Embed Size (px)
Citation preview
Your guide to providing high-quality health care to your employees
Your Kaiser Permanente AdministrAtion HAndbook
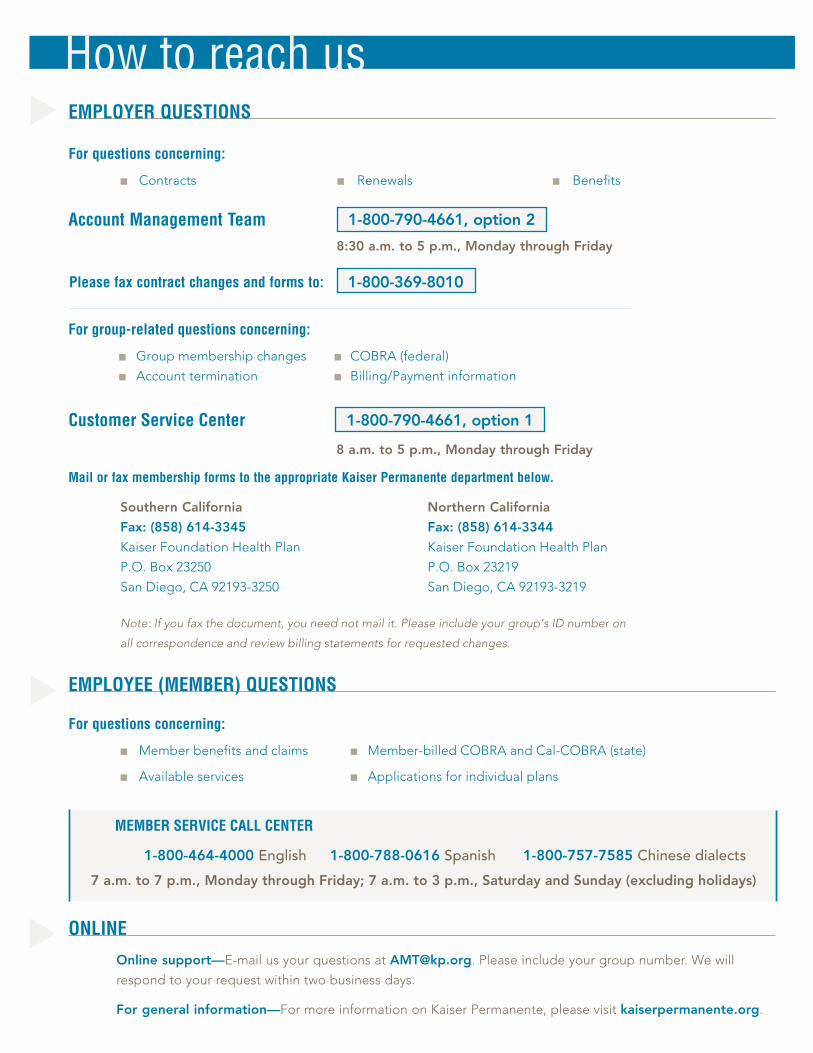
How to reach usEmPLoYEr QUEstions
For questions concerning:
■ Contracts ■ Renewals ■ Benefits
mail or fax membership forms to the appropriate kaiser Permanente department below.
SouthernCalifornia NorthernCalifornia
Fax:(858)614-3345 Fax:(858)614-3344
KaiserFoundationHealthPlan KaiserFoundationHealthPlan
P.O.Box23250 P.O.Box23219
SanDiego,CA92193-3250 SanDiego,CA92193-3219
Note:Ifyoufaxthedocument,youneednotmailit.Pleaseincludeyourgroup’sIDnumberon
allcorrespondenceandreviewbillingstatementsforrequestedchanges.
EmPLoYEE (mEmbEr) QUEstions
For questions concerning:
■ Memberbenefitsandclaims ■ Member-billedCOBRAandCal-COBRA(state)
■ Availableservices ■ Applicationsforindividualplans
mEmbEr sErvicE cALL cEntEr
1-800-464-4000English1-800-788-0616Spanish1-800-757-7585Chinese dialects
7a.m.to7p.m.,MondaythroughFriday;7a.m.to3p.m.,SaturdayandSunday(excludingholidays)
onLinE
Onlinesupport—E-mailusyourquestionsatAMT@kp.org.Pleaseincludeyourgroupnumber.Wewill
respondtoyourrequestwithintwobusinessdays.
Forgeneralinformation—FormoreinformationonKaiserPermanente,pleasevisitkaiserpermanente.org.
For group-related questions concerning:
■ Groupmembershipchanges ■ COBRA(federal)
■ Accounttermination ■ Billing/Paymentinformation
▼▼
▼
Please fax contract changes and forms to: 1-800-369-8010
1-800-790-4661,option1
8a.m.to5p.m.,MondaythroughFriday
customer service center
8:30a.m.to5p.m.,MondaythroughFriday
1-800-790-4661,option2Account management team


Everything you need to complete your group enrollment and administer your group health plan is right here.
Howtoreachus..................................................................... insidefrontcover
WelcometoKaiserPermanente.....................................................................3
sEction 1—Completingyourinitialgroupenrollment
Enrollmentchecklist..........................................................................................4
Declination of Coverage Form........................................................................7
Proprietor/Partner/Corporate Officer Form.................................................9
sEction 2—Administeringyourgrouphealthplan
Frequentlyaskedquestionsaboutadministeringgrouphealthplans...12
OnlineAccountServices.................................................................................18
Online Account Services User ID Request Form........................................23
COBRAandCal-COBRA.................................................................................25
Avoidingprocessingdelays...........................................................................26
Forms.................................................................................................................28
Account Change Form........................................................................29
Student Certification...........................................................................31
Termination Report.............................................................................33
Temporarypaymentcoupons...........................................................35
Temporarypaymentenvelopes............................. backcoverpocket
Tableof contEnts

2
3
Welcometo KaisEr PErmanEntE
ThankyouforselectingKaiserPermanenteforyourcompany’shealthcarecoverage.
Welookforwardtoprovidingyouandyouremployeeswithhigh-qualityhealthcare.
Thisbookletcontainsessentialinformationtohelpyoucompleteyournewgroupenrollment
andadministeryourKaiserPermanentehealthcareplan.We’veincludedeverythingyou
need—importantphonenumbers,answerstofrequentlyaskedquestions,andforms.In
thebackofthehandbook,wehavealsoincludedyourtemporarypaymentcouponsand
envelopes.Pleaseusethesecouponsandenvelopestomakemonthlypremiumpayments
untilyoureceiveyourfirstbill.
BesuretoalsotakeadvantageofOnlineAccountServices—aneasyonlinetooldesigned
tohelpyoumanageyourgroup’scoverage.Pleasetakeafewmomentstoreviewinformation
onOnlineAccountServicesonpage18.Ifyouhaveanyquestions,pleasecontactus.
Remember,we’reheretohelp.
■ Forquestionsaboutcompletingyourinitialgroupenrollment,callyour
KaiserPermanentesalesrepresentativeat1-800-730-4661forassistance.
■ Forquestionsaboutadministeringyourgrouphealthplan,refertothe
“Howtoreachus”guideinsidethefrontcoverforcontactinformation.
ThankyouforchoosingKaiserPermanente.Welookforwardtoalongandhealthy
relationshipwithyou.
4
comPlEtingYour initial grouP EnrollmEnt
¸ Enrollment cHEcKlist
Follow these six simple steps to complete your group’s enrollment
Tohelpusprocessyourenrollmentaccurately,pleasecompleteandreturnalltheitemslistedbelow.
Enrollingissimpleandfast,andcanbecompletedbyfaxformostgroups!
1.New Group Application—Ifyouhavenotalreadydoneso,completeandfaxthisformtostartyour
group’sapplicationprocessrightaway.Membershipislimitedtothoseindividualswholiveorworkwithin
theserviceareaZIPcodes.TorequestaNewGroupApplication,pleasecallyoursalesrepresentative.
