
88 Clin Pathol 1992;45:898-901
Nasopharyngeal carcinoma in situ innasopharyngeal carcinoma
C W Chan, J M Nicholls, J S T Sham, P Dickens, D Choy
AbstractAims: To assess the presence ofcarcinomain situ (CIS) in patients with nasopharyn-geal carcinoma (NPC) and to see if thenumber of biopsy sites facilitates detec-tion of CIS.Methods: Formalin fixed, paraffin waxembedded biopsy specimens (n = 285)from 187 patients with NPC in 1987 werestudied for the presence of CIS as well asfor the histological assessment of thesubtype of CIS.Results: Fifteen (8.0%) patients had CIS,representing 8-3% of all new patients withNPC and 11*6% ofpatients with persistentdisease or relapse. CIS was undifferen-tiated or poorly differentiated, no cases ofwell differentiated squamous celi CISwere identified. There was no significantdifference in the incidence of CIS whenmultiple endoscopic biopsy specimenswere taken rather than single forcepsbiopsy specimens.Conclusions: CIS can only be identified ina few patients with NPC largely because oflate presentation with advanced disease atthe time of diagnosis and the focal natureof the dysplastic process. The presence ofdysplasia in relapses ofNPC suggests thatthese tumours may be second growthsrather than regrowths of a primarytumour.
(7 Clin Pathol 1992;45:898-901)
yngeal carcinoma in situ using the two biopsytechniques was also assessed.
MethodsThe slides of all biopsy cases diagnosed in1987 as undifferentiated carcinoma, anaplasticcarcinoma, and squamous cell carcinoma fromthe nasopharynx were retrieved and examined.If slides had faded they were restained andextra sections were cut if necessary. Thespecimens had all been fixed in 10% formalin,embedded in paraffin wax, and the slidesstained with haematoxylin and eosin. Thepresence or absence of tumour was confirmed.Material from this period had been used in aprevious study.4 If more than one biopsyspecimen was taken from the nasopharynxduring an examination it was classified as amultiple biopsy specimen. For the purpose ofthis study the presence of carcinoma in situwas characterised by the presence of cyto-logical and architectural atypia affecting thewhole thickness of the epithelium. Alsoassessed was whether such change was con-tiguous with the invasive tumour. The assess-ment was initially performed by onepathologist (iN). To check for interobservererror the cases diagnosed as CIS were ran-domly distributed among those not showingCIS and shown to two other pathologists(CWC, PD). A Gomori reticulin stain wasperformed to confirm the confinement ofatypia to the epithelium and to exclude inva-sion whenever necessary.
Department ofPathology, Universityof Hong KongCW ChanJ M NichollsP DickensDepartment ofRadiation OncologyJ ST ShamRadiotherapy andOncology Division,Queen Mary HospitalD ChoyCorrespondence to:Dr J M Nicholls,Department of Pathology,University of Hong Kong,Hong KongAccepted for publication16 April 1992
In 1837 Durand-Fardel reported a case ofnasopharyngeal carcinoma (NPC). One of thefirst histological classifications was detailed in1921 by Schmincke and by Cappell in 1934and 1938. The high prevalence of NPC inHong Kong Chinese, was reported by Digby etal in 1940-1941.lThe World Health Organisa-tion classification introduced in 1978 has beenwidely accepted and used,2 providing a usefulframework for classifying NPC and comparingthe results. However, precursor lesions forNPC indicative of carcinoma in situ (CIS)have not been studied in depth and there havebeen only a few reports looking at the pathol-ogy of these lesions. This study was thereforeundertaken to look at the prevalence of naso-pharyngeal carcinoma in situ occurring incases of NPC seen within one year at ourhospital. As this was a period when bothmultiple endoscopic and single forceps biopsyspecimens were used for the diagnosis ofNPC,' the efficacy of detecting nasophar-
ResultsFrom January to December 1987 a total of 285biopsy specimens from 187 patients werepositive for malignancy. Of these 187 patients,144 (77%) had a total of 228 biopsy specimensfrom primary growths for the initial assessmentand staging of the tumour; 43 (23%) patientshad a total of 57 specimens to assess tumourrelapse or residual disease, 12 weeks after thecompletion of external radiation treatment. Ofthe 228 specimens for initial tumour assess-ment, 181 (79-3%) were multiple and 47(20 6%) were single. For the 57 biopsy speci-mens assessed for relapse or residual tumour,38 (67%) were multiple and 19 (33%) weresingle.On initial examination a total of 21 speci-
mens from 18 patients had nasopharyngealcarcinoma in situ of which 15 were taken fromprimary growths and six were taken for theevaluation of relapse or persistent tumour.
