Detailed Background and Research Plan APP1066835 Rayner
1
1. AIMS We propose a randomised, placebo-controlled trial of a twice daily 35g whey protein preload, taken before breakfast and dinner, to test the hypothesis that glycated haemoglobin (HbA1c) will be reduced by at least 0.5% compared to baseline at 12 weeks, in patients with type 2 diabetes who have relatively good glycaemic control (HbA1c ≤ 7.9%) on diet or metformin therapy alone. We will also test the secondary hypotheses that the whey preload:
• Induces slowing of gastric emptying, stimulation of incretin hormones and insulin, and reduces appetite and glycaemia after a standardised meal, and that these effects are sustained over 12 weeks;
• Induces greater reduction in HbA1c in subjects with more rapid gastric emptying at baseline;
• Is not associated with weight gain, due to “compensation” for the increased protein load; and
• Reduces HbA1c independently of changes in insulin resistance, weight, or body composition
2. BACKGROUND If current trends are maintained in Australia, more than a third of the population will develop type 2 diabetes within their lifetime (1). Early intervention to prevent and limit progression of micro- and probably macro-vascular complications can be achieved with fastidious glycaemic control, albeit at the risk of weight gain and hypoglycaemia with insulin therapy (2). There is now increasing recognition of the importance of specifically lowering postprandial, rather than fasting or preprandial, glycaemia in patients with mildly or moderately elevated HbA1c – who make up a majority of type 2 patients in the community (3). The recently updated ADA/EASD guidelines for managing type 2 diabetes advocate an individualised approach, with dietary intervention and weight management the cornerstone of therapy, and the need to balance reduction in HbA1c with the risk of hypoglycaemia (4). Newer therapies, particularly the glucagon-like peptide-1 (GLP-1) agonists, are useful for targeting postprandial glycaemic excursions with minimal risk of hypoglycaemia and modest weight loss, but these are expensive, require subcutaneous injection, and cannot be tolerated by a substantial proportion of patients due to adverse effects, particularly nausea. Broadly effective nutritional strategies to reduce postprandial glycaemia are therefore highly attractive, and represent the greatest opportunity for optimising glycaemic control at affordable cost as the healthcare demands of our society escalate.
Rationale for targeting postprandial glycaemic control Given that nutrients empty from the stomach in health in the range of 1 – 4 kcal/min (5; 6), and that people in modern societies generally consume three main meals per day, often with snacks in between, it is clear that most of the day is spent in the postprandial state, with only a few hours of true fasting before breakfast (7). The traditional focus on controlling “fasting” blood glucose in the management of type 2 diabetes is, therefore, often inappropriate. For the majority of type 2 patients, who have relatively good overall glycaemic control (in Australia, the median HbA1c in known type
Reducing postprandial blood glucose excursions in type 2 diabetes is increasingly being recognised as fundamental to achieving good overall glycaemic control, as assessed by glycated haemoglobin. Our work has established that the rate of emptying of carbohydrates from the stomach, and the secretion of the gut peptides GLP-1 and GIP (“incretins”) that drive postprandial insulin stimulation, are critical determinants of postprandial glycaemia. We have developed the concept of giving macronutrient “preloads” in advance of a meal in type 2 diabetes, to limit postprandial glycaemia by initiating gut hormone secretion and slowing gastric emptying of the subsequent meal. In particular, we established that a whey protein preload substantially reduces postprandial glycaemia when given acutely in type 2 patients. If this magnitude of postprandial glucose lowering is maintained with sustained use, the preload strategy will represent an important advance in the dietary management of type 2 diabetes.

Detailed Background and Research Plan APP1066835 Rayner
2
2 patients is 6.8% (3)), postprandial glycaemia predominates over fasting blood glucose in contributing to HbA1c, and a deterioration in postprandial glycaemic control precedes any substantial elevation of fasting blood glucose (8). Therapies that specifically target postprandial glycaemic excursions are therefore of fundamental importance in preventing the progression of diabetes and the emergence of micro- and macro-vascular complications, whose incidence is related closely to the HbA1c (2). This is not to say that the importance of controlling postprandial glycaemia is limited to “early” type 2 diabetes; there is increasing recognition that even insulin-treated patients benefit from the addition of an agent that targets postprandial blood glucose, such as a GLP-1 agonist, once basal insulin has provided control of fasting glycaemia (9; 10).
The gastrointestinal tract as a key determinant of postprandial glycaemia It should not be surprising that the gastrointestinal tract, which is responsible for storing ingested nutrients in the stomach and regulating their delivery to the small intestine at a controlled rate to optimise digestion and absorption, plays a central role in determining postprandial glycaemic excursions (11). When nutrients interact with the small intestine, they generate feedback that slows further gastric emptying and suppresses appetite, via both neural and hormonal mechanisms. The latter include cholecystokinin (CCK), peptide YY (PYY), and GLP-1. The small and large intestine also secrete peptides that account for the “incretin effect” – the phenomenon by which insulin secretion is at least doubled when glucose is given by the enteral route when compared to an isoglycaemic intravenous glucose infusion (12; 13). The two known incretins are glucose-dependent insulinotropic polypeptide (GIP) and GLP-1. It is only in recent years, with the advent of incretin-based therapy for type 2 diabetes (ie. GLP-1 agonists and DPP-4 inhibitors), that the role of the gut in postprandial glycaemic control has been widely appreciated. Such therapies have focussed on GLP-1, since it retains much of its activity on type 2 diabetes, unlike GIP (14).
GLP-1 agonists are appealing for the management of postprandial glycaemia in type 2 diabetes because they stimulate insulin secretion and suppress glucagon in a glucose-dependent manner (ie. mainly when the blood glucose concentration is elevated above normal fasting values), so carry little risk of hypoglycaemia, and they are also associated with modest weight loss. However, their predominant action to lower postprandial blood glucose is to slow gastric emptying, and their efficacy is relatively less in patients who already have abnormally slow emptying at baseline (15). Due to their expense, the need for regular subcutaneous injections, and the high prevalence of adverse effects such as nausea, GLP-1 agonists are not appropriate for the majority of patients with type 2 diabetes. Initial reports that patients with longstanding diabetes have impaired GLP-1 secretion after mixed meals (16; 17) did not take differences in gastric emptying into account, and have not been confirmed subsequently (18). We have reported that type 2 patients controlled with diet or metformin alone have intact GLP-1 secretion in response to an intraduodenal glucose challenge (19), supporting the concept that dietary approaches to enhance the stimulation of endogenous GLP-1 and other gut peptides may be a useful strategy in the management of type 2 diabetes. Harnessing nutrient-gut interactions to improve postprandial glycaemia – development of the “preload” concept Nutritional therapies to improve glycaemic control in type 2 diabetes, such as adopting low carbohydrate, low glycaemic index, or high protein diets, have generally had relatively modest benefits over sustained periods, probably largely due to the need to adhere to relatively rigid restrictions (20). Our approach differs, in that the only prescribed element of the diet is the “preload”, which acts by stimulating nutrient-gut interactions in order to optimise metabolism of the subsequent meal. In recent years we have undertaken a series of acute physiological studies in patients with type 2 diabetes that have allowed us to refine this concept.
We initially evaluated the effects of a fat preload, given the potency of fat for stimulating GLP-1 and slowing gastric emptying (21; 22). A preload of 30 mL olive oil was consumed 30 min before a

