Develop. Med. Child Neurol. 1970, 12, 145-152
A Syndrome of Congenital Malformations possibly due to Maternal Diabetes
D. A . J . Williamson
THE relationship between diabetes mellitus during pregnancy and congenital mal- formations in the resulting infants has interested paediatricians and obstetricians for many years. Many workers claim that the risk of congenital abnormality is significantly increased for babies born to diabetic mothers, although there is a con- siderable discrepancy among the published figures (Table I). To some extent the con- fusion is due to the difficulty in defining just what is understood by a congenital abnormality; somc workers include every minor blemish as an abnormality while others consider only major or lethal deformities. Pedersen et al. (1964), taking major malformations only, found an incidence of 5.2 per cent in the infants of diabetic mothers, compared with 1 -2 per cent in a control series, but there was no increase in the incidence of minor abnor- malities. Analysis of Farquhar’s (1965) cases shows that 10 (6.6 per cent) of 152 liveborn infants of diabetic mothers had major congenital abnormalities, but he claims that this proportion is no higher than that in his series of carefully matched controls. It is, however, three times greater than the overall incidence of 2.3 per cent given by McKeown and Record (1960).
All types of malformations have been described among infants of diabetic mothers and most authors do not suggest that there is any particular pattern in this group; however Herre and Horky (1964) and Roszkowski and Kietlinska (1965) have reported a relatively high incidence of central nervous system abnormalities and Pedersen et a/. (1964) mention that several of their cases had severe bony abnormalities of the limbs. Lenz and Maier (1964) have drawn attention to a number of uncommon abnormalities which they claim may be particularly related to maternal diabetes. Reporting 2 cases with femoral aplasia and other deformities of the legs, they note that 7 of the cases reported by Pedersen et a/. (1964) were similarly affected. In a subsequent review of the literature, Kucera et al. (1965) collected the records of 31 infants born to diabetic mothers whose major abnormality was either aplasia or hypo- plasia of the femora, agenesis of the lower vertebrae, or both. They refer to this as the ‘Syndrome of Caudal Regression’, as described by Duhamel (1 961), and they point out that among the 50 cases of sacral agenesis reported by Blumel et al. (1959), 6 were the offspring of diabetic mothers. Further examples of this syndrome have
~
Southampton Children’s Hospital, Winchester Road, Southampton SO9 4WR.
145

DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1970, 12
TABLE I Incidence of Congenital Abnormalities among (he Infants of Diabetic Mothers
Author
Peel and Oakley (1950) . . Hargbard e t a / . (1959) . . Pitt (1962) .- .. Pedersen et a/ . (1984, . . Herre and Horky (1964) . . Farquhar ( I 965) .. Hubbell et a / . (1965j . . Breidahl(l966) . . . . Watson (1968) . . . . Barashnev (1968) . . . .
Dunn (1964)’ ‘ ..
Total No. of Infants Centre
I-
London .. .. Stockholm .. New Zealand . . Birmingham .. Copenhagen .. Karlsburg . . . . Edinburgh .. Boston . . . . Melbourne .. London .. .. Moscow .. ..
I 4 2 514 1 I 3 69
853 143 I 5 2 413 200 197 -
Overall Incidence of Congenital Abnormalities
McKeown and Record ( I 960) Birmingham . . I 51,160
Percentage Abnormal
6 . 3 7 . 6 4 .4 1 . 5 5 . 2 6 . 8 6 . 6
13 .0 2 0 . 0 10.7 5 . 0
2 .31
been reported by Aubertin et al. (1964), Stern el al. (1965), Rusnak and Driscoll (1966), Frantz and Aitken (1967) and Hiertonn et al. (1967), but so far no British cases have been described.
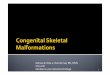
Case-Records Case 1 (Fig. 1)
This first-born female infant was delivered by caesarean section at 36 weeks gestation, weighing 2,460 g. At birth she was noticed to have micrognathia, cleft lip and palate, and a small upright tongue. The neck was short and there was a Sprengels’ deformity of the left shoulder. The left femur was considerably shorter than the right and there was bilateral metatarsus varus deformity of the feet. After considerable difficulty with feeding due to glossoptosis, the child made good progress. She has had a number of corrective operations and can now walk well. Her intelligence is normal.