2.Employee Enrollment Form—Makesureeachemployeecompletes,signs,anddates
hisorherenrollmentapplication.Pleasemakesureemployeeskeepphotocopiesoftheirenrollment
applicationstobeusedalongwiththeirTemporaryMembershipIDs.
3.Declination of Coverage—Alleligibleemployeeswhovoluntarilydeclinetoenrollinthehealthplan
duringtheenrollmentperiodmustcompleteandsigntheDeclinationofCoverage.
4. dE 6 (quarterly wage report)—Includeacopyofyourmostrecentquarterlywagereport.Ifyou
donotfileaDE6,manyotherdocumentsmaysatisfytherequirement(e.g.,afictitiousbusinessname
statement,currentbusinesslicense,legalpartnershipagreement,articlesofincorporation,etc.).Please
consultyoursalesrepresentativetodiscussyouroptions.
5.copy of initial premium—Pleasemakeyourfirstmonth’spremiumcheckpayabletoKaiserPermanente.
Photocopythecompletedpremiumcheckandincludethecopywiththeenrollmentforms.Important:Your
companynamemustbeprintedonthecheck.Also,writeyourpurchasernumberandyourgroup’seffective
dateonyourcheck.Faxtheitemslistedaboveto1-800-369-8010.

5
Ifyouareunabletofaxthedocuments,mailthemtothefollowingappropriateaddress.
(Sendingmaterialsviaovernightdeliverywillexpeditetheenrollmentofyourgroup.)
U.s. mail address overnight delivery address Kaiser Permanente Kaiser Permanente Small Business Unit Small Business Unit P.O. Box 7104 100 S. Los Robles, 4th Floor Pasadena, CA 91109 Pasadena, CA 91109
6.Firstmonth’spremiumcheck—Onceyourgroup’senrollmentisconfirmed,mailtheoriginal
premiumchecktotheappropriateaddresslistedbelow.
northern california groups KaiserFoundationHealthPlan,Inc.
FileNumber73030
P.O.Box60000
SanFrancisco,CA94160-3030
southern california groups KaiserFoundationHealthPlan,Inc.
FileNumber5915
LosAngeles,CA90074-5915
Forassistance,pleasecallyourKaiserPermanentesalesrepresentativeat1-800-730-4661.

6
7
IhavebeenofferedgrouphealthcoveragethroughKaiserFoundationHealthPlan,Inc.(HealthPlan),bymyemployer,
______________________________________________________________________.Groupnumber_______________________.
IvoluntarilychoosenottoenrollintheHealthPlanthroughmyemployeratthistime.Iunderstandmynextopportunity
toenrollmyselformyeligibledependentswillbeduringtheopenenrollmentperiod.TheHealthPlan’sEvidenceof
Coveragealsoinformsthegroupofmyenrollmentrightsdueto:(1)specialenrollmentduetonewdependents,and
(2)specialenrollmentduetolossofothercoverage.
ReasonPrintemployee‘sname Employee’ssignature SocialSecuritynumber Date (mustcheckonebox) ❑Iamcoveredbyother
groupinsurance.
❑Ideclineemployer-sponsoredhealthcoverage.
❑Iamcoveredbyothergroupinsurance.
❑Ideclineemployer-sponsoredhealthcoverage.
❑Iamcoveredbyothergroupinsurance.
❑Ideclineemployer-sponsoredhealthcoverage.
❑Iamcoveredbyothergroupinsurance.
❑Ideclineemployer-sponsoredhealthcoverage.
❑Iamcoveredbyothergroupinsurance.
❑Ideclineemployer-sponsoredhealthcoverage.
❑Iamcoveredbyothergroupinsurance.
❑Ideclineemployer-sponsoredhealthcoverage.
❑Iamcoveredbyothergroupinsurance.
❑Ideclineemployer-sponsoredhealthcoverage.
❑Iamcoveredbyothergroupinsurance.
❑Ideclineemployer-sponsoredhealthcoverage.
❑Iamcoveredbyothergroupinsurance.
❑Ideclineemployer-sponsoredhealthcoverage.
❑Iamcoveredbyothergroupinsurance.
❑Ideclineemployer-sponsoredhealthcoverage.
dEcLinAtion oF covErAgE
––
––
––
––
––
––
––
––
––
9
(Pleasefilloutthisformforanyproprietor,partner,orcorporateofficernotlistedontheDE6.)Toestablishtherelationshipbetweenproprietors,partners,and/orcorporateofficerstothebelow-referencedcompany,pleasecompleteandreturnthisform.
Iattestthat,althoughmynamedoesnotappearonthe DE 6wagereportofthebelow-namedcompany,thefollowingconditionsaretrue:
1. Iamasoleproprietor,partnerofapartnership,orcorporateofficer.
2. Iactivelyworkatthebelow-namedcompany.
3. Idrawwages,dividends,orotherdistributionsfromthebelow-namedcompanyonatleastamonthlybasisandamnoteligibleforgrouphealthcoveragefromanyotheremployment.
4. Iworkonapermanent,full-timebasisforthebelow-namedcompanyforatleast20hoursperweek.
5. Isatisfiedthedesignatedwaitingperiodbeforecoveragebecameeffective.
6. Imustprovide,uponrequestfromKaiserPermanente,acopyofmycompany’sfictitiousnamestatement,DBA,legalpartnershipagreementandScheduleK,articlesofincorporation,ScheduleC,currentbusinesslicense,orcurrentprofessionallicense.
IunderstandthatthisinformationmaybesubjecttoverificationandagreetoprovideKaiserFoundationHealthPlan,Inc.,withanyinformationnecessarytodoso.IalsounderstandthatfailuretomeettheaboveconditionsmayresultindenialorterminationofgrouphealthcoveragefromKaiserFoundationHealthPlan,Inc.,forthebelow-namedcompany.
XProprietor,partner,orcorporateofficer’ssignature
Printproprietor,partner,orcorporateofficer’sname
Title
Date
Companyname
XProprietor,partner,orcorporateofficer’ssignature
Printproprietor,partner,orcorporateofficer’sname
Title
Date
Companyname
ProPriEtor/PArtnEr/ corPorAtE oFFicEr Form

11
administEringYour grouP HEaltH Plan
12
Accounting and billing
▲WhomdoIcontactwithbillingquestions?
YoumayuseOnlineAccountServicestochecktheenrollmentstatusofyouremployees,verifybills,
andconfirmreceiptofpayment.Visitemployers.kaiserpermanente.org,selectyourcompany’s
region,andclickon“Accessaccount.”
YoumayalsocalltheCustomerServiceCenterat1-800-790-4661,option1,from8a.m.to5p.m.,
MondaythroughFriday.
▲WherecanIfindmygroup’srates?
PleaserefertoyourrenewedGroupAgreementcontract,whichwillbemailedtoyouatleast30days
priortoyourgroup’sanniversarydateeachyear.
benefits
▲WherecanIfindinformationaboutmygroup’sbenefits?
PleaseseeyourGroupAgreementcontract.
▲Whomdomyemployeescalliftheyhavebenefitquestions?
YouremployeesandtheirfamiliesmaycallourMemberServiceCallCenterat1-800-464-4000,from
7a.m.to7p.m.weekdays,and7a.m.to3p.m.weekends(excludingholidays).
cobrA and cal-cobrA
▲HowdoIputsomeoneonCOBRAorCal-COBRA?
PleaserefertotheCOBRA/Cal-COBRAsectiononpage25ofthisbooklet.
FaQFrequently asked questions aboutadministeringgrouphealthplans
13
contract and rates
▲HowcanIgetacopyofmyGroup Agreement contractorfindoutaboutrates?
