www.elsevier.com/locate/schres
Schizophrenia Research
A neuropsychological investigation into violence and mental illness
Ian Barkatakia,*, Veena Kumaria,b, Mrigendra Dasc, Mary Hillc, Robin Morrisb,
Paul O’Connellc, Pamela Taylorc, Tonmoy Sharmad
aDepartment of Psychological Medicine, Institute of Psychiatry, London, United KingdombDepartment of Psychology, Institute of Psychiatry, London, United Kingdom
cBroadmoor Special Hospital, Crowthorne, Berkshire, United KingdomdClinical Neuroscience Research Centre, Dartford, Kent, United Kingdom
Received 26 May 2004; received in revised form 31 July 2004; accepted 1 August 2004
Available online 11 September 2004
Abstract
Previous research has reported cognitive impairment in patients with schizophrenia and antisocial personality disorder
(APD), the two psychiatric illnesses most implicated in violent behaviour. Previous studies have focused on either group
exclusively, and have been criticized for procedural inadequacies and sample heterogeneity. The authors investigated and
compared neuropsychological profiles of individuals with APD and violent and nonviolent individuals with schizophrenia in a
single investigation. The study involved four groups of subjects: (i) individuals with a history of serious violence and a
diagnosis of APD, (ii) individuals with a history of violence and schizophrenia, (iii) individuals with schizophrenia without a
history of violent behaviour and (iv) healthy control subjects. All study groups were compared on a neuropsychological battery
designed to assess general intellectual function, executive function, attention, and processing speed. Cognitive deficits were
more widespread among individuals with schizophrenia regardless of history of violence, compared with those with APD.
Significant impairment in patients with APD was limited to processing speed. Violent individuals with schizophrenia
demonstrated poorer performance than their nonviolent schizophrenia peers on a measure of executive function. Different
cognitive impairments are manifested by individuals with APD and schizophrenia with violent behaviours, suggesting
differences in underlying pathology. Furthermore, cognitive impairment appears to be more a feature of schizophrenia than of
violent behaviour, although there is evidence that a combination of schizophrenia and violent behaviour is associated with
greater cognitive deficits.
D 2004 Elsevier B.V. All rights reserved.
Keywords: Violence; Aggression; Antisocial personality disorder; Schizophrenia; Neuropsychology
0920-9964/$ - see front matter D 2004 Elsevier B.V. All rights reserved.
doi:10.1016/j.schres.2004.08.001
* Corresponding author. PO58, Section of Cognitive Pharma-
cology, Division of Psychological Medicine, Institute of Psychiatry,
De Crespigny Park, Demark Hill, London SE5 8AF, United
Kingdom. Tel.: +44 207 848 0702; fax: +44 207 848 0646.
E-mail address: [email protected] (I. Barkataki).
1. Introduction
There is an undoubted significant if small associ-
ation between psychosis and violent behaviour
74 (2005) 1–13

I. Barkataki et al. / Schizophrenia Research 74 (2005) 1–132
(Angermeyer, 2000; Tiihonen et al., 1997). The
relationship between personality disorder and violence
is much less clear, because of confounding between
measures of personality and of antisocial behaviour,
but personality disorders are heavily over-represented
in prison populations, even if antisocial personality
disorder (APD) per se is excluded (Fazel and Danesh,
2002). Furthermore, among people who have commit-
ted the most serious violence, many are co-morbid for
psychosis and/or personality disorder and the two
disorders most frequently implicated in violent behav-
iour are APD and schizophrenia (Taylor et al., 1998).
Neurobiological studies have suggested that certain
structural neural abnormalities are associated with
violent behaviour in mentally ill patients (Chesterman
et al., 1994). The two neural regions that have been
consistently cited in relation to violent behaviour in
both APD and schizophrenia in neuroimaging studies
are the prefrontal cortex and the limbic system (Das et
al., 2002). The prefrontal cortex (PFC) mediates
executive function and social conduct, in addition to
exerting an inhibitory influence on certain behaviours,
such as aggression (Damasio, 1995). Furthermore,
neuroimaging studies examining this region have
reported structural abnormalities in both schizophre-
nia (Buchanan et al., 1998) and APD samples (Raine
et al., 2000). The other implicated region is the limbic
system, an area involved in the processing of external
emotional stimuli and relaying it into emotional
response (Aggleton, 1992), and studies have demon-
strated abnormal limbic structure and function in both
schizophrenia (Chesterman et al., 1994) and APD
(Laakso et al., 2001). At the neurobiological level,
increases in violent behaviour has been linked with
reductions in serotonin (Soderstrom et al., 2001;
Volavka, 1999), reductions in dopamine (Berman
and Coccaro, 1998) as well as increases in testoster-
one (Book et al., 2001). Substance abuse is also
widely reported to exacerbate violent behaviour
(Reiss et al., 1994; Bushman and Cooper, 1990), via
its influence and interaction with neurochemical
agents such as serotonin (Virkkunen and Linnoila,
1993) and GABA (Miczek et al., 1997).
Neuropsychological studies examining cognitive
functioning in violent groups have supported neuro-
biological findings. Numerous reviews of antisocial
behaviour and neuropsychological function have
frequently cited the causal relationship between neural
dysfunction and violence (reviews: Brower and Price,
2001; Morgan and Lilienfeld, 2000; Golden et al.,
1996; Yeudall, 1977). These studies have generally
reflected the cognitive deficits that can be representa-
tive of certain types of neuropathology such as
executive function deficits reflecting PFC impairment,
but Jones (1992) proposed multiple neuropsychopa-
thological factors contributing to violent behaviour
including reduced inhibition, as well as impairment in
memory, attention and concentration.
Neuropsychological assessments of schizophrenia
populations have demonstrated deficits in a wide
range of cognitive domains including impairments in
attention, cognitive processing speed and IQ (reviews:
Sharma and Antonova, 2003; Goldberg and Gold,
1995). Schizophrenia has been linked to poor per-
formance on several aspects of executive functioning
using tests of working memory (Pantelis et al., 1997),
inhibition (Perlstein et al., 1998), and strategy
formation and planning (Morris et al., 1995). Within
the schizophrenia population, those with violent
histories are found to demonstrate impaired perform-
ance than those without a violent history on the
Wechsler Adult Intelligence Scale (WAIS) (Krakow-
ski et al., 1989) and Luria–Nebraska tests (Adams et
al., 1990). One study that directly compared non-
aggressive and aggressive (co-morbid APD) schizo-
phrenia groups (Rasmussen et al., 1995) reported the
aggressive group to perform poorly than the non-
aggressive group on tasks of frontal functioning with
the reverse being true for reaction time tasks.
Unlike schizophrenia, investigations of APD and
psychopathy (a closely related condition) do not show
significant differences in general intellectual perform-
ance in comparison to healthy groups (Walsh, 1991;
Miller, 1987; Prentice and Kelly, 1963). However,
these groups still exhibit deficits in executive function
across a range of tasks especially on those indexing
response inhibition and cognitive flexibility (Dolan
and Park, 2002; Morgan and Lilienfeld, 2000;
Lapierre et al., 1995; Devonshire et al., 1988;
Gorenstein, 1982). Furthermore, performance on tests
of impulsivity and emotional response have been cited
as particularly impaired in APD (Dinn and Harris,
2000; Lapierre et al., 1995). Overall, the literature
consistently reports that APD groups display PFC-
related deficits in executive function, inhibitory
control and emotional recognition. However, these

I. Barkataki et al. / Schizophrenia Research 74 (2005) 1–13 3
findings are controversial, as other studies have been
unable to find deficits on putatively PFC tasks
(Crowell et al., 2003; Hare, 1984) or have reported
deficits in some tasks but not others (Dinn and Harris,
2000). Published neuropsychological investigations of
APD and schizophrenia with violence have, however,
focused exclusively on either group, and there are as
yet no direct comparisons.