Her mother, who was 23 at the time of Fig. 1
the pregnancy, had been treated for Case 2 (Fig. 2) diabetes since the age of 16. Throughout This female infant was delivered by the pregnancy there had been little medical caesarean section at 38 weeks gestation, supervision and the diabetes was known weighing 3,150 g. She was noted to have a to have been poorly controlled with lente markedly ‘Cushingoid’ facies, and the insulin. lower half of her body was grossly
146

D. A. J. WILLIAMSON
Fig. 3
Fig. 2
abnormal. There was marked shortening of both legs with fixed abduction and external rotation of the hips and flexion of the knees. The feet were abnormally small and had varus deformities. The upper arms also seemed to be shorter than normal. X-rays confirmed the shortening of all the long bones of the legs and also of the humeri. Agenesis of the vertebrae from L.4 downwards was demonstrated with consequent collapse of the pelvis (Fig. 3). The infant subsequently developed con- gestive heart failure and was found to have cardiac enlargement and a systolic murmur. She never thrived and eventually died at the age of five weeks. Post-mortem examination showed the heart to be grossly abnormal with severe pulmonary stenosis and post-stenotic dilatation of the pulmonary artery. A widely patent ductus arteriosus joined the aorta just distal to a severe coarctation. The left ventricle was
hypoplastic and there was a small ventri- cular septal defect. In addition, she had multiple spleneculae and a malrotation of thecolon.The tongue was small andupright.
The infant’s mother was 24 at the time of pregnancy and had been a known diabetic since the age of 15. Two previous and one subsequent pregnancy produced normal babies. Her diabetes had been well con- trolled with lente insulin throughout the pregnancy.
Cuse 3 (Fig. 4) This male child was delivered by
caesarean section. At birth he had gross abnormalities of the lower half of the body. The abdominal musculature was very poor and there were large bilateral herniae. There was bilateral dislocation of the hips. The left tibia was hypoplastic and the upper end of the right tibia was not expanded. The left knee-joint was grossly abnormal. There were six toes on each foot. In addition, there was shortening of the right forearm. The ears were pointed. He was later found to have a systolic murmur, believed to be due to a small ventricular septal defect. He has under- gone numerous operations, including an
147

DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1970, 12
Fig. 6
amputation of the left leg at the knee-joint. At the age of 12 years he is now remarkably fit and attends a normal school.
His mother, who was 33 at the time of the pregnancy, had been diabetic for 8 years. During the first trimester her diabetes had been poorly controlled and she had been in hypoglycaemic coma several times.
Fig. 5
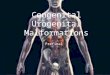
Case 4 (Fig. 5 ) This male infant was born at 36 weeks
gestation, weighing 6 lb. 10 oz. He had severe abnormalities of the lower half of the body. Shortly after birth he developed hypoglycaemia, requiring treatment with intravenous glucose. The legs were abnormally short, with very little muscular development below the knees. The feet were small, and movement at the ankle and tarsal joints was much restricted. Extension of the knees was also somewhat limited. There was a diffuse swelling it1 the sacral region and two marked dimples over the buttocks. X-rays confirmed the hypoplasia of the long bones of the legs and revealed agenesis of the vertebrae from L.3 down-
148

D. A. J. WILLIAMSON
wards with consequent collapse of the pelvis (Fig. 6).
His mother was 32 at the time of the pregnancy. She had had two previous pregnancies; the first was normal but the second resulted in a full-term stillborn infant weighing 109 lb. During the third pregnancy she was found to be diabetic at the fourth month and was treated with 24 units of soluble insulin daily. Since delivery, however, it has been possible to control her diabetes with dietary treatment only.
Discussion The collection of a group of patients
having in common reduction defects of the legs with or without agenesis of the lower segments of the spinal column involves a degree of selection, but the resulting clinical picture is sufficiendy unusual and
striking to warrant the use of the term ‘syndrome’. In only a minority of the recorded cases of caudal regression has maternal diabetes been noted, but this may well be due to the author’s failure to appreciate the significance of this feature. Conversely, many other abnormalities have been observed in infants with the caudal regression syndrome born to diabetic mothers. Table I1 sets out the pattern of associated defects described in the recorded cases. This list is probably incomplete, as many of the case-reports in the literature are very brief. It will be seen that certain malformations, particularly those of the upper limbs, mouth, palate and heart, occur frequently. How far it is possible to include these other abnormalities in the syndrome must be a matter of opinion, but it would seem that the term ‘Syndrome of Caudal Regression’ may be too circumscribed.
