Embed Size (px)
Citation preview
J Clin Pathol 1987;40:412-417
Xanthogranulomatous cholecystitis: clinico-pathological study of 13 cases
K M ROBERTS, M A PARSONS
From the Department of Pathology, University ofSheffield Medical School, Sheffield
SUMMARY In a retrospective three year study 13 cases of xanthogranulomatous cholecystitis(XGC) (seven female, six male) were found in 724 gallbladders (1 8%), an estimated incidence of 1 7cases per 1O00000 population per annum. Symptoms often began with an episode of acute chole-cystitis and persisted for up to five years. There was extension of xanthogranulomatous tissue intoadjacent organs in nine cases. Three patients had fistulae from the gall bladder, one to skin, and twoto the duodenum; this is the first report of this complication in XGC. In two patients XGCsufficiently resembled carcinoma for the surgeon to request intraoperative frozen section diagnosis.There was a high rate of postoperative infective complication, with one subphrenic abscess andthree wound infections (one fatal), two in patients with fistulae.
Xanthogranulomatous cholecystitis (XGC) is anuncommon inflammatory disease of the gall bladdercharacterised by a focal or diffuse destructiveinflammatory process, with varying proportions offibrous tissue, acute and chronic inflammatory cells,and lipid laden macrophages. Macroscopically, areasof XGC appear as yellow masses within the wall ofthe gall bladder.Xanthogranulomatous cholecystitis was first
described in 1970 by Christensen and Ishak' as"fibroxanthogranulomatous inflammation." Sincethen over 60 cases have been described under a varietyof synonyms, including "ceroid or ceroid-likehistiocytic granuloma of gallbladder,"2 3 and "biliarygranulomatous cholecystitis."4 The pathogenesis ofXGC is uncertain, but reported opinion favours aninflammatory response to extravasated bile, possiblyfrom ruptured Rokitansky-Aschoff sinuses.3 The trueincidence of this apparently rare condition is difficultto establish; although Takahashi et al3 reported theincidence in Japan to be 1-2% of all surgically excisedgall bladders, there has been no report of its incidencein a Western country.
In the studies where clinical information was avail-able XGC was described as an uncomplicated mass inthe wall of the gall bladder. Christensen and Ishak,'however, reported that in two of their 40 cases "the
Accepted for publication 21 October 1986
question of a mesenchymal sarcoma was raised by thecontributing pathologist."
In this paper we present the detailed clinical andpathological features and complications of the 13cases of XGC presenting in a teaching hospital of 730beds from 1983-85.
Material and methods
The files of the department of histopathology at theRoyal Hallamshire Hospital, Sheffield, for the threeyears 1983-85, were examined retrospectively forcases of inflammatory disease of the gall bladder. Atotal of 724 surgically excised gall bladders were sub-mitted for pathological examination during thisperiod; among these, 13 cases of xantho-granulomatous cholecystitis were identified. Theclinical records of these patients were reviewed forsymptoms, signs, laboratory data, operative findings,and details of postoperative progress. Organ imagingdata were obtained from the reports in the medicalrecords. The macroscopic appearance of the gallbladder was compiled from the surgeons' notes andthe detailed description in the pathologist's report.
After cholecystectomy the gall bladders wereopened longitudinally and fixed in 10% neutral phos-phate buffered formol saline. Sections were processedto paraffin wax, cut at 4pum, and stained withhaematoxylin and eosin, periodic acid Schiff, Gram,Ziehl-Neelsen, Perl's Prussian blue and methenaminesilver methods.
412
on 20 May 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.40.4.412 on 1 April 1987. D
ownloaded from
Xanthogranulomatous cholecystitisTissue for intraoperative diagnosis was rapidly fro-
zen, and cryostat sections cut at 8pm and stainedwith haematoxylin and eosin, and oil red 0 for fat.
