ARDS was first described in the medical lit-erature in the 1960s as a mysterious condi-tion associated with traumatic injuries and amortality rate as high as 70%. However,case reports dating back as far as WorldWar I suggested that injuries, includingtrauma and sepsis, adversely affected lungfunction. Despite a better understanding ofthe pathophysiology of ARDS and advancesin mechanical ventilation and antibiotictherapy, it remains somewhat of a mystery.Although mortality rates have decreased toaround 40%, ARDS is difficult to diagnoseand can prove fatal within 48 hours of onsetif not promptly diagnosed and treated.Some patients who survive ARDS recovercompletely, whereas others experience last-ing damage to their lungs and other healthproblems. It’s hopeful that the use of newtreatment modalities, such as lung protec-tive strategies and permissive hypercapnia,will help lower mortality rates.
In this article, we’ll begin by reviewinghow ARDS occurs, the pathophysiologybehind it, and its diagnostic criteria; thenwe’ll discuss current management strategies
and nursing interventions and take a look atthe possible future of treatment.
Lung injury gone haywireARDS is a form of pulmonary edema char-acterized by severe hypoxemia that canrapidly lead to acute respiratory failure. Itoccurs as the result of a direct or indirectlung injury; it doesn’t occur in isolation. Examples of a direct lung injury include:• gastric aspiration• bacterial, fungal, or viral pneumonia• pulmonary contusion• near drowning• prolonged inhalation of high concentra-tions of oxygen, smoke, or toxic substances.
An indirect injury occurs outside thelungs. Examples include:• sepsis• shock (any cause)• drug overdose• fat embolism• prolonged hypotension• nonthoracic trauma• cardiopulmonary bypass• head injury
32 Nursing made Incredibly Easy! November/December 2009 www.NursingMadeIncrediblyEasy.com
2.3ANCC
CONTACT HOURS
Acute respiratory distress syndrome (ARDS) is a life-threateningcondition affecting about 190,000 patients a year in the UnitedStates, according to the National Heart Lung and Blood Institute.With prompt treatment, 7 out of 10 patients survive. We give youtried-and-true management strategies and nursing interventionsand fill you in on what’s new in treatment research.By Laura Blume, RN, CCRN, BSNClinical Nurse Educator • Presbyterian Hospital • Charlotte, N.C.Diane Byrum, RN, CCNS, CCRN, MSN, FCCMCritical Care Clinical Nurse Specialist • Presbyterian Hospital • Charlotte, N.C.
The authors have disclosed that they have no significant relationships with or financial interest in any commercial companies that pertain tothis educational activity.
Unraveling the mystery of

www.NursingMadeIncrediblyEasy.com November/December 2009 Nursing made Incredibly Easy! 33
ARDS

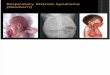
A closer look at ARDS
• acute pancreatitis• uremia• hematologic disorders, such as disseminat-ed intravascular coagulation, or multipleblood transfusions.
An acute responseARDS can be categorized into three mainphases: the exudative phase, the prolifera-tive phase, and the fibrotic phase (see Acloser look at ARDS for a further breakdownof the underlying pathophysiologic phases).Let’s take a closer look.
In the exudative phase, an injury to thelungs, whether direct or indirect, leads to anacute inflammatory response, lasting up to 1week. First, chemical mediators are called tothe scene of the injury and released into thesystemic circulation, including tumor necro-sis factor alpha, numerous interleukins (IL-1;IL-4, 5, and 6; and IL-8), platelet-activatingfactor, nitric oxide (NO), prostacyclin, oxy-gen-free radicals, histamine, and bradykinin.These chemical mediators call on leukocytes
to connect with cells involved in the injuryand destroy the invading organisms. Themost important of these leukocytes are neu-trophils, which can adhere to the lining ofblood vessels, squeeze between endothelialcells, and enter tissue. The neutrophils thenphagocytize, or eat, the invading organ-isms. If further phagocytosis is needed,macrophages move in within 24 hours andtake over the job of cleaning up dead tissueand any remaining organisms. However, thepresence of macrophages leads to a chronicinflammatory process.