CalltheAccountManagementTeamat1-800-790-4661,option2,from8:30a.m.to5p.m.,Monday
throughFriday.
Account authorization
▲CanIauthorizeotherpeopletoaccessandadministermygroupaccount?YoucanassignanemployeeoryourbrokerasanInterestedParty.AnInterestedPartyisanindividual
authorizedtoaccessandadministerprivateinformationaboutyourgroupaccountonyourbehalf.
ToassignanInterestedParty,pleasecalltheCustomerServiceCenterat1-800-790-4661,option1,
toobtainaPurchaserContactChangeForm.Faxthecompletedformto1-800-369-8010.Ifyouhave
furtherquestions,pleasecalltheCustomerServiceCenterat1-800-790-4661,option1,from8a.m.
to5p.m.,MondaythroughFriday.
dates
▲HowcanIfindoutmygroup’srenewal/anniversarydate?
PleaserefertoyourGroupAgreementcontract.
▲Whatisanevent date?
Aneventdateisthedateofaqualifyingeventthatresultedeitherintheenrollmentofanemployeeor
intheadditionordeletionofadependent.
Examples of event dates:
■ Dateofbirth ■ Datecoveragewaslost ■ Dateofhire
■ Dateofmarriage ■ Dateofadoption ■ Dateofrehire
FaQ

14
dental
▲HowandwhencanIaddDeltaDentalcoverage?
YoucanaddDeltaDentalcoverageonyourgroup’srenewal/anniversarydate.ForDeltaDentalof
Californiahighlightsandrates,calltheAccountManagementTeamat1-800-790-4661,option2,
8:30a.m.to5p.m.,MondaythroughFriday.
dependents
▲Whatisthemaximumagelimitfordependentchildren?
Childrencanstayonagroupplanuntiltheyare19;studentscanremainontheplanuntilthey
are24ifthesubscribercompletestheStudentCertificationForm.Disableddependentsmay
remainontheplanaslongastheymeettheeligibilityrequirementsfordisableddependents.
PleaserefertoyourGroupAgreementfordetails.
▲HowdoIaddordeletedependents?
Toaddordeleteadependent,completeanAccountChangeForm(providedonpage29of
thisbooklet).YoumayalsoaddordeletedependentselectronicallyusingOnlineAccount
Services.Visitemployers.kaiserpermanente.organdselectyourcompany’sregion;thenclick
on“Accessyouraccount”(seepage18formoreinformation).
▲Arefamilymemberscovered?
Employeescanenrollspouses,domesticpartners,biologicalchildren,adoptedchildren,
stepchildren,childrenoftheirdomesticpartners,orchildrenforwhomtheemployeehas
obtainedlegalguardianshipasdescribedintheGroupAgreement.
FaQcontinued
15
Enrollment
▲HowdoIenrollanewemployee?
Onceanewemployeehascompletedthenew-hireeligibilityperiod,theemployeeneedsto
completeandsignanEnrollmentForm.Youmayenrollnewemployeeselectronicallyusing
OnlineAccountServices.Visitemployers.kaiserpermanente.organdselectyourcompany’s
region.Clickon“Accessyouraccount”(seepage18formoreinformation).Ifyoudonothave
accesstotheInternet,sendcompletedenrollmentformsviafaxormailto:
northern california southern california KaiserFoundationHealthPlan KaiserFoundationHealthPlan
P.O.Box23219 P.O.Box23250
SanDiego,CA92193-3219 SanDiego,CA92193-3250
Fax:(858)614-3344 Fax:(858)614-3345
▲HowdoIgetanEnrollment FormoranAccount Change Form?
YoumayrequestformsbycallingtheCustomerServiceCenterat1-800-790-4661,
option1,8a.m.to5p.m.,MondaythroughFriday.OryoumayvisitourWebsiteat
kp.org/ca/smallbusinesscustomertodownloadandprinttheseandotherforms.
▲HowdoIfindoutifyouhavereceivedanEnrollment Formoran Account Change Form?
CalltheCustomerServiceCenterat1-800-790-4661,option1,from8a.m.to5p.m.,Monday
throughFriday.Wecanverifywhetherwehavereceivedfaxedformsafter72hours.Mostformsare
processedwithin7to10daysofreceipt.
▲Whendoescoverageforarehirebecomeeffective?
Coverageforarehireiseffectiveonthefirstofthemonthfollowingthedateofrehire,iftherehire
dateiswithinoneyearoftheoriginalterminationdate.Iftherehiredateislaterthanoneyear
followingtermination,theemployeeisconsideredtobeanewhireandmustsatisfythenew-hire
eligibilityperiod.
16
▲Whatislossofcoverage?
Lossofcoverageiswhenanemployeeloses
grouphealthcarecoveragethroughnofault
ofhisorherown.Theemployeeiseligible
forcoverageonagroupplanonthefirstof
themonthfollowingthedateofloss.When
completingtheEnrollmentForm,check
“Other”intheenrollmentboxandwritein
lossofcoverage.(Inthiscase,theeventdate
isthedatecoveragewaslost.)
▲Whatisanew-hireprobationaryperiod?
Thenew-hireprobationaryperiodisthelength
oftimeanemployeemustwaitbeforebecoming
eligibleforhealthcoverageonthefirstofthe
followingmonth.Youselectyournew-hire
probationaryperiodwhenyouactivateorrenew
yourcontract.
▲Whatisopenenrollment?
Openenrollmentistheperiodoftimeduring
whichyouareallowedtoofferhealthcare
coveragetoemployeeswhodidnotelect
coveragewhentheybecameeligibleandto
addemployeeswhowishtochangetheirhealth
carriers.Employeesmayalsoadddependents
notpreviouslyenrolledduringthistime.
Openenrollmentusuallyoccursduringthe
monthbeforetheanniversaryofyourcompany’s
enrollmentinKaiserPermanente.
▲Howmanyhoursdoesmyemployee havetoworktobeeligibleforhealth coverage?
Employeesmustwork20hoursormoreperweek.
Youmaydetermineyourcompany’sowneligibility
requirementsaslongaseligibleemployeeswork
atleast20hoursperweek.
17
identification card▲HowcanmyemployeesobtainservicespriortoreceivingKaiserPermanente identificationcards?
Employeescanreceivecareatourfacilitiesanytimeafteryourgroup’scoveragebecomes
effective.AnemployeewillsimplyfillouttheTemporaryMembershipIDFormfoundinthe
enrollmentbookandpresentittothereceptionist,alongwithacopyofhisorherEnrollment
FormandpictureID.
▲HowcanmyemployeesreplacetheirKaiserPermanenteidentificationcards?
EmployeescancallourMemberServiceCallCenterat1-800-464-4000from7a.m.to7p.m.
weekdays,and7a.m.to3p.m.weekends(excludingholidays).
information online▲CanIdownloadinformationandformsfromyourWebsite?
Foryourconvenience,thefollowingdocumentscanbedownloadedandprintedatanytimefrom
ourWebsiteatemployers.kp.org.
■ AccountChangeForm
■ SubscriberTerminationandTransferForm
■ COBRAInformationSheetandCOBRAEnrollmentForm
■ PlanChangeRequestForm
■ ContinuationofCoverageOptions
■ RequestforScheduleA
■ StudentCertification
■ DisabledDependentEnrollmentApplication
termination▲HowdoIterminateanemployee’scoverage?
UsetheTerminationReportonpage33.AllformsmustbereceivedbyKaiserPermanente
withintwomonthsofthedateoftermination.Theeffectivedateisalwaysthefirstofthemonth
followingthedateoftermination.
18
onlinE account servicesit’s easier electronicallyNomatterwhatsizeyourbusinessis,youcantakeadvantageofKaiserPermanente’stime-saving
e-businessfunctions.
our Web site is simple to use—you’ll be surprised at just how easy it is to manage your account online.
