
County of San Diego 2018 Employee Benefits Open Enrollment
October 2nd – 26th, 2017
2018 Open Enrollment
Agenda • 2018 Employee Benefits Open Enrollment
Overview
⁻ Medical, Dental, Vision and Life Insurance Plans
• Ancillary Benefit Plans
⁻ Critical Illness
⁻ Short Term & Long Term Disability Plans
• Reimbursement Accounts
2018 Open Enrollment
Open Enrollment Overview
• 2018 Employee Benefits Open Enrollment Period ‒ Monday, October 2nd - Thursday, October 26th ‒ New Premium Rates and Open Enrollment election changes
• REQUIRED Enrollment ‒ All employees must participate in Open Enrollment and complete
their elections in the PeopleSoft System. Flexible Spending Accounts must be re-elected every year.
• New Medical Carrier-UnitedHealthcare
2018 Benefits Plans
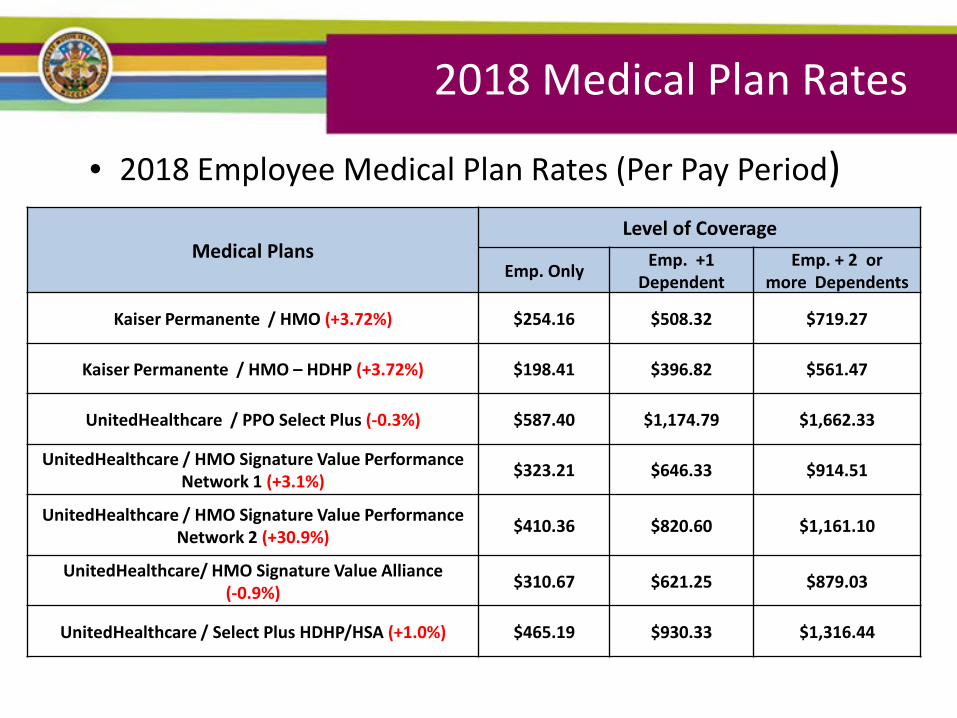
• 2018 Employee Medical Plan Rates (Per Pay Period)
Medical Plans Level of Coverage
Emp. Only Emp. +1 Dependent
Emp. + 2 or more Dependents
Kaiser Permanente / HMO (+3.72%) $254.16 $508.32 $719.27
Kaiser Permanente / HMO – HDHP (+3.72%) $198.41 $396.82 $561.47