The current study compares neuropsychological
performance in individuals with APD and a history of
severe violence, those with schizophrenia who had
been similarly violent, non-violent individuals with
schizophrenia, and healthy control subjects, character-
izing the cognitive impairments associated with
violence in patients with these mental disorders. The
principal hypotheses were: (i) relative to the healthy
control subjects, subjects in all clinical groups will
show impaired neuropsychological performance; (ii)
individuals with APD will demonstrate impairment on
executive function and speed of processing tasks
(related to dorsolateral prefrontal cortex function) but
will not display deficits on tasks of attention and
general intellectual functioning; (iii) the non-violent
individuals with schizophrenia will show impairment
in processing speed, attention and general intellectual
functioning, in addition to executive functioning; (iv)
individuals with schizophrenia who have also been
violent will display a greater range and magnitude of
deficits than any other groups on cognitive measures,
especially in executive functioning.
2. Methods
2.1. Subjects
Initially, 64 participants were recruited into the
study, but 6 were excluded due to withdrawal of
consent or nonparticipation. The final sample con-
sisted of incarcerated patients with a history of
violence diagnosed with APD (APD: n=14) or
schizophrenia (VS: n=13), schizophrenia patients
without violent history (NVS: n=15) and healthy
control subjects (n=15). The violent patient samples
were recruited from Broadmoor Special Hospital and
the Denis Hill unit of the Bethlem Royal Hospital.
The NVS group was recruited from South London and
Maudsley Trust Hospitals, London and control sub-
jects were recruited from general public advertise-
ments in the South London Press.
Inclusion into the study required all subjects to be
male, right handed, between 18 and 45 years of age,
speak English as their first language, be free of current
substance abuse (tested by urine analysis), and have
no history of neurological conditions or head injury.
Entry to the APD group required a DSM-IV diagnosis
of antisocial personality disorder, no co-morbid
diagnosis of schizophrenia and a history of violent
behaviour that would score 4 for seriousness of
offence on the Gunn and Robertson Scale for
violence, indicative of a fatal or near fatal act of
violence against another (Gunn and Robertson, 1976).
Both VS and NVS were required to fulfill the DSM-
IV criteria for schizophrenia and could not have co-
morbid diagnosis of APD. The VS group also had to
show similar violent history as described for the APD
group while the NVS group was required to have no
significant history of violence. In addition to the
overall inclusion criteria, the control group had to
have no previous psychiatric diagnoses without any
significant history of violence.
Groups were matched according to age, ethnicity
and socio-economic background. Subjects were also
matched for number of years in education, which seems
to have resulted in comparable levels of estimated
verbal IQ as measured by the National Adult Reading
Test (Nelson and Willison, 1991). Duration of incar-
ceration was also matched for APD and VS groups.
Medication information at study entry was recorded
and neuroleptic dosage was converted into chlorpro-
mazine dosage equivalents where applicable (Table 1).
For certain tasks, the total sample number is reduced
due to equipment failure or nonparticipation and these
instances are stated in Table 2. All participants
provided written informed consent. The protocol for
this study was approved by the ethics committees of the
Institute of Psychiatry and Maudsley Hospital, London
and Broadmoor Hospital Berkshire.
2.2. Clinical ratings
Diagnoses for violent groups were based on
classification by respective treating consultants at
secure units, using the Structured Clinical Interview
for DSM-IVAxis I disorder (SCID, First et al., 1995)
for the VS group, and the Structured Clinical Inter-
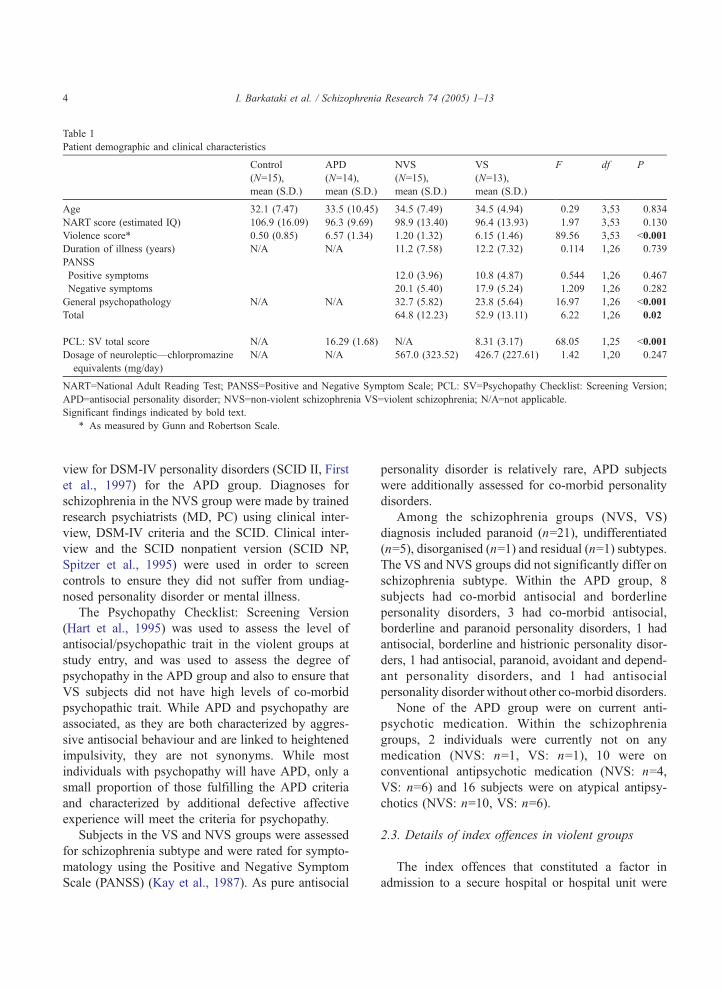
Table 1
Patient demographic and clinical characteristics
Control
(N=15),
mean (S.D.)
APD
(N=14),
mean (S.D.)
NVS
(N=15),
mean (S.D.)
VS
(N=13),
mean (S.D.)
F df P
Age 32.1 (7.47) 33.5 (10.45) 34.5 (7.49) 34.5 (4.94) 0.29 3,53 0.834
NART score (estimated IQ) 106.9 (16.09) 96.3 (9.69) 98.9 (13.40) 96.4 (13.93) 1.97 3,53 0.130
Violence score* 0.50 (0.85) 6.57 (1.34) 1.20 (1.32) 6.15 (1.46) 89.56 3,53 b0.001
Duration of illness (years) N/A N/A 11.2 (7.58) 12.2 (7.32) 0.114 1,26 0.739
PANSS
Positive symptoms 12.0 (3.96) 10.8 (4.87) 0.544 1,26 0.467
Negative symptoms 20.1 (5.40) 17.9 (5.24) 1.209 1,26 0.282
General psychopathology N/A N/A 32.7 (5.82) 23.8 (5.64) 16.97 1,26 b0.001
Total 64.8 (12.23) 52.9 (13.11) 6.22 1,26 0.02
PCL: SV total score N/A 16.29 (1.68) N/A 8.31 (3.17) 68.05 1,25 b0.001
Dosage of neuroleptic—chlorpromazine
equivalents (mg/day)
N/A N/A 567.0 (323.52) 426.7 (227.61) 1.42 1,20 0.247
NART=National Adult Reading Test; PANSS=Positive and Negative Symptom Scale; PCL: SV=Psychopathy Checklist: Screening Version;
APD=antisocial personality disorder; NVS=non-violent schizophrenia VS=violent schizophrenia; N/A=not applicable.