TABLE I1 Abnormalities found in 43 cases of Diabetic Embryopathy Syndrome
Abnormality
Spinal : Vertebral agenesis, dorsal . . . . . . Vertebral agenesis, lumbar . . . . . . Vertebral agenesis, sacral . . . . . . Meningom yelocele . . . . . . . . Spina bifida occulta . . . . . . Other spinal abnormalities . . . . . .
Leg : Aplasia of femur.. . . . . . . . . Hypoplasia of femur . . . . . . . . Hypoplasia of lower leg . . . . . . Syrenomelia . . . . . . . . . . Other leg abnormalities . . . . . . . .
~~~~ ~
Abnormalities of the arm . . . . . . . . Joint :
Dislocation of him . . . . Talipes . . . . . . . . . . . . Arthrokryposis . . . . . . . . . .
Cleft lip . . . . . . . . . . . . Cleft palate . . . . . . . . SmaU tongue . . . . . . . . . . Micrognathia . . . . . . . . . .
Mouth:
Other paletal abnormaliiiks . . . . . .
Heart abnormality . . . . . . . . . .
No.
1 16 23
1 4 2
5 14 7 2
15
6
10 12 7
149

DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1970, 12
The ‘Diabetic Embryopathy Syndrome’ might be appropriate, but careful epidemi- ological studies will first have to be made to establish the exact relationship between the congenital abnormalities and maternal diabetes.
There is little direct evidence to suggest how maternal diabetes can affect the early development of the fetus. Pedersen et al. (1964) have shown that the degree of control of the diabetes has little influence on the risk of the infant being deformed. Mice rendered diabetic by Alloxan have been shown to give birth to a high proportion of malformed young (Watanabe and Jngalls 1963, Endo 1966), many of which have abnormalities of the mouth and palate but not of the spine or limbs. I t is possible that the clinical manifestations of overt diabetes are not of themselves embryopathic but that more fundamental factors may be concerned. Of particular interest in this respect are the reports of two apparently typical cases of the syn- drome born to mothers who later developed clinical diabetes-in one case one year and the other six years after the baby’s birth (Kalitski 1965, McCracken 1965). Navarete et al. (1967) have pointed out that prediabetic mothers have an in- creased risk of producing infants with malformations, particularly of the CNS, and it is well known that they may give birth to overweight babies many years before developing diabetes. Vallance-Owen and his co-workers (1966, 1967) have found increased levels of insulin antagonists in the serum of mothers who had given birth to infants with certain types of malforma- tion, and it is claimed that these findings show the women to be cases of essential diabetes. Three groups of mothers were studied by these workers: those whose
infants were born with defects of the spine (including spina bifida), those with infants having cleft lip or palate and those with infants having deformities of the arms or hands (including a number of ‘thalidomide babies’). Of the 66 mothers studied, 52 had increased insulin antagonism and werz thus considered to be essential diabetics, compared with only 14 out of the 50 controls. The way in which insulin antagon- ists might affect the developing embryo remains obscure, although the possibility that insulin itself might be embryopathic has to be considered. Vallance-Owen and Lilley (1961) claim that increased insulin antagonism stimulates increased insulin production. Increased urinary excretion of insulin has been found in untreated juvenile diabetics by Steinke et a/. (1961) and in the sibs of juvenile diabetics by McArthur and Stimmler (1966). It has long been known that the injection of insulin into chick embryos produces rumplessness in a high proportion of the resultant chicks (Landauer 1945). Durais- wami (1950) has shown that when the insulin is injected in the first two days of incubation, the vertebral column is pri- marily affected, with agenesis of the lower segments, whereas if the injection is delayed until the fourth or fifth day, the limb-bones, particularly the tibiae, and the beak are mainly affected. The similarity between these deformities in the chick and the syndrome described in humans is most striking.