You’ll have round-the-clock access to help ensure the accuracy of your bills and reduce processing times.
register for our e-business services today.
Efficienteligibilitymanagement
Visitemployers.kaiserpermanente.organdselectyourcompany’sregion.Clickon“Accessyour
account.”Fromthere,youcan:
■ take a tour of our online services.
■ register. WhenyoufilloutaUserIDRequestForm,we’llmailyouaccessand
sign-oninstructions.
■ sign in.Useyourusernameandpasswordtoaccessandmanageyouraccount
anytimeusingouronlineadministrationtools.
Withouronlineservices,youcanlogonanytimetoenrollorterminateemployeesandtheirdependents
andamenddemographicinformation.Mosttransactionsarecompletedimmediately.Pleaseprintacopy
ofthecompletedformsforyourrecords.
Promptcustomerservice
Useouronlinefunctionstochecktheenrollmentstatusofyouremployeesandtheirdependents,
verifybills,andconfirmreceiptofpayments.OurWebsiteoffersconvenientcommunicationwith
ourAccountManagementTeam.
19
Onlinebillpayment
There’snomorewaitingforbillstoarriveinthemail—withourpaperlessbillingfunction,we’lle-mail
youwhenyourbillisreadyforviewing(youwillcontinuetoreceiveapaperbillinthemail).Youcan
submityourpaymentelectronically.Onlinedataentryandcommunicationbetweenyourgroupand
KaiserPermanentehelpimproveaccuracyofinformation.
WhatareOnlineAccountServices?
OnlineAccountServicesaresecurefeaturesdevelopedspecificallytohelpemployersmanage
theirKaiserPermanenteaccounts.Theseservicesallowyouto:
■ Addorterminateemployeeanddependentcoverage*
■ Changeemployeeanddependentdemographicinformation
■ Viewalistofsubscribersandtheircovereddependents
■ Viewyourbalancedue
■ Viewtransactionhistory
■ Viewyourmonthlybill
■ Payyourbill
Aretheseservicesfree?
Yes.
Areenrollmentchangesimmediatelycompleted?
Demographicandcoveragechangesarecompletedimmediately.(Coveragechangesmayinclude
addinganewborn,newspouse,orotherdependents,aswellasterminations.)Thatmeanstheyare
registeredonoursystemwhenyouclickthe“Submit”button.Terminationsareeffectivethefirstday
ofthefollowingmonth.Whentheonlinesystemcan’tmatchtheenrolleetoanexistingrecordwith
100percentaccuracy,theinformationwillbesenttoanaccountadministrationrepresentativefor
manualprocessing.Ourservicegoalistoprocesstheseenrollmentswithintwobusinessdays.
*Whenaddinganemployee,pleaseprintacopyoftheEnrollmentForm,havetheemployeesign
theform,andkeepitforyourrecords.
onlinE account services
20
onlinE account services continued
CanIstilltransmitmembershipinformationviaelectronicfiletransfer?
Yes.Infact,weencourageit.Sendingmembershipchangeselectronicallyisagreatwaytogo.
However,theonlinefunctionscanstillbenefityouby:
■ Providingaquickwaytogetastatusonyouraccountwithoutmakingaphonecall
■ Allowingyoutoworkaccordingtoyourschedule,withoutlimitingyoutoKaiserPermanente’s
servicehours
WillIstillreceiveapaperbill?
Yes,youwillalsoreceiveapaperbill.
DoIhavetousetheInternetforeverything?
No.WeareofferingyoutheuseoftheInternetasanadditional,convenientwaytoworkwith
KaiserPermanente.WebelieveitmakestheadministrationofyourKaiserPermanentehealthcare
planeasier.ThinkofOnlineAccountServicesasa“healthplanATM,”asitprovidesyouwithfast
service.Youwillstillhaveanassignedaccountadministrationrepresentativewhoisavailablefrom
8a.m.to5p.m.,MondaythroughFriday,forone-on-onecustomerservice.
WillthisservicehandleCOBRAenrollments?
Yes,youcanprocessCOBRAenrollmentsusingOnlineAccountServices.*
*ThisfeaturedoesnotapplytoCOBRAplansdirectlybilledtothemember.
21
WillmyemployeeshaveaccesstotheOnlineAccountServicessite?
No.Thesiteisonlyfortheuseofyourdesignatedcompanyrepresentativetomanageyourhealth
planaccountsonline.EmployeeswhohaveselectedKaiserPermanenteastheirhealthplancanuse
ourWebsite,members.kaiserpermanente.org,to:
■ Requestroutineappointments*
■ Usethehealthanddrugencyclopedias
■ Contactapharmacistwithanonurgentquestion*
■ Accessotherusefulfeaturestohelpthemmanagetheirhealthcare
CanIcreateanadditionaluserIDforanotherperson?
Absolutely.KaiserPermanentewillprovideyouwithoneuserIDthatgivesyouadministrator
privileges.ThatIDallowsyoutocreateadditionaluserIDsforthoseyouwishtoaccessthesite
andtovarytheirprivilegesaccordingtotheirresponsibilities.(Youwillfindthisfunctionunder
the“Accountaccess”drop-downmenuwithinOnlineAccountServices.)
WhencanIbeginusingOnlineAccountServices?
AssoonasyoureceiveyourpurchaserID,youcanpreviewOnlineAccountServicesbytakingasite
tour.AttheendofthetouryoucandownloadaUserIDRequestForm(thisformcanalsobefound
onpage23ofthishandbook)andfaxittous.YoushouldreceiveauserIDandpasswordinthemail
withinsevenbusinessdayssoyoucanbeginusingthesite.Pleasenotethatyoumustlistyourselfas
the“Requester”ontheform.Forsecuritypurposes,wewillonlymailtheuserIDandpasswordtoyou.
*Someservicesarenotavailableinallareas.

22
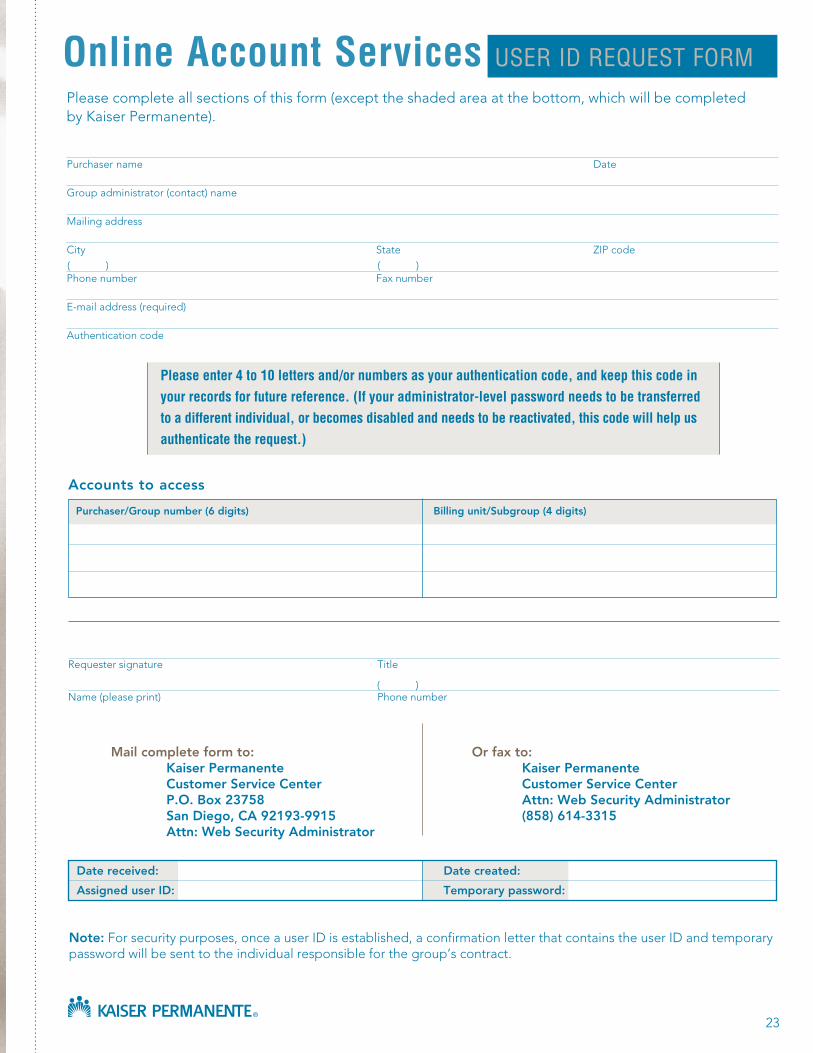
23
Note:Forsecuritypurposes,onceauserIDisestablished,aconfirmationletterthatcontainstheuserIDandtemporarypasswordwillbesenttotheindividualresponsibleforthegroup’scontract.