898
on Septem
ber 17, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.45.10.898 on 1 O
ctober 1992. Dow
nloaded from

Nasopharyngeal carcinoma in situ in nasopharyngeal carcinoma
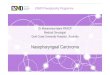
Figure 1 Carcinoma in situ of a poorly differentiated type resembling transitional celcarcinoma (haematoxylin and eosin).
Following a review by the two other patholo-gists (PD, CWC) the distinction between insitu change and tumour replacement of theepithelium was considered too difficult tomake in two cases from primary growths and inone from a recurrent tumour. These were
excluded so that in the final analysis there were15 patients with CIS-1 1 with primarygrowths and four with relapse. One patient hadnasopharyngeal carcinoma in situ in the pre-
Figure 2 Carcinoma in situ of an undifferentiated type (haematoxylin and eosin).
treatment biopsy specimens and in the recur-rent tumour. CIS was therefore present in8-0% of the patients with NPC. Eleven of 144(7 6%) of all new patients with NPC hadnasopharyngeal carcinoma in situ and five of43 (11 6%) with relapse or persistent tumourshowed the presence of nasopharyngeal carci-noma in situ. Of all the 219 multiple biopsyspecimens, CIS was present in 14 (6 4%) andin four (6-1%) of the 66 single biopsy speci-mens. Two patients with both single andmultiple biopsy specimens taken had CIS.There were no cases of well differentiatedsquamous cell CIS. Seven of our cases were oftransitional or poorly differentiated type CIS(fig 1) and eight were analogous with anundifferentiated CIS using WHO criteria (fig2), with an attenuated form of CIS identified(fig 3). Continuity of the CIS with tumourcould only be confirmed in six cases.
DiscussionThere are many types of neoplasm which mayarise in the nasopharynx and these reflect thevariety ofnormal tissue elements in this region.The most common form of cancer in this areais NPC.5 The epithelial nature of this tumourhas been well characterised by electron micros-copy6 as well as by immunohistochemistry.'There is little doubt that NPC originates in theepithelium of the nasopharynx even thoughcontinuity oftumour with the epithelium is notalways seen.8 Crypt epithelial cells may have arole in NPC as they have similar histologicalfeatures to undifferentiated carcinoma.Though we detected no single criterion todifferentiate dysplastic from normal epithe-lium, we found that in the latter condition thenuclear size and irregularity, prominence ofnucleoli, decrease of lymphocyte numbers andabsence of differentiation in the adjacent epi-thelium allowed attenuated dysplasia to bediagnosed in two cases.There has been considerable disagreement
and discussion on the histopathology of NPC,but the amount of information on precursorlesions is, by comparison, minimal. One of thefirst reports on nasopharyngeal carcinoma insitu was byTeoh in 1957' in which he analysed31 necropsies between 1949 and 1955, withmalignant growths in the nasopharynx. Thematerial is currently being reanalysed usingimmunohistochemical techniques. In one ofhis patients (case 6) he noted that as well as aprimary growth in the left tubal elevationsections; ". . . other parts of the nasopharynxreveal carcinoma in situ in the epitheliumlining a crypt in the posterior wall .. ." Unfor-tunately there were no photographs to docu-ment this lesion. In 1962 Liang et al looked at500 fresh cases of NPC in the Chung ShanMedical College (in the province of Guang-dong in southern China). Of their 500 biopsycases 16 (3 2%) showed precancerous change,17 (3-4%) showed CIS, and 34 (7 2%) showedearly invasive carcinoma. No mention wasmade, however, of these changes in necropsymaterial from cases without NPC.9Wieland referred to nasopharyngeal carcin-
899
on Septem
ber 17, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.45.10.898 on 1 O
ctober 1992. Dow
nloaded from

Chan, Nicholls, Sham, Dickens, Choy
Figure 3 Carcinoma insitu of an undifferentiatedtype occurring inattenuated epithelium(haematoxylin and eosin).
oma in situ in American referral cases ofNPC8in which he stated that in keratinising squa-mous cell carcinoma the tumour always occur-red on the surface of the epithelium fromwhich it originated. An apparently in situcomponent was frequently observed. By com-parison, it was unusual to see an apparently insitu component in non-keratinising tumours;moreover, when this was seen it was difficult toprove that it represented true in situ carcinomaand not epithelial replacement from an under-lying tumour.