Detailed Background and Research Plan APP1066835 Rayner
3
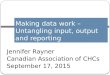
high carbohydrate potato meal in diet-controlled type 2 patients (mean HbA1c 6.2% ± standard error 0.3 %) (23). This preload substantially slowed the emptying of the subsequent meal (Fig. 1), with a corresponding delay in the postprandial glycaemic excursion (Fig. 2) – effects which were much greater than when the same amount of oil was consumed with the meal, indicating the importance of timing of the preload. The fat preload stimulated an enhanced endogenous GLP-1 response, but insulin secretion was suppressed rather than increased, due to the delay in entry of carbohydrate to the small intestine, and the fact that the insulinotropic effect of GLP-1 is glucose-dependent and blood glucose was < 10 mmol/L when GLP-1 peaked. As a result, the decrease in the magnitude of the postprandial blood glucose excursion was modest, without a significant difference in peak blood glucose.
Acute effects of protein preloads in type 2 diabetes
Protein would potentially represent a more favourable preload than fat, given that it is more satiating and would therefore be less likely to promote weight gain (24). We established that protein can slow gastric emptying and reduce glycaemic excursions when added to a glucose drink, associated with stimulation of insulin, GLP-1, and GIP (25). Moreover, the profiles of gut peptide concentrations after various protein preloads, including whey, have been well documented (26), with the peak changes in hormone concentrations occurring within 30 to 60 minutes of preload ingestion. Whey protein, a by-product of cheese manufacture, had been observed to lower blood glucose and stimulate insulin secretion when provided as a supplement with meals (27). We therefore evaluated the effects of a preload of 55g whey protein in type 2 patients (HbA1c 6.5 ± 0.2%) under a similar protocol to the fat preload study (23), with an interval of 30 min between
Fig. 1. Gastric emptying (% retention as determined by scintigraphy) of a mashed potato meal when 30 ml olive oil was consumed before the meal (oil), 30 ml water was consumed before the meal (water), or 30 ml water was consumed before a meal that also contained 30 ml olive oil (water and oil) in type 2 patients (n=6). Data are the mean ± SEM. *P<0.05 oil vs. water; #P<0.05 oil vs. water and oil; ^P<0.05 water vs. water and oil. The oil preload substantially delayed the emptying of the potato meal (Gentilcore et al J Clin Endocrinol Metab 2006).
Fig. 2. Blood glucose, and plasma insulin, GIP, and GLP-1 concentrations after ingestion of the mashed potato meal; symbols are defined in the legend to fig. 1. The oil preload stimulated GLP-1 and delayed the postprandial rise in blood glucose, with a corresponding reduction in the insulin response (Gentilcore et al J Clin Endocrinol Metab 2006).

Detailed Background and Research Plan APP1066835 Rayner
4
preload and meal (28). As with the fat preload, gastric emptying of the meal was substantially slower after whey (Fig. 3).
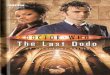
In contrast to fat, however, the whey preload was associated with a marked reduction in postprandial blood glucose (peak value ~3 mmol/L lower), and while GLP-1 and GIP concentrations increased after whey, there was also substantial stimulation of insulin (Fig. 4), possibly due to a combination of the incretin effect with direct stimulation of beta cells by absorbed amino acids (29). It might be expected that GLP-1 would predominate over GIP in contributing to the incretin effect in type 2 patients, given the loss of the insulinotropic effect of GIP in type 2 diabetes (14), although this may not be the case in patients with very good glycaemic control (30).
Appropriate preloads for sustained use
Given that fat or protein preloads entail additional intake of energy, the use of a non- or low-energy preload would be appealing as a dietary strategy for prolonged use. We have established that artificial sweeteners such as sucralose do not stimulate GLP-1 release or slow gastric emptying in humans (31), unlike rodents (32). We did show that preloads of 3-O-methylglucose, a glucose analogue that is absorbed via the sodium-dependent glucose transporter-1 but not metabolised and, therefore, yields no energy, can achieve stimulation of GLP-1 and slowing of gastric emptying that is at least as potent as glucose (33), but the expense of this analogue is prohibitive. Xylose is a poorly absorbed pentose sugar that shows promise in reducing postprandial glycaemia when given to type 2 patients as a preload, particularly when combined with the dipeptidyl peptidase-4
Fig. 3. Gastric emptying (% retention as determined by scintigraphy) of a mashed potato meal when 55g whey protein was consumed before the meal (filled circles), or with the meal (open circles), or when no whey was consumed (open squares) in type 2 patients (n=8). Data are the mean ± SEM. *P<0.05 whey preload vs. whey in meal; #P<0.05 whey in meal vs. no whey; §P<0.05 whey preload vs. no whey. The whey preload slowed gastric emptying of the potato meal substantially (Ma et al Diabetes Care 2009).
Fig. 4. Blood glucose, and plasma insulin, GLP-1, and GIP concentrations after ingestion of the mashed potato meal when 55g whey protein was consumed before the meal (filled circles), or with the meal (open circles), or when no whey was consumed (open squares) in type 2 patients (n=8). Data are the mean ± SEM. *P<0.05 whey preload vs. whey in meal; #P<0.05 whey in meal vs. no whey; §P<0.05 whey preload vs. no whey. The whey preload markedly lowered postprandial blood glucose, and was associated with stimulation of GLP-1, GIP, and insulin (Ma et al Diabetes Care 2009).

Detailed Background and Research Plan APP1066835 Rayner
5
inhibitor, sitagliptin, to prolong the half life of the active form of GLP-1 (34). However, diarrhoea and flatulence due to the presence of unabsorbed xylose in the large bowel are likely to limit its tolerability in the long term.
Despite the additional energy intake that a protein preload entails, protein has a dose-dependent satiating effect if given ≤ 2 hours before a subsequent meal (35; 36), and subjects tend to compensate for the additional energy load by eating less at a subsequent ad libitum meal (37; 38). Whey in particular appears more satiating than other proteins such as casein (39). Therefore, protein preloads are unlikely to add substantially to overall energy intake, and if they lead to a reduction in energy intake at the following meal, including intake of carbohydrate, this would provide an additional mechanism for lowering glycaemia. Sustained effects of a whey protein preload with regular exposure
In order for regular use of protein preloads to be a viable strategy for reducing postprandial glycaemic excursions, their effects would need to be sustained in the long term. The gut is known to adapt to supplementation with some macronutrients, notably glucose and fat, so that the feedback inhibition of gastric emptying is reduced (40; 41). It is noteworthy, however, that the attenuation of feedback appears to be nutrient-specific, so that glucose supplementation is associated with accelerated emptying of glucose, but not of fat (42). We would anticipate, therefore, that prolonged exposure to a protein supplement would not affect the rate of gastric emptying of carbohydrate. To clarify this issue, we studied 8 patients with diet-controlled type 2 diabetes (HbA1c 5.9 ± 0.5%) who consumed a 25g whey protein preload or placebo three times daily in randomised fashion, 30 min before each meal for 4 weeks, before crossing over to the alternative treatment after a 2 week “washout” period (manuscript submitted). Patients attended the laboratory on the first and last day of each 4 week intervention for measurement of gastric emptying (scintigraphy) and glycaemic responses to a standardised potato meal, so that there were 4 visits in total (Fig. 5).
We observed that the capacity of the whey preload to slow gastric emptying of the potato meal and reduce the postprandial glycaemic excursion remained intact after 4 weeks exposure, and did not differ from the effect at the beginning of the intervention. Although a 4 week intervention was insufficient to evaluate a change in HbA1c, we observed that the energy load of the preload was compensated for, so that there was no difference in overall energy intake, as evaluated by 3 day diet diaries before and during the last week of the intervention, nor did weight change. Moreover, compliance with the preload as measured by sachet count was high, and the whey supplement was well tolerated. The decrement in blood glucose after the standardised meal was smaller than for our previous study (28). A lower dose of whey in theory might not have been a disadvantage, given that
Fig. 5. Blood glucose concentrations and gastric emptying (mean ± SEM) in type 2 patients (n=8) after a mashed potato meal eaten 30 min after a 25g whey preload or placebo, at the beginning (“study 1”) and end (“study 2”) of each 4 week intervention. * P < 0.05, 1st whey day vs. 1st placebo day; # P < 0.05, 2nd whey day vs. 2nd placebo day. The effect of the whey preload to slow gastric emptying and lower postprandial blood glucose was not diminished after 4 weeks’ exposure (manuscript submitted).

