Clinical and Visual Outcomes of Children With Peters Anomaly
Asim Ali, MD, FRCSC
Uri Elbaz, MD
Hermina Strungaru, MD, PhD
Kamiar Mireskandari, MBChB, FRCSEd,
FRCOphth, PhD.
Department of Ophthalmology and Vision Sciences, The Hospital for Sick Children, University of Toronto, Toronto, Ontario, CanadaThe authors have no financial interest to disclose

PURPOSE The purpose of this study is to investigate the
visual and clinical outcomes in a large Peters anomaly cohort stratified by disease severity and selective treatment modalities in order to improve management of this disease.
Our study is the first to include the visual and clinical outcomes of different treatment modalities for both traditional subtypes of the disease.

METHODS The charts of all patients diagnosed with Peters
anomaly from January 2000 to December 2012 were reviewed retrospectively.
For treatment purposes, patients were classified as Peters I or II, depending on lens involvement (please refer also to e-poster 17590 “Characterizing the Phenotypic Spectrum of Peters Anomaly: From Mild to Severe Disease”).
Patients were further classified depending on corneal opacity location and size.

METHODS Visual and clinical data were collected and
stratified per treatment modality chosen.
Visual outcomes included final best corrected distance visual acuity (CDVA) and the presence of nystagmus.
Clinical outcomes included incidence of glaucoma and PKP survival in transplanted eyes.

RESULTS Sixty eyes of 40 patients were included in the
study.
The mean patient age at presentation was 6.2±20.7 months (0.0-111.0 months) with a mean follow-up time of 75.8±52.9 months (12.1-225.3 months).

≥ 20/200n (%)
<20/200-CFn (%)
CF or HMn (%)
Mean CDVAlogMAR ± SD p-Value LP or NLP n (%) p-Value
Overall (n=59*) 33 (55.9) 9 (15.3) 4 (6.8) 0.9±0.7 13 (22.0)
Peters I (n=42) 27 (64.3) 8 (19.0) 2 (4.8) 0.8±0.60.2
5 (11.9)0.003
Peters II (n=17) 6 (31.6) 1 (5.3) 2 (10.5) 1.2±1.1 8 (42.1)
Unilateral (n=20) 10 (50.0) 3 (15.0) 3 (15.0) 1.1±1.00.16
4 (20.0)0.78
Bilateral (n=39) 23 (59.0) 6 (15.4) 1 (2.6) 0.8±0.5 9 (23.1)
Mild Peters I (n=7) 7 (100.0) 0 (0.0) 0 (0.0) 0.4±0.3 0 (0.0)
Moderate Peters I (n=9) 8 (88.9) 0 (0.0) 1 (11.1) 0.7±0.7 0 (0.0)
Severe Peters I (n=25) 12 (48.0) 8 (32.0) 1 (4.0) 1.0±0.6 4 (16.0)
Small opacity Type II (n=4) 2 (50.0) 1 (25.0) 0 (0.0) 0.9±0.5 1 (25.0)
Large opacity Type II (n=11) 4 (36.4) 0 (0.0) 2 (18.2) 1.4±1.3 5 (45.5)
Eyes with glaucoma (n=19) 5 (26.3) 7 (36.8) 3 (15.8) 1.5±0.90.00004
4 (21.1)0.9
Eyes without glaucoma (n=40) 28 (70.0) 2 (5.0) 1 (2.5) 0.6±0.5 9 (22.5)
Glaucoma Peters I (n=13) 2 (15.4) 6 (46.2) 1 (7.7) 1.5±0.70.0002
4 (30.8)0.01
No glaucoma Peters I (n=29) 25 (86.2) 2 (6.8) 1 (3.4) 0.6±0.5 1 (3.4)
Glaucoma Peters II (n=6) 3 (50.0) 1 (16.7) 2 (33.3) 1.5±1.20.17
0 (0.0)0.004
No glaucoma Peters II (n=11) 3 (27.3) 0 (0.0) 0 (0.0) 0.5±0.2 8 (72.7)
Final visual acuity stratified by disease severity and in relation to glaucoma.
*In one Peters II anomaly eye visual acuity was not obtained due to severe developmental delay. CDVA – corrected distance visual acuity

