Embed Size (px)
Citation preview

CASE REPORT
Zopiclone-Induced Acute Interstitial Nephritis
Naser Hussain, MD, Martin MacKinnon, MD, and Ayub Akbari, MD
● Zopiclone, a relatively new nonbenzodiazepine short-acting hypnotic medication is prescribed frequently forinsomnia. The authors report a case of zopiclone-induced acute interstitial nephritis in a young, otherwise healthyman. The patient presented with anuric acute renal failure requiring hemodialysis. Kidney biopsy results showedacute interstitial nephritis with a prominent eosinophilic infiltrate in the interstitium. He recovered his renal functionafter stopping the medication and receiving corticosteroids. Am J Kidney Dis 41:E17.© 2003 by the National Kidney Foundation, Inc.
INDEX WORDS: Zopiclone; interstitial nephritis; acute renal failure (ARF).
ACUTE INTERSTITIAL nephritis (AIN) isan important cause of acute renal failure,
accounting for 15% of cases in some centers.1 Itmay occur in association with either kidney-limited or systemic autoimmune processes suchas systemic lupus erythematosus, sarcoidosis,1
infections,2 or result from exposure to medica-tions.3 In this report, we describe a case ofreversible acute renal failure secondary to AIN,which was most likely caused by zopiclone, ashort acting nonbenzodiazepine hypnotic agent,in an otherwise young healthy man. The patientrequired hemodialysis but recovered renal func-tion. To our knowledge, this is the first report ofAIN associated with the use of zopiclone.
CASE REPORT
An 18-year-old man presented to his familyphysician with a 2-week history of malaise, weak-ness, nausea, and vomiting. He reported de-creased urine output over a 3-day period. Atpresentation to our institution he had not passedurine for the last 12 hours. Urinary bladdercatheterization found 10 mL of urine. He deniedgross hematuria, fever, or upper respiratory tractsymptoms. Three weeks earlier, he was seen byhis family doctor for a skin rash involving hisarms and legs. At the time he denied any associ-ated symptoms such as arthralgias, iritis, or fe-ver.
The patient’s past medical history was signifi-cant for a schizophrenic episode approximately 2years before the current illness. The patient’sonly current medication was zopiclone (Imov-ane), 7.5 mg at night, which was started approxi-mately 4 weeks before for sleep disturbance. Thepatient denied the use of any over-the-countermedications, herbal remedies, or intravenous drug
use. He was a user of marijuana and had lastsmoked marijuana about 3 weeks before admis-sion to hospital.
Physical examination found a young man whowas in no distress. Blood pressure was 130/80,heart rate was 85 beats per minute, and respira-tory rate was 14 breaths per minute. There was anonraised, nontender erythematous rash cover-ing the chest and upper abdomen. The findingson cardiovascular and respiratory examinationswere within normal limits. With the exception ofthe rash, the abdominal examination findingswere normal. There was no lymphadenopathy orperipheral edema.
On admission, laboratory evaluation found ahemoglobin of 11.3 g/dL (113 g/L); white bloodcell count (WBC) of 9.8 � 103/�L (9.8 � 109/L),and eosinophill count was normal (0.1 � 109/L).His serum sodium concentration was 129 mEq/L(129 mmol/L), potassium was 3.5 mEq/L (3.5mmol/L), chloride was 89 mEq/L (89 mmol/L),and bicarbonate was 25 mEq/L (25 mmol/L).The urea was 141 mg/dL (50.3 mmol/L), andserum creatinine was 10.06 mg/dL (889 �mol/L). Serologic studies (antinuclear antibody andantineutrophil cytoplasmic antibodies), all werenegative. Complement levels (C3, C4) were
From the Department of Medicine and the Kidney Re-search Center, University of Ottawa, Ottawa, Ontario, Can-ada.
Received November 13, 2002; accepted in revised formDecember 18, 2002.