Detailed Background and Research Plan APP1066835 Rayner
6
protein ingestion results in dose-dependent stimulation of glucagon as well as insulin (43). Our data indicate, however, that the dose should optimally be higher than 25g. Concerns have been raised that a long-term increase in protein in the diet might have adverse effects on bone density and renal function (44; 45). We have not documented any reduction in bone density in a 2 year weight loss study in postmenopausal women, or loss of renal function in a one year weight loss study in patients with type 2 diabetes who had microalbuminuria (CIB, manuscript submitted).
Having established persisting efficacy and safety of protein supplementation, we believe it is now pivotal to determine the capacity for regular use of protein preloads to improve glycaemic control, in a randomised controlled trial that is powered sufficiently to detect an improvement in HbA1c. We will study patients with relatively good glycaemic control (HbA1c ≤ 7.9%) since this is the group in which postprandial hyperglycaemia makes the dominant contribution to HbA1c (46). Given that a third or more of patients with longstanding diabetes have abnormally slow gastric emptying (47), and that the capacity for GLP-1 to slow gastric emptying is markedly diminished in this subset (15), it will be important to determine whether the rate of gastric emptying at baseline predicts the efficacy of protein preloads for improving glycaemic control. Since high protein diets have the capacity to induce weight loss yet preserve lean mass, with a corresponding reduction in insulin resistance (44), it will also be important to take these variables into account when evaluating effects of whey preloads on glycaemia.
3. RESEARCH PLAN - METHODS AND TECHNIQUES Organisation of the proposed study
The study capitalises on the complementary skills of the investigators, who have international reputations in gut physiology relating to diabetes (CIs Rayner, Horowitz, Jones) and the performance of prolonged large scale dietary intervention trials for glycaemic control and weight loss, with an emphasis on manipulation of dietary protein (CI Clifton). The preload approach has been refined during our NHMRC project grant 627139 (2010-12), and the proposed study will occur in the context of our NHMRC Centre of Research Excellence in Translating Nutritional Science to Good Health (2013-17). The latter will provide essential support, including the assistance of a biostatistician and technical support for hormone assays, but cannot directly fund the project. CI Rayner will be responsible for driving the study, supported by the nutritional trial expertise of CI Clifton and intellectual input of CI Horowitz, while CI Jones will contribute particularly to the evaluation of gastric emptying. The study will involve higher degree students – the CIs currently supervise PhD/Masters students who are dieticians and physicians training in endocrinology and gastroenterology. However, an experienced full time research assistant will be essential to coordinate recruitment and the large number of screening and study visits required. The investigators have substantial experience in attracting relatively well-controlled patients with type 2 diabetes from the community to participate in studies, and CI Clifton has completed numerous dietary studies on a comparable scale to that proposed, with modest dropout rates (~20%). We expect to recruit the majority of subjects by advertisement (The Advertiser is the sole daily newspaper in South Australia, with good coverage of the population), facilitated by our ability to publicise our research in the media (CI Rayner’s prior preload studies generated substantial media interest, and CI Clifton is interviewed regularly on television and radio). In our experience, the target population of patients with relatively good glycaemic control is the segment that is most easily attracted to participate in trials of nutritional interventions. We also advertise through Diabetes SA, the Diabetes Centre at the Royal Adelaide Hospital, and several large suburban general practices with the involvement of diabetes educators.
The sample size has been calculated with the assistance of our CRE biostatistician (Ms K Lange) for α=0.05 and β=0.2, based on the primary outcome measure of a reduction in HbA1c of ≥ 0.5% at

Detailed Background and Research Plan APP1066835 Rayner
7
12 weeks compared to baseline in the group taking whey preloads, with allowance for a 25% dropout rate. It is anticipated that recruitment will be complete by the second quarter of year 3 (2016), and that all subjects will have completed the trial by the third quarter of 2016, allowing 3 months for data analysis and manuscript preparation. Methods and techniques
All the required techniques are established in our group. Gastric emptying of a standardised mashed potato meal will be measured using a 13C-octanoate breath test with which we have extensive experience (34), and which has been validated against the gold standard of scintigraphy (48-50). Plasma insulin, C-peptide, glucose, GLP-1, GIP, CCK, PYY and glucagon will be measured as previously (51; 52); assays can be performed “in house” at cost, utilizing CRE resources. We have access to dual energy X-ray absorptiometry (DEXA) in the Endocrine Unit at the Royal Adelaide Hospital, which we will use to measure body composition (total body fat mass and fat free mass) at the beginning and end of the intervention. Weight will be monitored at each study visit using calibrated scales, and insulin resistance will be estimated from fasting insulin and glucose concentrations by homeostasis model assessment (HOMA-IR) (53).
The dose of whey (35g) will be intermediate between that of our acute study (55g (28)) and our four week trial (25g), in order to optimise the balance between the magnitude of reduction in postprandial glycaemia with the provision of additional energy to the diet and the capacity of protein to stimulate glucagon. Packaging of the whey preload into sachets will be carried out by contract food manufacturer Omniblend (Campbellfield, Victoria); CI Clifton has an established relationship with this company for the production of high protein supplements, and our hospital pharmacy will coordinate randomization. The placebo will consist of low-energy powdered flavouring that can be added to water. Both the whey and the placebo will be sweetened with artificial sweeteners, which we have shown do not elicit gut hormone secretion or modify gastric emptying or the glycaemic response to a subsequent meal (31). Subjects will be offered three choices of flavouring for both the whey and placebo preloads, and will be allowed to swap flavours during the trial, in order to optimise compliance.
Detailed study protocol The study will have a randomised, placebo controlled parallel group design. We have opted against a crossover study, which although reducing the number of subjects required, would be open to the potential for order effects and would require twice the number of study visits for individual subjects. Both the subjects and the investigators analysing the data will be blinded to treatment allocation. Because the appearance of the active and placebo preloads will not be identical, the research assistant who interacts with the subjects cannot be blinded, but will not be involved in data analysis. Participants will not receive any specific dietary advice during the study; a particular feature of the preload approach is that subjects are not constrained by a rigid dietary regimen. Inclusion criteria
• Male or female patients with a diagnosis of type 2 diabetes by WHO criteria (plasma glucose ≥ 7 mmol/L fasting, or ≥ 11.1 mmol/L two hours after a glucose challenge) or with a history of HbA1c ≥ 6.5%, managed by diet or metformin alone.
• Age 18 – 70 years • Body mass index 19-35 kg/m2, and weight-stable • HbA1c ≥ 6.0% and ≤ 7.9% at the time of screening
Exclusion criteria
• Requirement for insulin or other diabetes medications, other than metformin • Significant gastrointestinal symptoms, or history of gastrointestinal disease including
known gastroparesis, or surgery (other than appendicectomy or cholecystectomy), including bariatric surgery