Results
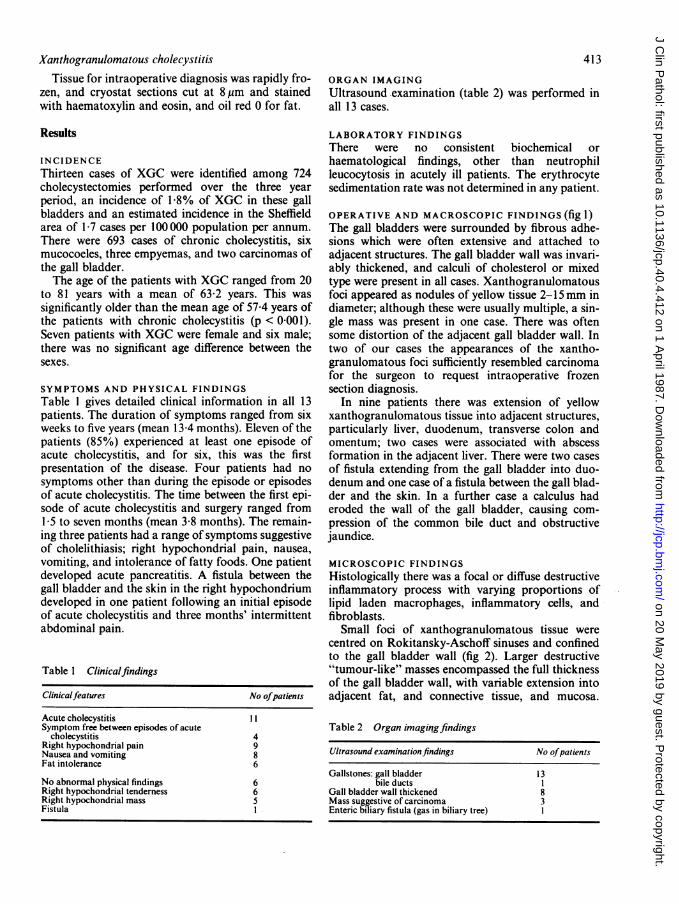
INCIDENCEThirteen cases of XGC were identified among 724cholecystectomies performed over the three yearperiod, an incidence of 1 8% of XGC in these gallbladders and an estimated incidence in the Sheffieldarea of 1-7 cases per 100 000 population per annum.There were 693 cases of chronic cholecystitis, sixmucocoeles, three empyemas, and two carcinomas ofthe gall bladder.The age of the patients with XGC ranged from 20
to 81 years with a mean of 63-2 years. This wassignificantly older than the mean age of 57A4 years ofthe patients with chronic cholecystitis (p < 0-001).Seven patients with XGC were female and six male;there was no significant age difference between thesexes.
SYMPTOMS AND PHYSICAL FINDINGSTable 1 gives detailed clinical information in all 13patients. The duration of symptoms ranged from sixweeks to five years (mean 13-4 months). Eleven of thepatients (85%) experienced at least one episode ofacute cholecystitis, and for six, this was the firstpresentation of the disease. Four patients had nosymptoms other than during the episode or episodesof acute cholecystitis. The time between the first epi-sode of acute cholecystitis and surgery ranged from1-5 to seven months (mean 3-8 months). The remain-ing three patients had a range of symptoms suggestiveof cholelithiasis; right hypochondrial pain, nausea,vomiting, and intolerance of fatty foods. One patientdeveloped acute pancreatitis. A fistula between thegall bladder and the skin in the right hypochondriumdeveloped in one patient following an initial episodeof acute cholecystitis and three months' intermittentabdominal pain.
Table 1 Clinicalfindings
Clinicalfeatures No ofpatients
Acute cholecystitis 11Symptom free between episodes of acute
cholecystitis 4Right hypochondrial pain 9Nausea and vomiting 8Fat intolerance 6
No abnormal physical findings 6Right hypochondrial tenderness 6Right hypochondrial mass 5Fistula I
413ORGAN IMAGINGUltrasound examination (table 2) was performed inall 13 cases.
LABORATORY FINDINGSThere were no consistent biochemical orhaematological findings, other than neutrophilleucocytosis in acutely ill patients. The erythrocytesedimentation rate was not determined in any patient.