UnitedHealthcare / PPO Select Plus (-0.3%) $587.40 $1,174.79 $1,662.33
UnitedHealthcare / HMO Signature Value Performance Network 1 (+3.1%) $323.21 $646.33 $914.51
UnitedHealthcare / HMO Signature Value Performance Network 2 (+30.9%) $410.36 $820.60 $1,161.10
UnitedHealthcare/ HMO Signature Value Alliance (-0.9%) $310.67 $621.25 $879.03
UnitedHealthcare / Select Plus HDHP/HSA (+1.0%) $465.19 $930.33 $1,316.44
2018 Medical Plan Rates
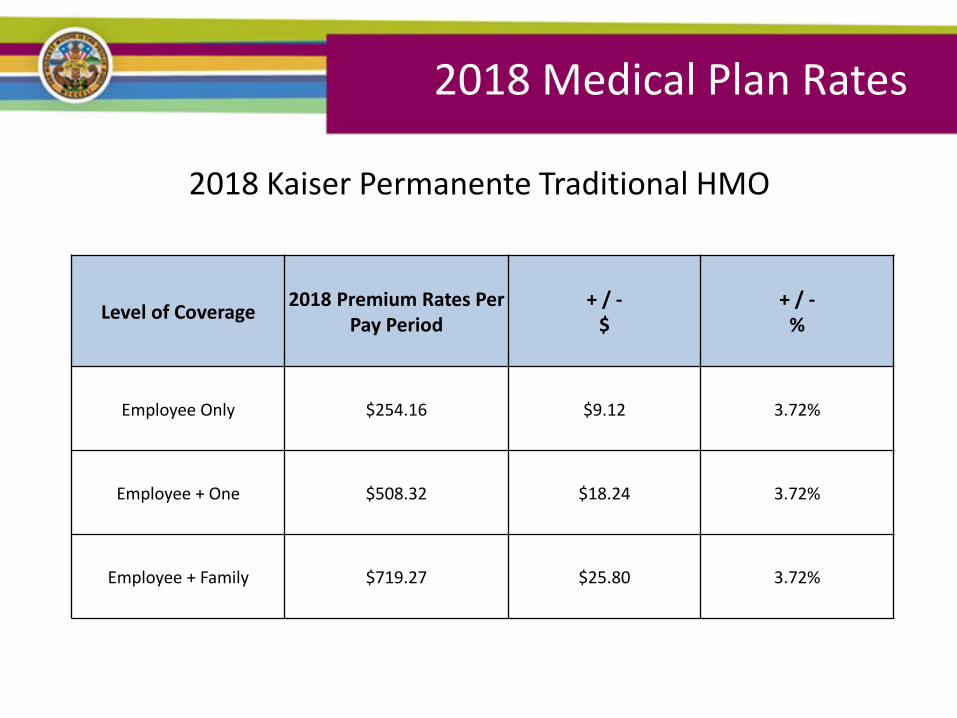
2018 Kaiser Permanente Traditional HMO
2018 Medical Plan Rates
Level of Coverage 2018 Premium Rates Per Pay Period
+ / - $
+ / - %
Employee Only $254.16 $9.12 3.72%
Employee + One $508.32 $18.24 3.72%
Employee + Family $719.27 $25.80 3.72%
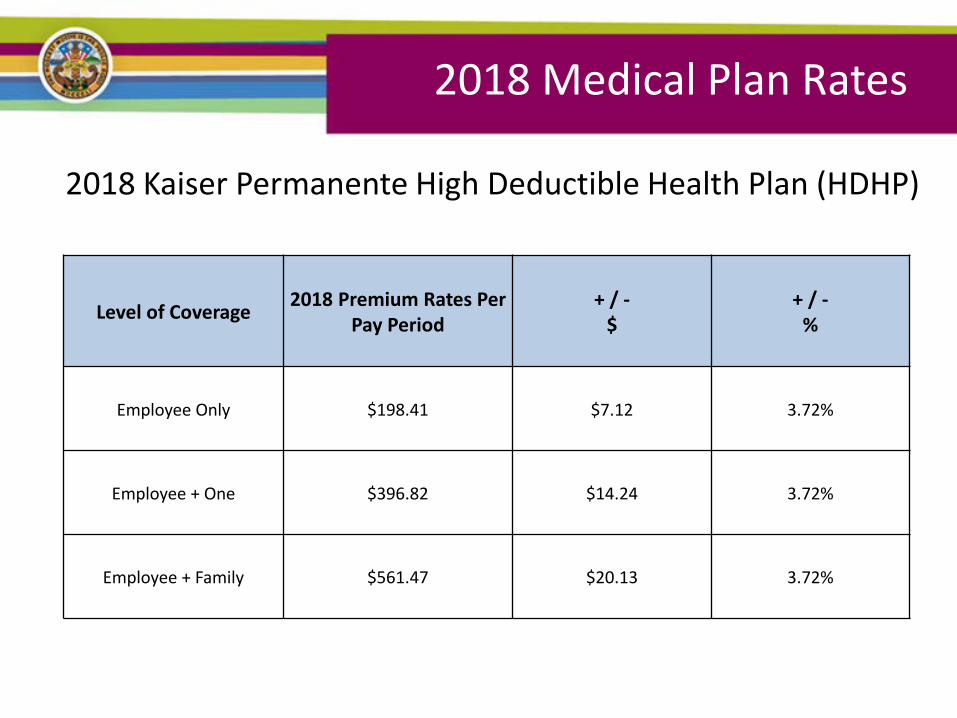
2018 Kaiser Permanente High Deductible Health Plan (HDHP)
2018 Medical Plan Rates
Level of Coverage 2018 Premium Rates Per Pay Period
+ / - $
+ / - %
Employee Only $198.41 $7.12 3.72%
Employee + One $396.82 $14.24 3.72%
Employee + Family $561.47 $20.13 3.72%
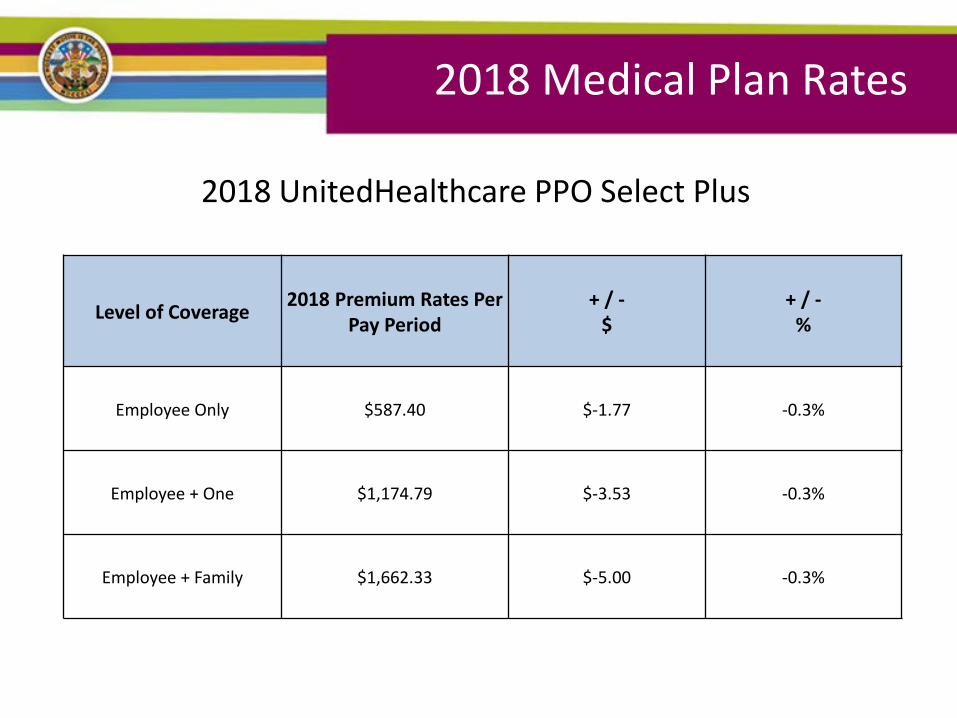
2018 UnitedHealthcare PPO Select Plus
