane lies between the radial collateral ligament and the tendon sheaths of the abductor pollicis longus and extensor pollicis brevis. Displacement or absence of the fat stripe is seen in 87% of scaphoid fractures. 13
Lateral View
Positioning for the lateral view has similarities to positioning for the PA view except that the forearm and wrist are positioned so the ulna is adjacent
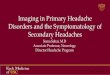
FIGURE 2. Lateral view of the wrist of a patient with pain after a fall. The pronator fat stripe (white open arrows) is displaced, which should lead one to look more carefully for a fracture or other osseous abnormality in the distal radius. Dorsal soft-tissue swelling and a subtle dorsal triquetral fracture (white arrow) can also be seen. Notice the normal linear alignment of the radius (R), lunate (L), capitate (C), and third metacarpal (3).
FIGURE 3. Oblique (A) and scaphoid (B) views of the wrist, with anatomy labeled. GM = greater multangular or trapezium.
to the cassette and the thumb and fingers are extended. The central beam is centered on the carral bones and perpendicular to the x-ray cassetteY
The bony relationships of the radius, lunate, capitate, and third metacarpal are clearly demonstrated on the lateral view (Fig. 2). The distal articular surface of the capitate articulates with the third metacarpal. The convex proximal articular surface of the capitate articulates with the lunate and the lunate articulates with the radius. When these structures are normally positioned, a straight line can be drawn through their axis. However, slight flexion or extension of the wrist can disrupt this normal alignment.1,10-12
Careful evaluation of the soft-tissue anatomy is as useful on the lateral view as it is with the PA view. The pronator fat strip (Fig. 2) can be identified along the volar or ventral aspect of the distal radius yo Subtle fractures can cause displacement or obliteration of this fat plane. This finding may be the only clue to a sl,lbtle wrist injury.l,1O
Oblique/Scaphoid Views
In addition to PA and lateral views, most institutions also obtain a scaphoid view or oblique viewsYO-12 The scaphoid view (Fig. 3) is particularly important, for the scaphoid is the most commonly fractured carEal bone and injuries to it are often subtle (Fig. 1). ,7,10
Oblique views (Fig. 3A) are obtained by rotating the wrist 45° internally or 45° externally, which improves the anatomic display and provides two additional views to deal with the problems of bony overlap encountered when only PA and lateral views are obtained.1,10
The scaphoid view (Fig. 3B) is obtained with the wrist in ulnar deviation and the hand palmdown. The thumb is extended and aligned with the radius.1,lo
April-June 1996 109

There are numerous other views of the wrist designed to demonstrate specific anatomy and reduce bony overlap. These include the pisiform view (hand and wrist rotated 30° from the lateral position), which is designed to show the pisiform in profile, and the carpal tunnel view, which is designed to show the hook of the hamate and the softtissue compartment of the carpal tunne1.1,10-12
Motion studies are performed to evaluate wrist motion, to identify bony relationships, and to detect changes that may indicate subtle ligament injury or instability.l,4,10-12 The motion series includes the PA and lateral views described above (Figs. 1 and 2) and lateral views in maximal flexion and extension· (Figs. 4A and 4B) and PA views in radial and ulnar deviation (Figs. 4C and 4D). We also routinely include a clenched-fist view to evaluate scapholunate ligament injury. This image, taken in the AP view, stresses the scapholunate ligament. Widening of the scapholunate joint, indicating ligament injury, is
110 JOURNAL OF HAND THERAPY
more obvious with this technique. Fluoroscopically positioned motion studies provide a dynamic realtime method of observing carpal motion. Fluoroscopy also allows optimal positioning for spot films.1,4,11,13
COMPUTED TOMOGRAPHY
Thin-section conventional tomograph X has been replaced by CT at most institutions1 ,15; CT provides valuable information about subtle bone and certain soft-tissue disorders, though MRI is more often used for the latter.15,16 Transaxial CT images are obtained with 1-3-mm-thick sections to allow reformatting in other image planes (i.e., sagittal or coronal) or three-dimensional reconstruction. Reformulated images are obtained electronically from the original axial image. The patient does not change position. Figure 5 demonstrates the advan-
FIGURE 4. Motion studies of the right wrist with the wrist extended (A) and flexed (B) in the lateral projection and in radial (C) and ulnar (D) deviation on the PA views. Notice the changes in the shape of the scaphoid (5) and its relationship to the lunate (L) on these normal studies.

FIGURE 5. Patient with continued pain after surgical fusion of the scaphoid to the trapezium and trapezoid (SIT arthrodesis). Thin-section CT images were reformatted into the coronal (A) and sagittal (B) planes. There is irregularity along the operative site (arrows) due to non-union. S = scaphoid, L = lunate, T = triquetrum, C = capitate, H = hamate hook, tr = trapezium, tp = trapezoid.
tages of reformatted CT images in a patient with a failed carpal fusion.