In the proliferative phase (sometimescalled the fibroproliferative phase), theinflammatory process in the lungs occurssystemically throughout all tissues, leadingto increased capillary permeability andmovement of fluid out of the vascular spaceand into the tissue. In the lung bed, this leadsto pulmonary and interstitial alveolar edemaand inactivation of surfactant, which resultsin alveolar flooding and collapse (atelectasis)and reduced compliance, or stretch, of lung
34 Nursing made Incredibly Easy! November/December 2009 www.NursingMadeIncrediblyEasy.com
1PhaseIn phase 1, injury reduces normal bloodflow to the lungs. Platelets aggregate andrelease histamine (H), serotonin (S), andbradykinin (B).
2PhaseIn phase 2, those substances—especiallyhistamine—inflame and damage the alveolocapillary membrane, increasingcapillary permeability. Fluids then shift intothe interstitial space.
3PhaseIn phase 3, as capillary permeability increases, proteins and fluids leak out, increasing interstitial osmotic pressureand causing pulmonary edema.

tissue. Decreased compliance, along with anincreased work of breathing, leads to hypox-emia that’s unresponsive to increasing levelsof supplemental oxygen. The result is pul-monary edema, decreased ability to extractoxygen, and, eventually, cellular death.
In addition to leaky capillaries, the coag-ulation (clotting) and fibrinolytic (clotbreakdown) systems are activated. Clotsform in the small capillaries of the lungs.When blood is diverted around these clots, ventilation/perfusion, or V/Q, mismatchoccurs because of impaired gas exchangedue to decreased ventilation or perfusion atthe alveolar capillary membrane, leading toworsening hypoxemia. In addition, smallclots are formed all over the body, whichleads to multiple organ dysfunction. As theprocesses of leaking capillaries and clot for-mation continue over time, the alveoli losetheir elastic properties and become fibrotic.This phase can last up to 3 weeks.
In the fibrotic phase (sometimes called theresolution or recovery phase), the lungs
begin to recover. Lung function may contin-ue to improve over a period of 6 to 12months. Typically, patients suffer long-termeffects, such as permanent loss of lung tissueand diminished vital capacity, which lead toimpaired pulmonary gas exchange andobstructive and restrictive pulmonarydefects. Patients may have difficulty per-forming activities of daily living for the restof their lives.
Rapid onset of signs andsymptomsThe acute phase of ARDS is marked byrapid onset of severe dyspnea, usually oc-curring 12 to 48 hours after the initial injury(see Is the stage set for ARDS?). The patientwill experience arterial hypoxemia thatdoesn’t respond to supplemental oxygenand will have worsening bilateral infiltrateson chest X-ray. The acute lung injury willthen progress to fibrosing alveolitis withpersistent, severe hypoxemia. He’ll also haveincreased alveolar dead space (ventilation to
www.NursingMadeIncrediblyEasy.com November/December 2009 Nursing made Incredibly Easy! 35
4PhaseIn phase 4, decreased blood flow and fluids in the alveoli damage surfactant andimpair the cell’s ability to produce more. Asa result, alveoli collapse, impeding gas ex-change and decreasing lung compliance.
5PhaseIn phase 5, sufficient oxygen can’t crossthe alveolocapillary membrane, but carbon dioxide (CO2) can and is lost withevery exhalation. Oxygen (O2) and CO2levels decrease in the blood.
6PhaseIn phase 6, pulmonary edema worsens,inflammation leads to fibrosis, and gas exchange is further impeded.

the alveoli but poor perfusion) and decreased lung compliance.
Other signs of ARDS include:• rapid, shallow breathing• cyanosis• intercostal retractions• pulmonary crackles• rhonchi• altered mental status• tachycardia.
With severe ARDS, signs include:• hypotension
• decreased urine output• respiratory alkalosis.