Detailed Background and Research Plan APP1066835 Rayner
8
• Proteinuria or eGFR < 45 mL/min • Intake of > 20 g alcohol on a daily basis, or cigarette smoking • Current use of medications which are likely to affect gastrointestinal function or appetite
(opiates, anticholinergics, levodopa, calcium-channel antagonists, beta blockers, clonidine, nitrates, tricyclic antidepressants, selective serotonin re-uptake inhibitors, phosphodiesterase type 5 inhibitors, sumatriptan, metoclopramide, domperidone, cisapride, tegaserod, or erythromycin)
• Current pregnancy or lactation; • Inability to maintain a regular pattern of meal intake due to shift work, frequent travel or
dining out (> 2x/week), or habitual omission of breakfast; • Widely fluctuating exercise patterns • Change in weight ≥ 3% during the previous 12 months, without attempts to lose weight
during this period
Sample size 240 subjects will be recruited in total, with 120 randomised to each group. This will provide sufficient power to detect a 0.5% difference in HbA1c with whey preloads at 12 weeks compared to baseline, assuming a standard deviation of 1.2% (54), and allowing for a 25% dropout rate (≥90 subjects are required to complete the study in each group). Screening visit
Subjects will attend the laboratory for a screening visit where the diagnosis and duration of known diabetes will be reviewed, medical history and medications recorded, and physical examination carried out, including documentation of height and weight, and the presence of micro- and macro-vascular complications of diabetes. Autonomic nerve function will be evaluated using standardised cardiovascular reflex tests (variation in heart rate during deep breathing, heart rate response to standing, and fall in systolic blood pressure in response to standing). Each test result will be scored according to age-adjusted pre-defined criteria as 0 = normal, 1 = borderline and 2 = abnormal, for a total maximum score of 6. A score ≥ 3 will be considered to indicate autonomic dysfunction (55). A standardised questionnaire will be completed to score gastrointestinal symptoms (56). Urine will be tested by dipstick to exclude proteinuria, and blood will be sampled for complete blood picture, biochemistry, lipids, and HbA1c. Subjects who fulfil the inclusion and exclusion criteria and provide informed consent will then be randomised. They will also complete a validated 3 day diet diary prior to the intervention commencing, which will include two weekdays and one weekend day (57).
Laboratory assessments at beginning and end of the 12 week intervention period On the first and last day of the intervention period, subjects will attend the laboratory at ~0830h. They will be provided with a standard beef lasagne meal to consume at 1900h the evening before, with a non-alcoholic beverage and a piece of fruit (in order to minimise variation in baseline incretin measurements (33; 34; 58)), after which they will fast from solids and liquids, but may consume water until 2400h. They will be will be weighed, and will provide a spot urine sample for measurement of the urea/creatinine ratio (an index of protein intake). An intravenous cannula will be inserted into an antecubital vein for blood sampling, and a baseline sample will be collected for measurement of fasting blood glucose concentration and HbA1c. On each study day, subjects will consume the preload in 200 mL water, between T= -30 to -28 min. Thirty minutes later (T = 0 min), they will eat a meal consisting of 65 g powdered potato and 20 g glucose, reconstituted with 200 mL water and 1 egg yolk containing 100µL 13C-octanoic acid. Subjects will consume the meal within 5 minutes. Breath samples will be collected immediately before, and every 5 minutes after, meal ingestion in the first hour and every 15 minutes for a further 3 hours for the measurement of gastric emptying. Venous blood samples (~15 mL) will be taken immediately before the preload administration (T = -30 min), and at T = 0, 15, 30, 60, 90, 120, 180

Detailed Background and Research Plan APP1066835 Rayner
9
and 240 min for the measurements of blood glucose, insulin, C-peptide, total GLP-1 and GIP, CCK, PYY, and glucagon. At the same intervals used for blood sampling, appetite and gastrointestinal sensations will be assessed by means of validated 100mm visual analogue scales (39). Gastric emptying of the carbohydrate meal, labelled with 13C octanoic acid, will be measured by excretion of 13CO2 in the breath by mass spectrometer, and expressed as a calculated half-emptying time.
At the conclusion of the first laboratory assessment, subjects will be provided with two weeks’ supply of preload, and given another 3 day diet diary to complete during the second week of the intervention. On each of the two study days, subjects will have body composition measured by DEXA.
Clinic visits throughout the 12 week intervention period Subjects will visit the Department every 2 weeks during the intervention (ie. weeks 2, 4, 6, 8, and 10), at which time they will be weighed, return all used and remaining preload packages, and submit their diet diary. They will provide a spot urine sample from which the urea/creatinine ratio will be measured; an increase over the baseline value in subjects in the active treatment group will provide supporting evidence of compliance. They will then be provided with a supply of preload sachets for the following 2 weeks, and a new diet diary. In addition, a venous blood sample will be collected at the week 6 visit for HbA1c.
In the intervening weeks (ie. weeks 1, 3, 5, 7, 9, and 11) an investigator will telephone each subject to reinforce compliance with the preload regimen.
Data analysis Outcomes will be analysed for all patients who complete the 12 week intervention regardless of compliance, although we expect to achieve adherence to at least two thirds of prescribed preload doses on the basis of three times daily drug regimens for chronic disease (59). Analysis of covariance (ANCOVA) will be used to compare changes in HbA1c in each group at 12 weeks, together with fasting and postprandial blood glucose values at the standardised meal tests, gastric half-emptying times, plasma concentrations of insulin, C-peptide, GLP-1, GIP, CCK, PYY, and glucagon, appetite scores, weight, and energy and macronutrient intake from diet diaries, adjusting for baseline values of the outcome parameter (60). The assumptions of normality, constant variance of the residuals, and equality of slopes between the baseline covariate and 12 week outcome will be assessed visually using diagnostic plots. If assumptions are not met then transformations of the outcome (normality, constant variance) or interactions between treatment group and baseline covariate (equality of slopes) will be used. To determine the influence of the baseline rate of gastric emptying on efficacy, the relationship between gastric half-emptying time and the change in HbA1c will be explored within the group receiving whey preloads, and the strength of linear and curvilinear relationships will be summarised by R2.
Data will also be analysed using multiple linear regression to evaluate whether the preload’s effect to improve glycaemia is independent of changes in insulin resistance (HOMA-IR), weight, or body composition. 4. OUTCOMES AND SIGNIFICANCE For the majority of patients with type 2 diabetes in the community, who are relatively well-controlled (HbA1c ≤ 7.9%), postprandial hyperglycaemia must be specifically targeted to optimise overall glycaemic control and prevent complications. The ideal strategy to achieve this would be a nutritional one. The proposed study represents the pivotal next step in translating the insights of our acute physiological “preload” studies to a clinically relevant approach.

Associate Investigator (AI) Contribution APP1066835 Rayner
10
Ms Kylie Lange Kylie Lange is an experienced biostatistician dedicated fulltime to the NHMRC CRE for Translating Nutritional Science to Good Health at the University of Adelaide, in which CIs A, B, C and D are all Chief Investigators. She has experience in nutritional clinical trials, has been involved in the current study design and analysis plan, and will be closely involved in the management of data collection and storage, and in the statistical analysis.