For several years Chinese publications havereferred to the precursor lesions of NPC.' "However, they use different terminologiesfrom those used in the West and their termin-ologies have mainly been based on the mor-phology seen in animal experiments. There arethree proposed gradings of abnormal findingsin the nasopharynx-namely, simple hyper-plasia or metaplasia, atypical hyperplasia ormetaplasia, and carcinoma in situ. This classifi-cation is therefore similar to the preneoplasticlesions seen in the bladder. Most Westernresearchers would consider carcinoma in situas atypia involving the whole thickness of theepithelium when applied to squamous epith-elium, but Li et al.'° state that CIS of thenasopharynx does not always involve the wholethickness of the epithelium and may be mani-fest as a few atypical, morphologically abnor-mal cancer cells among hyperplastic ormetaplastic tissue. The results of anotherChinese monograph" found 98 cases (8 6%)of CIS/microinvasive carcinoma among 1136cases of NPC biopsy specimens.The first article devoted entirely to naso-
pharyngeal carcinoma in situ was only publi-shed in 1986.12 The authors found anincidence of 2-3% in 2742 biopsy specimens,
and of these, the abnormal cells occupied thewhole thickness of the epithelium in 85A4% ofcases while in 14-9% of cases the abnormalcells occupied only part of it. Most of thelesions were found in the surface epitheliumwhile only 1 8-4% were seen in the cryptepithelium. In the cases of nasophryngealcarcinoma in situ there was significantly morenuclear DNA than in normal and metaplasticsquamous epithelium.
In an initial report'3 and later in a mono-graph'4 Lee et al compared the nasopharyngealin situ and premalignant lesions to those in thecervix and proposed the term nasopharyngealintraepithelial neoplasia (NPIN), with threegrades ranging from NPIN I to NPIN III.Their data showed that 73-3% of cases ofNPCwere NPIN and 12-3% of surgical biopsyspecimens from the normal nasopharynx wereNPIN. They also found NPIN in 1-5% of aseries of necropsy cases.Our results of 8-0% are closer to the findings
of Zong'2 and Liang9 than those of Lee.'4 Thediscrepancy could be that we only looked atCIS, which involves the whole thickness of theepithelium, while Lee looked at all cases withepithelial atypia. Clearly, pathologists havebeen unable to agree on terminology, and whatis called dysplasia by some may be called atypiaby others." We therefore chose to concentrateon looking at the high grade dysplastic lesionsand found that there was reliable interobserverconcordance for the diagnosis of such lesions.The reason for looking at nasophyaryngealcarcinoma in situ and classifying it is morethan an academic exercise: a recent study onCIS in a selected population showed that thecategorisation of precursor lesions remains animportant aspect in the early detection ofNPC.16 Though Lee mentioned the presence
900
on Septem
ber 17, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.45.10.898 on 1 O
ctober 1992. Dow
nloaded from

Nasopharyngeal carcinoma in situ in nasopharyngeal carcinoma
of koilocytic changes in biopsy material,'4other authors have not mentioned this, and wefound no convincing cases in which we couldidentify this abnormality in our material whereNPC was present.Our study is the first to use the multiple
biopsy technique to look at the presence orabsence of tumour and CIS. As Zong et almentioned in their earlier paper, by the natureof its anatomical location the nasopharynx isnot easily accessible and the same degree ofaccuracy cannot be applied to assessing naso-pharyngeal carcinoma in situ as in the cervix.'2Weiland also stated that the small size of biopsymaterial did not facilitate an accurate, con-sistent, and meaningful classification of NPC.Though no mention was made of the site of thebiopsy in any of the preceding reports, weassume that they were taken straight from thetumour site and not adjacent to it. For the yearstudied, about 80% of the biopsy specimensfor the initial assessment of NPC were multi-ple; for relapses the single biopsy specimensdetected 33%. This is because the pretreat-ment multiple biopsy technique was con-sidered at that time to be important in thestaging of the tumour17 and the posttreatmentbiopsy specimen was just to document thepresence or absence of tumour. We found CISin 6-8% of the multiple biopsy specimens andin 6-1% of the single specimens; this differencewas not significant. The multiple biopsy tech-nique may be advantageous for staging pur-poses but it does not promise better detectionof CIS.The prevalence of nasopharyngeal carci-
noma in situ associated with invasive NPC ismuch less than CIN which has been used bysome as a model for the nasopharynx. Weattribute this to two reasons: first, we wereunable to visualise the nasopharynx in as greata detail as the cervix. Secondly, and moreimportantly, NPC tends to present at a laterstage than carcinoma of the cervix and most ofthe biopsy specimens of tumour do not showsufficient epithelium because this has beenreplaced by tumour. It should also be appre-ciated that CIS is an evolving lesion and thebiopsy specimen represents one stage in thedeveloping lesion. The tumour is also differentfrom the cervical lesion in that it does notappear to go through all the stages of CISbefore frank invasion develops. In this respectit is perhaps better to think of the nasophar-yngeal mucosa as being more similar in beha-viour to bladder rather than cervical mucosa.One very interesting point of our study was
that five cases of nasopharyngeal carcinoma insitu were found among the cases of relapse or
disease persisting 12 weeks after radiotherapyhad been completed. Four of these cases werein relapse while one was persistent disease. Ifthe case of persistent disease is removed, therewere four cases occurring in 24 patients withrelapse (16-7%), a figure higher than that ofthe primary cases. Traditionally, relapse hasbeen considered regrowth of tumour that hasnot been eradicated, but our findings suggestthat it could represent a second growth.Further study is being conducted in this area.