Significant findings indicated by bold text.
* As measured by Gunn and Robertson Scale.
I. Barkataki et al. / Schizophrenia Research 74 (2005) 1–134
view for DSM-IV personality disorders (SCID II, First
et al., 1997) for the APD group. Diagnoses for
schizophrenia in the NVS group were made by trained
research psychiatrists (MD, PC) using clinical inter-
view, DSM-IV criteria and the SCID. Clinical inter-
view and the SCID nonpatient version (SCID NP,
Spitzer et al., 1995) were used in order to screen
controls to ensure they did not suffer from undiag-
nosed personality disorder or mental illness.
The Psychopathy Checklist: Screening Version
(Hart et al., 1995) was used to assess the level of
antisocial/psychopathic trait in the violent groups at
study entry, and was used to assess the degree of
psychopathy in the APD group and also to ensure that
VS subjects did not have high levels of co-morbid
psychopathic trait. While APD and psychopathy are
associated, as they are both characterized by aggres-
sive antisocial behaviour and are linked to heightened
impulsivity, they are not synonyms. While most
individuals with psychopathy will have APD, only a
small proportion of those fulfilling the APD criteria
and characterized by additional defective affective
experience will meet the criteria for psychopathy.
Subjects in the VS and NVS groups were assessed
for schizophrenia subtype and were rated for sympto-
matology using the Positive and Negative Symptom
Scale (PANSS) (Kay et al., 1987). As pure antisocial
personality disorder is relatively rare, APD subjects
were additionally assessed for co-morbid personality
disorders.
Among the schizophrenia groups (NVS, VS)
diagnosis included paranoid (n=21), undifferentiated
(n=5), disorganised (n=1) and residual (n=1) subtypes.
The VS and NVS groups did not significantly differ on
schizophrenia subtype. Within the APD group, 8
subjects had co-morbid antisocial and borderline
personality disorders, 3 had co-morbid antisocial,
borderline and paranoid personality disorders, 1 had
antisocial, borderline and histrionic personality disor-
ders, 1 had antisocial, paranoid, avoidant and depend-
ant personality disorders, and 1 had antisocial
personality disorder without other co-morbid disorders.
None of the APD group were on current anti-
psychotic medication. Within the schizophrenia
groups, 2 individuals were currently not on any
medication (NVS: n=1, VS: n=1), 10 were on
conventional antipsychotic medication (NVS: n=4,
VS: n=6) and 16 subjects were on atypical antipsy-
chotics (NVS: n=10, VS: n=6).
2.3. Details of index offences in violent groups
The index offences that constituted a factor in
admission to a secure hospital or hospital unit were
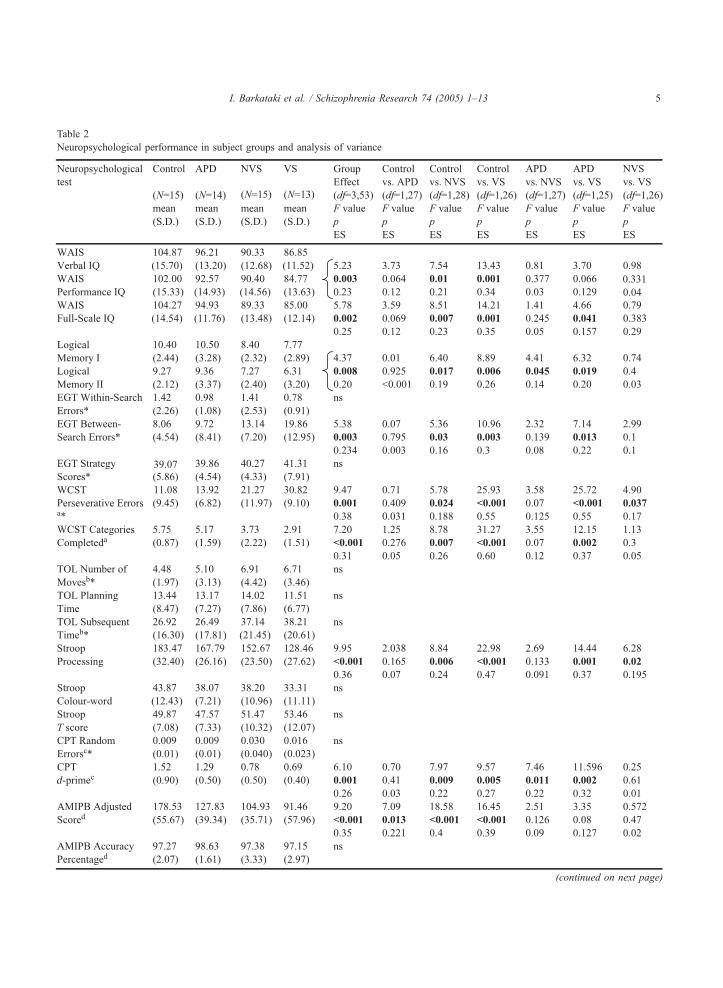
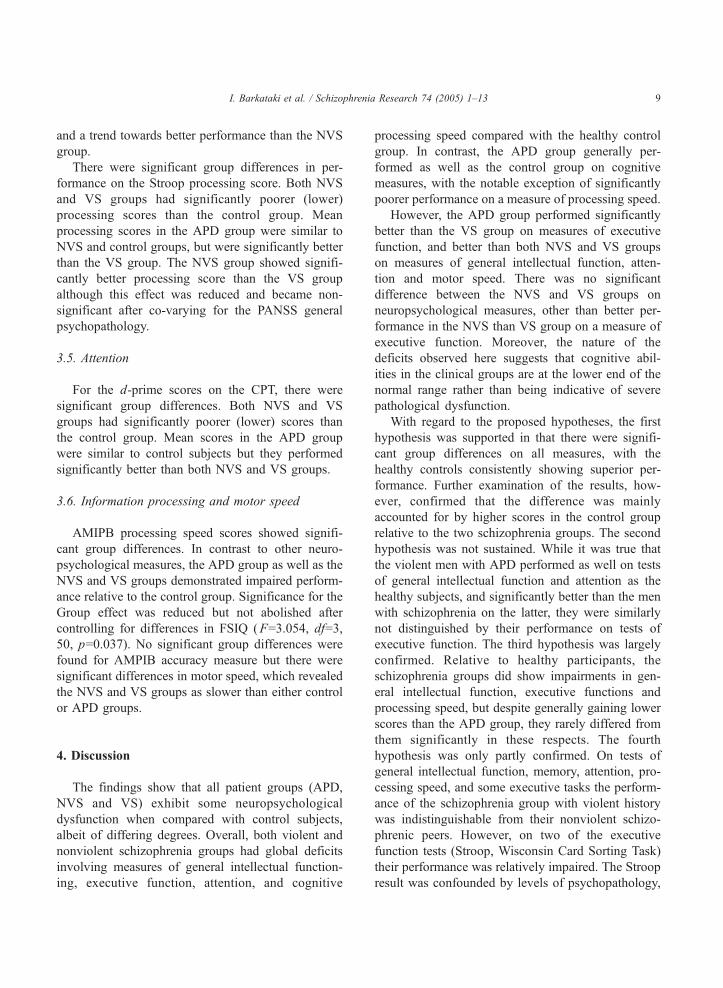
able 2
europsychological performance in subject groups and analysis of variance
(continued on next page)
I. Barkataki et al. / Schizophrenia Research 74 (2005) 1–13 5
T
N
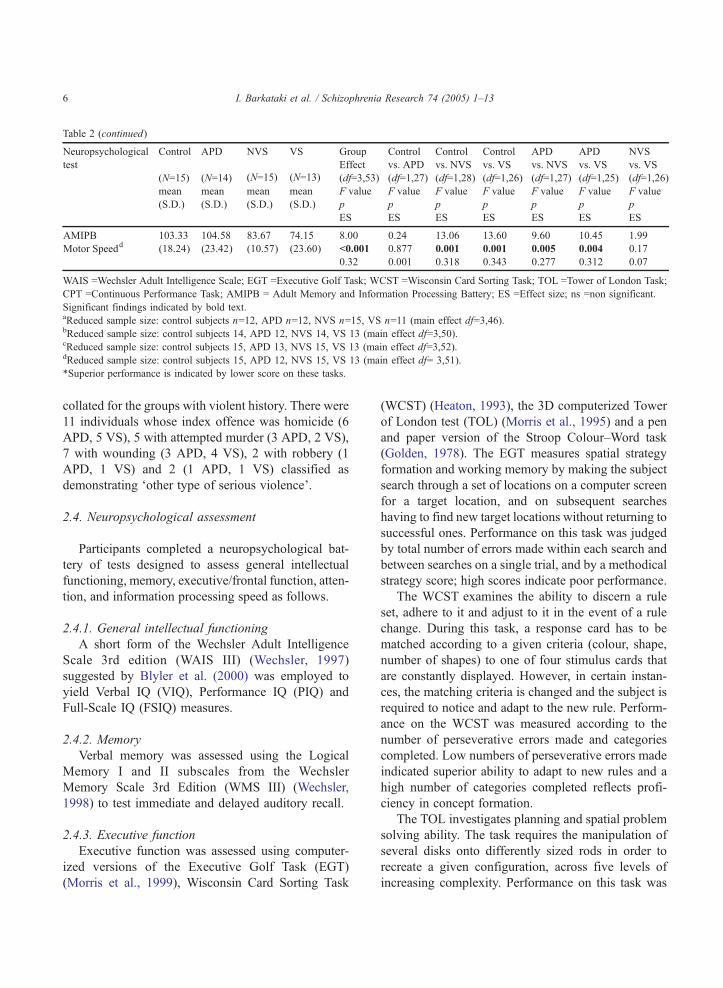
WAIS =Wechsler Adult Intelligence Scale; EGT =Executive Golf Task; WCST =Wisconsin Card Sorting Task; TOL =Tower of London Task;
CPT =Continuous Performance Task; AMIPB = Adult Memory and Information Processing Battery; ES =Effect size; ns =non significant.
Significant findings indicated by bold text.aReduced sample size: control subjects n=12, APD n=12, NVS n=15, VS n=11 (main effect df=3,46).bReduced sample size: control subjects 14, APD 12, NVS 14, VS 13 (main effect df=3,50).cReduced sample size: control subjects 15, APD 13, NVS 15, VS 13 (main effect df=3,52).dReduced sample size: control subjects 15, APD 12, NVS 15, VS 13 (main effect df= 3,51).
*Superior performance is indicated by lower score on these tasks.
Table 2 (continued)
I. Barkataki et al. / Schizophrenia Research 74 (2005) 1–136
collated for the groups with violent history. There were