Computed tomography is also useful alone or with arthrography to evaluate subluxation of the distal radioulnar joint and injuries to ligaments and the triangular fibrocartilage. ,15,16
RADIONUCLIDE SCINTIGRAPHY
Three-phase radionuclide imaging of the wrist is useful for evaluating subtle acute and chronic disorders of the wrist? Technetium-99m coupled to phosphate compounds such as methylene disphosphate (MOP) is most often used. Three-phase techniques provide advantages over delayed (two to three hours after injection) images. The delayed image is the third phase of a three-phase study (Phase III). Phase I is a flow phase, with images obtained in rapid sequence for 1-2 minutes following intravenous injection of the isotope. This phase demonstrates changes in flow to the abnormal wrist compared with the normal side. Phase II images are obtained during the soft-tissue distribution phase,
when the isotope is in the extracellular space. Abnormal uptake of the isotope may be diffuse during the first two phases, but it is usually more focal during the delayed third phase (Fig. 6). Bone scans are obtained to detect subtle osseous injury, reflex sympathetic dystrophy, and early inflammation or infection. A negative bone scan is a good indicator that there is no bone deranpement or soft-tissueattachment abnormality.v,n,1
MAGNETIC RESONANCE IMAGING
A complete discussion of the physics and methods of image creation with MRI is beyond the scope of this review. However, because MRI is often the second test selected following routine radiographs, its advantages and disadvantages compared with other imaging techniques deserve mentionY7
Magnetic resonance imaging uses a strong magnetic field and racjjofrequency pulses to produce images. Altho\lgh there is no ionizing radiation, patients with certain metal or electrical im-
FIGURE 6. Three-phase bone scan of the wrist of a patient wit chronic wrist pain. Early blood pool images (1) and more delayed images in the PA (2) and lateral (3) positions show focal abnormal uptake at the luno-triquetral junction (arrow). This could be due to any of multiple causes (fracture, arthritis, avascular necrosis, etc.). However, it localizes the bone abnormality for further studies such as CT.
April-June 1996 111

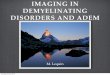
FIGURE 7. Gymnast with wrist pain and tingling in the median nerve distribution. Sagittal Tl-weighted (A) and axial T2-weighted (B) MR images demonstrate tenosynovitis, seen as high signal intensity around the tendons on the axial image (B). The median nerve (MN) is clearly visible in the carpal tunnel adjacent to the transverse ligament (t/). S = scaphoid, L = lunate, P = Pisiform, MN = median nerve, tl = transverse ligament, C = capitate, R = radius, 3 = third metacarpal, ft = flexor tendons.
FIGURE 8. Coronal T2-weighted image of the wrist, showing the high signal intensity of joint fluid and the growth plates (arrows) in an adolescent patient.
plants such as cardiac pacemakers cannot be examined. Also, patients with claustrophobia may find it difficult to tolerate the confining tubular MR gantry.3
Magnetic resonance images have superior contrast compared with CT, and ima?es can be obtained in any plane (Figs. 7 and 8). ,3,17-19 For wrist imaging, we use pulse sequences, which provide all ne,cessary information. Therefore, we may select Tlweighted and T2-weighted sequences or choose to use gadolinium. The latter is a paramagnetic compound that can be used in the way that conventional contrast medium is used for arthrography.3,9,13,18,19
Tl-weighted images show disorders or tissues with long Tl as dark. Tendons, cortical bone, ligaments, and air are also dark. Fat and bone marrow have bright signal intensity (white) on Tl-weighted MR images (Fig. 7 A). Using T2-weighted sequences, tissue abnormalities and joint fluid are
112 JOURNAL OF HAND THERAPY
bright. Thus, these sequences give an arthrogram effect (Figs. 7B and 8) on MR images. The growth plate has increased signal intensity on T2-weighted images of skeletally immature patients (Fig. 8). This finding disappears with growth-plate fusion.3,9,2o
Thus, MRI is also useful for evaluating growthplate injuries and the associated complications.3
Magnetic resonance imaging is a sensitive technique for detection of bone disorders such as avascular necrosis, subtle fractures, and neoplasms. Soft-tissue injuries (Fig. 7), nerve disorders, and other soft-tissue lesions are also easily detected due
FIGURE 9. Illustration of the compartments of the wrist with typical injection sites marked (+). 1 = distal radioulnar joint, 2 = radiocarpal joint, 3 = intercarpal or midcarpal joint, Arrows show the flow of contrast away from the injection sites in the radiocarpal (2) and intercarpal (3) joints. TFC = triangular fibrocartilage complex, SL = scapholunate ligament, LT = lunotriquetral ligament.