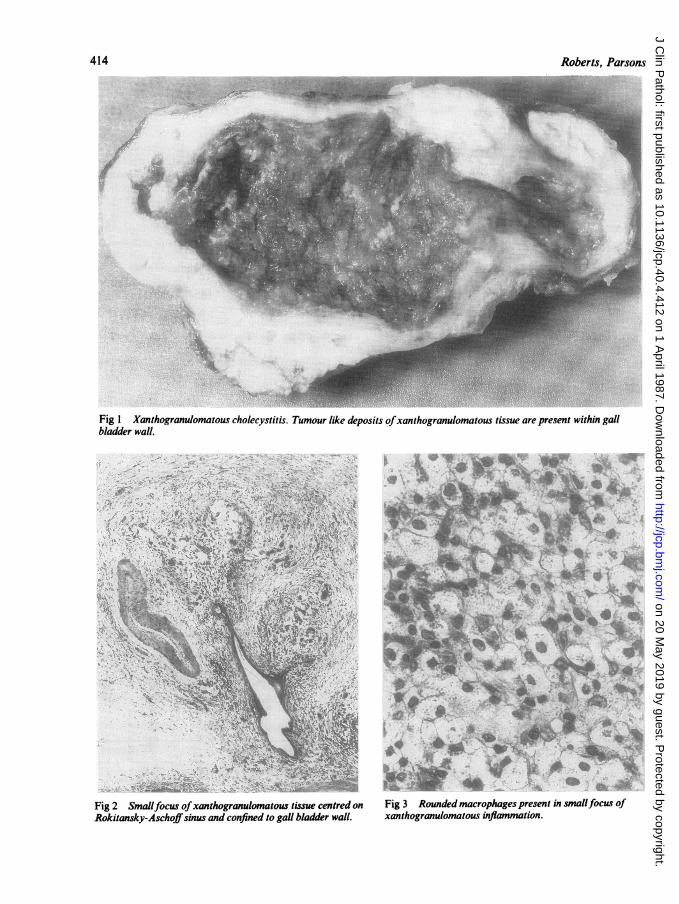
OPERATIVE AND MACROSCOPIC FINDINGS (fig 1)The gall bladders were surrounded by fibrous adhe-sions which were often extensive and attached toadjacent structures. The gall bladder wall was invari-ably thickened, and calculi of cholesterol or mixedtype were present in all cases. Xanthogranulomatousfoci appeared as nodules of yellow tissue 2-15mm indiameter; although these were usually multiple, a sin-gle mass was present in one case. There was oftensome distortion of the adjacent gall bladder wall. Intwo of our cases the appearances of the xantho-granulomatous foci sufficiently resembled carcinomafor the surgeon to request intraoperative frozensection diagnosis.
In nine patients there was extension of yellowxanthogranulomatous tissue into adjacent structures,particularly liver, duodenum, transverse colon andomentum; two cases were associated with abscessformation in the adjacent liver. There were two casesof fistula extending from the gall bladder into duo-denum and one case of a fistula between the gall blad-der and the skin. In a further case a calculus haderoded the wall of the gall bladder, causing com-pression of the common bile duct and obstructivejaundice.
MICROSCOPIC FINDINGSHistologically there was a focal or diffuse destructiveinflammatory process with varying proportions oflipid laden macrophages, inflammatory cells, andfibroblasts.
Small foci of xanthogranulomatous tissue werecentred on Rokitansky-Aschoff sinuses and confinedto the gall bladder wall (fig 2). Larger destructive"tumour-like" masses encompassed the full thicknessof the gall bladder wall, with variable extension intoadjacent fat, and connective tissue, and mucosa.
Table 2 Organ imagingfindings
Ultrasound examinationfindings No ofpatients
Gallstones: gall bladder 13bile ducts I
Gall bladder wall thickened 8Mass suggestive of carcinoma 3Enteric biliary fistula (gas in biliary tree) I
on 20 May 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.40.4.412 on 1 April 1987. D
ownloaded from
414 RbrsPasn
* ,. .. .... s_E;. ^~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.......~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.. t..;........
Fig I Xanthogranulomatous cholecystitis. Tumour like deposits ofxanthogranulomatous tissue are present within gallbladder wall.