2018 Medical Plan Rates
Level of Coverage 2018 Premium Rates Per Pay Period
+ / - $
+ / - %
Employee Only $587.40 $-1.77 -0.3%
Employee + One $1,174.79 $-3.53 -0.3%
Employee + Family $1,662.33 $-5.00 -0.3%
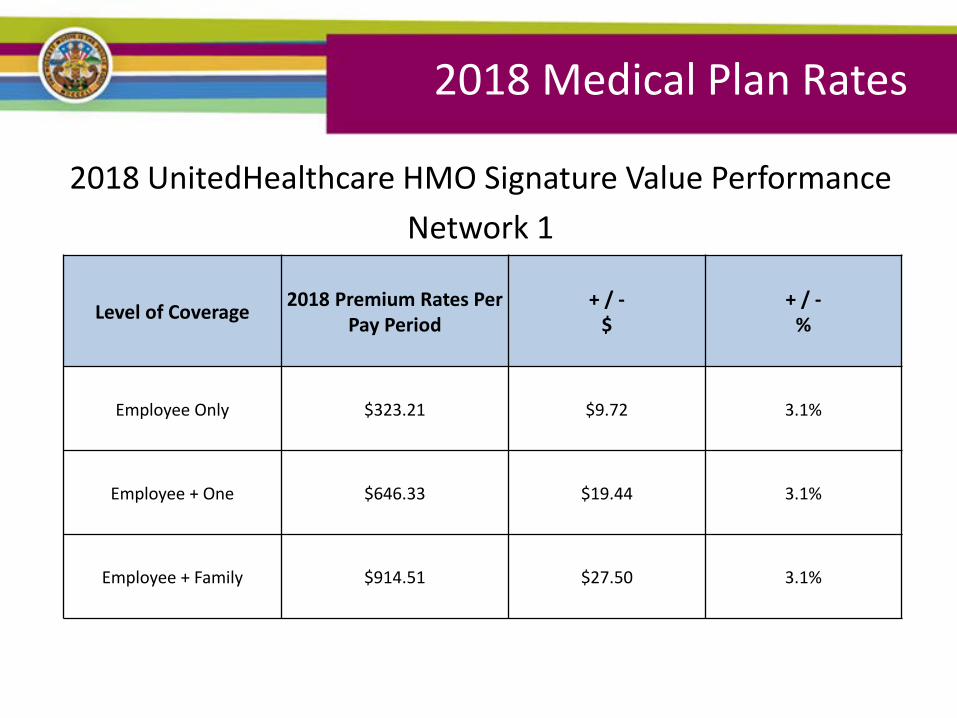
2018 UnitedHealthcare HMO Signature Value Performance Network 1
2018 Medical Plan Rates
Level of Coverage 2018 Premium Rates Per Pay Period
+ / - $
+ / - %
Employee Only $323.21 $9.72 3.1%
Employee + One $646.33 $19.44 3.1%
Employee + Family $914.51 $27.50 3.1%
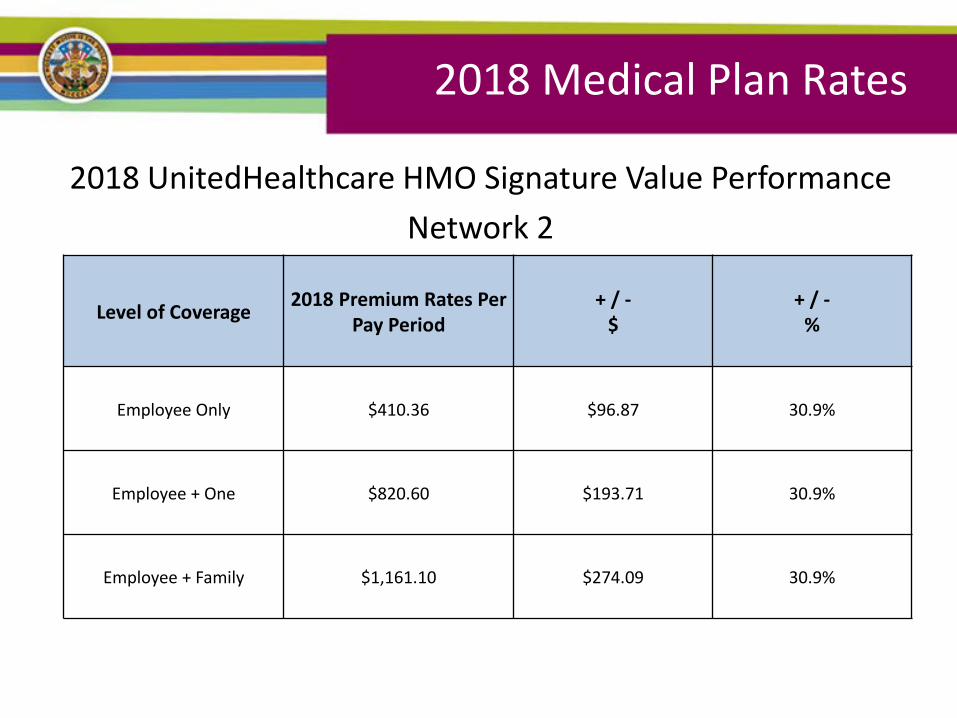
2018 Medical Plan Rates
Level of Coverage 2018 Premium Rates Per Pay Period
+ / - $
+ / - %
Employee Only $410.36 $96.87 30.9%
Employee + One $820.60 $193.71 30.9%
Employee + Family $1,161.10 $274.09 30.9%
2018 UnitedHealthcare HMO Signature Value Performance Network 2
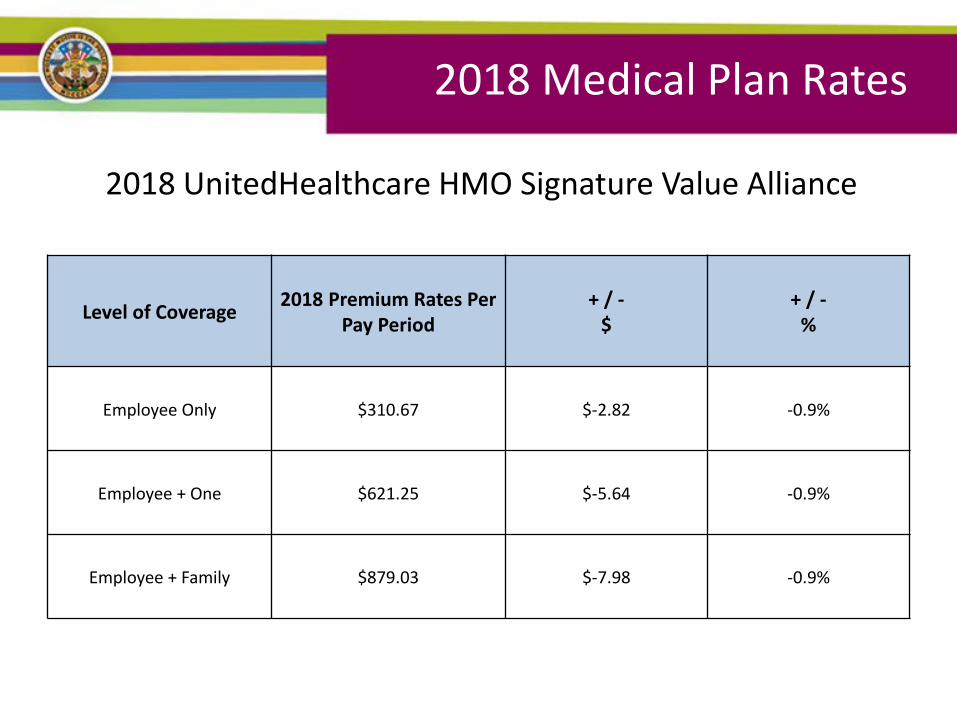
2018 UnitedHealthcare HMO Signature Value Alliance
2018 Medical Plan Rates
Level of Coverage 2018 Premium Rates Per Pay Period
+ / - $
+ / - %
Employee Only $310.67 $-2.82 -0.9%
Employee + One $621.25 $-5.64 -0.9%