Diagnostic criteriaThe criteria for establishing a diagnosis ofARDS include the following:• the occurrence of an acute lung injury ora history of systemic or pulmonary risk fac-tors• acute onset of respiratory distress• diffuse, bilateral infiltrates on chest X-ray(ARDS can occur in patients who have
36 Nursing made Incredibly Easy! November/December 2009 www.NursingMadeIncrediblyEasy.com
Is the stage set for ARDS?Timing after initial injury Physiologic changes Clinical and diagnostic indicators
Within 24 hours • Neutrophils and protein-filled fluid leak into • Mild hypoxemia, dyspnea, and tachypnea, whichthe alveoli. may be masked by an underlying problem, such as• Problems with surfactant production and pneumonia or exacerbation of chronic obstructivefunction occur. pulmonary disease
• Possibly, evidence of alveolar edema on chest X-ray
Within 48 hours • Surfactant decreases or becomes ineffective. • Manifestations of acute respiratory failure,• Inflammatory mediators and free radicals are including agitation, tachypnea, tachycardia,released. The endothelium becomes inflamed hypertension or hypotension, and pallorand the interstitial spaces and capillaries • Patient generally needs endotracheal intubationbecome congested. and mechanical ventilation with PEEP• The patient develops widespread • Increase in oxygen saturation level doesn’tmicroatelectasis as his pulmonary correspond to increased oxygen concentrationmicrovasculature breaks down. delivered via the ventilator due to loss of functioning
alveoli; this is a hallmark of ARDS• Patchy bilateral alveolar infiltrates on chest X-ray• Decreased partial pressure of arterial oxygen (PaO2) and partial pressure of carbon dioxide in arterial blood (PaCO2) levels
2 to 10 days • The alveoli become consolidated with • Manifestations of acute respiratory failurecellular and fibrin deposits; hyaline • Possibly, development of systemic inflammatorymembranes develop. response syndrome (SIRS) and eventual • Surfactant production is greatly decreased. multisystem organ dysfunction
• Hemodynamic instability common, especially hypotension during position changes• Alveolar infiltrates and dependent atelectasis on chest X-ray• Eventually, partial pressure of carbon dioxide (PcO2) levels rise
10+ days after injury • Fibroproliferation results in fibrosing alveolitis. • Fever, continued SIRS• Significant fibrosis may lead to chronic • PEEP less effective at maintaining PaO2 levelspulmonary fibrosis.

undergone a pneumonectomy and haveonly one lung.)• severe refractory hypoxemia, demon-strated by a partial pressure of arterial oxy-gen (PaO2)/fraction of inspired oxygen(FiO2), or P/F, ratio of less than 200 mm Hg(To calculate the P/F ratio, divide the PaO2by the FiO2. A normal P/F ratio is greaterthan 300 mm Hg; with acute lung injury,the P/F ratio is less than 300 mm Hg.)• no clinical evidence of left-sided heartfailure (left atrial hypertension), demon-strated by a pulmonary capillary wedgepressure (PCWP) of less than 18 mm Hg.(In ARDS, a patient may exhibit pulmonaryedema, but PCWP must be within normallimits [noncardiogenic pulmonary edema].)
True blue managementstrategiesTreatment for ARDS primarily involvessupportive care in the ICU, includingproviding adequate oxygenation withavoidance of complications, drug therapy,nutritional support, prone positioning, andpermissive hypercapnia.
Supportive therapy almost alwaysincludes endotracheal intubation andmechanical ventilation. In the past, patientswith ARDS were mechanically ventilatedusing a high tidal volume, which oftenresulted in barotrauma (injury or damage tothe lung tissue that can lead to entry of airinto the pleural space [pneumothorax] or thetracking of air along the vascular bundle tothe mediastinum [pneumomediastinum]).Practice changed after the National HeartLung and Blood Institute ARDS ClinicalNetwork, or ARDSNet, ALVEOLI Study,which showed improved survival rates inpatients mechanically ventilated using lowtidal volumes. From this study, lung protec-tive strategies were derived.
The goal of lung protective strategies isto protect the lungs from overdistension(volutrauma) and end-expiratory collapse(atelectrauma) by using a low tidal volume,pressure-limited approach with low or mod-
erately high positive end-expiratory pressure(PEEP) (see Why high ventilator settings areout). An initial tidal volume of 8 mL/kg isselected and then adjusted every 2 hoursbased on peak plateau pressure (the measureof pressure in the smaller airways and alve-oli). Ideal peak plateau pressure is less than30 cm H2O. The goal is to titrate the tidal vol-ume to 6 mL/kg. In addition to adjusting thetidal volume, FiO2 and PEEP are titrated toachieve an oxygen saturation level of 88%to 95% or a PaO2 value of 55 to 80 mm Hgat the lowest possible FiO2, according toARDSNet. PEEP should be kept between 5and 20 cm H2O.
Although a gold standard medication reg-imen for ARDS has yet to be developed,antibiotic therapy is often used in the treat-ment of sepsis-related ARDS or to treat con-firmed or suspected underlying infection. Adiuretic may be used to increase renal excre-tion of water, which decreases pulmonaryinterstitial and alveolar edema. A mechani-cally ventilated patient may need to besedated. If sedation doesn’t prevent thepatient from “fighting” the ventilator, a neu-romuscular blocking agent may be consid-ered. The administration of fluids in patientswith ARDS has been examined and stillremains somewhat controversial. The debatecenters around the need for fluid to achievehemodynamic stability versus the fact thattoo much fluid may result in worsened pul-monary edema and pulmonary hypertension.