11 individuals whose index offence was homicide (6
APD, 5 VS), 5 with attempted murder (3 APD, 2 VS),
7 with wounding (3 APD, 4 VS), 2 with robbery (1
APD, 1 VS) and 2 (1 APD, 1 VS) classified as
demonstrating dother type of serious violenceT.
2.4. Neuropsychological assessment
Participants completed a neuropsychological bat-
tery of tests designed to assess general intellectual
functioning, memory, executive/frontal function, atten-
tion, and information processing speed as follows.
2.4.1. General intellectual functioning
A short form of the Wechsler Adult Intelligence
Scale 3rd edition (WAIS III) (Wechsler, 1997)
suggested by Blyler et al. (2000) was employed to
yield Verbal IQ (VIQ), Performance IQ (PIQ) and
Full-Scale IQ (FSIQ) measures.
2.4.2. Memory
Verbal memory was assessed using the Logical
Memory I and II subscales from the Wechsler
Memory Scale 3rd Edition (WMS III) (Wechsler,
1998) to test immediate and delayed auditory recall.
2.4.3. Executive function
Executive function was assessed using computer-
ized versions of the Executive Golf Task (EGT)
(Morris et al., 1999), Wisconsin Card Sorting Task
(WCST) (Heaton, 1993), the 3D computerized Tower
of London test (TOL) (Morris et al., 1995) and a pen
and paper version of the Stroop Colour–Word task
(Golden, 1978). The EGT measures spatial strategy
formation and working memory by making the subject
search through a set of locations on a computer screen
for a target location, and on subsequent searches
having to find new target locations without returning to
successful ones. Performance on this task was judged
by total number of errors made within each search and
between searches on a single trial, and by a methodical
strategy score; high scores indicate poor performance.
The WCST examines the ability to discern a rule
set, adhere to it and adjust to it in the event of a rule
change. During this task, a response card has to be
matched according to a given criteria (colour, shape,
number of shapes) to one of four stimulus cards that
are constantly displayed. However, in certain instan-
ces, the matching criteria is changed and the subject is
required to notice and adapt to the new rule. Perform-
ance on the WCST was measured according to the
number of perseverative errors made and categories
completed. Low numbers of perseverative errors made
indicated superior ability to adapt to new rules and a
high number of categories completed reflects profi-
ciency in concept formation.
The TOL investigates planning and spatial problem
solving ability. The task requires the manipulation of
several disks onto differently sized rods in order to
recreate a given configuration, across five levels of
increasing complexity. Performance on this task was

I. Barkataki et al. / Schizophrenia Research 74 (2005) 1–13 7
assessed on total number of moves above the possible
minimum taken to complete the task, with low number
of moves indicative of efficiency at problem solving.
Planning time taken between the start of the task and
the manipulation of the first disk and time taken for
subsequent execution of the task were also measured,
with quicker times signifying better performance.
The Stroop Colour–Word task tests the capacity to
suppress prepotent responses to stimuli as a measure
of inhibition. The task consists of three lists: a word
list of words in black ink that describe colour, a colour
list of differently coloured inks, and a colour–word list
of words describing colours, which is printed in a
colour of ink different to that colour described by the
word. Subjects are scored by the number of words
successfully read out in the last of these conditions. In
this task, high colour–word and T scores indicate
superior inhibitory ability, and high scores in the
colour list and word list (both combined into an
overall processing score) are indicative of better
processing speed.