References APP1066835 Rayner
11
1. Magliano DJ, et al. Lifetime risk and projected population prevalence of diabetes. Diabetologia 2008;51:2179-2186 2. UKPDS Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes. Lancet 1998;352:837-853 3. Kemp TM, et al. Glucose, lipid, and blood pressure control in Australian adults with type 2 diabetes: the 1999-2000 AusDiab. Diabetes Care 2005;28:1490-1492 4. Inzucchi SE, et al. Management of hyperglycemia in type 2 diabetes: a patient-centered approach: position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2012;35:1364-1379 5. Brener W, et al. Regulation of the gastric emptying of glucose. Gastroenterology 1983;85:76-82 6. Elias E, et al. The slowing of gastric emptying by monosaccharides and disaccharides in test meals. J Physiol (Lond) 1968;194:317-326 7. Monnier L Is postprandial glucose a neglected cardiovascular risk factor in type 2 diabetes? Eur J Clin Invest 2000;30 Suppl 2:3-11 8. Monnier L, et al. The loss of postprandial glycemic control precedes stepwise deterioration of fasting with worsening diabetes. Diabetes Care 2007;30:263-269 9. Buse JB, et al. Use of twice-daily exenatide in Basal insulin-treated patients with type 2 diabetes: a randomized, controlled trial. Ann Intern Med 2011;154:103-112 10. Nauck MA, et al. Pharmacotherapy: GLP-1 analogues and insulin: sound the wedding bells? Nat Rev Endocrinol 2011;7:193-195 11. Rayner CK, et al. Relationships of upper gastrointestinal motor and sensory function with glycemic control. Diabetes Care 2001;24:371-381 12. Elrick H, et al. Plasma insulin response to oral and intravenous glucose administration. J Clin Endocrinol Metab 1964;24:1076-1082 13. McIntyre N, et al. New interpretation of oral glucose tolerance. Lancet 1964;41:20-21 14. Nauck MA, et al. Preserved incretin activity of glucagon-like peptide 1 [7-36 amide] but not of synthetic human gastric inhibitory polypeptide in patients with type-2 diabetes mellitus. J Clin Invest 1993;91:301-307 15. Linnebjerg H, et al. Effect of exenatide on gastric emptying and relationship to postprandial glycemia in type 2 diabetes. Regul Pept 2008;151:123-129 16. Toft-Nielsen MB, et al. Determinants of the impaired secretion of glucagon-like peptide-1 in type 2 diabetic patients. J Clin Endocrinol Metab 2001;86:3717-3723 17. Vilsboll T, et al. Reduced postprandial concentrations of intact biologically active glucagon-like peptide 1 in type 2 diabetic patients. Diabetes 2001;50:609-613 18. Vollmer K, et al. Predictors of incretin concentrations in subjects with normal, impaired, and diabetic glucose tolerance. Diabetes 2008;57:678-687 19. Ma J, et al. Effects of variations in duodenal glucose load on glycaemic, insulin, and incretin responses in type 2 diabetes. Diabet Med 2012;29:604-608 20. Layman DK, et al. Protein in optimal health: heart disease and type 2 diabetes. Am J Clin Nutr 2008;87:1571S-1575S 21. Feinle C, et al. Plasma glucagon-like peptide-1 (GLP-1) responses to duodenal fat and glucose infusions in lean and obese men. Peptides 2002;23:1491-1495 22. Stacher G, et al. Fat preload delays gastric emptying: reversal by cisapride. Br J Clin Pharmacol 1990;30:839-845 23. Gentilcore D, et al. Effects of fat on gastric emptying of, and the glycemic, insulin and incretin responses to, a carbohydrate meal in type 2 diabetes. J Clin Endocrinol Metab 2006;91:2062-2067 24. Clifton PM, et al. Metabolic effects of high-protein diets. Curr Atheroscler Rep 2007;9:472-478 25. Karamanlis A, et al. Effects of protein on glycemic and incretin responses and gastric emptying after oral glucose in healthy subjects. Am J Clin Nutr 2007;86:1364-1368 26. Bowen J, et al. Energy intake, ghrelin, and cholecystokinin after different carbohydrate and protein preloads in overweight men. J Clin Endocrinol Metab 2006;91:1477-1483

References APP1066835 Rayner
12
27. Frid AH, et al. Effect of whey on blood glucose and insulin responses to composite breakfast and lunch meals in type 2 diabetic subjects. Am J Clin Nutr 2005;82:69-75 28. Ma J, et al. Effects of a protein preload on gastric emptying, glycemia, and gut hormones after a carbohydrate meal in diet-controlled type 2 diabetes. Diabetes Care 2009;32:1600-1602 29. Fieseler P, et al. Physiological augmentation of amino acid-induced insulin secretion by GIP and GLP-I but not by CCK-8. Am J Physiol 1995;268:E949-955 30. Hojberg PV, et al. Four weeks of near-normalization of blood glucose has no effect on postprandial GLP-1 and GIP secretion, but augments pancreatic B-cell responsiveness to a meal in patients with Type 2 diabetes. Diabet Med 2008;25:1268-1275 31. Ma J, et al. Effect of the artificial sweetener, sucralose, on gastric emptying and incretin hormone release in healthy subjects. Am J Physiol Gastrointest Liver Physiol 2009;296:G735-739 32. Jang HJ, et al. Gut-expressed gustducin and taste receptors regulate secretion of glucagon-like peptide-1. Proc Natl Acad Sci U S A 2007;104:15069-15074 33. Wu T, et al. Effects of different sweet preloads on incretin hormone secretion, gastric emptying, and postprandial glycemia in healthy humans. Am J Clin Nutr 2012;95:78-83 34. Wu T, et al. Effects of a D-xylose preload with or without sitagliptin on gastric emptying, glucagon-like peptide-1, and postprandial glycemia in type 2 diabetes. Diabetes Care online 28 Jan 2013 35. Astbury NM, et al. Dose-response effect of a whey protein preload on within-day energy intake in lean subjects. Br J Nutr 2010;104:1858-1867 36. Anderson GH, et al. Protein source, quantity, and time of consumption determine the effect of proteins on short-term food intake in young men. J Nutr 2004;134:3011-3015 37. Bertenshaw EJ, et al. Dose-dependent effects of beverage protein content upon short-term intake. Appetite 2009;52:580-587 38. Potier M, et al. A high-protein, moderate-energy, regular cheesy snack is energetically compensated in human subjects. Br J Nutr 2009;102:625-631 39. Hall WL, et al. Casein and whey exert different effects on plasma amino acid profiles, gastrointestinal hormone secretion and appetite. Br J Nutr 2003;89:239-248 40. Horowitz M, et al. The effect of short-term dietary supplementation with glucose on gastric emptying of glucose and fructose and oral glucose tolerance in normal subjects. Diabetologia 1996;39:481-486 41. Cunningham KM, et al. Gastrointestinal adaptation to diets of differing fat composition in human volunteers. Gut 1991;32:483-486 42. Beckoff K, et al. Effects of glucose supplementation on gastric emptying, blood glucose homeostasis, and appetite in the elderly. Am J Physiol Regul Integr Comp Physiol 2001;280:R570-576 43. Claessens M, et al. Glucagon and insulin responses after ingestion of different amounts of intact and hydrolysed proteins. Br J Nutr 2008;100:61-69 44. Clifton P Effects of a high protein diet on body weight and comorbidities associated with obesity. Br J Nutr 2012;108 Suppl 2:S122-129 45. Jesudason D, et al. The interaction between dietary protein and bone health. J Bone Miner Metab 2011;29:1-14 46. Monnier L, et al. Contributions of fasting and postprandial plasma glucose increments to the overall diurnal hyperglycemia of type 2 diabetic patients: variations with increasing levels of HbA(1c). Diabetes Care 2003;26:881-885 47. Horowitz M, et al. Relationships between oesophageal transit and solid and liquid gastric emptying in diabetes mellitus. Eur J Nucl Med 1991;18:229-234 48. Braden B, et al. Measuring gastric emptying of semisolids in children using the 13C-acetate breath test: a validation study. Dig Liver Dis 2004;36:260-264 49. Ziegler D, et al. [13C]Octanoic acid breath test for non-invasive assessment of gastric emptying in diabetic patients: validation and relationship to gastric symptoms and cardiovascular autonomic function. Diabetologia 1996;39:823-830