Fig 2 Smallfocus ofxanthogranulomatous tissue centred on Fig 3 Rounded macrophages present in smallfocus ofRokitansky-Aschoffsinus and confined to gall bladder wall. xanthogranulomatous inflammation.
V, Z
on 20 May 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.40.4.412 on 1 April 1987. D
ownloaded from
Xanthogranulomatous cholecystitis
Mucosal ulceration was present in six cases. Histolog-ical evidence of extension of XGC into the liver wasseen in two cases.
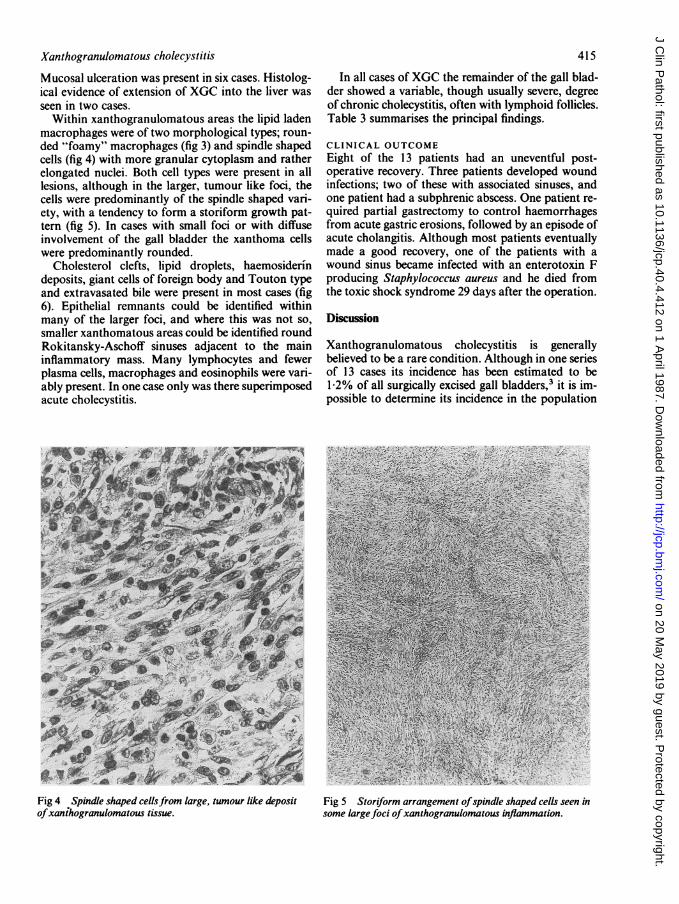
Within xanthogranulomatous areas the lipid ladenmacrophages were of two morphological types; roun-ded "foamy" macrophages (fig 3) and spindle shapedcells (fig 4) with more granular cytoplasm and ratherelongated nuclei. Both cell types were present in alllesions, although in the larger, tumour like foci, thecells were predominantly of the spindle shaped vari-ety, with a tendency to form a storiform growth pat-tern (fig 5). In cases with small foci or with diffuseinvolvement of the gall bladder the xanthoma cellswere predominantly rounded.