2.4.4. Attention
The Continuous Performance Task—Identical
Pairs variant (CPT) (Cornblatt et al., 1988) was
used to gauge attention. In this computerized task,
subjects had to respond to identical consecutive four-
digit numbers by using a mouse to respond, while
ignoring nonconsecutive stimuli. Performance was
measured as the number of random errors commis-
sioned and by d-prime, a measure of vigilance
determined by how well an individual discriminates
Fig. 1. Order of neuropsycholog
between target and nontarget stimuli. Higher scores
indicate better performance.
2.4.5. Processing speed
Processing speed was measured by the informa-
tion processing subtests of the Adult Memory and
Information Processing Battery (AMIPB) (Coughlan
and Hollows, 1985). These are critically timed
number cancellation tasks which provide measures
of motor speed, of cognitive processing speed, and
processing accuracy. Processing speed was calculated
as the average of the adjusted scores derived from a
conversion table (Coughlan and Hollows, 1985),
which takes into account the total number of items
correctly cancelled within the time limit, and
performance on the motor speed task for both tasks.
Accuracy was calculated from the mean percentage
of correctly cancelled items on both scales. Motor
speed performance was assessed by the number of
cancelled items within a given time limit on a
separate noncognitive task.
Order of presentation of tests is given in Fig. 1.
The battery took approximately 2 h to administer
with a break given half way through (between tasks
5 and 6).
2.5. Statistical analysis
For categorical demographic data, chi-square tests
were used to analyze between group differences. One-
way analysis of variance (ANOVA) was used for all
other demographic and clinical variables.
ical battery administration.

I. Barkataki et al. / Schizophrenia Research 74 (2005) 1–138
The scores on Performance and Verbal IQ were
subjected to a 4 (Group: control subjects, APD,
NVS, VS)�2 (Measure: PIQ, VIQ) mixed-model
ANOVA. The scores on Logical Memory scales
were examined using a 4 (Group)�2 (Measure:
Logical Memory I score, Logical Memory II score)
mixed-model ANOVA. For both comparisons,
dGroupT was the between-subjects factor and
dMeasureT was the within-subjects factor. All other
cognitive tests were analyzed with a one-way
ANOVA with the score as the dependant variable
and Group as the independent factor. For significant
group effects, follow-up analysis of comparisons
between individual group pairs was conducted using
lower-order ANOVA with the two appropriate
groups as the between-subjects factor. For mixed-
model ANOVA, the Greenhouse–Geisser correction
was applied where appropriate.
Given the difference in symptoms between the
NVS and VS groups (see Table 1), any cognitive
variables differentiating these two groups were re-
evaluated using analyses of co-variance with the
PANSS general psychopathology scores as a cova-
riate. Any measure showing impaired performance in
all three APD, NVS, and VS groups relative to
healthy subjects was re-evaluated after co-varying for
Full-Scale IQ to estimate the variance it might share
with the general intellectual functioning. Statistical
analysis was conducted using SPSS v.10 with level of
significance maintained at p=0.05 unless specified
otherwise.
3. Results
3.1. Demographic and clinical variables
There were no significant differences between
groups on demographic variables (Table 1). Charac-
teristic variables that defined groups (i.e. PCL score
and violence rating) differed as did PANSS General
psychopathology score.
3.2. General intellectual functioning
Means and standard deviations for all neuro-
psychological variables, classified by subject groups,
and ANOVAs are presented in Table 2.
For PIQ and VIQ scores, there were statistically
significant group differences. PIQ/VIQ scores were
significantly lower in the NVS and VS groups than in
healthy participants. The APD group displayed a trend
for lower scores than the control group, but had higher
scores than the VS group. Examination of FSIQ
revealed significant group differences as both NVS
and VS groups showed significantly lower mean
FSIQ compared to the healthy participants. Moreover,
the APD group exhibited a trend towards having a
lower FSIQ than the control group. Although mean
FSIQ scores in the APD were not significantly
different from the NVS group, they were significantly
higher than those of the VS group.
3.3. Memory
For the scores on the Logical Memory I and II
scales, there were significant group differences. The
NVS and VS groups performed worse than the control
group. The APD group did not differ from control
group but performed significantly better than NVS
and VS subjects. In general, all groups had higher
immediate memory relative to delayed memory scores
(F=21.22, df=1,53, pb0.001), but no Group� Meas-
ure interaction was found.
3.4. Executive functioning
On the EGT task, there were no significant group
differences for within-search errors or for strategy score
but there were significant group differences in the
between-search error scores. The NVS and VS subjects
made significantly more between-search errors than
control subjects. The APD group made fewer between-
search errors than the VS groups but did not signifi-
cantly differ from NVS or healthy participants.
WCST scores also showed significant group differ-
ences. Both the NVS and VS groups made more
perseverative errors than the control group. The VS
and NVS groups also made more errors than APD
subjects. The difference between NVS and VS groups
was not diminished when PANSS general psychopa-
thology scores was co-varied for (F=5.119, df=1, 23,
p=0.033). For the WCST number of categories
completed, both NVS and VS groups performed worse
than the control group. The APD group showed
significantly better performance than the VS group
I. Barkataki et al. / Schizophrenia Research 74 (2005) 1–13 9
and a trend towards better performance than the NVS
group.
There were significant group differences in per-
formance on the Stroop processing score. Both NVS
and VS groups had significantly poorer (lower)
processing scores than the control group. Mean
processing scores in the APD group were similar to
NVS and control groups, but were significantly better
than the VS group. The NVS group showed signifi-
cantly better processing score than the VS group
although this effect was reduced and became non-
significant after co-varying for the PANSS general
psychopathology.
3.5. Attention
For the d-prime scores on the CPT, there were
significant group differences. Both NVS and VS
groups had significantly poorer (lower) scores than
the control group. Mean scores in the APD group
were similar to control subjects but they performed
significantly better than both NVS and VS groups.
3.6. Information processing and motor speed
AMIPB processing speed scores showed signifi-
cant group differences. In contrast to other neuro-
psychological measures, the APD group as well as the
NVS and VS groups demonstrated impaired perform-
ance relative to the control group. Significance for the
Group effect was reduced but not abolished after
controlling for differences in FSIQ (F=3.054, df=3,
50, p=0.037). No significant group differences were
found for AMPIB accuracy measure but there were
significant differences in motor speed, which revealed
the NVS and VS groups as slower than either control
or APD groups.
4. Discussion
The findings show that all patient groups (APD,
NVS and VS) exhibit some neuropsychological
dysfunction when compared with control subjects,
albeit of differing degrees. Overall, both violent and
nonviolent schizophrenia groups had global deficits
involving measures of general intellectual function-
ing, executive function, attention, and cognitive
processing speed compared with the healthy control
group. In contrast, the APD group generally per-
formed as well as the control group on cognitive
measures, with the notable exception of significantly
poorer performance on a measure of processing speed.
However, the APD group performed significantly
better than the VS group on measures of executive
function, and better than both NVS and VS groups
on measures of general intellectual function, atten-
tion and motor speed. There was no significant
difference between the NVS and VS groups on
neuropsychological measures, other than better per-
formance in the NVS than VS group on a measure of
executive function. Moreover, the nature of the
deficits observed here suggests that cognitive abil-
ities in the clinical groups are at the lower end of the
normal range rather than being indicative of severe
pathological dysfunction.