Employee + Family $879.03 $-7.98 -0.9%
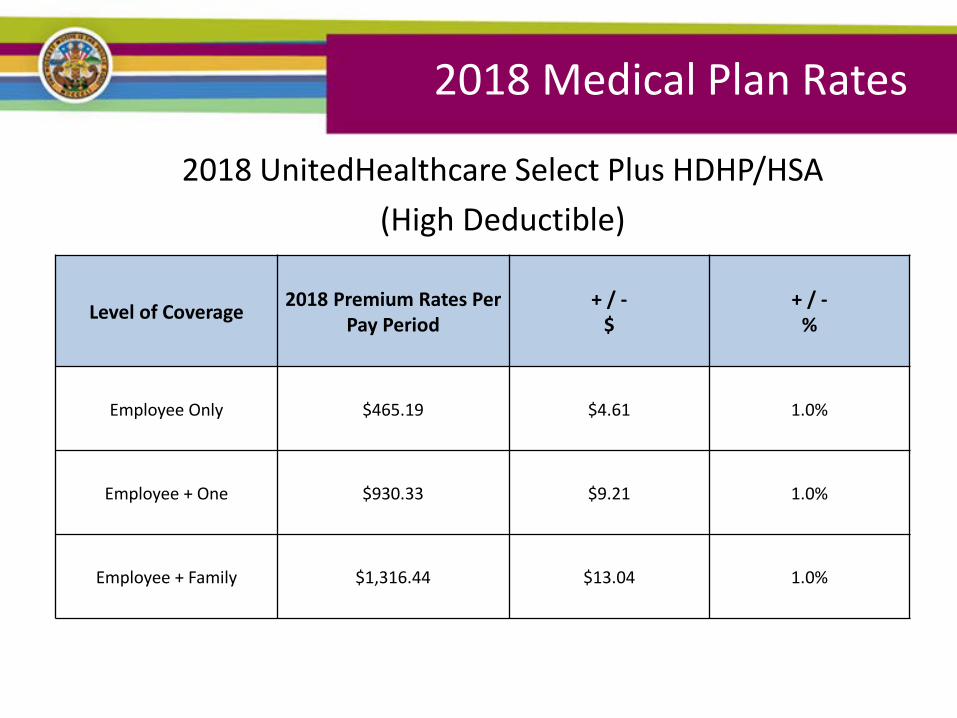
2018 UnitedHealthcare Select Plus HDHP/HSA (High Deductible)
2018 Medical Plan Rates
Level of Coverage 2018 Premium Rates Per Pay Period
+ / - $
+ / - %
Employee Only $465.19 $4.61 1.0%
Employee + One $930.33 $9.21 1.0%
Employee + Family $1,316.44 $13.04 1.0%
2018 Dental and Vision Plans
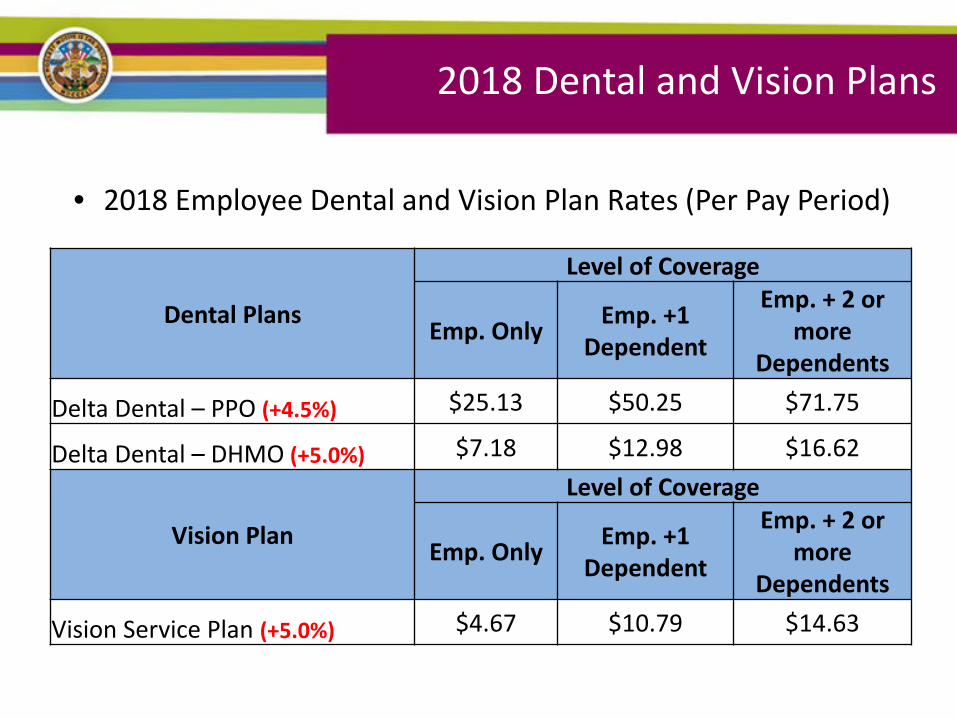
• 2018 Employee Dental and Vision Plan Rates (Per Pay Period)
Dental Plans
Level of Coverage
Emp. Only Emp. +1 Dependent
Emp. + 2 or more
Dependents
Delta Dental – PPO (+4.5%) $25.13 $50.25 $71.75
Delta Dental – DHMO (+5.0%) $7.18 $12.98 $16.62
Vision Plan
Level of Coverage
Emp. Only Emp. +1 Dependent
Emp. + 2 or more
Dependents
Vision Service Plan (+5.0%) $4.67 $10.79 $14.63
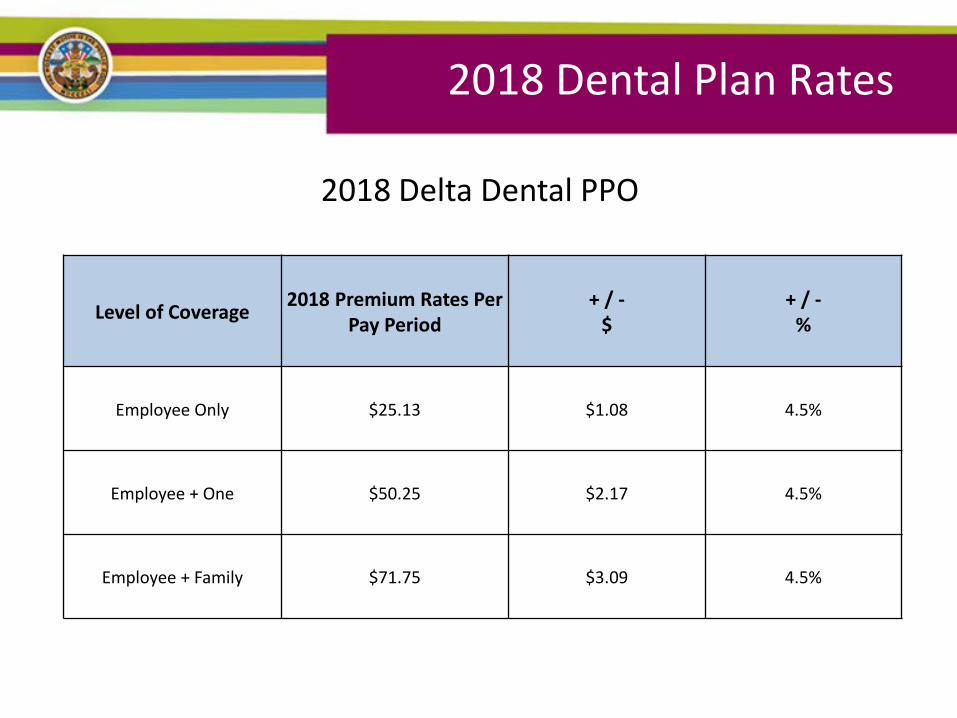
2018 Delta Dental PPO
2018 Dental Plan Rates
Level of Coverage 2018 Premium Rates Per Pay Period
+ / - $
+ / - %
Employee Only $25.13 $1.08 4.5%
Employee + One $50.25 $2.17 4.5%
Employee + Family $71.75 $3.09 4.5%
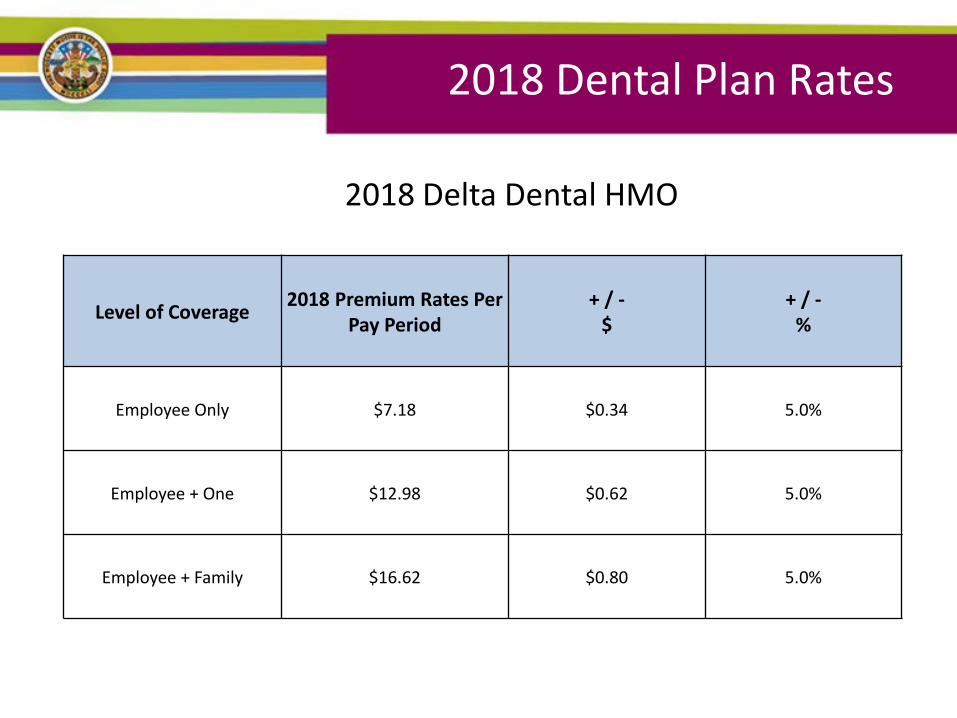
2018 Delta Dental HMO