Nutritional sup-port is critical for thepatient with ARDS.Because metabolicdemand is high, hiscaloric needs will beincreased. Enteralnutrition is pre-ferred; however,parenteral nutritionmay also be consid-ered. Adequate calo-ries and proteinshould be provided,
www.NursingMadeIncrediblyEasy.com November/December 2009 Nursing made Incredibly Easy! 37
Criteria fordiagnosis ofARDS• Occurrence of an acute lung injury ora history of systemic or pulmonary riskfactors• Acute onset of respiratory distress• Diffuse, bilateral infiltrates on chest X-ray • Severe refractory hypoxemia (P/F ratio ofless than 200 mm Hg) • No clinical evidence of left-sided heart failure
sheet
cheat
memory joggerUse the acronymARDS to remem-ber key treatments.Antibiotics (if bacterial infectionis present)Respiratory sup-portDiureticsSituate the patientin the prone position

38 Nursing made Incredibly Easy! November/December 2009 www.NursingMadeIncrediblyEasy.com
including polyunsaturated fatty acids suchas gamma linolenic acid, which can assist indecreasing platelet aggregation and the pro-duction of pro-inflammatory agents. Enteralnutrition formulas have been developed thatprovide a large amount of fat calories ratherthan carbohydrates because the breakdownof carbohydrates results in a surplus of car-
bon dioxide. Remember, the patient’sinjured lungs are already workingovertime to get rid of carbon
dioxide.Prone positioning is a treat-
ment modality that can be usedfor mechanically ventilated
patients with ARDS who requirehigh FiO2 levels. Although it may
potentially trigger complica-tions, such as pressure ulcers,corneal abrasions, and brachialnerve injury, prone positioningcan facilitate blood flow to
areas of the lungs that are mildly injured andbetter oxygenated than those areas that areseverely injured. It may also help diaphragmmovement. It’s recommended that pronepositioning be considered early in the
course of treatment.Additional researchis needed to evalu-ate whether pronepositioning maydecrease ventilatordays and mortalityrates.
Permissive hyper-capnia—theallowance of highlevels of carbondioxide in thebloodstream—is anewer managementstrategy for ARDS.It has been shownto reduce lung injuryand is thought toprovide a protectivemechanism against
injury from inflammation. Permissivehypercapnia is achieved by setting low tidalvolumes on the ventilator. Research is ongo-ing to determine at what pH the best out-comes are achieved; currently, the patient’spH is allowed to reach levels as low as 7.2.
What’s your role?A patient with ARDS is critically ill and re-quires close monitoring in the ICU. Becauseyour patient’s condition could quickly be-come life-threatening, frequent assessmentof his status, including arterial blood gasvalues and hemodynamic parameters, andevaluation of the effectiveness of treatmentare necessary. But what else can you do?
Encourage frequent coughing if yourpatient can cough, which will help loosenexcessive airway mucus and maintain openalveoli. If he can’t cough, you can suction theairway if your assessment determines it’sneeded. If he’s being mechanically ventilated,be sure to hyperventilate and hyperoxy-genate him following your facility’s protocolbefore suctioning the airway. Keep suction-ing times as short as possible (less than 10 to15 seconds), make as few passes with the suc-tion catheter as possible (maximum of twosuction passes), and don’t interrupt PEEP.
Frequent turning and repositioning hasbeen found to improve ventilation and per-fusion in the lungs and enhance secretiondrainage. If prone positioning is being usedfor your patient, closely monitor hisresponse and for deterioration in oxygena-tion: Moving him from the supine positionto the prone position can lead to changes inhemodynamic stability. Be alert to areas ofpressure while your patient is in the proneposition, including the knees, face, andabdomen. Apply eye lubrication as orderedto prevent corneal abrasions. Use foam sup-port pillows to support your patient’s headand face, chest, pelvis, genitals, and dorsa ofthe feet to reduce the chance of skin break-down. And take care not to overextend hisshoulders to reduce the chance of brachialplexus injury.
Why high ventilatorsettings are outHistorically, ventilator therapy for ARDS con-sisted of high tidal volumes (10 to 12 mL/kg)with high PEEP (20 to 25 cm H2O) to improveoxygen delivery. But high airway pressurescommonly caused patients to develop pneu-mothorax (barotrauma) and decreased venousreturn contributed to decreased cardiac output.