With regard to the proposed hypotheses, the first
hypothesis was supported in that there were signifi-
cant group differences on all measures, with the
healthy controls consistently showing superior per-
formance. Further examination of the results, how-
ever, confirmed that the difference was mainly
accounted for by higher scores in the control group
relative to the two schizophrenia groups. The second
hypothesis was not sustained. While it was true that
the violent men with APD performed as well on tests
of general intellectual function and attention as the
healthy subjects, and significantly better than the men
with schizophrenia on the latter, they were similarly
not distinguished by their performance on tests of
executive function. The third hypothesis was largely
confirmed. Relative to healthy participants, the
schizophrenia groups did show impairments in gen-
eral intellectual function, executive functions and
processing speed, but despite generally gaining lower
scores than the APD group, they rarely differed from
them significantly in these respects. The fourth
hypothesis was only partly confirmed. On tests of
general intellectual function, memory, attention, pro-
cessing speed, and some executive tasks the perform-
ance of the schizophrenia group with violent history
was indistinguishable from their nonviolent schizo-
phrenic peers. However, on two of the executive
function tests (Stroop, Wisconsin Card Sorting Task)
their performance was relatively impaired. The Stroop
result was confounded by levels of psychopathology,

I. Barkataki et al. / Schizophrenia Research 74 (2005) 1–1310
but the error rate on the Wisconsin Card Sorting Task
was independent of the PANNS general psychopa-
thology score.
Contrary to the expectations, the APD group did
not show deficits in executive function compared to
control subjects or patients with nonviolent schizo-
phrenia, but did show impairment in processing
speed. The lack of observable significant impairment
in executive function does not support the theory that
dysfunction of the dorsolateral prefrontal cortex is a
core component of APD (Chesterman et al., 1994;
Das et al., 2002; Raine et al., 2000), and lends support
to the studies reporting executive functioning parity
between APD and healthy individuals (Crowell et al.,
2003; Hare, 1984). These studies advocate attribution
of antisocial behaviour in APD to emotional or
socialization factors rather than straightforward com-
promise of executive function, and suggest that
prefrontal cortical dysfunction can serve to facilitate
aggression and violence in APD, but is not an
essential prerequisite.
Interestingly, the novel finding of reduced process-
ing speed in individuals with APD in this study
suggests that the impulsive and risk-taking character-
istics of APD may be related to failure to appropri-
ately process data indicating the presence of danger in
adequate time. This deficit may also be responsible for
the irresponsibility and failure in foresight that are
characteristic of individuals with APD, as the inad-
equate processing of data may result in the individual
in making maladaptive decisions (inability to bthink it
through properlyQ), especially in scenarios where
thinking time available is brief (e.g. within confronta-
tional situations). There is also the possibility of a
specificity of effect to this particular type of task, as
performance on planning time within the TOL did not
differentiate between control and APD subjects.
Currently, there are no investigations focusing on
processing speed in APD, and the issue of processing
speed impairment being specifically related to APD
requires further research.
Deficits in information processing speed have
traditionally been associated with multiple sclerosis
(Rao, 1995), but studies of Parkinson’s disease
(Grossman et al., 2002) and head injury (Schmitter-
Edgecombe et al., 1992) have also found impairments
in this domain. Information processing in such
instances could consist of a sequence, which begins
with sensory input and ends with motor output. It can
be subdivided into three main components: automatic
processing (involuntary recognition of sensory input),
controlled processing (the conscious manipulation of
information) and motor programming (Vlaar and
Wade, 2003). As the APD group did not differ on
the motor speed component of the task, and they also
did not show deficits in the recognition aspects of
other tasks (see Results), it could be speculated that
this particular deficit was localised to the controlled
processing component. Contemporary research into
neural correlates of information processing speed
related to white matter (Posthuma et al., 2003) and
frontal lobe volumes (Schretlen et al., 2000), the latter
of which has previously been implicated in APD
function.
Information processing speed is just one of several
possible measures of impulsivity, and other neuro-
biological studies examining antisocial populations
have reported similar deficits in impulsivity using
different methods. There have been reports of
increased rate of error during motor inhibition tasks
in psychopathic (Lapierre et al., 1995) and APD
subjects (Dolan and Park, 2002) when compared to
normal controls, which has been attributed to increased
impulsivity characteristic of the disorders. Further-
more, a recent functional neuroimaging study examin-
ing impulsivity using a similar motor inhibition task
(Vollm et al., 2004) demonstrated PFC activation
during inhibition in controls and a displacement of
activation to the medial superior gyrus and anterior
cingulate in personality disordered subjects (including
APD), suggesting that impulsivity may be related to
PFC dysfunction and the use of alternative neural
pathways to deal with inhibitory demands. It has been
theorized that poor impulse control in APD is due to
impairment in the PFC (Horn et al., 2003) based on the
observations of reduced metabolism and grey matter
volume in this region (Raine et al., 1997, 2000).
The performance in the schizophrenia groups
demonstrated here supports prior findings of the
presence of widespread deficiencies in cognitive
function. In addition, a greater degree of impairment
was observed in violent compared to nonviolent
schizophrenia patients. This finding confirms certain
earlier findings of violent groups with schizophrenia
displaying impaired performance compared to non-
violent groups (Adams et al., 1990; Krakowski et al.,

I. Barkataki et al. / Schizophrenia Research 74 (2005) 1–13 11
1989). However, this impairment may only be
prevalent when the violent group with schizophrenia
does not have co-morbid psychopathy (as in the
current study), as there has been some indication that
the presence of a personality disorder of the antisocial
type may have a protective factor against certain
neuropsychological deficits normally found in schiz-
ophrenia (Rasmussen et al., 1995). Overall, these
results corroborate published reports of cognitive
deficits in intellectual function (Allen et al., 1998),
executive function (Adams et al., 1990; Bustini et al.,
1999), attention (Mirsky, 1988; Franke et al., 1994)
and cognitive processing (Perlstein et al., 1998) in
patients with schizophrenia. In addition, the findings
suggest that moderate cognitive impairment in schiz-
ophrenia is present regardless of the presence or
absence of violent behaviours, and the poor perform-
ance in executive function tasks implies the existence
of prefrontal cortex dysfunction.
Despite attempting to account for external factors
and potential confounding variables, this study has
some limitations. Although the violent mentally ill
sample in the current study is large compared to other
published research, we encountered a high attrition
rate in terms of total sample size as well as within
individual tests, and as a result the sample was
relatively small. The reasons for dropouts were
withdrawal of consent and noncooperation, as well
as logistic and circumstantial issues. The number of
subjects dropping out of the study was, however,
evenly distributed across the four study groups with
no apparent difference between those who dropped
out and those who remained in the study on the
demographic and estimated IQ variables.
Other limitations, with some potential for con-
founding in our results, include the use of APD
subjects with other co-morbid personality disorders,
the use of schizophrenia subjects with various
subtypes and symptoms and the possibility of
previous substance abuse in all groups. Finally, due
to the array of neuropsychological tasks and four
study groups investigated in this study, it was
necessary to perform many statistical comparisons,
which would normally necessitate a correction to the
alpha value to reduce potential type-one error.
However, we felt it would be more appropriate to
maintain the conventional level of significance in
order to examine the subtle but meaningful differences
between groups and report the effect sizes pertaining
to our proposed hypotheses.
In conclusion, this study demonstrated some level
of dysfunction in all three pathological groups.
Individuals with APD displayed marginal impairment
in cognitive processing speed, but not in executive
function, suggesting that an alternate hypothesis of the
pathogenesis of behaviors characteristic of these
patients is needed. Widespread cognitive deficits are
present in patients with schizophrenia both with and
without a history of violence, but deficits in executive
function are more pronounced in violent than non-
violent patients. These findings suggest that violence
in patients with schizophrenia and APD is linked to
different aspects of impaired neuropsychological
function. There is a need for additional research to
elucidate the factors and impairments that facilitate
violence in individuals with mental illness.