2018 Dental Plan Rates
Level of Coverage 2018 Premium Rates Per Pay Period
+ / - $
+ / - %
Employee Only $7.18 $0.34 5.0%
Employee + One $12.98 $0.62 5.0%
Employee + Family $16.62 $0.80 5.0%
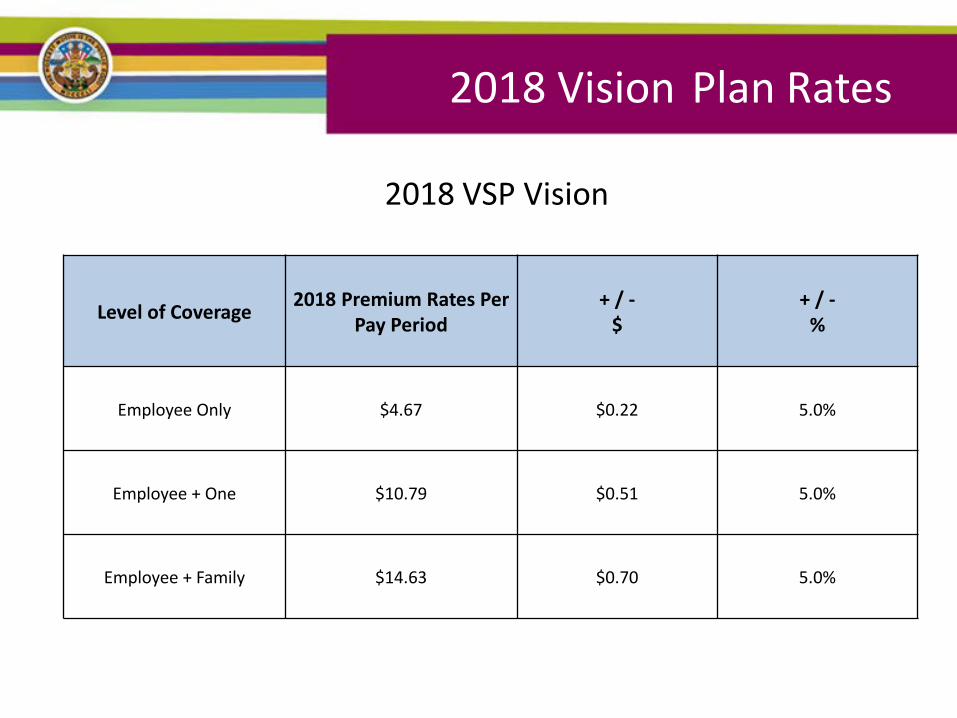
2018 VSP Vision
2018 Vision Plan Rates
Level of Coverage 2018 Premium Rates Per Pay Period
+ / - $
+ / - %
Employee Only $4.67 $0.22 5.0%
Employee + One $10.79 $0.51 5.0%
Employee + Family $14.63 $0.70 5.0%
2018 Plan Details
UnitedHealthcare THREE HMO Plans:
• Signature Value Alliance HMO – Includes Scripps and UCSD
• Signature Value Performance HMOs –Network 1-Similar to Anthem Select network
includes Sharp, does NOT include UCSD –Network 2-includes, Greater Tri-Cities IPA,
Multi-Cultural MG
• Call UnitedHealthcare between Dec 11th and Dec 15th to designate your HMO primary care provider (PCP) 888-586-6365
UnitedHealthcare The PPO Plan is designed to allow you to choose your health care providers from a network. Unlike an HMO, you do not need to enroll with a primary care physician and you do not need a referral to see a specialist.