Accountstoaccess
Requestersignature Title
Name(pleaseprint) Phonenumber
Mailcompleteformto: Orfaxto: KaiserPermanente KaiserPermanente CustomerServiceCenter CustomerServiceCenter P.O.Box23758 Attn:WebSecurityAdministrator SanDiego,CA92193-9915 (858)614-3315 Attn:WebSecurityAdministrator
Pleasecompleteallsectionsofthisform(excepttheshadedareaatthebottom,whichwillbecompletedbyKaiserPermanente).
Purchasername Date
Groupadministrator(contact)name
Mailingaddress
City State ZIPcode
Phonenumber Faxnumber
E-mailaddress(required)
Authenticationcode
() ()
()
Please enter 4 to 10 letters and/or numbers as your authentication code, and keep this code in your records for future reference. (if your administrator-level password needs to be transferred to a different individual, or becomes disabled and needs to be reactivated, this code will help us authenticate the request.)
Purchaser/Groupnumber(6digits) Billingunit/Subgroup(4digits)
Datereceived: Datecreated:
AssigneduserID: Temporarypassword:
online Account services usEr id rEQuEst Form

24
25
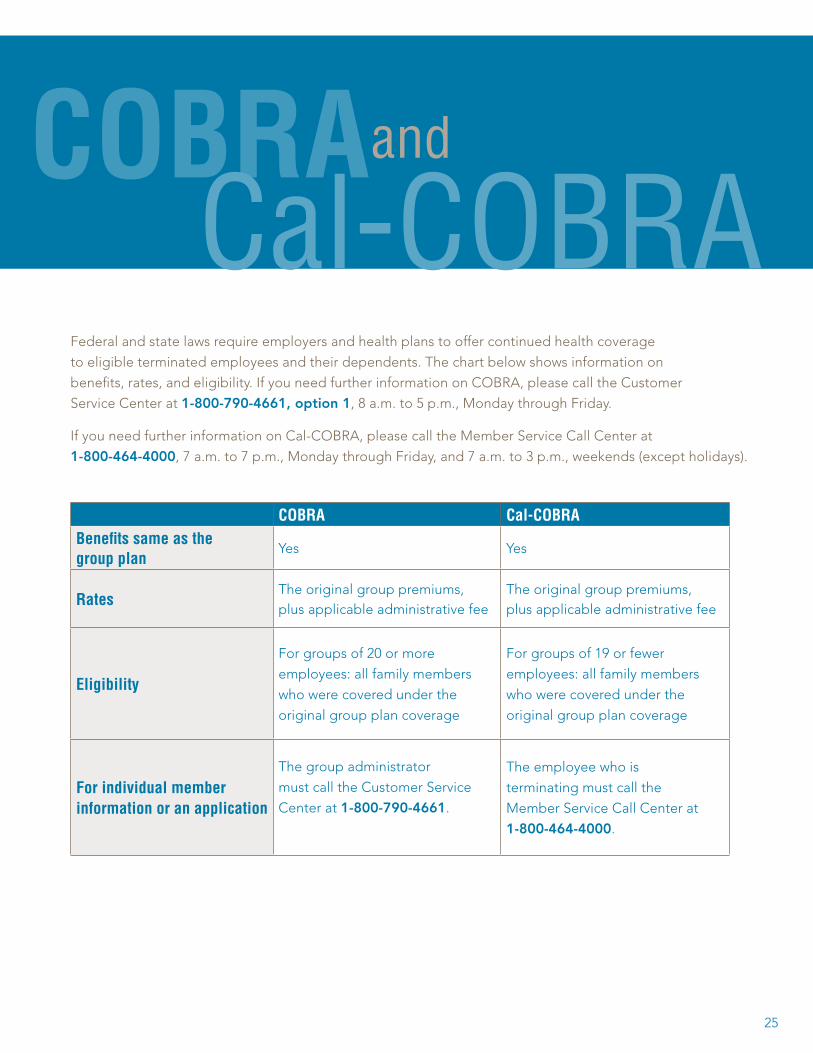
Federalandstatelawsrequireemployersandhealthplanstooffercontinuedhealthcoverage
toeligibleterminatedemployeesandtheirdependents.Thechartbelowshowsinformationon
benefits,rates,andeligibility.IfyouneedfurtherinformationonCOBRA,pleasecalltheCustomer
ServiceCenterat1-800-790-4661,option1,8a.m.to5p.m.,MondaythroughFriday.
IfyouneedfurtherinformationonCal-COBRA,pleasecalltheMemberServiceCallCenterat
1-800-464-4000,7a.m.to7p.m.,MondaythroughFriday,and7a.m.to3p.m.,weekends(exceptholidays).
cobrA cal-cobrAbenefits same as the group plan
Yes Yes
ratesTheoriginalgrouppremiums,plusapplicableadministrativefee
Theoriginalgrouppremiums,plusapplicableadministrativefee
Eligibility
Forgroupsof20ormore
employees:allfamilymembers
whowerecoveredunderthe
originalgroupplancoverage
Forgroupsof19orfewer
employees:allfamilymembers
whowerecoveredunderthe
originalgroupplancoverage
For individual memberinformation or an application
Thegroupadministrator
mustcalltheCustomerService
Centerat1-800-790-4661.
Theemployeewhois
terminatingmustcallthe
MemberServiceCallCenterat
1-800-464-4000.
cobrA cal-coBra
and
26
Avoiding processing delays
Topreventprocessingdelays,youshouldsubmitcompletedEnrollmentForms
throughoutthemonth—assoonasyoureceivethemfromyouremployees.Delays
inprocessingareoftenduetomissingandinaccurateinformation.Usethefollowing
checklisttohelpmakecertainallthenecessaryinformationiscompleteandcorrect.
Formscanbefaxedormailedto:
NorthernCalifornia SouthernCaliforniaKaiserFoundationHealthPlan KaiserFoundationHealthPlan
P.O.Box23219 P.O.Box23250
SanDiego,CA92193-3219 SanDiego,CA92193-3250
Fax:(858)614-3344 Fax:(858)614-3345
Haveyouincludedthefollowing?
■ Groupnumber
■ Enrollment/Billingunitnumber/plan
■ Medicalrecordnumber(ifknown)foreachsubscriberanddependent
■ Dateofbirthforeachsubscriberanddependent
■ SocialSecuritynumberforeachsubscriberanddependent
■ Fulladdresses
■ Signatureofthesubscriber
■ Dateofhireorqualifyingevent
Remembertokeepacopyforyourrecords.

Avoiding processing delays

28
Usethefollowingformstorequestchangestoyouraccount.Ifyouneedadditionalforms,youcanmake
copiesoftheoriginalsorcalltheCustomerServiceCenterat1-800-790-4661,option1,from8a.m.to
5p.m.,MondaythroughFriday,toordermore.Youcanalsodownloadandprinttheseformsonlineat
anytimethroughourWebsiteatemployers.kaiserpermanente.org.
