A case of progressive pseudorheumatoid arthropathy of‘childhood’ with the diagnosis delayed to the fifth decade
A. CEFLE,1 K. CEFLE,2 M. TUNACI,3 S . OZTURK, 2 S . PALANDUZ2
Kocaeli University,1 Medical Faculty, Department of Internal Medicine, Division of Rheumatology, Kocaeli, Istanbul
University,2 Istanbul Medical Faculty, Department of Internal Medicine, Division of Medical Genetics, IstanbulxUniversity,3 Istanbul Medical Faculty, Department of Radiology, Istanbul, Turkey
SUMMARY
Progressive pseudorheumatoid arthropathy of childhood
(PPAC) is a rare single gene disorder which is frequently
misdiagnosed as juvenile rheumatoid arthritis. It is char-
acterised with arthralgia, joint contractures, bony swelling
of metacarpophalangeal and interphalangeal joints and
platyspondyly. Clinical and laboratory signs of joint
inflammation such as synovitis, a high erythrocyte sedi-
mentation rate and an elevated C-reactive protein level are
usually absent. Although the disease begins early in life
(usually between 3 and 8 years of age), the diagnosis may
be delayed. In the present case report, we describe a male
patient diagnosed with PPAC at the age of 46 years,
although he had been exhibiting the typical radiological
and clinical features of the disease since the age of 7 years.
Keywords: Progressive pseudorheumatoid arthropathy of
childhood
ª 2006 Blackwell Publishing Ltd
I N T R O D U C T I O N
Progressive pseudorheumatoid arthropathy of childhood
(PPAC) is a single gene disorder which is inherited in an
autosomal recessive manner. Alternative names of the dis-
ease are ‘spondyloepiphyseal dysplasia tarda (SEDT) with
progressive arthropathy’ and ‘progressive pseudorheumatoid
dysplasia’ (1). Although the frequency of the disease is not
known exactly, it is estimated to be one per million in Uni-
ted Kingdom. The main clinical features are arthralgia, joint
contractures, enlarged metacarpophalangeal and interphalan-
geal joints, platyspondyly and short stature. The onset of
the disease is usually between 3 and 8 years of age, and it is
frequently diagnosed erroneously as juvenile rheumatoid
arthritis (JRA). In the present case report, we describe a
male patient diagnosed with PPAC as late as at the age of
46 years, although he had been displaying the typical clin-
ical and radiological features of the disease since childhood.
C A S E
A 46-year-old male patient was admitted due to back and hip
pain of 4 years’ duration. His history was remarkable for
‘swelling’ of the interphalangeal and metacarpophalangeal
joints accompanied with a decrease in joint mobility which
had begun at the age of 7 years. He also described ‘enlarge-
ment of knees’ during the following years and a gradual
decrease of mobility involving nearly all the joints (knees,
shoulders, hips, servical and thoracal spine). He had also
joint pain mainly during physical activity, occasionally
intensifying also at rest and necessitating administrations of
non-steroidal anti-inflammatory drugs. He denied other
signs of arthritis including erythema and soft tissue swelling.
He had been evaluated in various hospitals without a defin-
ite diagnosis. For the last 4 years, the hip and back pain
worsened to the point of limiting daily activities without a
satisfactory response to non-steroid anti-inflammatory drugs.
The patient was born from a first-cousin marriage.
Remarkably, his sister and mother had a ‘joint disease’ with
many similarities: swelling of interphalangeal joints and knees
beginning in childhood, gradual limitation of mobility of
both peripheral and axial joints and back and hip pain.
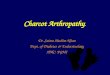
The height of the patient was 146 cm, and the weight
was 56 kg. On physical examination, the neck and the
trunk were found to be shortened. Flexion contractures and
bony enlargement of proximal and distal interphalangeal
joints were noted (Figures 1 and 2). Also bilateral wrist,
elbow, shoulder, knee and hip movements were limited.
Physical examination was normal otherwise.
The results of a urine analysis, complete blood count and
routine blood chemistry (including serum creatinine, calcium,
phoshorus alkaline phosphatase, aspartate aminotransferase
and alanine aminotransferase) were normal. The thyroid-
stimulating hormone, follicule-stimulating hormone, luteinis-
ing hormone and testosterone levels were normal. The
Correspondence to:Dr Kivanc Cefle, Istanbul Universitesi, Istanbul Tip Fakultesi, Ic
Hastaliklari AD, Tibbi Genetik BD, 34093 Capa, Istanbul, Turkey
Tel.: þ 90 212 414 23 22
Fax: þ 90 212 532 42 08
Email: [email protected]
CASE REPORT d o i : 1 0 . 1 1 1 1 / j . 1 7 4 2 - 1 2 4 1 . 2 0 0 5 . 0 0 6 6 2 . x
ª 2006 Blackwell Publishing Ltd Int J Clin Pract, October 2006, 60, 10, 1306–1309

erythrocyte sedimentation rate was 24 mm ⁄ h; C-reactive pro-
tein was in the normal range. The rheumatic facor was
negative. Echocardiographic and ophtalmological examina-
tion was unremarkable.