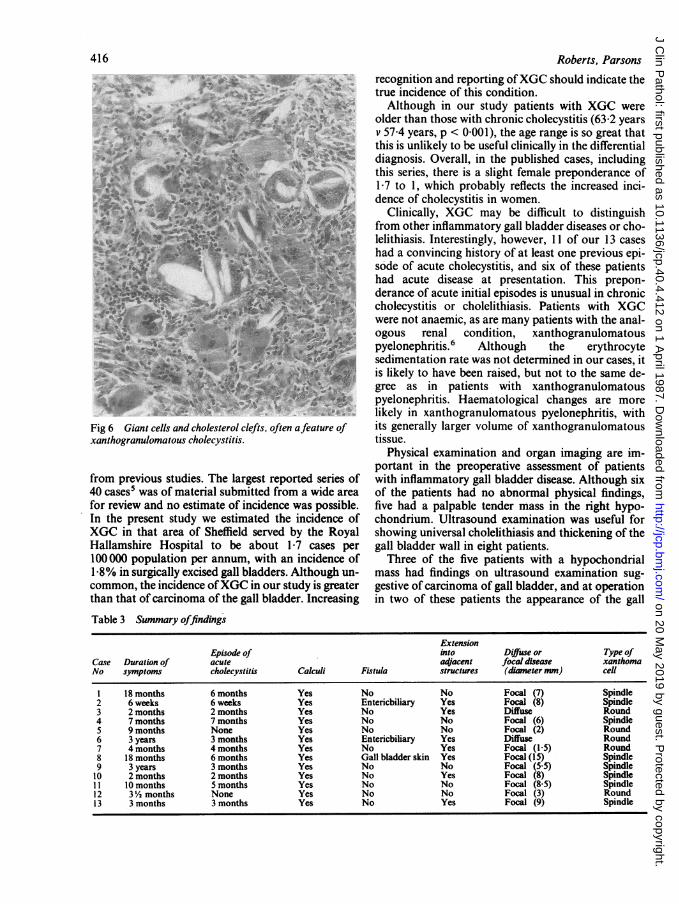
Cholesterol clefts, lipid droplets, haemosiderindeposits, giant cells of foreign body and Touton typeand extravasated bile were present in most cases (fig6). Epithelial remnants could be identified withinmany of the larger foci, and where this was not so,smaller xanthomatous areas could be identified roundRokitansky-Aschoff sinuses adjacent to the maininflammatory mass. Many lymphocytes and fewerplasma cells, macrophages and eosinophils were vari-ably present. In one case only was there superimposedacute cholecystitis.
415
In all cases of XGC the remainder of the gall blad-der showed a variable, though usually severe, degreeof chronic cholecystitis, often with lymphoid follicles.Table 3 summarises the principal findings.
CLINICAL OUTCOMEEight of the 13 patients had an uneventful post-operative recovery. Three patients developed woundinfections; two of these with associated sinuses, andone patient had a subphrenic abscess. One patient re-quired partial gastrectomy to control haemorrhagesfrom acute gastric erosions, followed by an episode ofacute cholangitis. Although most patients eventuallymade a good recovery, one of the patients with awound sinus became infected with an enterotoxin Fproducing Staphylococcus aureus and he died fromthe toxic shock syndrome 29 days after the operation.
Discussion
Xanthogranulomatous cholecystitis is generallybelieved to be a rare condition. Although in one seriesof 13 cases its incidence has been estimated to be1 2% of all surgically excised gall bladders,3 it is im-possible to determine its incidence in the population
Fig 5 Storiform arrangement ofspindle shaped cells seen insome largefoci ofxanthogranulomatous inflammation.
Fig 4 Spindle shaped cellsefom large, tumour like depositofxanthogranulomatous tissue.
on 20 May 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.40.4.412 on 1 April 1987. D
ownloaded from
416
Fig 6 Giant cells and cholesterol clefts, often afeature ofxanthogranulomatous cholecystitis.
from previous studies. The largest reported series of40 cases' was of material submitted from a wide areafor review and no estimate of incidence was possible.In the present study we estimated the incidence ofXGC in that area of Sheffield served by the RoyalHallamshire Hospital to be about 1-7 cases per100000 population per annum, with an incidence of1 8% in surgically excised gall bladders. Although un-common, the incidence ofXGC in our study is greaterthan that of carcinoma of the gall bladder. Increasing
Roberts, Parsons
recognition and reporting ofXGC should indicate thetrue incidence of this condition.Although in our study patients with XGC were
older than those with chronic cholecystitis (63.2 yearsv 57T4 years, p < 0-001), the age range is so great thatthis is unlikely to be useful clinically in the differentialdiagnosis. Overall, in the published cases, includingthis series, there is a slight female preponderance of1-7 to 1, which probably reflects the increased inci-dence of cholecystitis in women.