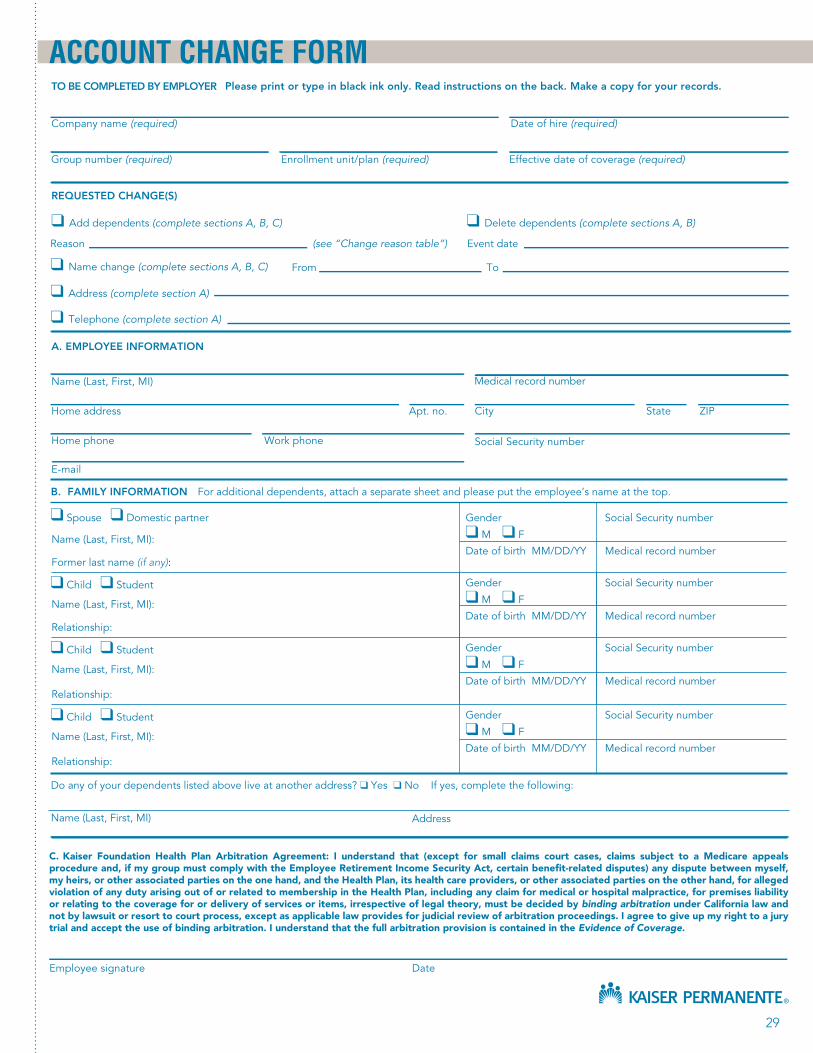
Account Change Form:Usethisformtoenrollnewemployees,addordeletedependents,ormake
addressornamechanges.Seepage29.
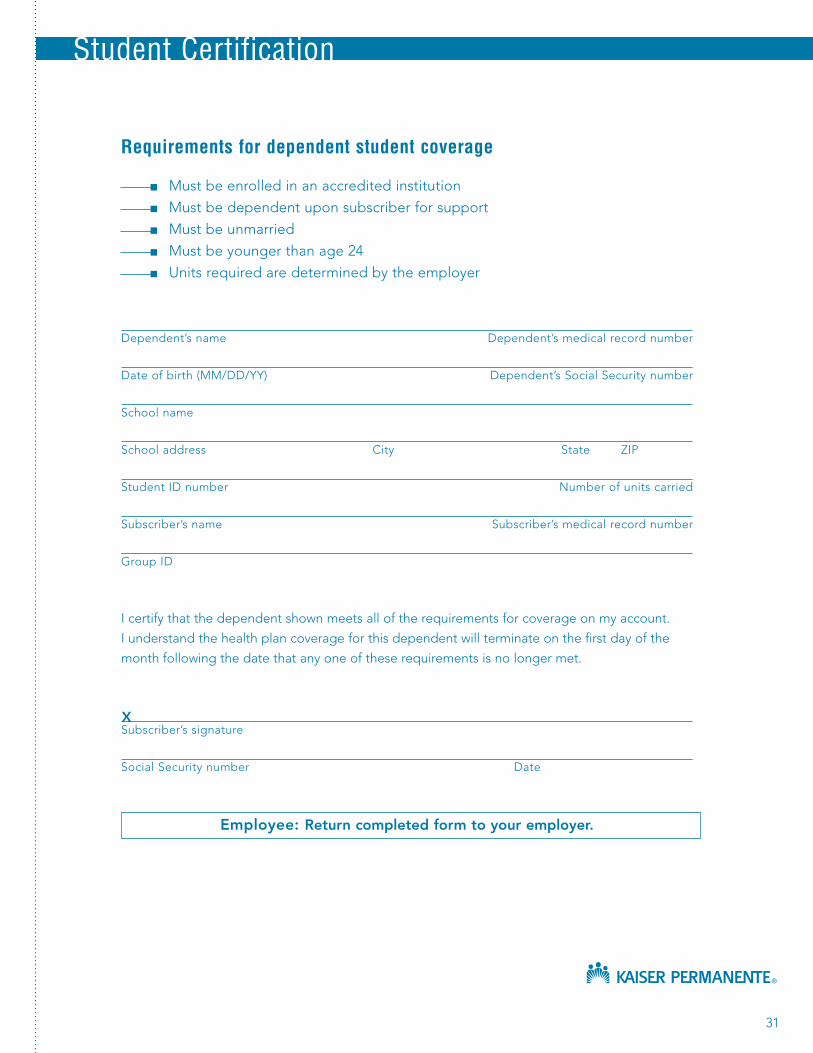
Student Certification:Thesubscribermustcompletethisformcertifyingthatthedependentqualifies
forcoverageasaneligiblestudent.Seepage31.
Termination Report:Completethisformtoshowterminationstoyouraccount.Seepage33.
FormsAccount Change Form
Student Certification
Termination Report
temporary payment coupons
29
C. Kaiser Foundation Health Plan Arbitration Agreement: I understand that (except for small claims court cases, claims subject to a Medicare appeals procedure and, if my group must comply with the Employee Retirement Income Security Act, certain benefit-related disputes) any dispute between myself, my heirs, or other associated parties on the one hand, and the Health Plan, its health care providers, or other associated parties on the other hand, for alleged violation of any duty arising out of or related to membership in the Health Plan, including any claim for medical or hospital malpractice, for premises liability or relating to the coverage for or delivery of services or items, irrespective of legal theory, must be decided by binding arbitration under California law and not by lawsuit or resort to court process, except as applicable law provides for judicial review of arbitration proceedings. I agree to give up my right to a jury trial and accept the use of binding arbitration. I understand that the full arbitration provision is contained in the Evidence of Coverage.
TO BE COMPLETED BY EMPLOYER
Company name (required) Date of hire (required)
Group number (required) Enrollment unit/plan (required) Effective date of coverage (required)
REQUESTED CHANGE(S)
❑ Add dependents (complete sections A, B, C) ❑ Delete dependents (complete sections A, B)
Reason (see “Change reason table”) Event date
❑ Name change (complete sections A, B, C) From To
❑ Address (complete section A)
❑ Telephone (complete section A)
Employee signature Date
ACCOUNT CHANGE FORMPlease print or type in black ink only. Read instructions on the back. Make a copy for your records.