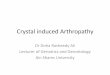
Plain radiographs of the hands showed bony enlargement of
metacarpophalangeal, proximal interphalangeal joints and joint
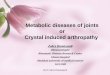
narrowing.Theknee jointswereenlarged similarly.Radiographs
of the spine (dorsal and lumber region) revealed osteophyitic
degeneration, decreased vertebral height (platyspondyly) and
narrowing of the intervertebral space (Figures 3, 4 and 5).
Coxofemoral joints were found to be heavily sclerosed with
narrowing of the joint space. Analysis of bone mineral density
by dual energy X-ray absorptometry (DEXA) showed a lomber
T-score of )3.65 and Z score of )3.28. Femoral T and Z scores
were 8.87and10.26, respectively.
The patient was diagnosed with PPAC based on the typical
clinical (childhood onset, bony swelling of interphalangeal
joints, gradual decrease in joint mobility, disabling hip and
back pain, lack of overt signs of arthritis and absence of
synovial involvement) and laboratory findings (osseous enlarge-
ment of joints and platyspondyly on skeletal radiograms,
normal erythrocyte sedimentation rate and C-reactive protein
level).
D I S C U S S I O N
PPAC was first described in 1983 by Spranger et al. (2) in five
patients as a hereditary arthropathy affecting ‘major and
minor joints’ (2). It is a rare hereditary disorder with auto-
somal recessive inheritance characterised by bony enlargement
of interphalangeal and metacarpophalangeal joints, flexion
Figure 1 Flexion deformity and ‘apparent’ swelling of proximal
interphalangeal joints
Figure 2 Bony enlargement of metacarpophalangeal and
proximal interphalangeal joints
Figure 3 X-ray of the hands revealing ‘swelling’ of the
metacarpophalangeal and proximal interpahalangeal joints. General
narrowing of the joint spaces; irregularity of the first metacarpop-
galangeal joint on the left
Figure 4 X-ray showing osseous enlargement of the knees with
extremely narrowed joint spaces. Sclerosing and irregularity of
joint contours are noted
A CASE OF PROGRESSIVE PSEUDORHEUMATOID ARTHROPATHY 1307
ª 2006 Blackwell Publishing Ltd Int J Clin Pract, October 2006, 60, 10, 1306–1309

deformities of fingers, reduced mobility of knees and coxofe-
moral joints and platyspondyly; severe involvement of the
joints may be disabling. Although apparently rare in western
countries with an incidence of one per million in United
Kingdom, it is probably more frequent in Middle East and
Gulf States with more than two-thirds of the reported patients
belonging to Arab and Mediterranean populations (3,4). To
our knowledge, this is the third case report of a patient with
PPAC from Turkey (5,6).
Initial mapping studies assigned the gene responsible for
the disease to the long arm of chromosome 6. However,
examination of COL10A1, which is a candidate gene in this
region, did not reveal any mutations (7,8). Using a positional
candidate approach, Hurvitz et al. (4) found homozygous
mutations in the WISP gene which also resides in 6q. WISP
is a member of CCN gene family which encodes cysteine-rich
secreted proteins with roles in cell growth and differentiation.
However, the exact mechanism of the disease is not clear at
the present.
The clinical course of the present patient is typical for the
disease. Joint involvement, characterised with painless swel-
ling of interphalangeal joints, had begun when he was 7 years
old. Although joint symptoms most commonly begin
between 3 and 8 years of age, skeletal findings may be present
even at birth (9). In this patient, severe pain, which occurred
as a relatively late symptom, affected mainly hips and the
back, and it was unresponsive to non-steroidal anti-inflamma-
tory drugs. Osteoarthritic degeneration of the coxofemoral
joints, which is revealed by intense sclerotic changes seen on
plain radiographs, may become an indication for hip replace-
ment (10). An interesting feature of the present case is the
decreased bone mineral density of the lomber vertebrae.
Because the patient did not display any clinical and laboratory
signs of other disorders associated with osteoporosis, we sug-
gest that the decreased bone density may be a direct conse-
quence of PPAC. However, the exact mechanism of this
relation is unclear at the present. On the other hand, the
increased bone mineral density of the femoral neck is
explained with the heavy osteosclerosis.
PPAC is frequently confused with JRA. There are at least
five case reports describing its striking similarity to JRA
(2,6,10–12). The main reasons of confusion appear to be
early onset at childhood, swelling and restriction of peripheral
and axial joints. However, the absence of arthritic and other
inflammatory findings, especially synovitis and radiological
absence of destructive joint changes, should alert the clinician
in excluding JRA and considering other diagnostic possibilities.
It should also be emphasised that joint swelling is osseous in
nature and is not due to synovial involvement. Furthermore, a
normal erythrocyte sedimentation rate and a normal level of
C-reactive protein may be additional clues in excluding JRA in
addition to platyspondyly, which is highly unusual for JRA.