FIGURE 10. A, normal radiocarpal arthrogram. The contrast material does not enter the other joints (see Fig. 9). + = injection site; arrows demonstrate contrast flow. VR = volar recess, PR = prestyloid recess. B, Contrast injection into the distal radioulnar joint (+) with flow (arrow) into the radiocarpal joint (RC) due to a tear in the triangular fibrocartilage.
to the superior soft-tissue contrast between normal and abnormal tissue.3
,18
Despite the many advantages of MRI, it is an expensive technique. Alternative techniques described above and arthroteno!?raphy still play valuable roles in wrist imaging. 1, ,21
ARTHROGRAPHY-TENOGRAPHY
Injection of the compartments of the wrist or tendon sheaths about the wrist can provide valuable information regarding anatomy and soft-tissue integrity. In addition, combined with anesthetic injection, the exact site of pain can be localized and confirmed.8,22
Wrist arthrograms are useful to define the articular cartilage and synovial lining of the wrist. The integrity of the triangular fibrocartilage complex, ligaments, and capsule can also be as-
sessed.1,5,6,1l,I2 Although some advocate injection of
all three compartments (Fig. 9)/ we prefer a systematic approach, starting at the symptomatic site (Fig. 10) and proceeding with additional injections as necessary. 1,
Figure 10 demonstrates a normal radiocarpal arthrographic injection (A) and a tear of the triangular fibrocartilage (B) with communication between the radiocarpal and distal radioulnar joints.
REFERENCES 1. Berquist TH: Imaging of Orthopedic Trauma. New York,
Raven Press, 1992. 2. Dalinka MK: MR imaging of the wrist. AJR 164:1-9, 1995. 3. Berquist TH: MRI of the Musculoskeletal System, 3rd Ed.
New York, Lippincott-Raven, 1995. 4. Bond JR, Berquist TH: Radiographic evaluation of hand and
wrist motion. Hand Clin 7:113-123, 1991. 5. Levinsohn ME, Palmer AK, Cohen AB, et al: Wrist arthrog
raphy: the value of the three compartment injection technique. Skel Radiol 16:539-544, 1987.
6. Manaster BJ: The clinical efficacy of triple-injection wrist arthrography. Radiology 178:267-270, 1991.
7. Nielsen DT, Heberdoe J, Thommesen P: Bone scintigraphy in evaluation of fracture of the carpal scaphoid bone. Acta Orthop Scand 54:303-306, 1983.
8. Resnick D, Dalinka MK: Arthrography and tenography of the wrist. In: Dalinka MK (ed.) Arthrography. New York, Springer-Verlag, 1980.
9. Zlatkin MB, Chris Pc, Osterman AL, et al: Chronic wrist pain: evaluation with high resolution MR imaging. Radiology 173:723-279, 1989.
10. Bemau A, Berquist TH: Orthopedic Positioning in Diagnostic Radiology. Baltimore, Urban and Schwarzenberg, 1983.
11. Gilula LA: Carpal injuries: analytical approach and case exercises. AJR 133:513-517, 1979.
12. Gilula LA, Destouet JM, Weeks PM, et al: Roentgen diagnosis of the painful wrist. Clin Orthop 187:51-64, 1984.
13. Terry DW, Ramin JE: The navicular fat strip. A useful roentgen feature for evaluating wrist trauma. AJR 124:25, 1975.
14. Cone RO, Szabo R, Resnick D, et al: Computed tomography of the normal soft tissues of the wrist. Invest Radiol 18: 541-545,1983.
15. Quinn SJ, Belsole RS, Green TL, et al: Post-arthrographic computed tomography of the wrist: evaluation of the triangular fibro-cartilage complex. Skel Radiol 17:565-569, 1989.
16. Magid D, Thompson JS, Fishman EK: Computed tomography of the hand and wrist. Hand Clin 7:219-234, 1991.
17. Berquist TH: The elbow/and wrist. Top Magn Res Imaging 1:15-27, 1989.
18. Rominger MB, Bemreuter WK, Kenny PJ: MR imaging of the anatomy and tears of wrist ligaments. Radio-Graphics 13:1233-1246, 1993.
19. Shih C, Chang C-Y, Penn I-W, et al: Chronically stressed wrists in adolescent gymnasts: MR imaging appearance. Radiology 195:855-859, 1995.
20. Timins ME, Jahnke JP, Krah SF, et al: MR imaging of the major carpal stabilizing ligaments: normal anatomy and clinical examples. RadioGraphics 15:575-587, 1995.
21. Gundry CR, Kurismoglis-Brahme S, Schwaighofer B, et al: Is MR better than arthrography for evaluating the ligaments of the wrist? In vitro study. AJR 154:337-341, 1990.
22. Berquist TH: Diagnostic and therapeutic injections as an aid to musculoskeletal diagnosis. Semin Intervent Radiol 10: 326-343, 1993.
April-June 1996 113