A. EMPLOYEE INFORMATION
Social Security number
Home phone Work phone
Home address Apt. no. City State ZIP
Name (Last, First, MI) Medical record number
Do any of your dependents listed above live at another address? ❑ Yes ❑ No If yes, complete the following:
Name (Last, First, MI) Address
B. FAMILY INFORMATION For additional dependents, attach a separate sheet and please put the employee’s name at the top.
❑ Spouse ❑ Domestic partner Gender Social Security number
Name (Last, First, MI): ❑ M ❑ F
Date of birth MM/DD/YY Medical record numberFormer last name (if any):
❑ Child ❑ Student Gender Social Security number
Name (Last, First, MI): ❑ M ❑ F
Date of birth MM/DD/YY Medical record numberRelationship:
❑ Child ❑ Student Gender Social Security number
Name (Last, First, MI): ❑ M ❑ F
Date of birth MM/DD/YY Medical record numberRelationship:
❑ Child ❑ Student Gender Social Security number
Name (Last, First, MI): ❑ M ❑ F
Date of birth MM/DD/YY Medical record numberRelationship:
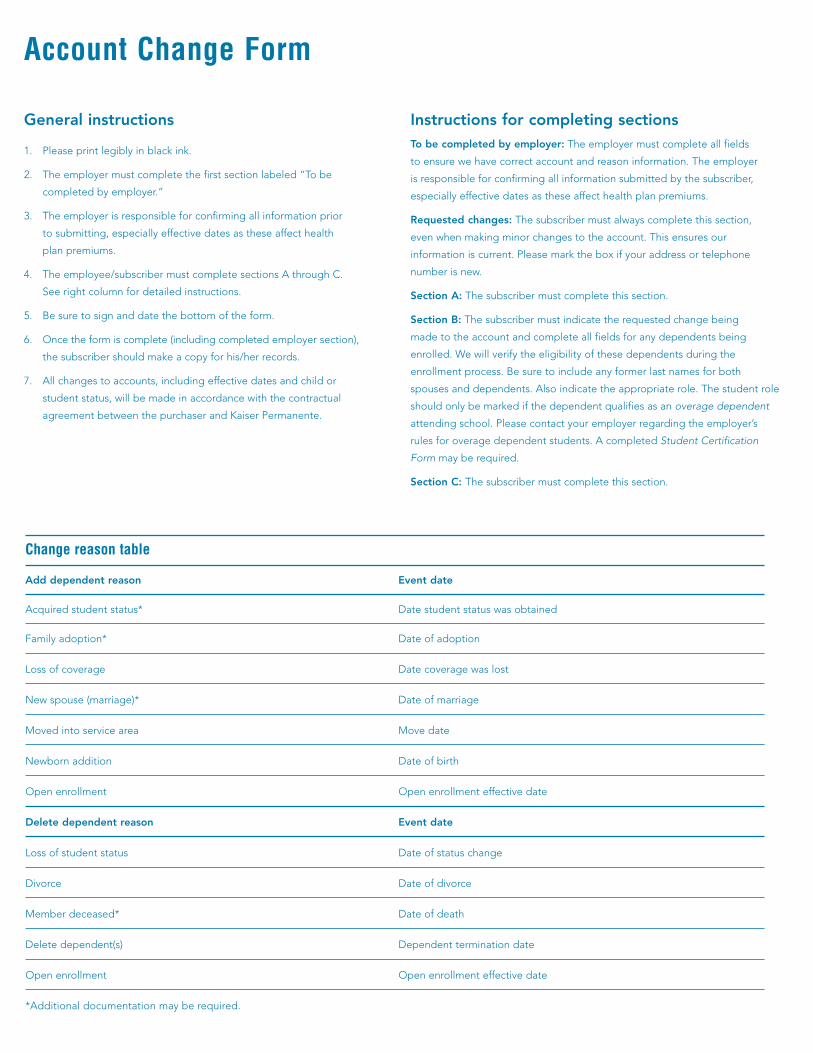
change reason table
Adddependentreason Eventdate
Acquiredstudentstatus* Datestudentstatuswasobtained
Familyadoption* Dateofadoption
Lossofcoverage Datecoveragewaslost
Newspouse(marriage)* Dateofmarriage
Movedintoservicearea Movedate
Newbornaddition Dateofbirth
Openenrollment Openenrollmenteffectivedate
Deletedependentreason Eventdate
Lossofstudentstatus Dateofstatuschange
Divorce Dateofdivorce
Memberdeceased* Dateofdeath
Deletedependent(s) Dependentterminationdate
Openenrollment Openenrollmenteffectivedate
*Additionaldocumentationmayberequired.
Account change Form
Generalinstructions
1. Pleaseprintlegiblyinblackink.
2. Theemployermustcompletethefirstsectionlabeled“Tobe
completedbyemployer.”
3. Theemployerisresponsibleforconfirmingallinformationprior
tosubmitting,especiallyeffectivedatesastheseaffecthealth
planpremiums.
4. Theemployee/subscribermustcompletesectionsAthroughC.
Seerightcolumnfordetailedinstructions.
5. Besuretosignanddatethebottomoftheform.
6. Oncetheformiscomplete(includingcompletedemployersection),
thesubscribershouldmakeacopyforhis/herrecords.
7. Allchangestoaccounts,includingeffectivedatesandchildor
studentstatus,willbemadeinaccordancewiththecontractual
agreementbetweenthepurchaserandKaiserPermanente.
InstructionsforcompletingsectionsTobecompletedbyemployer:Theemployermustcompleteallfields
toensurewehavecorrectaccountandreasoninformation.Theemployer
isresponsibleforconfirmingallinformationsubmittedby thesubscriber,
especiallyeffectivedatesastheseaffecthealthplan premiums.
Requestedchanges:Thesubscribermustalwayscompletethissection,
evenwhenmakingminorchangestotheaccount.Thisensuresour
informationiscurrent.Pleasemarktheboxifyouraddressortelephone
numberisnew.
SectionA:Thesubscribermustcompletethissection.
SectionB:Thesubscribermustindicatetherequestedchangebeing
madetotheaccountandcompleteallfieldsforanydependentsbeing
enrolled.Wewillverifytheeligibilityofthesedependentsduringthe
enrollmentprocess.Besuretoincludeanyformerlastnamesforboth
spousesanddependents.Alsoindicatetheappropriaterole.Thestudentrole
shouldonlybemarkedifthedependentqualifiesasanoveragedependent
attendingschool.Pleasecontactyouremployerregardingtheemployer’s
rulesforoveragedependentstudents.AcompletedStudentCertification
Formmayberequired.
SectionC:Thesubscribermustcompletethissection.
31
requirements for dependent student coverage
■ Mustbeenrolledinanaccreditedinstitution
■ Mustbedependentuponsubscriberforsupport
■ Mustbeunmarried
■ Mustbeyoungerthanage24
■ Unitsrequiredaredeterminedbytheemployer
Dependent’sname Dependent’smedicalrecordnumber
Dateofbirth(MM/DD/YY) Dependent’sSocialSecuritynumber
Schoolname
Schooladdress City State ZIP
StudentIDnumber Numberofunitscarried
Subscriber’sname Subscriber’smedicalrecordnumber
GroupID
Icertifythatthedependentshownmeetsalloftherequirementsforcoverageonmyaccount.
Iunderstandthehealthplancoverageforthisdependentwillterminateonthefirstdayofthe
monthfollowingthedatethatanyoneoftheserequirementsisnolongermet.
Subscriber’ssignature
SocialSecuritynumber Date
Employee:Returncompletedformtoyouremployer.