PPO Network
Obtain care directly from any United Healthcare PPO
Network Provider, Nationwide
You pay less for care services when you use this level
Out-of-Network
Obtain care directly from any provider
You pay the highest costs when you use
this level
UnitedHealthcare • County of San Diego VEBA Advocacy Call Center
888-276-0250 (UnitedHealthcare Plans only) • Provides support regarding:
– Selecting a network during Open Enrollment, New Hire Enrollment, or Qualifying Life Event Change
– Accessing Care and Emergency Prescription Drugs – Transitioning Care to a New Provider – Complaints and Suggestions on Quality of Care or Access to a
Timely Appointment – Navigating the System to Deal with Complex Health Issues
• VEBA is a joint Labor-Management trust under Internal Revenue
Code 501, includes over 120,000 school district employees and is now available for all public sector employees
Kaiser Permanente - HMO
Kaiser HMO Plan:
• Co-payments apply
• No annual deductible
• Annual out-of-pocket maximum: $1,500 per individual and $3,000 per family
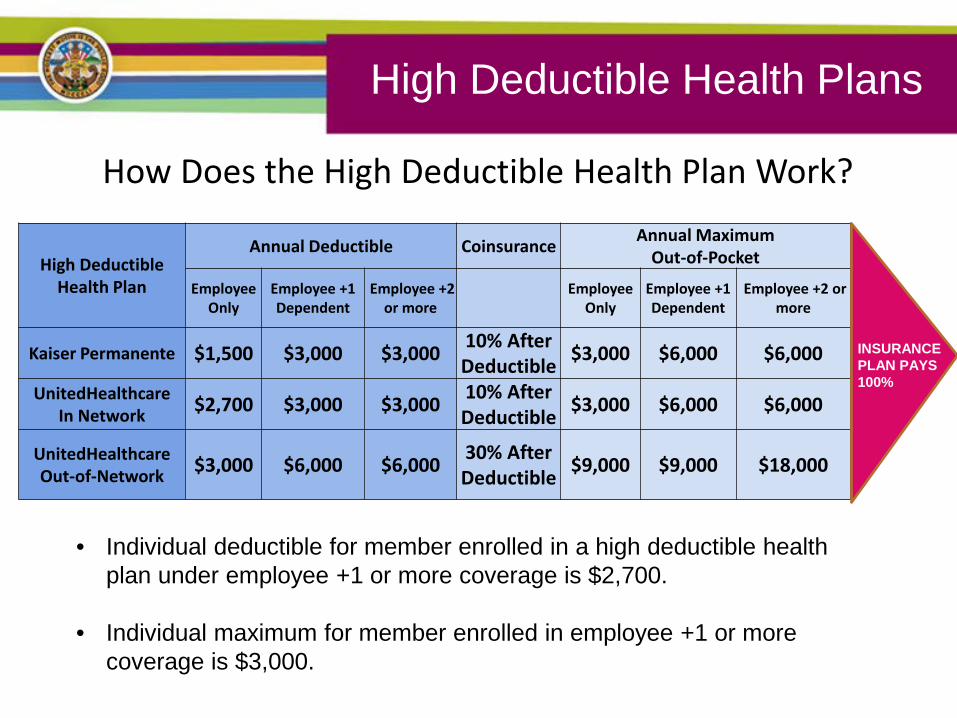
How Does the High Deductible Health Plan Work?
High Deductible
Health Plan
Annual Deductible Coinsurance Annual Maximum Out-of-Pocket
Employee Only
Employee +1 Dependent
Employee +2 or more
Employee Only
Employee +1 Dependent
Employee +2 or more
Kaiser Permanente $1,500 $3,000 $3,000 10% After Deductible $3,000 $6,000 $6,000
UnitedHealthcare In Network $2,700 $3,000 $3,000 10% After
Deductible $3,000 $6,000 $6,000
UnitedHealthcare Out-of-Network $3,000 $6,000 $6,000 30% After
Deductible $9,000 $9,000 $18,000
INSURANCE PLAN PAYS 100%
High Deductible Health Plans
• Individual deductible for member enrolled in a high deductible health plan under employee +1 or more coverage is $2,700.
• Individual maximum for member enrolled in employee +1 or more coverage is $3,000.
Dental Plans
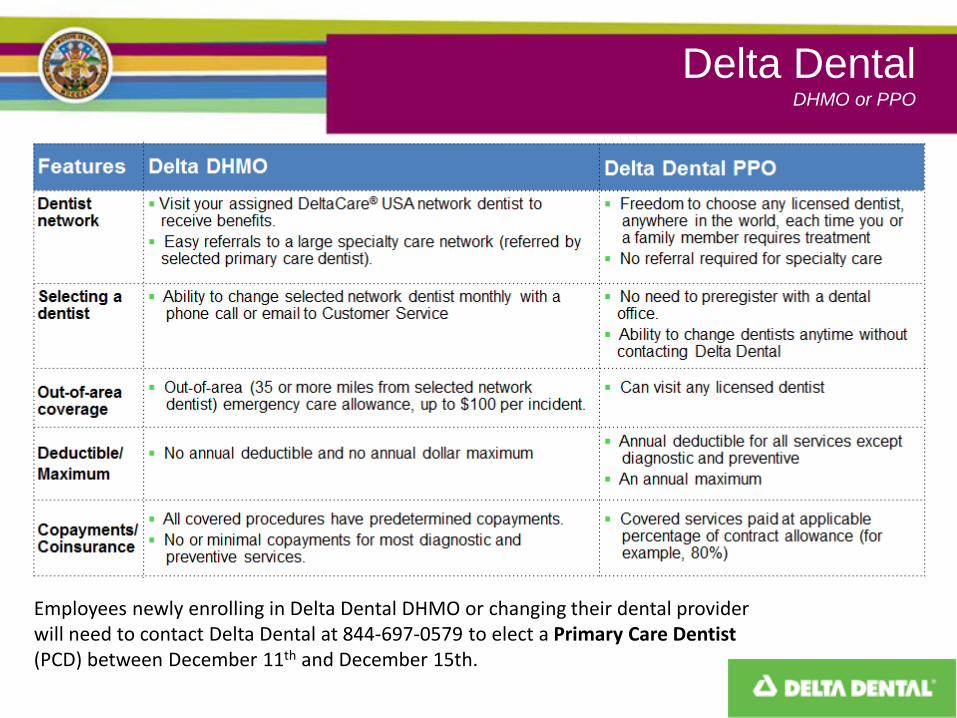
Delta Dental DHMO or PPO
Employees newly enrolling in Delta Dental DHMO or changing their dental provider will need to contact Delta Dental at 844-697-0579 to elect a Primary Care Dentist (PCD) between December 11th and December 15th.