Acknowledgements
This study was funded by grants from The Zito
Trust and the Community Fund, UK, and the Stanley
Medical Research Institute, USA. Veena Kumari
holds a Wellcome Trust Senior Research Fellowship
in Basic Biomedical Science. We express our appre-
ciation to the staff of Broadmoor Special Hospital and
the Denis Hill Unit of the Royal Bethlem Hospital,
and to Ms. Catherine Hughes for assistance with this
study.
References
Adams, J.J., Meloy, J.R., Moritz, M.S., 1990. Neuropsychological
deficits and violent behavior in incarcerated schizophrenics. J. of
Nerv. Ment. Dis. 178, 253–256.
Aggleton, J., 1992. The Amygdala. Neurobiological Aspects of
Emotion, Memory and Mental Dysfunction. Wiley-Liss,
New York.
Allen, D.N., Huegel, S.G., Seaton, B.E., Goldstein, G., Gurklis Jr.,
J.A., van Kammen, D.P., 1998. Confirmatory factor analysis of
the WAIS-R in patients with schizophrenia. Schizophr. Res. 34,
87–94.
Angermeyer, M.C., 2000. Schizophrenia and violence. Acta
Psychiatr. Scand., Suppl. 102, 63–67.
Berman, M.E., Coccaro, E.F., 1998. Neurobiologic correlates of
violence: relevance to criminal responsibility. Behav. Sci. Law
16, 303–318.
I. Barkataki et al. / Schizophrenia Research 74 (2005) 1–1312
Blyler, C.R., Gold, J.M., Iannone, V.N., Buchanan, R.W., 2000.
Short form of the WAIS-III for use with patients with
schizophrenia. Schizophr. Res. 46, 209–215.
Book, A.S., Starzyk, K.B., Quinsey, V.L., 2001. The relationship
between testosterone and aggression: a meta-analysis. Aggress.
Violent Behav. 6, 579–599.
Brower, M.C., Price, B.H., 2001. Neuropsychiatry of frontal lobe
dysfunction in violent and criminal behaviour: a critical review.
J. Neurol. Neurosurg. Psychiatry 71 (6), 720–726.
Buchanan, R.W., Vladar, K., Barta, P.E., Pearlson, G.D., 1998.
Structural evaluation of the prefrontal cortex in schizophrenia.
Am. J. Psychiatry 155, 1049–1055.
Bushman, B.J., Cooper, H.M., 1990. Effects of alcohol on human
aggression: an integrative research review. Psychol. Bull. 107,
341–354.
Bustini, M., Stratta, P., Daneluzzo, E., Pollice, R., Prosperini, P.,
Rossi, A., 1999. Tower of Hanoi and WCST performance in
schizophrenia: problem-solving capacity and clinical correlates.
J. Psychiatr. Res. 33, 285–290.
Chesterman, L., Taylor, P., Cox, T., Hill, M., Lumsden, J., 1994.
Multiple measures of cerebral state in dangerous mentally
disordered inpatients. Crim. Behav. Ment. Health 4, 228–239.
Cornblatt, B.A., Risch, N.J., Faris, G., Friedman, D., Erlenmeyer-
Kimling, L., 1988. The Continuous Performance Test, identical
pairs version (CPT-IP): I. New findings about sustained
attention in normal families. Psychiatry Res. 26, 223–238.
Coughlan, A., Hollows, S., 1985. The Adult Memory and
Information Processing Battery (AMIPB) Test Manual. Cough-
lan, Leeds, England.
Crowell, T.A., Kieffer, K.M., Kugeares, S., Vanderploeg, R.D.,
2003. Executive and nonexecutive neuropsychological function-
ing in antisocial personality disorder. Cogn. Behav. Neurol. 16,
100–109.
Damasio, A.R., 1995. On some functions of the human prefrontal
cortex. Ann. N.Y. Acad. Sci. 769, 241–251.
Das, M., Barkataki, I., Kumari, V., Sharma, T., 2002. Neuroimaging
violence in the mentally ill: what can it tell us? Hosp. Med. 63,
604–609.
Devonshire, P.A., Howard, R.C., Sellars, C., 1988. Frontal lobe
functions and personality in mentally abnormal offenders. Pers.
Individ. Differ. 9, 339–344.
Dinn, W.M., Harris, C.L., 2000. Neurocognitive function in
antisocial personality disorder. Psychiatry Res. 97, 173–190.
Dolan, M., Park, I., 2002. The neuropsychology of antisocial
personality disorder. Psychol. Med. 32, 417–427.
Fazel, S., Danesh, J., 2002. Serious mental disorder in 23000
prisoners: a systematic review of 62 surveys. Lancet 359,
545–550.
First, M., Spitzer, R., Gibbon, M., Williams, J., 1995. Structured
Clinical Interview for DSM-IVAxis I Disorders, Patient Edition
(SCID-P), Version 2. New York State Psychiatric Institute,
Biometrics Research, New York.
First, M., Gibbon, M., Spitzer, R., Williams, J., Benjamin, L., 1997.
Users Guide for the Structured Clinical Interview for DSM IV
Axis II Personality Disorders. New York State Psychiatric
Institute, Biometrics Research, New York.
Franke, P., Maier, W., Hardt, J., Hain, C., Cornblatt, B.A., 1994.
Attentional abilities and measures of schizotypy: their variation
and covariation in schizophrenic patients, their siblings, and
normal control subjects. Psychiatry Res. 54, 259–272.
Goldberg, T., Gold, J., 1995. Neurocognitive deficits in schizo-
phrenia. In: Hirsh, S., Weinberger, D. (Eds.), Schizophrenia.
Blackwell, Oxford.
Golden, C., 1978. Stroop Color and Word Test: A Manual for
Clinical and Experimental Uses. Stoelting, Wood Dale, IL.
Golden, C.J., Jackson, M.L., Peterson-Rohne, A., Gontkovsky, S.T.,
1996. Neuropsychological correlates of violence and aggres-
sion: a review of the clinical literature. Aggress. Violent Behav.
1 (1), 3–25.
Gorenstein, E.E., 1982. Frontal lobe functions in psychopaths.
J. Abnorm. Psychology 91, 368–379.
Grossman, M., Zurif, E., Lee, C., Prather, P., Kalmanson, J., Stern,
M.B., Hurtig, H.I., 2002. Information processing speed and
sentence comprehension in Parkinson’s disease. Neuropsychol-
ogy 16, 174–181.
Gunn, J., Robertson, G., 1976. Drawing a criminal profile. Br. J.
Criminol. 16, 156–160.
Hare, R.D., 1984. Performance of psychopaths on cognitive tasks
related to frontal lobe function. J. Abnorm. Psychology 93,
133–140.
Hart, S., Cox, D., Hare, R., 1995. The Hare Psychopathy
Checklist—Revised Screening Version. Multi-Health Systems,
Toronto.
Heaton, R., 1993. Wisconsin Card Sorting Test Computer Version 2
Research Edition. Psychological Assessment Resources,
Odessa, FL.
Horn, N.R., Dolan, M., Elliot, R., Deakin, J.F.W., Woodruff, P.W.R.,
2003. Response inhibition and impulsivity: an fMRI study.
Neuropsychologia 41, 1959–1966.