Research has shown that high tidal volumesand PEEP levels significantly overdistend thealveoli (volutrauma), which triggers release ofinflammatory cytokines and decreases surfac-tant production. In ARDS, these effects exacer-bate the underlying disease process.
The current ventilation strategy is to deliver alow tidal volume and low to moderately highPEEP to keep the alveoli open and diminish thenegative effects of high-pressure settings.
How on Earth didyou guys get so
tangled up?

Monitor your patient for signs and symp-toms of cardiovascular compromise, partic-ularly a decreased cardiac output, whichmay be caused by decreased venous returnor because of positive pressure ventilation.Be alert for changes in BP; decreased pulseintensity, oxygen saturation, or urinary output; and mental status changes. Alsomonitor his lab values, especially the hemo-globin level because an adequate amount ofhemoglobin is needed to carry oxygen tothe tissues.
Your patient will be extremely anxious andagitated because of increasing hypoxemia anddyspnea. It’s important to decrease his anxi-ety because anxiety increases heart rate andmyocardial oxygen demand. Administeranalgesia and sedation as indicated to opti-mize patient comfort and reduce anxiety.
He’ll also be at risk for developing hospi-tal-acquired conditions from invasivedevices, such as ventilator-associated pneu-monia, catheter-related bloodstream infec-tion, and catheter-associated urinary tractinfection. Follow the CDC’s guidelines forproper hand hygiene to help prevent infec-tion. To help prevent VAP, implement theInstitute for Healthcare Improvement’s ven-tilator bundle: Elevate the head of the bedfrom 30 to 45 degrees to prevent aspiration,administer peptic ulcer disease prophylaxisto decrease the risk of aspiration and to pro-tect against a greater inflammatory responseif aspiration does occur, use daily sedationvacations and assess the patient’s readinessfor extubation, and provide deep veinthrombosis prophylaxis to decrease the riskof venous thromboembolism.
Looking toward the futureMany new treatments are still being stud-ied, including:• continuous lateral rotational therapy—involves placing the patient in a bed thatturns or repositions him from one side tothe other; it’s recommended that rotationaltherapy be performed at least 18 hours/dayfor optimal effectiveness
• partial liquid ventilation—involves grad-ually filling the lungs with a fluid calledperfluorocarbon, which is believed to helpcarry oxygen to areas of the lungs that arefilled with fluid and other substances andrid the lungs of harmful substances that arepreventing the alveoli from opening; the pa-tient must be sedated for this treatment andalthough it seems promising, improvementin mortality rates hasn’t been seen so far• corticosteroids—the use of steroids to re-duce inflammation in ARDS remains con-troversial; however, recent studies haveshown some benefit to low-dose corticos-teroid administration• inhaled NO gas—NO may be used as arescue therapy for refractory hypoxemia inARDS because it relaxes vascular smoothmuscle, reducing pulmonary hypertensionand improving oxygenation; the benefitsgenerally don’t last more than 24 hours• surfactant replacement therapy—thistherapy has been used successfully inneonates with respiratory distress syn-drome but the effectiveness in adults remains unclear; the use of aerosolized sur-factant for adults continues to be studied.
A mystery still being solvedAs we learn more about the complexprocesses associated with ARDS, we’ll beable to develop new strategies to help de-crease morbidity and mortality in this pa-tient population. Meanwhile, the use oflung protective strategies is still the most ef-fective way to manage patients with ARDS.Although the prognosis isn’t always posi-tive, your patient will have a better chanceat survival with your help. ■
Learn more about itARDS Support Center. Understanding ARDS. http://www.ards.org/learnaboutards/whatisards/brochure/.
Bosma K, Fanelli V, Ranieri VM. Acute respiratory dis-tress syndrome: update on the latest developments in basic and clinical research. Curr Opin Anaesthesiol. 2005;18(2):137-145.
Gallagher JJ. Taking aim at ARDS. Nursing2009. 2009;39(10):42-48.
www.NursingMadeIncrediblyEasy.com November/December 2009 Nursing made Incredibly Easy! 39
Whew! What a relief!