Clinically, XGC may be difficult to distinguishfrom other inflammatory gall bladder diseases or cho-lelithiasis. Interestingly, however, 11 of our 13 caseshad a convincing history of at least one previous epi-sode of acute cholecystitis, and six of these patientshad acute disease at presentation. This prepon-derance of acute initial episodes is unusual in chroniccholecystitis or cholelithiasis. Patients with XGCwere not anaemic, as are many patients with the anal-ogous renal condition, xanthogranulomatouspyelonephritis.6 Although the erythrocytesedimentation rate was not determined in our cases, itis likely to have been raised, but not to the same de-gree as in patients with xanthogranulomatouspyelonephritis. Haematological changes are morelikely in xanthogranulomatous pyelonephritis, withits generally larger volume of xanthogranulomatoustissue.
Physical examination and organ imaging are im-portant in the preoperative assessment of patientswith inflammatory gall bladder disease. Although sixof the patients had no abnormal physical findings,five had a palpable tender mass in the right hypo-chondrium. Ultrasound examination was useful forshowing universal cholelithiasis and thickening of thegall bladder wall in eight patients.
Three of the five patients with a hypochondrialmass had findings on ultrasound examination sug-gestive of carcinoma of gall bladder, and at operationin two of these patients the appearance of the gall
Table 3 Summary offindings
ExtensionEpisode of into Diffuse or Type of
Case Duration of acute adjacent focal disease xanthomaNo symptoms cholecystitis Calculi Fistula structures (dimeter mm) cell
1 18 months 6 months Yes No No Focal (7) Spindle2 6 weeks 6 weeks Yes Entericbiliary Yes Focal (8) Spindle3 2 months 2 months Yes No Yes Diffuse Round4 7 months 7 months Yes No No Focal (6) Spindle5 9 months None Yes No No Focal (2) Round6 3 years 3 months Yes Entericbiliary Yes Diffuse Round7 4 months 4 months Yes No Yes Focal (1 5) Round8 18 months 6 months Yes Gall bladder skin Yes Focal (15) Spindle9 3 years 3 months Yes No No Focal (5-5) Spindle10 2 months 2 months Yes No Yes Focal (8) Spindle11 10 months 5 months Yes No No Focal (8.5) Spindle12 3V/2 months None Yes No No Focal (3) Round13 3 months 3 months Yes No Yes Focal (9) Spindle
on 20 May 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.40.4.412 on 1 April 1987. D
ownloaded from

Xanthogranulomatous cholecystitis 417bladder sufficiently resembled carcinoma for thesurgeon to request rapid frozen section diagnosis. Theability of XGC to resemble carcinoma clinically andmacrospically is further complicated by its ability tomimic tumours histologically. Confusion with a neo-plasm is perhaps most likely where spindle shapedxanthoma cells predominate with a storiform growthpattern. XGC lacks true malignant features, such aspleomorphism, cellular atypia, and increased or bi-zarre mitotic figures. An awareness of the conditionand good liaison with the clinician is required so thatinterpretation of histological findings may be made inthe light of clinical, organ imaging, and macroscopicfindings; this is of particular importance in rapid fro-zen section diagnosis, where a small sample may ex-acerbate the problem.An important complication of XGC, which has not
been reported previously, is the development offistulae, present in three of our cases and otherwiserare in cholecystitis. Thus XGC seems to share thepotential for fistula formation with xantho-granulomatous pyelonephritis, where fistula for-mation is well recognised.6 9The pathogenesis of XGC is unclear, although the
role of cholesterol and bile is thought to be im-portant.2 - s10 Bile degradation within histiocytes as acause of the xanthoma cells has been proposed.2Takahashi et al3 and Goodman and Ishaks have sug-gested that the important event is the extravasation ofbile into the gall bladder wall, either from rupturedRokitansky-Aschoff sinuses or focal mucosal ulcer-ation. Fligel and Lewin'0 believe that in addition tothe presence of bile, a more important feature may bea long standing or recurrent inflammatory process.They also draw the analogy to xanthogranulomatouspyelonephritis, where obstruction with stasis is im-portant, and suggested the possible role of gallstonesin causing obstruction in XGC. In the largest pub-lished series of cases ofXGC gallstones were presentin only three quarters of the cases; in our series theywere present in all cases. In most cases foci of XGCseem to be centred on Rokitansky-Aschoff sinuses.We believe that the pathogenesis ofXGC is similar