References APP1066835 Rayner
13
50. Ghoos YF, et al. Measurement of gastric emptying rate of solids by means of a carbon-labeled octanoic acid breath test. Gastroenterology 1993;104:1640-1647 51. Meier JJ, et al. Glucagon-like peptide 1 abolishes the postprandial rise in triglyceride concentrations and lowers levels of non-esterified fatty acids in humans. Diabetologia 2006;49:452-458 52. Meier JJ, et al. Suppression of glucagon secretion is lower after oral glucose administration than during intravenous glucose administration in human subjects. Diabetologia 2007;50:806-813 53. Matthews DR, et al. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985;28:412-419 54. Fonseca VA, et al. Efficacy and Safety of the Once-Daily GLP-1 Receptor Agonist Lixisenatide in Monotherapy: A randomized, double-blind, placebo-controlled trial in patients with type 2 diabetes (GetGoal-Mono). Diabetes Care 2012;35:1225-1231 55. Ewing DJ, et al. Diagnosis and management of diabetic autonomic neuropathy. Br Med J 1982;285:916-918 56. Quan C, et al. Development and validation of the Diabetes Bowel Symptom Questionnaire. Aliment Pharmacol Ther 2003;17:1179-1187 57. Sturm K, et al. Appetite, food intake, and plasma concentrations of cholecystokinin, ghrelin, and other gastrointestinal hormones in undernourished older women and well-nourished young and older women. J Clin Endocrinol Metab 2003;88:3747-3755 58. Chandarana K, et al. Subject standardization, acclimatization, and sample processing affect gut hormone levels and appetite in humans. Gastroenterology 2009;136:2115-2126 59. Claxton AJ, et al. A systematic review of the associations between dose regimens and medication compliance. Clin Ther 2001;23:1296-1310 60. Vickers AJ, et al. Statistics notes: Analysing controlled trials with baseline and follow up measurements. BMJ 2001;323:1123-1124

Summary/Final Reports and Progress Reports APP1066835 Rayner
14
Final Report: NHMRC 627139 – Project grant. Upper gastrointestinal function and glycaemic control in diabetes mellitus. Rayner CK, Horowitz M, Jones KL, Feinle-Bisset C. (2010-2012) The proposed studies have proceeded efficiently; the following have been published/accepted for publication in the 12 months since the previous progress report: Original Papers
1. Ma J, Pilichiewicz AN, Feinle-Bisset C, Wishart JM, Jones KL, Horowitz M, Rayner CK. Effects of variations in duodenal glucose load on glycaemic, insulin, and incretin responses in type 2 diabetes. Diabet Med 2012;29:604-8.
2. Stevens JE, Horowitz M, Deacon CF, Nauck M, Rayner CK, Jones KL. The effects of sitagliptin on gastric emptying in healthy humans – a randomised, controlled study. Aliment Pharmacol Ther 2012; 36: 379-90
3. Chang J, Russo A, Bound M, Rayner CK, Jones KL, Horowitz M. A 25 year longitudinal evaluation of gastric emptying in diabetes mellitus. Diabetes Care 2012;35:2594-6
4. Wu T, Bound MJ, Standfield SD, Gedulin B, Jones KL, Horowitz M, Rayner CK. Effects of rectal administration of taurocholic acid on glucagon-like peptide-1 and peptide YY secretion in healthy humans. Diabetes Obes Metab. (accepted 21st November 2012)
5. Chang J, Rayner CK, Jones KL, Horowitz M. Prognosis of diabetic gastroparesis – a 25 year evaluation. Diabet Med. (accepted 30th November 2012)
6. Wu T, Bound MJ, Zhao BR, Standfield SD, Bellon M, Jones KL, Horowitz M, Rayner CK. Effects of a D-xylose preload, with or without sitagliptin, on gastric emptying, glucagon-like peptide-1 and postprandial glycemia in type 2 diabetes. Diabetes Care (accepted 24th December 2012)
7. Wu T, Bound MJ, Standfield SD, Jones KL, Horowitz M, Rayner CK. Effects of taurocholic acid on glycemic, glucagon-like peptide-1, and insulin responses to small intestinal glucose infusion in healthy humans. J Clin Endocrinol Metab (accepted 29th January 2013)
8. Chang J, Wu T, Greenfield JR, Samocha-Bonet D, Horowitz M, Rayner CK. Effects of intraduodenal glutamine on incretin hormone and insulin release, the glycemic response to an intraduodenal glucose infusion and antropyloroduodenal motility in health and type 2 diabetes. Diabetes Care (accepted 1st February 2013)
9. Ma J, Checklin HL, Wishart JM, Stevens JE, Jones KL, Horowitz M, Meyer JH, Rayner CK. A randomized trial of enteric-coated nutrient pellets to stimulate gastrointestinal peptide release and lower glycaemia in type 2 diabetes. Diabetologia (accepted 11th February 2013)
Reviews/Editorials
1. Marathe CS, Rayner CK, Jones KL, Horowitz M. Relationships between gastric emptying, postprandial glycemia and incretin hormones. Diabetes Care (accepted 16th November 2012)
2. Marathe CS, Rayner CK, Jones KL, Horowitz M. Glucagon-like peptides 1 and 2 in health & disease: a review. Peptides (accepted 31st January 2013)
3. Thazhath SS, Jones KL, Horowitz M, Rayner CK. Diabetic gastroparesis: recent insights into pathophysiology and implications for management. Expert Rev Gastroenterol Hepatol. 2013 Feb;7(2):127-39

Summary/Final Reports and Progress Reports APP1066835 Rayner
15
Progress Report: NHMRC Project Grant 627189: Gastric, small intestinal and cardiovascular mechanisms of postprandial hypotension. KL Jones, Gentilcore D, Visvanathan R, Chapman I, Rayner C, Horowitz M 2010 – 2013. Progress in the project has been satisfactory. The following studies have been completed: 1. Tai K, Gentilcore D, Jones KL, Banh L, Gilja OH, Hammond AJ, Feinle-Bisset C, Horowitz
M, Chapman IM. Orlistat accentuates the fat-induced fall in blood pressure in older adults. Br J Nutr 2011;106:417-24.
2. Stevens JE, Gilja OH, Gentilcore D, Hausken T, Horowitz M, Jones KL. Measurement of gastric emptying of a high-nutrient liquid by 3D ultrasonography in diabetic gastroparesis. Neurogastroenterol Motil 2011;23:220-e114.
3. Vanis L, Hausken T, Gentilcore D, Rigda R, Rayner CK, Feinle-Bisset C, Horowitz M, Jones KL. Comparative effects of glucose and xylose, on blood pressure, gastric emptying and incretin hormones in healthy older subjects. Br J Nutr 2011;4:1-8.
4. Gentilcore D, Vanis L, Teng JC, Wishart JM, Buckley JD, Rayner CK, Horowitz M, Jones KL. The oligosaccharide, alpha (α)-cyclodextrin, has modest effects to slow gastric emptying and modify the glycaemic response to sucrose in healthy older adults. Br J Nutr 2011;106:583-7.
5. Gentilcore D, Vanis L, Wishart JM, Rayner CK, Horowitz M, Jones KL. The alpha (α)-glucosidase inhibitor, acarbose, attenuates the blood pressure and splanchnic blood flow responses to intraduodenal sucrose in older adults. J Gerontol A Biol Sci Med Sci 2011;66:917-24.
6. Vanis L, Gentilcore D, Rayner CK, Wishart JM, Horowitz M, Feinle-Bisset C, Jones KL. Effects of small intestinal glucose load on blood pressure, splanchnic blood flow, glycemia and GLP-1 release in healthy older subjects. Am J Physiol Regul Integr Comp Physiol 2011;300:R1524-31.
7. Trahair LG, Vanis L, Gentilcore D, Lange K, Rayner CK, Horowitz M, Jones KL. Effects of variations in duodenal glucose load on blood pressure, heart rate, superior mesenteric artery blood flow and plasma noradrenaline in healthy young and older subjects. Clin Sci (Lond). 2012;122:271-9.
8. Vanis L, Gentilcore D, Lange K, Gilja OH, Rigda RS, Trahair LG, Rayner CK, Horowitz M, Jones KL. Effects of variations in intragastric volume on blood pressure and splanchnic blood flow during intraduodenal glucose infusion in healthy older subjects. Am J Physiol Regul Integr Comp Physiol 2012;302:R391-9.
9. Trahair LG, Horowitz M, Rayner CK, Gentilcore D, Lange K, Wishart JM, Jones KL. Comparative effects of variations in duodenal glucose load on glycemic, insulinemic, and incretin responses in healthy young and older subjects. JCEM 2012;97:844-51.
10. Rigda R, Little T, Trahair L, Gentilcore D, Rayner CK, Horowitz M, Jones KL. Effects of length and region of small intestine exposed to glucose on BP, HR and SMA flow in healthy older subjects. (manuscript in preparation).
Current studies: 11. Trahair L, Gentilcore D, Rayner CK, Visvanathan R, Horowitz M, Jones KL. Effects of small
intestinal glucose load on BP, HR, SMA flow in patients with PPH. (Commenced). 12. Trahair L, Gentilcore D, Rayner CK, Visvanathan R, Horowitz M, Jones KL. Evaluation of
the combined effects of acarbose and gastric distension (water preload) after oral sucrose in patients with PPH. (Commenced).
13. Trahair L, Gentilcore D, Rayner CK, Horowitz M, Jones KL. Effect of exogenous GLP-1 on the response to oral glucose in healthy older subjects. (Commenced).
14. Trahair L, Kimber T, Rigda R, Hausken T, Rayner CK, Thompson P, Horowitz M, Jones KL. PPH in Parkinson's disease - impact of gastric emptying and SMA flow. (Commenced).
15. Rajendran S, Trahair L, Visvanathan R, Rayner CK, Horowitz M, Jones KL. Cardiovascular responses to an oral glucose load in healthy subjects and PPH (to commence February 2013).