Acknowledgemen/s: My thanks are due to Prof. A. W. Wilkinson and Dr. R. E. Bonham-Carter, and to Dr T. H. Hughes Davies for allowing me to publish details of their cases (Nos. 3 and 4); also to the Department of Medical Illustration at the Hospital for Sick Children, Great Ormond Street, London for figure 4.
150

D. A. J. WILLIAMSON
SUMMARY There is a recognised association between maternal diabetes and certain congenital
malformations, particularly agenesis of the lower segments of the spinal column and redu- tion defects of the legs, and the literature on such cases is reviewed. Four further cases are described. The pathogenesis of the syndrome is briefly discussed and the suggestion is made that insulin itself might be embryopathic.
RESUME Syndrome de malformations congenitales probablement d6es h un diabPte maternel
On a not6 une association entre le diabtte maternel et certaines malformations con- gdnitales, en particulier l’agkndsie des segments infdrieurs de la colonne vertdbrale et des ddfauts de jambe 8 type d’insuffisance de ddveloppement. Les auteurs font une revue de ces cas dans la littiratwe. Quatre cas sont ddcrits. Puis la pathogdnie du syndrome est discutde britvement et il est sugg6rC que l’insuline par elle-m&me ait un r61e embryopathique.
ZUSAMMENFASSUNG Ein Syndrom congenitaler Missbildungen moglicherweise auf Grund eines mutterlichen
Diabetes Es gibt eine anerkannte Verbindung zwischen miitterlichem Diabetes und bestimmten
congenitalen MiSbildungen, insbesondere Aplasie der unteren Ruckenmarkssegmente und Reduktionsdefekte der Beine; die Literatur uber solche Falle wird besprochen. Es werden vier Falle beschrieben. Die Pathogenese dieses Syndroms wird kurz diskutiert und die Vermutung geauBert, daB das Insulin selbst embryopathisch wirken kann.
RESUMEN Un sindrome de malformaciones congenitas debido posiblemente a diabetes materna
Existe una reconocida asociacidn entre diabetes materna y ciertas malformaciones congdnitas, especialmente agenesia de segmentos bajos del raquis y defectos por reduccidn de las piernas. Se revisa la literatura que trata de estos casos. Se decriben cuatro casos. Se discute brevemente la patogenia del sindome y la sugerencia de que la propia insulina pueda tener una accidn embriophtica.
REFERENCES Aubertin, E., Aubertin, J., Gay, J. (1964) ‘Importance de la valeur du traitement antidiabetique chez les
diabetiques encientes.’ J. Mkd. Bordeaux, 141, 333. Barashnev, Y. 1. (1968) Personal communication. Blumel, J., Evans, E. A., Eggers, G. W. N. (1959) ‘Partial and complete agenesis or malformation of the
sacrum with associated anomalies: etiologic and clinical study with special reference to heredity. A prelim- inary report.’ J. Bone Jt Surg., 41A, 497.
Breidahl, H. D. (1966) ‘The growth and development of babies born to mothers with diabetes.’ Med. J. Aust., i, 268.
Dandrow, R. V., O’Sullivan, J. B. (1966) ‘Obstetric hazards of gestational diabetics’ Amer. J. Obstet. Cynec., 96,1144.
Duhamel, B. (1961) ‘From the mermaid to anal imperforation: the syndrome of caudal regression.’ Arch. Dis. Childh., 36, 152.
Dunn, P. M. (1964) ‘Congenital malformation and maternal diabetes .’ Lancet, U, 644. Duraiswani. P. K. (19501 ‘Insulin-induced skeletal abnormalities in developing chickens.’ Brit. med. J., U, . . - -
384.
Hlth, 12,492.
Recent Advances in Paediatncs, 3rd. ed. London: J. & A. Churchill, p. 121.
1531.
Endo, A. (1966) ‘Teratogenesis in diabetic mice treated with alloxan prior to conception.’ Arch. envrronm.
Farquhar, J. W . (1965) ‘The hfluence of maternal diabetes on mother and child.’ In Gairdner, D. (Ed.)
Frantz, G. H., Aitken, G. T. (1967) ‘Complete absence of lumbar spine and sacrum.’J. BoneJt Surg., 49A,
151

DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1970, 12
Hargbard, L., Olow, I., Reinand, T. (1959) ‘A follow-up study of 514 children of diabetic mothers.’ Acta paediat. (Uppsala), 48, 184.