to that proposed by Parsons et al for xantho-granulomatous pyelonephritis.6 The essential ingredi-ents are inflammation associated with infection,obstruction of the biliary outflow from the gall blad-der due to calculi, and a source of lipid-in this casebiliary cholesterol. A gall bladder with partial or totalobstruction of bile outflow by calculi becomes acutelyinflamed, most probably as a result of infection. Thisresults in rupture of Rokitansky-Aschoff sinuses ormucosal ulceration with subsequent extravasation ofbile into the gall bladder wall. Histiocytes accumulatein an attempt to phagocytose the biliary cholesteroland xanthoma cells form. As the lesion increases insize some of the fat within the xanthoma cells may bederived from adipose tissue on the serosal surface ofthe gall bladder or from adherent omentum. With
time, organisation of the inflammatory mass occursand eventually the xanthoma cells elongate into aspindle shaped configuration and fibrosis increases. Itis at this stage that confusion with a neoplasm is mostlikely. Failure of drainage of the inflammatoryinfiltrate in the acute phase may lead to extension ofthe xanthogranulomatous inflammation beyond thegall bladder with the formation of abscesses, sinuses,or fistulae draining to bowel, skin, or elsewhere.We support the view of Goodman and Ishak5 that
the best name for this condition is xantho-granulomatous cholecystitis as this emphasises itsinflammatory nature and its conceptual similarity tothe renal condition, xanthogranulomatouspyelonephritis. We believe XGC deserves recognitionas a distinct clinicopathological entity, not only be-cause of its possible confusion with malignancy butalso because of its associated complications.
Surgery is likely to be complicated by the presenceof dense fibrous adhesions, abscesses, and adherenceof the gall bladder to adjacent structures. Post-operative wound infection or sinuses seem dis-proportionately common. As the condition has thepotential for fistula formation, percutaneous needlebiopsy is probably contraindicated, and it may benecessary to confirm the benign nature of the lesionby intraoperative frozen section diagnosis.
We thank Mr M Eaton for photographic assistanceand Mrs M Hogg and Mrs B Barrass for typing themanuscript.
References
1 Christensen AH, Ishak KG. Benign tumours and pseudotumoursof the gall bladder. Archives of Pathology 1970;90:423-32.
2 Amazon K, Rywlin AM. Ceroid granulomas of the gall bladder.Am J Clin Pathol 1980;73:123-7.
3 Takahashi K, Oka K, Hakozaki H, Kojima M. Ceroid-likehistiocytic granuloma of gall bladder. Acta Pathol Jpn1976;26:25-46.
4 Mehrotra ML, Bhatnagar BNS. Biliary granulomatous chole-cystitis. J Indian Med Assoc 1982;79:144-5.
5 Goodman ZO, Ishak KG. Xanthogranulomatous cholecystitis.Am J Surg Pathol 1981;5:653-9.
6 Parsons MA, Harris SC, Longstaff AJ, Grainger RG. Xan-thogranulomatous pyelonephritis. A pathological, clinical andaetiological analysis of 87 cases. Diagn Histopathol1983;6:203-19.
7 Parsons MA, Harris SC, Grainger RG, Ross B, Smith JAR, Will-iams JL. Fistula and sinus formation in xanthogranulomatouscholecystitis. BJ Urol 1986;58:488-93.
8 Malek RS, Elder JS. Xanthogranulomatous pyelonephritis: acritical analysis of 26 cases and of the literature. J Urol1978;1 19:589-93.
9 Tolia BM, Iloreta A, Freed SZ, Fruchtman B, Bennet B,Newman HR. Xanthogranulomatous pyelonephritis: detailedanalysis of 29 cases and a brief discussion of atypicalpresentations. J Urol 1980;126:437-42.
10 Fligel S, Lewin KJ. Xanthogranulomatous cholecystitis. ArchPathol Lab Med 1982;106:302-4.
Requests for reprints to: Dr KM Roberts, Department ofPathology, University of Sheffield Medical School, BeechHill Road, Sheffield S1O 2RX, England.
on 20 May 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.40.4.412 on 1 April 1987. D
ownloaded from