Vision Plans
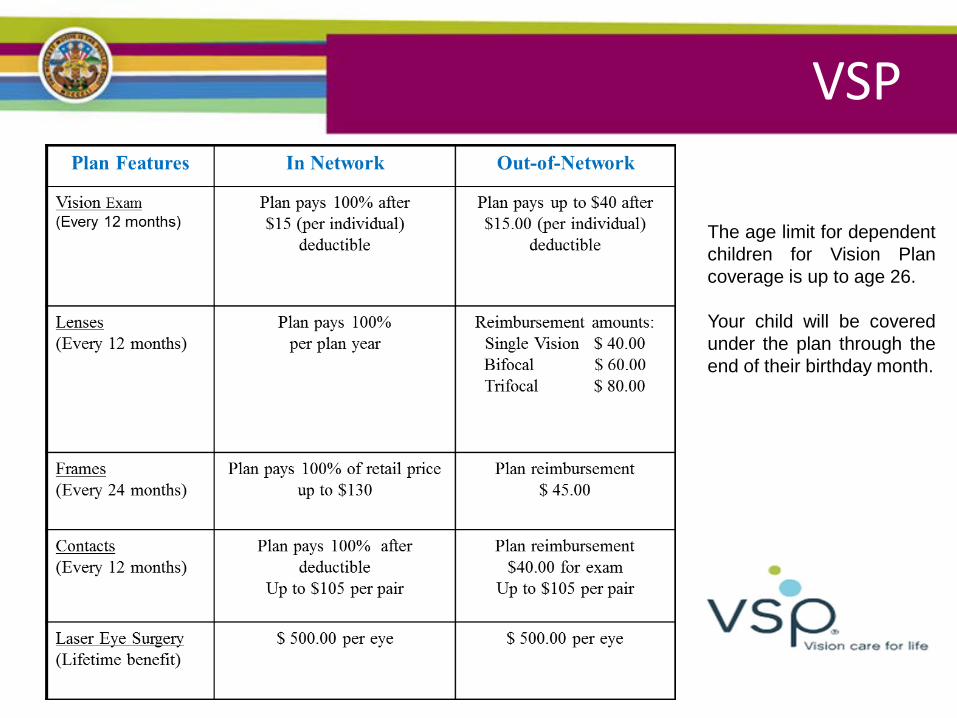
VSP
The age limit for dependent children for Vision Plan coverage is up to age 26. Your child will be covered under the plan through the end of their birthday month.

Life Insurance Plans
Life Insurance • Basic Life Insurance
⁻ The County provides life insurance coverage for their employees.
⁻ The coverage amount varies depending upon your job classification
⁻ The County also provides Life insurance in the amount of $2,000 for each qualified spouse and eligible children
• Supplemental Life Insurance ⁻ 1, 2, or 3 times your basic annual salary ⁻ Employee only coverage
Accidental Death & Dismemberment
Basic AD&D Coverage • The County provides insurance for you at no cost • The amount varies depending upon your job
classification • Covers loss of limb, leg or eyesight due to an
accident • Covers accidental death Supplemental AD&D Coverage • 1, 2 or 3 times your basic annual salary • Employee Only or Employee and Family
A Few Things To Remember
• Evidence of Insurability (Statement of Health) for all supplemental life increases or first time elections outside of new hire enrollment
• Can purchase with flex credits • 1, 2 or 3X annual salary
Ancillary Benefit Plans
Critical Illness
Critical Illness
• Critical Illness Plan – Provides a lump sum payment if employee or
family member is diagnosed with a critical illness • Cancer • Heart attack • Stroke
– Helps offset health plan co-payments or lost wages – Includes a $100 annual wellness benefit – Deductions are taken post-tax
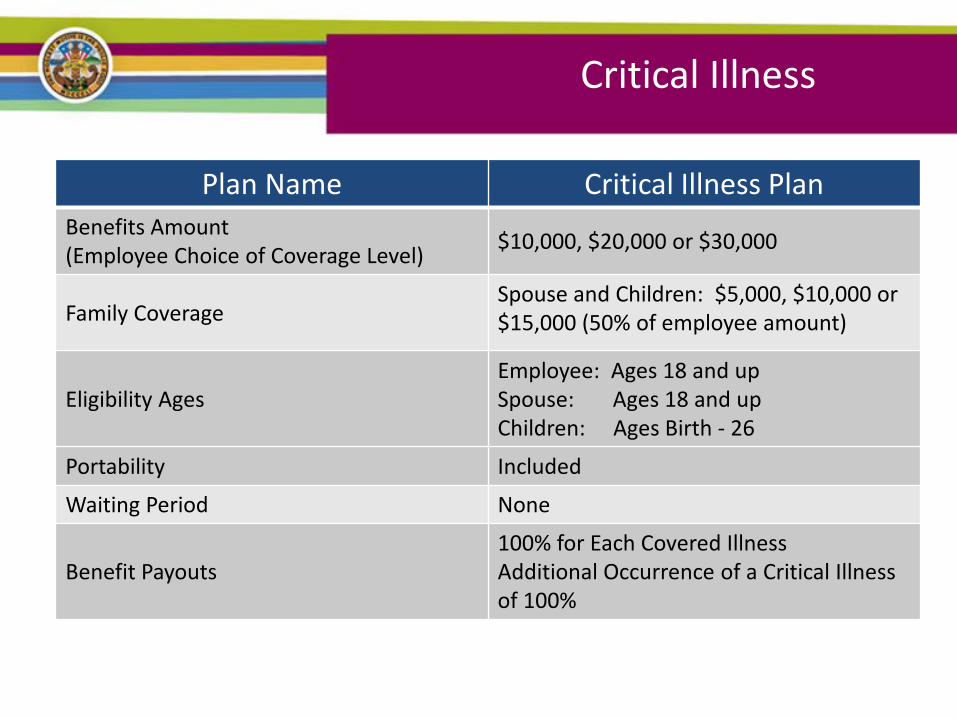
Plan Name Critical Illness Plan Benefits Amount (Employee Choice of Coverage Level) $10,000, $20,000 or $30,000
Family Coverage Spouse and Children: $5,000, $10,000 or $15,000 (50% of employee amount)
Eligibility Ages Employee: Ages 18 and up Spouse: Ages 18 and up Children: Ages Birth - 26
Portability Included
Waiting Period None
Benefit Payouts 100% for Each Covered Illness Additional Occurrence of a Critical Illness of 100%
Critical Illness
Disability Plans • Short Term Disability
• Long Term Disability
Voluntary Short Term
Disability Plans
Voluntary Short Term Disability
California State Disability Insurance (SDI) • 60% of earnings (for most individuals) up to a maximum weekly
benefit (maximum amount TBD). • Benefits begin on the 8th day and continue for up to twelve
months
Voluntary Supplemental Short Term Disability Plan • An additional 25% of earnings up to a maximum additional
benefit of $1,000/week • Benefits start on the 15th day and continue up to 24 weeks • Income replacement = 85% of pre-disability earnings
‒ 60% SDI (for most) + 25% Voluntary Supplemental Short Term Disability = 85% total
‒ This benefit is a supplement to CA SDI
Voluntary Short Term Disability
Voluntary Short Term Disability Plan • 60% of earnings up to a maximum benefit of
$1,500/week • Benefits start on the 8th day of disability • Benefit duration range from 3 – 12 weeks
‒ Duration period is determined by employee based on their leave balances and individual needs
• Voluntary Short Term Disability is a “Bridge” to Long Term Disability
Voluntary Long Term Disability
(LTD) Plans
• Voluntary Long Term Disability (LTD) Plan ‒ 60% of earnings up to a maximum benefit of
$5,000/month
‒ Benefits after 180 day elimination period
‒ Benefit duration is up to Social Security normal retirement age
Voluntary Long Term Disability
A Few More Things on Ancillary Benefits
• Deductions taken as post-tax – Benefits collected as non-taxable
• Benefits can be purchased with excess flex credits
• If planning to use benefit for maternity leave, cannot already be pregnant – payment into plan does not begin until first payroll deduction

Flexible Spending Accounts Plans
& Health Saving Accounts
Types of Accounts
Flexible Spending Accounts • Health Care • Dependent Care • Limited Purpose
• Health Savings Account • Health Reimbursement Account
2018 Flexible Spending Accounts • Minimum contribution is $120 per year.
• Maximum contributions per year:
‒ Healthcare - $2,600 out of pocket - **NO EMPLOYER MONEY**
‒ Dependent Care - $5,000 per year
‒ Limited Purpose Flexible Spending Account (Dental & Vision expenses only, for High Deductible Plan users only) - $2,600 out of pocket
• Estimate carefully and contribute only as much as you think you will spend