≥ 20/200
n (%)<20/200-CF
n (%)CF or HM
n (%)Mean CDVA logMAR ± SD
p-ValueLP or NLP
n (%)p-Value
Nystagmus n (%)
Obseravation (n=7) 7 (100.0) 0 (0.0) 0 (0.0) 0.4±0.3 0 (0.0) 2 (28.6)
Optical management (n=13) 10 (76.9) 1 (7.7) 1 (7.7) 0.7±0.6 1 (7.7) 4 (30.8)
Peters I (n=9) 8 (88.9) 0 (0.0) 1 (11.1) 0.7±0.70.8
0 (0.0)0.12
2 (22.2)
Peters II (n=4) 2 (50.0) 1 (25.0) 0 (0.0) 0.9±0.5 1 (25.0) 2 (50.0)
PKP (n=36) 16 (44.4) 8 (22.2) 3 (8.3) 1.1±0.8 9 (25.0) 30 (81.1)
Peters I (n=25) 12 (48.0) 8 (32.0) 1 (4.0) 1.0±0.60.4
4 (16.0)0.06
18 (72)
Peters II (n=11*) 4 (36.4) 0 (0.0) 2 (18.2) 1.4±1.3 5 (45.5) 12 (100)
No treatment (n=3) 0 (0.0) 0 (0.0) 0 (0.0) NA 3 (100.0) 2 (66.7)
Final visual acuity and nystagmus prevalence stratified by treatment modality
Causes of graft failure in 27 transplants of 12 eyes (12 primary and 15 repeat transplants)
Cause No of transplants (%)
Rejection 7 (25.9)
Limbal stem cell deficiency 5 (18.5)
Corneal ulcer 1 (4.0)
Uncontrolled glaucoma 4 (14.8)
Silicone oil 2 (7.4)
Retrocorneal membrane 4 (14.8)
Unknown 4 (14.8)
*In one Peters II anomaly eye in the PKP group visual acuity was not obtained due to severe developmental delay. Nystagmus data was available in all eyes. CDVA – corrected distance visual acuity. NA – not applicable .

Risk factor Hazarad ratio 95% CI p - Value
Laterality 0.93 0.26 – 3.38 0.91Iridocorneal adhesion 1.45 0.18 - 11.60 0.73Keratolenticular adhesion 2.91 0.81 – 10.40 0.13Vascularization 3.22 0.92 – 11.34 0.07Microphthalmos 3.69 1.06 – 12.82 0.04Donor size (>6mm) 2.44 0.08 – 1.33 0.19Donor age (> 40 years) 1.32 0.26 – 4.93 0.68Glaucoma 3.18 0.82 – 12.29 0.09Glaucoma surgery after 1st PKP 1.81 0.53 – 6.21 0.35Lens surgery 5.62 1.21 – 26.16 0.03lens surgery along with1st PKP 1.05 0.13 – 8.54 0.97Lens surgery after 1st PKP 4.77 1.26 – 18.07 0.02Peters Type I 0.27 0.08 – 0.90 0.03
Univariate analysis of preoperative and intraoperative variablesaffecting primary PKP survival.
Risk factor Odds ratio 95% CI p - Value
Laterality 0.82 0.24 - 2.84 0.75
Iridocorneal adhesion 0.51 0.09 - 2.92 0.45
Keratolenticular adhesion 0.33 0.09 - 1.17 0.09
Posterior corneal defect 1.44 0.31 - 6.60 0.64
Vascularization 0.29 0.10 – 0.81 0.02
Microphthalmos 0.19 0.05 – 0.68 0.01
Glaucoma 0.23 0.08 – 0.67 0.007
Glaucoma surgery 0.16 0.04 – 0.67 0.01
Lens surgery 0.27 0.08 – 0.89 0.03 PKP 0.45 0.13 – 1.54 0.21 Optical iridectomy 0.98 0.17 – 5.71 0.98Optical management 2.53 0.60 – 10.72 0.21Peters type I 3.28 1.0 - 10.2 0.04
Univariate analysis of preoperative and intraoperative variables that associated with final visual acuity of 20/200 or better.

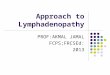
Kaplan Meier survival curves showing overall PKP survival probability (A), PKP survival probability stratified per disease type (B), and by the presence of glaucoma (C).
A
B C

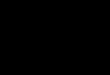
Peters anomaly
Severe disease
Moderate disease
Mild disease
Observen=7
Optical managementn=9
PKPn=25
Peters type I
Weigh risk against benefits.
Poor prognosisn=3 (1 Peters I & 2
Peters II eyes)
Peters type II
Keratolenticular touch and/or
cataract
Aphakia/lens remnant
Associated severe systemic/ocular abnormalities
Large axial
opacity(>3mm)
Small axial
opacity (≤3mm)
PKP n=12
(n=4) Optical management
Peripheral opacity
Paraxial opacity
Small axial
opacity (≤3mm)
Large axial
opacity(>3mm)
± Viscodissection ± Cataract extraction
n=3 0.9 ± 0.5 n=1 LP
0.4 ± 0.3 0.7 ± 0.7 n=21 1.0 ± 0.6 n=2LP
n=2NLP
n=6 1.4 ± 1.3n=2LP
n=3 NLP
n=3LP
Vision is expressed as mean ± standard deviation (logMAR units).

DISCUSSION In accordance to previous studies, our study shows that mild disease
has better visual outcomes than more severe disease and that there is no difference in the visual outcomes between unilateral and bilateral disease.
Our study also shows that in eyes that have undergone PKP, development of glaucoma is a major hurdle for graft survival and for good visual outcome.
Despite being considered the severe form of the disease, patients with Peters type II can still attain good visual outcome especially when optical management is feasible.
In our series, all patients who received optical management in both peters I and II groups had CDVA of 1.3 logMAR (20/400) or better with 8 patients having 0.5 logMAR (20/70) vision or better.

CONCLUSION Visual rehabilitation in Peters anomaly remains a
great challenge.
Cases necessitating observation or minor surgical intervention achieve good vision.
When PKP is indicated poorer outcomes are obtained, nevertheless patients can still attain functional visual acuity with encouraging graft longevity.
Recommended