1 TeohTB. Epidermoid carcinoma of the nasopharynx amongChinese: A study of 31 necropsies. Jf Pathol Bacteriol1957;58:451-65.
2 Sham JST, WeiWI, KwanWH, Chan CW, Choi PHK, ChoyD. Fibreoptic endoscopic examination and biopsy indetermining the extent of nasopharyngeal carcinoma.Cancer 1989;64: 1838-42.
3 Shanmugaramam K, Sobin LH. Histological types of upperrespiratory tract tumours. In: International histologicalclassification of tumours. No 19. Geneva: WHO 1978.
4 Nicholls JM, Sham JST, Chan CW, Choy D. Radiationtherapy for nasopharyngeal carcinoma. Histologicalappearances and patterns of tumour regression. HumPathol 1992;23:742-7.
5 Shanmugaratnam K. Histological types of nasopharyngealcarcinoma. In: de-The G, Ho Y, eds. Proceedings ofinternational symposium on nasopharyngeal carcinoma:Etiology and Control. Lyon: International Agency forResearch on Cancer, 1978:3-12.
6 Prasad U. Cells of origin of nasopharyngeal carcinoma: anelectron microscopic study. J Laryngol Otol 1974;88:1087-94.
7 Oppedal BR, Bohler PJ, Marton PF, Brandtzaeg P. Carcin-oma of the nasopharynx. Histopathological examinationwith supplementary immunohistochemistry. Histopath-ology 1987;11:1161-9.
8 Wieland LH. The histological spectrum of nasopharyngealcarcinoma. In: de-The G, Ho Y, eds. Proceedings ofinternational symposium on nasopharyngeal carcinoma:Etiology and Control. Lyon: International Agency forResearch on Cancer, 1978:41-50.
9 Liang PC, Chen CC, Chu CC, Hu YF, Chu HM, TsungHM. The histologic classification, biological charac-teristics and histogenesis of nasopharyngeal carcinoma.Chinese MedJ 1962;81:629-58.
10 Li CC, Pan QC, Chen CC. Hyperplasia and metaplasia inthe nasopharynx. In: U CC, Pan QC, Chen CC, eds.Nasopharyngeal carcinoma, clinical and laboratoryresearches. Gwangzhao: Gwangdong Scientific TechnicalPublications, 1983:143-53 (in Chinese).
11 ZongYS. Histopathology of nasopharyngeal carcinoma. In:Au PC, Zheng Y, eds. Aetiology and pathophysiology ofnasopharyngeal carcinoma. Beijing: People's Health Pub-lication, 1983:65-75 (in Chinese).
12 Zong YS, Li QX. Histopathology of paracancerous naso-pharyngeal carcinoma in situ. Chinese Med J1986;99:763-71.
13 Lee JCK, Suen MWN. Intraepithelial neoplasia in mucosaof human nasopharyngeal carcinoma. In: Abstracts of theXII International Congress of the International Academy ofPathology and 7th World Congress ofAcademic and Environ-mental Pathology. Vienna: IAP, German Division,1986:148.
14 Lee JCK. Precancerous changes. In: van Hasselt, CA, ed.Nasopharyngeal carcinoma. Hong Kong: Chinese Univer-sity Press, 1991:37-45.
15 Krutchkoff DJ, Eisenberg E, Anderson C. Dysplasia of oralmucosa: A unified approach to proper evaluation. ModPathol 1991,4:.113-19.
16 Sham JST, WeiWI, ZongYS, Choy D, GuoY-Q,Yan L, LinZX, Ng MH. Detection of subclinical nasopharyngealcarcinoma by fibreoptic endoscopy and multiple biopsy.Lancet 1990;335:371-4.
17 Sham JST, WeiWI, Nicholls J, Chan CW, Choy D. Extent ofnasopharyngeal carcinoma involvement inside the naso-pharynx: lack of prognostic value or local control. Cancer1992;69:854-9.
901
on Septem
ber 17, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.45.10.898 on 1 O
ctober 1992. Dow
nloaded from
Recommended






![Nasopharyngeal Carcinoma [Ind] - Fix 19](https://img.pdfslide.net/doc/110x75/55cf9043550346703ba47221/nasopharyngeal-carcinoma-ind-fix-19.jpg)