X
student certification

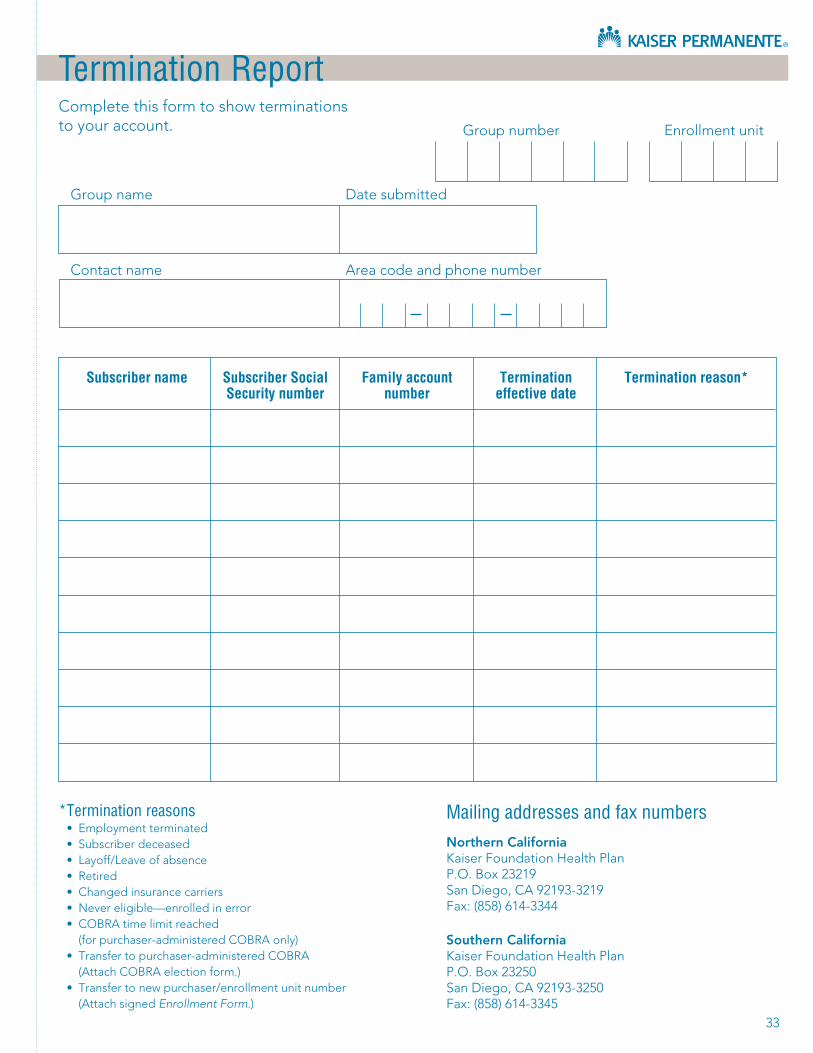
33
termination report
Groupnumber Enrollmentunit
Groupname Datesubmitted
Contactname Areacodeandphonenumber
subscriber name subscriber social Family account termination termination reason* security number number effective date
* termination reasons • Employmentterminated• Subscriberdeceased• Layoff/Leaveofabsence• Retired• Changedinsurancecarriers• Nevereligible—enrolledinerror• COBRAtimelimitreached (forpurchaser-administeredCOBRAonly)• Transfertopurchaser-administeredCOBRA (AttachCOBRAelectionform.)• Transfertonewpurchaser/enrollmentunitnumber (AttachsignedEnrollmentForm.)
mailing addresses and fax numbersNorthernCaliforniaKaiserFoundationHealthPlanP.O.Box23219SanDiego,CA92193-3219Fax:(858)614-3344
SouthernCaliforniaKaiserFoundationHealthPlanP.O.Box23250SanDiego,CA92193-3250Fax:(858)614-3345
Completethisformtoshowterminationstoyouraccount.

35
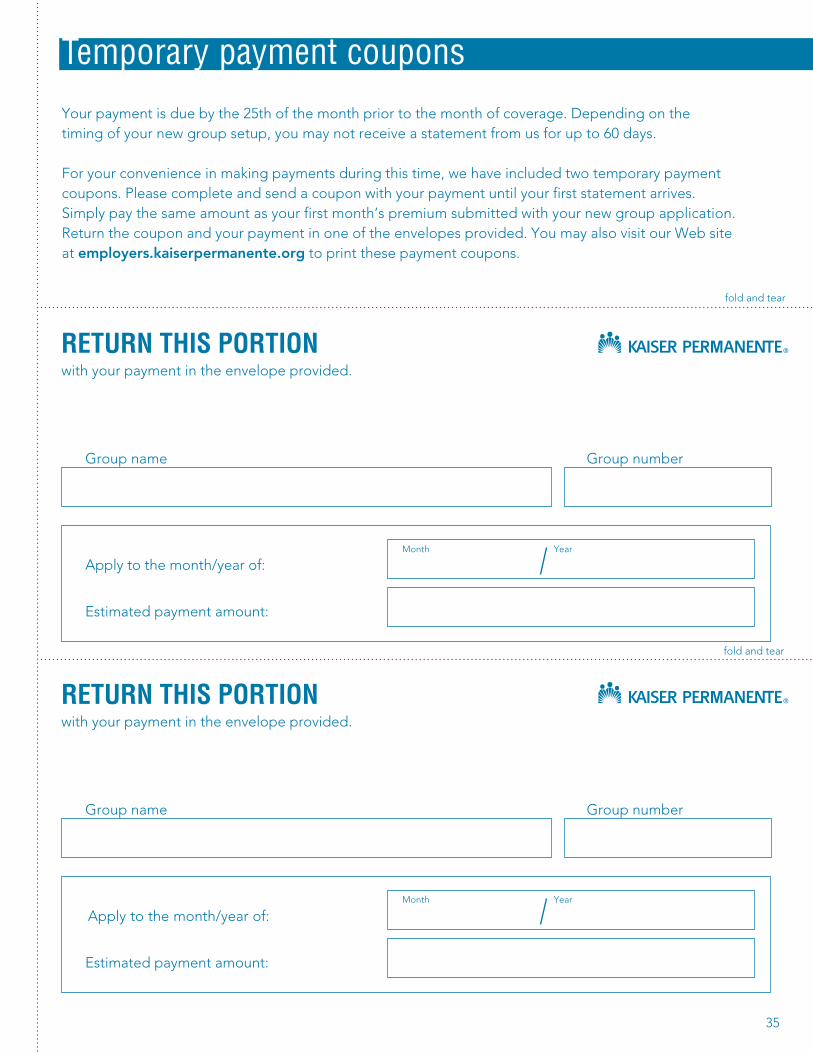
temporary payment coupons
Yourpaymentisduebythe25thofthemonthpriortothemonthofcoverage.Dependingonthetimingofyournewgroupsetup,youmaynotreceiveastatementfromusforupto60days.
Foryourconvenienceinmakingpaymentsduringthistime,wehaveincludedtwotemporarypaymentcoupons.Pleasecompleteandsendacouponwithyourpaymentuntilyourfirststatementarrives.Simplypaythesameamountasyourfirstmonth’spremiumsubmittedwithyournewgroupapplication.Returnthecouponandyourpaymentinoneoftheenvelopesprovided.YoumayalsovisitourWebsiteatemployers.kaiserpermanente.orgtoprintthesepaymentcoupons.
rEtUrn tHis Portionwithyourpaymentintheenvelopeprovided.
Groupname Groupnumber
Applytothemonth/yearof:
Estimatedpaymentamount:
rEtUrn tHis Portionwithyourpaymentintheenvelopeprovided.
Groupname Groupnumber
Applytothemonth/yearof:
Estimatedpaymentamount:
Month Year
foldandtear
foldandtear
Month Year

36
temporary payment envelopes
Mailyourmonthlypaymentusingthesepre-addressedremittance
envelopes.Ifyouneedadditionalenvelopes,pleasecallthe
CustomerServiceCenterat1-800-790-4661,option1,from8a.m.
to5p.m.,MondaythroughFriday.

kaiserpermanente.org
25651





