Girand TD, Bernard GR. Mechanical ventilation in ARDS:a state-of-the-art review. Chest. 2007;131(3):921-929.Institute for Healthcare Improvement. Implementingthe ventilator bundle. http://www.ihi.org/IHI/Topics/CriticalCare/IntensiveCare/Changes/ImplementtheVentilatorBundle.htm.Jacobs M. Ease the stress of managing ARDS. Nursingmade Incredibly Easy! 2005;3(1):6-18.
Mayo Clinic. ARDS. http://www.mayoclinic.com/health/ards/DS00944.
National Heart Lung and Blood Institute. What is ARDS?http://www.nhlbi.nih.gov/health/dci/Diseases/Ards/Ards_WhatIs.html.
National Heart Lung and Blood Institute ARDS Network.ALVEOLI. http://www.ardsnet.org/studies/alveoli.
Pathophysiology Made Incredibly Visual! Philadelphia, PA:Lippincott Williams & Wilkins;2008:44-45.
Peter JV, John P, Graham PL, Moran JL, George IA,Bersten A. Corticosteroids in the prevention and treat-
ment of acute respiratory distress syndrome(ARDS) inadults: meta-analysis. BMJ. 2008;336(7651):1006-1009.
Phua J, Stewart TE, Ferguson ND. Acute respiratory dis-tress syndrome 40 years later: time to revisit its definition.Crit Care Med. 2008,36(10):2912-2921.
Porth CM, Matfin G. Pathophysiology: Concepts of AlteredHeath States. 8th ed. Philadelphia, PA: Lippincott Williams& Wilkins; 2009:732-733.
Santacruz JF, Diaz Guzman Zavala E, Arroliga AC. Up-date in ARDS management: recent randomized controlledtrials that changed our practice. Cleve Clin J Med. 2006;73(3):217-219,223-225.
Smeltzer SC, Bare BG, Hinkle JL, Cheever KH. Brunner &Suddharth’s Textbook of Medical-Surgical Nursing. 11th ed.Philadelphia, PA: Lippincott Williams & Wilkins; 2008:656-659.
Zambon M, Vincent JL. Mortality rates for patients withacute lung injury/ARDS have decreased over time. Chest.2008;133(5):1120-1127.
40 Nursing made Incredibly Easy! November/December 2009 www.NursingMadeIncrediblyEasy.com
For more than 23 additional continuing education articles related to respiratory topics, go toNursingcenter.com/CE.
The moreCE, themerrier!
Earn CE credit online: Go to http://www.nursingcenter.com/CE/nmie and receive a certificate within minutes.
INSTRUCTIONS
Unraveling the mystery of ARDSTEST INSTRUCTIONS
• To take the test online, go to our secureWeb site at http://www.nursingcenter.com/
CE/nmie.• On the print form, record your answers in thetest answer section of the CE enrollment formon page 53. Each question has only one correctanswer. You may make copies of these forms.• Complete the registration information andcourse evaluation. Mail the completed form andregistration fee of $21.95 to: Lippincott Williams &Wilkins, CE Group, 2710 Yorktowne Blvd., Brick,NJ 08723. We will mail your certificate in 4 to 6weeks. For faster service, include a fax numberand we will fax your certificate within 2 businessdays of receiving your enrollment form.• You will receive your CE certificate of earned contact hours and an answer key to review yourresults.There is no minimum passing grade.• Registration deadline is December 31, 2011.
DISCOUNTS and CUSTOMER SERVICE
• Send two or more tests in any nursing journal published by Lippincott Williams &Wilkins together and deduct $0.95 from the price of each test.• We also offer CE accounts for hospitals and other health care facilities on nursingcenter.com. Call 1-800-787-8985 for details.
PROVIDER ACCREDITATION
Lippincott Williams & Wilkins, publisher of Nursing made Incredibly Easy!, will award2.3 contact hours for this continuing nursing education activity.
Lippincott Williams & Wilkins is accredited as a provider of continuing nursing edu-cation by the American Nurses Credentialing Center’s Commission on Accreditation.
This activity is also provider approved by the California Board of Registered Nursing,Provider Number CEP 11749 for 2.3 contact hours. Lippincott Williams & Wilkins is alsoan approved provider of continuing nursing education by the District of Columbia andFlorida #FBN2454. LWW home study activities are classified for Texas nursing continu-ing education requirements as Type I. Your certificate is valid in all states.
The ANCC’s accreditation status of Lippincott Williams & Wilkins Department ofContinuing Education refers only to its continuing nursing educational activities anddoes not imply Commission on Accreditation approval or endorsement of any com-mercial product.
Recommended