Herre, H. D., Horky, Z. (1964) Die Missbildungsfrequenz bei Kindern diabetischor Mutter.’ Zbl. Gynek., Pli ICR -”. .--.
Hiertonn, T., Holmgren, G., Holmgren, E. (1967) ‘Agensis of lumbosacral, vertebral, surgical and prosthetic
Hubbell, J. P., Muirhead. D. H., Drorbaugh, J. E. (1965) ‘The newborn infant of the diabetic mothers’ Men.
Kalitzki, M. (1965) ‘Congenital malformations and diabetes.’ Lancete, U, 641. Kucera, J., Lenz, W., Maier, W., (1965) ‘Missbildungen der Beine und kaudalen Wirbelsaule bei Kindern
Landauer, W. (1945) ‘Rumplessness of chicken embryos produced by the injection of insulin and other
management.’ Prosth. Int. 3, 24.
Clin. N . Amer., 49, 1035.
diabetlscher Mutter.’ Dtsch. med. Wschr., 90,901.
chemicals.’ J. exp. Zool., 98, 65. Lenz, W., Maier, W. (1964) ‘Congenital malformations and maternal diabetes.’ Lancet, ii, 1124. McArthur, R. G., Stimmler, L. (1966) ‘Urinaiy insulin excretion in healthy children and in siblings of child-
hood-onset diabetes.’ Lancet, I, 1236. Macracken. J. S. (1965) ‘Absence of foetal femur and maternal prediabetes.’ Lancet, i, 1274. McKeown, T., Record, R. G. (1960) ‘Malformations in a population observed for 5 years after birth.’ In
Wolstenholme, G. E. W., O’Connor, M. (Eds.) Ciba Foundation Symposium on Congenital Malforma- tions. London: J. & A. Churchill, p. 2.
Navarete, V. N., Torres, I. H., Rivera, I. R., Shor, V. P., Gracia, P. N. (1967) ‘Maternal carbohydrate disorder and congenital malformations.’ Diabetes, 16, 127.
Pedersen, L. M., Tyg,trup, I., Pedersen, J. (1964) ‘Congenital malformations in infants of diabetic mothers.’ Lancet, 1, 11 24.
Peel, J. H., Oakely ,W. G. (1950) ‘The management of pregnancy in diabetics.’ I n Bourne, A. W., Nixon, W. C. W. (Eds.) Tiansactions of the 12th British Congress for Obstetrics and Gynaecology. London: The Congress Committee with Austral Press. p. 161.
Pitt, D. B. (1962) ‘Congenital malformations: a review.’ Med. J. Aust., i, 82. Roszkowski, I., Kietlinska, Z. (1965) ‘Indirect causes of congenital malformation. An analysis of 212 cases.’
Gynecologia (Easel), 159.47. Rusnak, S . L., Driscoll, S. G. (1965) ‘Congenital spinal anomalies in infants of diabetic mothers.’ Pediatrics,
35,989. Steinke, J., Taylor, K. W.. Renold, A. E. (1961) ‘Insulin and insulin antagonists in the serum of untreated
juvenile diabetics.’ Lancet, 1, 30. Stem, L., Ramos, A., Light, I. (1965) ‘Congenital malformations and diabetics.’ Lancet, i, 1393. - B,aithwaite, F., Wilson, J. S. P.. Edwards, J. R. G., Maurice, D. G. (1967) ‘Cleft lip and palate deform-
ities and insulin antagonism.’ Lancet, U, 912. Vallance-Owen, J., Lilley, M. D. (1961) ‘An insulin antagonist associated with plasma-albumin.’ Lancet, i,
804. Watanabe, G., Ingalls, T. H. (1963) ‘Congenital malformations in the offspring of alloxan-diabetic mothers.’
Diabetes, 12.66. Watson, C. (1968) ‘A follow-up study of children born to diabetic mothers.’ Arch. Dis. Childh., 43,746. Wilson, J. S., Valiance-Owen, J. (1966) ‘Congenital deformities and insulin antagonism.’ Lancet, ii, 940.
152
Recommended