Jones, H., 1992. Neuropsychology of violence. Forensic Rep. 5,
221–233.
Kay, S., Fishbein, A., Opler, L.A., 1987. The positive and negative
syndrome scale (PANSS) for schizophrenia. Schizophr. Res. 13,
261–276.
Krakowski, M.I., Convit, A., Jaeger, J., Lin, S., Volavka, J., 1989.
Neurological impairment in violent schizophrenic inpatients.
Am. J. Psychiatry 146, 849–853.
Laakso, M., Vaurio, O., Koivisto, E., Savolainen, L., Eronen,
M., Aronen, H., Soininen, H., Tiihonen, J., 2001. Psychop-
athy and the posterior hippocampus. Behav. Brain Res. 118,
187–193.
Lapierre, D., Braun, C.M., Hodgins, S., 1995. Ventral frontal
deficits in psychopathy: neuropsychological test findings.
Neuropsychologia 33, 139–151.
Miczek, K.A., DeBold, J.F., van Erp, A.M., Tornatzky, W., 1997.
Alcohol, GABAA–benzodiazepine receptor complex, and
aggression. Recent Dev. Alcohol. 13, 139–171.
Miller, L., 1987. Neuropsychology of the aggressive psychopath: an
integrative review. Aggress. Behav. 13, 114–119.
Mirsky, A.F., 1988. Research on schizophrenia in the NIMH
Laboratory of Psychology and Psychopathology, 1954–1987.
Schizophr. Bull. 14, 151–156.
I. Barkataki et al. / Schizophrenia Research 74 (2005) 1–13 13
Morgan, A.B., Lilienfeld, S.O., 2000. A meta-analytic review of the
relation between antisocial behavior and neuropsychological
measures of executive function. Clin. Psychol. Rev. 20, 113–136.
Morris, R.G., Rushe, T., Woodruffe, P.W., Murray, R.M., 1995.
Problem solving in schizophrenia: a specific deficit in planning
ability. Schizophr. Res. 14, 235–246.
Morris, R.G., Rowe, A., Fox, N., Feigenbaum, J.D., Miotto, E.C.,
Howlin, P., 1999. Spatial working memory in Asperger’s
syndrome and in patients with focal frontal and temporal lobe
lesions. Brain Cogn. 41, 9–26.
Nelson, H., Willison, J., 1991. National Adult Reading Test Manual.
Nfer-Nelson, Windsor.
Pantelis, C., Barnes, T.R., Nelson, H.E., Tanner, S., Weatherley, L.,
Owen, A.M., Robbins, T.W., 1997. Frontal-striatal cognitive
deficits in patients with chronic schizophrenia. Brain 120,
1823–1843.
Perlstein, W.M., Carter, C.S., Barch, D.M., Baird, J.W., 1998. The
Stroop task and attention deficits in schizophrenia: a critical
evaluation of card and single-trial Stroop methodologies.
Neuropsychology 12, 414–425.
Posthuma, D., Baare, W.F., Hulshoff Pol, H.E., Kahn, R.S.,
Boomsma, D.I., De Geus, E.J., 2003. Genetic correlations
between brain volumes and the WAIS-III dimensions of verbal
comprehension, working memory, perceptual organization, and
processing speed. Twin Res. 6, 131–139.
Prentice, N.M., Kelly, F.J., 1963. Intelligence and delinquency:
a reconsideration. J. Soc. Psychol. 60, 327–337.
Raine, A., Buchsbaum, M., LaCasse, L., 1997. Brain abnormalities
in murderers indicated by positron emission tomography. Biol.
Psychiatry 42, 495–508.
Raine, A., Lencz, T., Bihrle, S., LaCasse, L., Colletti, P., 2000.
Reduced prefrontal gray matter volume and reduced autonomic
activity in antisocial personality disorder. Arch. Gen. Psychiatry
57, 119–127.
Rao, S.M., 1995. Neuropsychology of multiple sclerosis. Curr.
Opin. Neurol. 8, 216–220.
Rasmussen, K., Levander, S., Sletvold, H., 1995. Aggressive and
non-aggressive schizophrenics: symptom profile and neuro-
psychological differences. Psychol., Crime, Law 2, 119–129.
Reiss, A.J., Miczek, K.A., Roth, J.A., 1994. Understanding and
Preventing Violence: II. Biobehavioural Influences. National
Academy Press.
Schmitter-Edgecombe, M.E., Marks, W., Fahy, J.F., Long, C.J.,
1992. Effects of severe closed-head injury on three stages
of information processing. J. Clin. Exp. Neuropsychol. 14,
717–737.
Schretlen, D., Pearlson, G.D., Anthony, J.C., Aylward, E.H.,
Augustine, A.M., Davis, A., Barta, P., 2000. Elucidating the
contributions of processing speed, executive ability, and frontal
lobe volume to normal age-related differences in fluid intelli-
gence. J. Int. Neuropsychol. Soc. 6, 52–61.
Sharma, T., Antonova, L., 2003. Cognitive function in schizophre-
nia. Deficits, functional consequences, and future treatment.
Psychiatr. Clin. North Am. 26, 25–40.
Soderstrom, H., Blennow, K., Manheim, A., Forsman, A., 2001.
CSF studies in violent offenders. 5-HIAA as a negative and
HVA as a positive predictor of psychopathy. J. Neural Transm.
108, 869–878.
Spitzer, R., Williams, J., Gibbon, M., First, M., 1995. Structured
Clinical Interview for DSM-IV—Non-Patient Edition. Ameri-
can Psychiatric Press, Washington, DC.
Taylor, P., Leese, M., Williams, D., Butwell, M., Daly, R., Larkin,
E., 1998. Mental disorder and violence. A special (high security)
hospital study. Br. J. Psychiatry 172, 218–226.
Tiihonen, J., Isohanni, M., Rasanen, P., Koiranen, M., Moring, J.,
1997. Specific major mental disorders and criminality: a 26-year
prospective study of the 1966 northern Finland birth cohort.
Am. J. Psychiatry 154, 840–845.
Virkkunen, M., Linnoila, M., 1993. Brain serotonin, type II alcohol-
ism and impulsive violence. J. Stud. Alcohol 11, 163–169.
Vlaar, A.M., Wade, D.T., 2003. The Adult Memory and Information
Processing Battery (AMIPB) test of information-processing
speed: a study of its reliability and feasibility in patients with
multiple sclerosis. Clin. Rehabil. 17, 386–393.
Volavka, J., 1999. The neurobiology of violence. J. Neuropsychiatry
Clin. Neurosci. 11 (3), 307–314.
Vollm, B., Richardson, P., Stirling, J., Elliott, R., Dolan, M.,
Chaudhry, I., Del Ben, C., McKie, S., Anderson, I., Deakin, B.,
2004. Neurobiological substrates of antisocial and borderline
personality disorder: preliminary results of a functional fMRI
study. Crim. Behav. Ment. Health 14, 39–54.
Walsh, A., 1991. Intellectual Imbalance. Love, Deprivation and
Violent Delinquency: A Biosocial Perspective. Charles C.
Thomas, Springfield, IL.
Wechsler, D., 1997. Manual for Wechler adult Intelligence Scale—
Third Edition. The Psychological Corporation, San Antonio.
Wechsler, D., 1998. Wechsler Memory Scale—Third Edition. The
Psychological Corporation, London.
Yeudall, L.T., 1977. Neuropsychological assessment of forensic
disorders. Can. Ment. Health 25, 7–18.
Recommended