during the plan year. What you don’t use, you lose at the end of the year.
• Carryover of $500 ‒ Up to $500 of remaining flexible spending account funds can be carried
over from your health care spending account. It won’t impact your total contribution amount
‒ Carryover will be accessible in April, after filing period ends
Health Care Flexible Spending Account
Use Health Care Flexible Spending Account – HCFSA – for:
• Medical, Dental and Vision plan deductibles and co-payments for you and your eligible dependents
• Some over-the-counter medications are eligible with a valid
prescription • Full list of eligible expenses available at
www.asiflex.com/sdcounty
The Health Care Account can benefit you if you have predictable out-of-pocket medical, dental, and vision care expenses Annual Minimum Contribution: $120.00 2018 Annual Maximum Contribution: $2,600.00
Dependent Care Flexible Spending Account
• Use Dependent Care Account (FSA) for:
‒ Care of a child under age thirteen ‒ Care of another qualified dependent while you work ‒ $5,000 is the maximum per family. For a married couple, only
one can enroll in the plan with the full $5k annual contribution, or both can claim half of the amount
‒ NOTE: Reimbursement under the Dependent Care Spending Account cannot occur until the care has been fully provided, and/or after a deposit is made into the account.
** Dependent daycare contributions will not carryover
Limited Purpose Flexible Spending Account
• What is a Limited Purpose Flexible Spending Account (LPFSA)?
‒ A LPFSA, generally used in conjunction with a health
savings account (HSA), is a tax savings account that reimburses employees for eligible dental and vision care expenses only.
‒ A LPFSA is subject to “use it or lose it” IRS rule
‒ Annual contribution is limited to $2,600
HSA It’s yours
even if you switch jobs,
plans or retire
It’s held in a trust, like an
IRA
Funds roll over and
accumulate year to year if
not spent
Contributions are tax-free (subject to
limits)
If you are 55 years or older
you are eligible to deposit catch-up
contributions
• What is a Health Savings Account (HSA)? ‒ A HSA allows individuals to pay for qualified health
expenses and save for future medical and retiree health expenses on a tax free basis.
Health Savings Accounts
You are not eligible to open an HSA if:
Annual contribution limits are set by the IRS
You or your dependent are enrolled in Medicare
You are receiving health benefits under TRICARE
You are covered by another non-qualified health plan (such as a spouse’s plan)
You or your dependent can be claimed as a dependent on another individual’s tax return
Health Savings Accounts
• Maximum contributions per year:
‒ $3,450 (individual)
‒ $6,900 (family)
‒ Over 55 - (individual) $4,450 (Family) $7,900
• Enrollment in High Deductible Plan is required to participate in the HSA Plan
‒ Employees in HDHP will have excess Flex Credits contributed to an HSA
‒ Employees can also contribute out-of-pocket money to this account (subject to contribution maximums)
Health Savings Accounts
Health Reimbursement Accounts (HRAs)
• Employees must be enrolled in an eligible Group medical plan to be eligible for an HRA
• Employer excess flexible credit contributions up to $5,000
• Employer money only
• All Excess Flex credits will be defaulted to this account. Up to a max of $5,000
• Up to $500 will rollover
Reminders • While making elections, be sure to update Beneficiary Designations on all Life
Insurance Plans.
• Employees enrolling in the UnitedHealthcare HMO plans will need to contact UnitedHealthcare at 888-586-6365 to elect a Primary Care Physician (PCP).
• Employees newly enrolling in Delta Dental DHMO or changing their dental provider
will need to contact Delta Dental at 844-697-0579 to elect a Primary Care Dentist (PCD).
• PCP and PCD designations must be provided from December 11 to December 15, 2017 in order to have an ID card by January 1, 2018.
• If enrolling or adding a Dependent (Spouse, child or Domestic Partner) employee will
be required to submit proof of relationship.
• If Waiving Medical Benefits employee will be required to complete electronic waiver form
County of San Diego 2018 Employee Benefits Open Enrollment
October 2nd – 26th, 2017
Presented by: Elaine Pitpit- Human Resources Services Manager Department of Human Resources Employee Benefits Division
Recommended

















