Case report
Adams–Oliver syndrome: new evidence in variable
expressivity?
Meenakshi Girish*, MD, Nilofer Mujawar, MD, Umakant Anekar, MD and SheetalBhattad, MD
From the Department of Pediatrics, NKP
Salve Institute Of Medical Sciences &
Research Center, Nagpur, Maharashtra,
India
Correspondence
Dr. Meenakshi Girish
101, Shubham Enclave
Darda Marg
Rahate Colony
Nagpur 440022, Maharashtra
India
E-mail: [email protected]
Funding source: None.
Conflict of interest: None.
Introduction
Adams–Oliver syndrome (AOS) is characterized by con-genital absence of skin, known as aplasia cutis congenita(ACC), usually limited to the scalp vertex and terminaltransverse limb defects (TTLD). The disorder follows anautosomal dominant pattern of inheritance. Togetherwith TTLD, ACC constitutes the cardinal feature of AOS.We are reporting for the first time a scalp lesion that is
not ACC but rather congenital focal partial alopecia inan otherwise classical case of AOS.
Case report
An otherwise healthy 4-year-old boy, only child of noncon-sanguineous parents, was referred to us for limb defects.Pregnancy and birth were unremarkable. Examination of
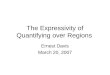
(a) (b)
Figure 1 (a) Top view of scalp of son, showing focal partial alopecia. Normal scalp tissue, no scar, but sparse vellus hair in theregion of midscalp. (b) Top view of scalp of father, showing focal cicatricial scar (area outlined). Father also had androgeneticalopecia
ª 2013 The International Society of Dermatology International Journal of Dermatology 2014, 53, 891–893
891

the scalp revealed patchy partial alopecia at the vertex,with hair that was soft (vellus), thin, and lightly pigmentedas compared with the rest of scalp hair. This patch wasreportedly completely bald at the time of birth. The patchmeasured about 5 9 5 cm, and there was no scar, distortedhair growth around the margin (hair collar sign), or under-lying bone defect (Fig. 1a). The right foot was malformed,and the entire left foot was absent (Fig. 2a). His handswere normal. There was a diffuse bilaterally symmetricalmottled reticulated pattern on the entire skin (Fig. 3),which had been present since birth. Systemic examinationwas normal, and there was no intellectual deficit. Thechild’s father was 35 years old and had cicatricial focal
alopecia of the scalp on the vertex measuring about5 9 8 cm (Fig. 1b), with parchment-like scar tissue but nobony defect.Both feet were absent, and both hands were malformed
(Fig. 2b). He was being treated for hypertension secondaryto coarctation of the aorta. The father did not have cutismarmorata, and there was no other systemic abnormality.There was no family history of similar complaints.
Discussion
The combination of ACC and TTLD is enough to make adiagnosis of AOS,1 though it can also be associated withextensive lethal anomalies of internal organs, includingthe central nervous, cardiopulmonary, gastrointestinal,and genitourinary systems. Limb defects, the most com-mon feature of this disease, are usually asymmetric, thelower limbs being more susceptible than the upper limbs.2
The extent of the defect could range from just brachy orsyndactyly to complete absence of part of a limb. Scalpdefects are the second most frequent finding in AOS3 andare usually in the form of ACC and rarely associated withsignificant underlying bony defect with resultant compli-cations.4 Focal partial alopecia without epidermal defecthas never been described. Our patient had all the classicfeatures of AOS but not ACC. Instead, there was a patchof sparse and altered hair growth from a normal lookingscalp epidermis. Great variability in expression of thissyndrome has been reported, but the scalp defect hasalways been an atrophic or hypertrophic scar covered byan epidermal membrane.5 This is the first time we have
(a) (b)
Figure 2 (a) Lower limbs of the son showing absent left foot and deformed right foot with hypoplastic toes. (b) Lower limbsand hands of father. Both feet are absent. Right first four fingers are absent and the thumb is short with hypoplastic nail. Indexand middle fingers of the left hand are hypoplastic, all the other fingers are short with poorly formed nails
Figure 3 Cutis marmorata telangiectatica congenita. Thinreticulated pattern on the skin covering the trunk and armsof the son
International Journal of Dermatology 2014, 53, 891–893 ª 2013 The International Society of Dermatology
Case report New evidence in variable expressivity? Girish et al.892

found a scalp lesion that is not the typical scar tissue ofan ACC but could very well represent a minor variantnot severe enough to cause scarring.This syndrome is known to manifest with a wide range
of interfamilial and intrafamilial variation.6 Both fatherand son have terminal limb defects, but while the son hascutis marmorata telangiectatica congenita, father hasACC and coarctation of the aorta. An abnormality in thesmall vessel wall structure occurring during embryogene-sis has been proposed as a pathogenic event responsiblefor the various manifestations.7 It is still difficult toexplain all the clinical presentations reported so far andthe focal partial alopecia seen in our patient with a singlepathogenetic mechanism, and the various patterns ofinheritance described in literature continue to pointtowards an etiological heterogeneity.
References
1 Snape KMG, Ruddy D, Zenker M, et al. The spectra ofclinical phenotypes in aplasia cutis congenita and terminaltransverse limb defects. Am J Med Genet 2009; 149A:1860–1881.
2 Seo JK, Kang JH, Lee HJ, et al. A case of adams–oliversyndrome. Ann Dermatol 2010; 22: 96–98.
3 Narang T, Kanwar AJ, Dogra S. Adams-Oliver syndrome:a sporadic occurrence with minimal disease expression.Pediatr Dermatol 2008; 25: 115–116.
4 Margileth AM. Dermatologic conditions. In: Avery GB,Fletcher MA, MacDonald MG, eds. Neonatology, 5th edn.Philadelphia: Lippincott Williams and Wilkins, 1999:1323.
5 Trobs RB, Barenberg K, Heminghaus M, et al. Herniationof the brain after conservative treatment of a largecongenital skull defect in an infant with Adams-Oliversyndrome. J Pediatr Surg 2010; 45: 2064–2067.
6 Jaeggi E, Kind C, Morger R. Congenital scalp and skulldefects with terminal transverse limb anomalies (Adams-Oliver syndrome): report of three additional cases. Eur JPediat 1990; 149: 565–566.
7 Swartz EN, Sanatani S, Sandor GG, Schreiber RA.Vascular abnormalities in Adams-Oliver syndrome: causeor effect? Am J Med Genet 1999; 82: 49–52.
ª 2013 The International Society of Dermatology International Journal of Dermatology 2014, 53, 891–893
Girish et al. New evidence in variable expressivity? Case report 893
Recommended