Summary/Final Reports and Progress Reports APP1066835 Rayner
16
Final report: NHMRC Project grant 565311: Effects of the fatty acid, lauric acid, on energy intake and gut motor and hormonal function in health and obesity. 2009 - 2012. Chief Investigators: Feinle-Bisset C, Horowitz M, Clifton PM, Rades T, Jones KL, Rayner CK The objectives of the project were to (i) characterise the GI mechanisms (ie oral, gastric, small intestinal, gut hormones) underlying the effects of nutrients (fatty acid) on appetite, (ii) determine the effects of oral formulations of C12 on appetite, energy intake, gastric emptying and gut hormone secretion in lean and obese subjects. The project was highly successful and has generated a large amount of data with a very high potential for translation into a public health outcome. As a result of this work we are now collaborating with an Australian biotech company that has the technical capabilities to produce a lauric-acid based formulation on a larger scale, which will enable us to perform a major clinical trial (funded by the company) to evaluate in a large cohort of obese individuals the effects on body-weight loss in the longer-term (6 - 12 months). The ultimate goal is to develop a TGA-registered product. Completed studies: Two studies have been completed and fully published (Publications (1), (2)). 3 major invited review articles have also resulted from this work (Publications (3)-(5)). 3 further studies, all relating to the effects of oral administration of lauric acid, have been completed and manuscripts prepared. These will be submitted for publication to high-impact journals, once all IP-related issues have been resolved. The studies are: (1) Dose-related effects of oral lauric acid administration on subsequent appetite and energy
intake. (2) Development of formulations that improve intragastric dispersion of lauric acid - effects on
acute energy intake in humans. (3) Effect of the timing of oral ingestion of lauric acid on subsequent energy intake. A sixth study evaluated the interactions between oral and small intestinal fatty acid exposure. This study has also been completed, and we are currently waiting for completion of the plasma analysis for gut hormones. The results will then also be summarised in a manuscript for publication. (4) Interactions between oral and small intestinal fatty acid exposure: effects on antropyloroduode-
nal pressures, gut hormone release, appetite and energy intake. Publications: (1) Seimon RV, Lange K, Little TJ, Brennan IM, Pilichiewicz AN, Feltrin KL, Smeets AJ,
Horowitz M, Feinle-Bisset C. Pooled-data analysis identifies pyloric pressures and plasma CCK concentrations as major determinants of acute energy intake in healthy lean males. Am J Clin Nutr 2010; 92: 61 - 68.
(2) Stewart JE, Seimon RV, Otto B, Keast RSJ, Clifton PM, Feinle-Bisset C. Marked differences in gustatory and gastrointestinal sensitivity to oleic acid between lean and obese men. Am J Clin Nutr 2011; 93: 703 - 711.
(3) Little TJ, Feinle-Bisset C. Oral and gastrointestinal sensing of dietary fat and appetite regulation in humans: modification by diet and obesity. Front Neurosci 2010; 4: 178.
(4) Stewart JE, Feinle-Bisset C, Keast RSJ. Fatty acid detection during food consumption and digestion: associations with ingestive behavior and obesity. Prog Lipid Res 2011; 50: 225 - 233.
(5) Little TJ, Feinle-Bisset C. Effects of dietary fat on appetite and energy intake in health and obesity - oral and gastrointestinal sensory contributions. Physiol Behav 2011; 104: 613 - 620.

Summary/Final Reports and Progress Reports APP1066835 Rayner
17
Final report: NHMRC Project grant 565312: Gastrointestinal function and appetite in obesity – acute and longer-term effects of changes in energy intake. 2009 - 2012. Chief Investigators: Feinle-Bisset C, Clifton PM, Horowitz M, Jones KL, Wittert GA This grant focussed on the broad hypothesis that, in response to dietary changes (energy restriction, or overconsumption in obesity), the sensitivity to nutrients in the gastrointestinal (GI) lumen is modified, associated with alterations in the GI mechanisms (gastric emptying and intragastric meal distribution, small intestinal transit, antropyloroduodenal motility and GI hormone secretion) that regulate appetite and energy intake and blood glucose control. Completed and published studies: (1) Comparative effects of fat and carbohydrate on appetite and energy intake. (Publications (1)) (2) Reproducibility of energy intake, gastric emptying, blood glucose, plasma insulin and
cholecystokinin responses in healthy young males. (Publications (2)) (3) Effects of acute dietary restriction on gut motor, hormone, and energy intake responses to
duodenal fat in obese men. (Publications (3)) (4) Comparative appetite-suppressant effects of high-carbohydrate, -protein or -fat meals in lean
and obese. (Publications (4)) (5) Acute effects of oral nutrients on gastric emptying, small intestinal transit, gut motility, GI
hormones, appetite and energy intake in lean, overweight and obese subjects. (Publications (5)) Completed, but not yet published studies: (6) Effects of the energy density of meals on appetite and energy intake in overweight men. Manuscript has been submitted for publication (Publications (6)). (7) Effects of acute energy restriction in lean and obese subjects, and long-term (12 weeks) energy
restriction in obese subjects, on GI motility, gut hormones, appetite and energy intake in response to duodenal nutrients. Manuscript is in preparation and will be submitted in March 2013.
Publications: (1) Seimon RV, Feltrin KL, Meyer JH, Brennan IM, Wishart JM, Horowitz M, Feinle-Bisset C.
Effects of varying combinations of intraduodenal lipid and carbohydrate on antropyloroduo-denal motility, hormone release and appetite in healthy males. Am J Physiol Regul Integr Comp Physiol 2009; 296; R912 - R920.
(2) Nair NS, Brennan IM, Little TJ, Gentilcore D, Hausken T, Jones KL, Wishart JM, Horowitz M, Feinle-Bisset C. Reproducibility of energy intake, gastric emptying, blood glucose, plasma insulin and cholecystokinin responses in healthy young males. Br J Nutr 2009; 101: 1094 - 1102.
(3) Brennan IM, Seimon RV, Luscombe-Marsh ND, Otto B, Horowitz M, Feinle-Bisset C. Effects of acute dietary restriction on gut motor, hormone, and energy intake responses to duodenal fat in obese men. Int J Obes 2011; 35: 448 - 456.
(4) Brennan IM, Luscombe-Marsh ND, Seimon RV, Otto B, Horowitz M, Wishart JM, Feinle-Bisset C. Effects of fat, protein and carbohydrate, and protein load, on appetite, plasma cholecystokinin, peptide YY and ghrelin, and energy intake in lean and obese men. Am J Physiol Gastrointest Liver Physiol 2012; 303: G129 - G140
(5) Seimon RV, Brennan IM, Russo A, Little TJ, Jones KL, Standfield S, Wishart JM, Horowitz M, Feinle-Bisset C. Gastric emptying, mouth-to-cecum transit, glycemic, insulin, incretin and energy intake responses to a mixed-nutrient liquid in lean, overweight and obese males. Am J Physiol Endocrinol Metab 2013; 304: E294 - E300.
(6) Luscombe-Marsh ND, Seimon RV, Bollmeyer E, Bellon M, Wishart JM, Horowitz M, Feinle-Bisset C. Effects of a high- vs low-energy density protein preload on appetite and energy intake, upper gut function and thermogenesis in overweight men. Asia Pac J Nutr (submitted 3. December 2012).