Address reprint requests to Ayub Akbari, MD, OttawaHospitals, Riverside Campus, 1967 Riverside, Suite5-25, Ottawa ON K1H 7W9, Canada. E-mail:[email protected]
© 2003 by the National Kidney Foundation, Inc.1523-6838/03/4105-0036$30.00/0PII: S0272-6386(03)00213-0
American Journal of Kidney Diseases, Vol 41, No 5 (May), 2003: E17 1
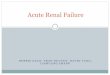
within the normal limits. Serum cryoglobulinswere negative. Anti–hepatitis B surface antibodywas positive, and hepatitis C serology was nega-tive. Results of a urinalysis showed microscopichematuria and no protein. Urine microscopy find-ings showed 5 to 30 white blood cells per high-power field and 5 to 30 red blood cells perhigh-power field and WBC casts. Urine micro-scopic examination for eosinophils was not per-formed. An abdominal ultrasound scan showedkidneys of normal size and appearance. Therewere no hydronephrosis, pelvic masses, or fluidcollections. The remainder of the abdomen wasnormal.
On admission, zopiclone was stopped, and thepatient received methylprednisolone, 250 mg in-travenously, on the first day and 500 mg intrave-nously on the second day. On the third day hewas switched to prednisone, 1 mg/kg/d (75 mg/d)orally. This dose was continued for 19 days. Thedose of prednisone then was decreased to 50mg/d for 1 week followed by 25 mg/d for 1 weekand then tapered by 5 mg every 3 days. Hemodi-alysis was initiated on the first day of admissionfor uremia and oligouric renal failure. On day 2,urine output began to improve. Hemodialysiswas stopped by day 3 when renal function hadsufficiently improved, and urine output had in-creased to 2 L/d.
A percutaneous left kidney biopsy, which wasdone on the second day of admission, found 10glomeruli, all of which were normal. The pathol-
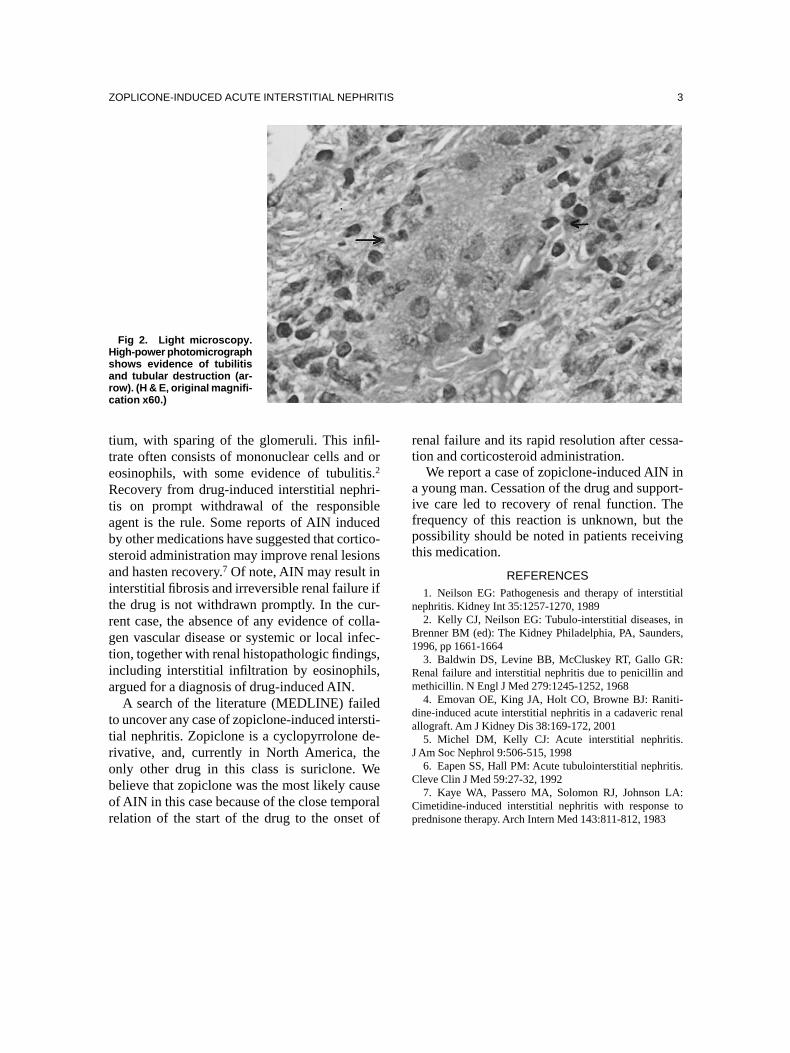
ogy in the interstitium showed marked edemaand a diffuse infiltrate of plasma cells, histio-cytes, and eosinophils. There was tubulitis andtubular destruction with a rare tubule containingred cells (Figs 1 and 2). Direct immunoflo-recence was negative for immunoglobulin G,immunoglobulin A, immunoglobulin M, orcomplement deposition. Overall, the features wereconsistent with an AIN.