A second diagnostic possibility to consider in the present case
could be SEDT. SEDT is an X-linked recessive disease mainly
involving the spine and hips. Recently, it has been found that
SEDT is associated with mutations in the ‘SEDL’ gene on the X
chromosome (13). Short stature with a disproportionally short
trunk, flattening of the vertebrae, short neck, pain and stiffness
of hips and osteoarhtritic degeneration of the coxofemoral
joints are main features of the syndrome. Although these are
also shared by the case under discussion, involvement of small
joints with stiffness and periarticular osseous enlargement are
not compatible with a diagnosis of SEDT.
The patient discussed here had been followed with unclear
diagnoses in other hospitals before. However, characteristic
history, bony enlargement of interpahalangeal joints, sparing
of the synovium and absence of past or present signs and
symptoms of inflammation made the diagnosis of PPAC
straightforward, and JRA was excluded easily. Also, the involve-
ment of joints other than axial skeleton and presence of
female members of the family exhibiting similar signs rule
out SEDT, which is X-linked.
We conclude that, from the practical point of view, although
PPAC is a disease which begins early in life, the diagnosis may
be delayed and should be considered in adult patients also. A
remote history of JRA should not be a reason to exclude PPAC,
because PPAC is frequently misdiagnosed as JRA.
R E F E R E N C E S
1 Online Mendelian Inheritance in Man, Omim (TM). Johns
Hopkins University, Baltimore, MD. MIM Number 208230:
8 ⁄ 27 ⁄ 1999: World Wide Web URL. http://www.ncbi.nlm.nih.
gov/omim/
Figure 5 Lateral X-ray view of the thoracal vertebrae shows
platyspondyly, narrowing and irregularity of intervertebral spaces
1308 A CASE OF PROGRESSIVE PSEUDORHEUMATOID ARTHROPATHY
ª 2006 Blackwell Publishing Ltd Int J Clin Pract, October 2006, 60, 10, 1306–1309

2 Spranger J, Albert C, Schilling F, Bartsocas C, Stoss H.
Progressive pseudorheumatoid arthritis of childhood (PPAC).
A hereditary disorder simulating rheumatoid arthritis. Eur J Pediatr
1983; 140: 34–40.
3 Alkhateeb A, al-Alami J, Leal SM, el-Shanti H, Alkbateeb A.
Fine mapping of progressive pseudorheumatoid dysplasia: a tool
for heterozygote identification. Genet Test 1999; 4: 329–33.
4 Hurvitz JR, Suwairi WM, Van Hul W et al. Mutations in the
CCN gene family member WISP3 cause progressive pseudor-
heumatoid dysplasia. Nat Genet 1999; 23: 94–8.
5 Adak B, Tekeoglu I, Sakarya ME, Ugras S. Progressive pseudo-
rheumatoid chondrodysplasia: a hereditary disorder simulating
rheumatoid arthritis. Clin Rheumatol 1998; 4: 343–5.
6 Balci S, Aypar E, Kasapcopur O, Tuysuz B, Arisoy N. An eleven-
year-old female Turkish patient with progressive pseudorheuma-
toid dysplasia mimicking juvenile idiopathic arthritis. Clin Exp
Rheumatol 2001; 19: 759.
7 el-Shanti H, Murray JC, Semina EV, Beutow KH, Scherpbier T,
al-Alami J. Assignment of gene responsible for progressive pseu-
dorheumatoid dysplasia to chromosome 6 and examination of
COL10A1 as candidate gene. Eur J Hum Genet 1998; 6: 251–6.
8 Fischer J, Urtizberea JA, Pavek S et al. Genetic linkage of
progressive pseudorheumatoid dysplasia to a 3-cM interval of
chromosome 6q22. Hum Genet 1998; 103: 60–4.
9 van Buggenhout G, De Smet L, Maroteaux P, Fryns JP.
Progressive pseudorheumatoid dysplasia: report of a patient
with symptoms present at birth. Genet Couns 1998; 9: 277–81.
10 Ehl S, Uhl M, Berner R, Bonafe L, Superti-Furga A, Kirchhoff
A. Clinical, radiographic, and genetic diagnosis of progressive pseu-
dorheumatoid dysplasia in a patient with severe polyarthropathy.
Rheumatol Int 2004; 24: 53–6.
11 Archik SG, Kamat RD. Progressive pseudorheumatoid chondro-
dysplasia simulating juvenile rheumatoid arthritis. Indian J
Pediatr 1990; 57: 785–8.
12 Mampaey S, Vanhoenacker F, Boven K, Van Hul W, De
Schepper A. Progressive pseudorheumatoid dysplasia. Eur
Radiol 2000; 10: 1832–5.
13 Gedeon AK, Colley A, Jamieson R et al. Identification of the
gene (SEDL) causing X-linked spondyloepiphyseal dysplasia
tarda. Nat Genet 1999; 22: 400–4.
Paper received April 2005, accepted July 2005
A CASE OF PROGRESSIVE PSEUDORHEUMATOID ARTHROPATHY 1309
ª 2006 Blackwell Publishing Ltd Int J Clin Pract, October 2006, 60, 10, 1306–1309
Recommended