The patient was discharged 5 days after admis-sion. On discharge, his rash had completely re-solved, he felt well, and serum creatinine levelwas 1.28 mg/dL (113 �mol/L) with normal elec-trolytes. He was advised not to take zopicloneagain. A follow-up check of his renal function 2weeks after discharge showed improved renalfunction with a serum creatinine level of 1.11mg/dL (98 �mol/L).
DISCUSSION
Drug-induced AIN typically manifests as acutenonoligouric renal failure associated with fever,skin rash, arthralgias, eosinophilia, and eosinophil-uria 7 to 21 days after exposure to a causativedrug.4 Drug hypersensitivity is now the leadingcause of AIN.5 Our patient did not have some ofthe classic symptoms of AIN such as fever,arthralgia, and eosinophilia, but recent studiessuggest that AIN is a heterogeneous disorder,and this classic picture is seen in less than 30%of cases.6 The hallmark of interstitial nephritis isinfiltration of inflammatory cells into the intersti-
Fig 1. Light microscopy.Low-power photomicrographshows a diffuse interstitialinfiltrate of lymphocytes,plasma cells, eosinophils,and interstitial edema. (H & E,original magnification x10.)
HUSSAIN, MACKINNON, AND AKBARI2
tium, with sparing of the glomeruli. This infil-trate often consists of mononuclear cells and oreosinophils, with some evidence of tubulitis.2
Recovery from drug-induced interstitial nephri-tis on prompt withdrawal of the responsibleagent is the rule. Some reports of AIN inducedby other medications have suggested that cortico-steroid administration may improve renal lesionsand hasten recovery.7 Of note, AIN may result ininterstitial fibrosis and irreversible renal failure ifthe drug is not withdrawn promptly. In the cur-rent case, the absence of any evidence of colla-gen vascular disease or systemic or local infec-tion, together with renal histopathologic findings,including interstitial infiltration by eosinophils,argued for a diagnosis of drug-induced AIN.
A search of the literature (MEDLINE) failedto uncover any case of zopiclone-induced intersti-tial nephritis. Zopiclone is a cyclopyrrolone de-rivative, and, currently in North America, theonly other drug in this class is suriclone. Webelieve that zopiclone was the most likely causeof AIN in this case because of the close temporalrelation of the start of the drug to the onset of
renal failure and its rapid resolution after cessa-tion and corticosteroid administration.
We report a case of zopiclone-induced AIN ina young man. Cessation of the drug and support-ive care led to recovery of renal function. Thefrequency of this reaction is unknown, but thepossibility should be noted in patients receivingthis medication.
REFERENCES1. Neilson EG: Pathogenesis and therapy of interstitial
nephritis. Kidney Int 35:1257-1270, 19892. Kelly CJ, Neilson EG: Tubulo-interstitial diseases, in
Brenner BM (ed): The Kidney Philadelphia, PA, Saunders,1996, pp 1661-1664
3. Baldwin DS, Levine BB, McCluskey RT, Gallo GR:Renal failure and interstitial nephritis due to penicillin andmethicillin. N Engl J Med 279:1245-1252, 1968
4. Emovan OE, King JA, Holt CO, Browne BJ: Raniti-dine-induced acute interstitial nephritis in a cadaveric renalallograft. Am J Kidney Dis 38:169-172, 2001
5. Michel DM, Kelly CJ: Acute interstitial nephritis.J Am Soc Nephrol 9:506-515, 1998
6. Eapen SS, Hall PM: Acute tubulointerstitial nephritis.Cleve Clin J Med 59:27-32, 1992
7. Kaye WA, Passero MA, Solomon RJ, Johnson LA:Cimetidine-induced interstitial nephritis with response toprednisone therapy. Arch Intern Med 143:811-812, 1983
Fig 2. Light microscopy.High-power photomicrographshows evidence of tubilitisand tubular destruction (ar-row). (H & E, original magnifi-cation x60.)
ZOPLICONE-INDUCED ACUTE INTERSTITIAL NEPHRITIS 3