Summary/Final Reports and Progress Reports APP1066835 Rayner
18
Progress report: NHMRC Project Grant 1025186: Optimising nutrient delivery and absorption in critically ill patients 2012 - 2014. Chief Investigators: Chapman MJ, Nguyen NQ, Horowitz M, Rayner CK, Jones K and Deane AM
The objectives of this project grant are to improved understanding of: (i) absorption of nutrient administered into the stomach & small intestine; (ii) differential absorption of the different macronutrients; and (iii) effects of small intestinal motility, mucosal architecture, mesenteric blood flow and gut hormones on the rate & extent of nutrient absorption.
The studies supported by this grant are proceeding efficiently.
Completed studies: (1) Comparative effects on glucose absorption of intragastric and postpyloric nutrient delivery
in the critically ill (published). (2) Effect of erythromycin on small intestinal nutrient absorption and transit in critically ill
patients (published) (3) Sucrose Malabsorption and Impaired Mucosal Integrity in Enterally Fed Critically Ill
Patients: A Prospective Cohort Observational Study
Studies currently ongoing: (1) Effects of meal composition on pyloric activity, gastric emptying & humoral profile.
(currently recruiting)
Original papers: (1) Comparative effects on glucose absorption of intragastric and postpyloric nutrient delivery
in the critically ill. Di Bartolomeo AE, Chapman MJ, Zaknic AV, Summers MJ, Jones KL, Nguyen NQ, Rayner CK, Horowitz M, Deane AM. Critical Care 2012 Sep 17;16(5):R167
(2) Effect of erythromycin on small intestinal nutrient absorption and transit in critically ill patients. Deane AM, Wong GL, Horowitz M, Zaknic AV Summers MJ, Di Bartolomeo AE, Sim JA, Maddox AF, Bellon MS, Rayner CK, Chapman MJ, Fraser RJL. American Journal of Clinical Nutrition. 2012 95: June: 1396-1402
(3) Sucrose Malabsorption and Impaired Mucosal Integrity in Enterally Fed Critically Ill Patients: A Prospective Cohort Observational Study. Burgstad CM, Besanko LK, Deane AM, Nguyen NQ, Saadat-Gilani K, Davidson G, Burt E, Thomas A, Holloway RH, Chapman MJ, Fraser RJL. Critical Care Medicine (in press: accepted 13 October 2012)
Reviews:
(1) Gastrointestinal dysmotility: evidence and clinical management. Chapman MJ, Nguyen NQ, Deane AM. Curr Opin Clin Nutr Metab Care. 2013 Mar; 16(2):209-16

Summary/Final Reports and Progress Reports APP1066835 Rayner
19
Progress Report: NHMRC Project Grant 627178: The effects of testosterone and a nutritional supplement on hospital admissions in under-nourished, older people. I Chapman, R Visvanathan, V Naganathan, P Hunter, J Karnon, M Horowitz. 2010-2013 with one year extension granted.
Commenced in 2010, recruitment has closed in South Australia and Victoria. 44 subjects have been recruited in South Australia, 1 in Victoria and 7 in New South Wales (NSW)- i.e. 52 subjects. Some delays faced in Victoria and NSW with ethics approval and recruitment has been slow across all 3 states. This is despite extensive newspaper advertising and several media appearances by thei investigators. In South Australia 252 subjects have been screened, 49 assessed and 44 recruited (17.5% recruitment rate). In Victoria 65 subjects were screened, 2 were assessed and only 1 recruited. In NSW to date, 100 subjects screened and 7 assessed and 7 recruited. Total number subjects enrolled is 51. Given that the subject in Victoria had withdrawn, the study has now stopped in Victoria as a result of the very poor recruitment rate. In South Australia, recruitment has closed and subjects are completing their 12 month participation and follow-up period. In NSW, recruitment is continuing because of the delayed start and the research team will review the rate to determine period of further recruitment.
To have a power of 90% to detect a significant (at P = 0.05 [2-sided]) difference in the number of days of hospitalization between the treatment groups 28 subjects per group are required (n=56). Therefore, the researchers are confident that this sample size will be achieved. Publications arising from the project:
1. Chapman IM. Weight loss in older persons. Med Clin North Am. 2011 95:579-93. Review.
2. Piantadosi C, Visvanathan R, Naganathan V, Hunter H, Cameron ID, Lange K, Karnon J, Chapman IM. The effect of testosterone and a nutritional supplement on hospital admissions in under-nourished, older people. BMC Geriatrics. 2011 11:66.

Summary/Final Reports and Progress Reports APP1066835 Rayner
20
Final report: NHMRC CCRE Grant 453557: Centre of Clinical Research Excellence in Nutritional Physiology, Interventions and Outcomes. 2007 - 2012. Chief Investigators: M Horowitz, PM Clifton, GA Wittert, IM Chapman, RJ Fraser, CK Rayner, C Feinle-Bisset, KL Jones The success of the Centre was overall outstanding, and a formal final report relating to outcomes in 2012 will be submitted to the NHMRC by the end of March 2013. Major achievements are outlined below: Research The productivity of the Centre has been enhanced by formalising collaborations with investigators of the Diabetes Centre of Clinical Research Excellence (Melbourne). We have built our capacity through a number of collaborations with the University of Adelaide School of Nursing (Professor Alison Kitson), and with Health Psychology (Professor Deborah Turnbull). As of January 2013, 382 peer-reviewed papers have been published by the CCRE Chief Investigators (63 in 2007, 56 in 2008, 59 in 2009, 57 in 2010, 62 in 2011, 85 in 2013 and 9 to date in 2013); the majority have capitalised on collaborations that have developed or been strengthened by the formal links that this funding scheme has enabled during the period of CCRE funding. Training The majority of CCRE funding supports early career researchers who are establishing a track record to enable them to compete successfully for independent research funding. The evidence for the success of this approach has been the success of a number of our Postdoctoral Fellows in obtaining independent funding in the form of New Investigator Project Grants since 2010. We have also provided support in the form of mentoring and financial support to 9 investigators who have obtained independent funding. In 2012 the Centre has supported 4 postdoctoral fellows, 11 PhD students, and 3 physicians pursuing a Masters in Philosophy in clinical research, 1 who has upgraded to a PhD. A regular series of research seminars was instigated in 2007 and this has substantially raised the profile of the CCRE. A new Research Forum was instigated in 2011. This forum has proved a major success in providing a focal point for all researchers involved in nutrition research in South Australia, and a forum for numerous visiting international speakers. Translation The translational strategies of the group (involvement in the media, dietary publications for the public, health policy, rollout of obesity management software, etc.) are proceeding according to plan.

Track Record APP1066835 Rayner
21
Team Quality and Capability. The team consists of four CIs, who bring together international reputations in gut physiology and clinical trials of dietary interventions, and an AI who is a professional biostatistician, all of whom are active in an NHMRC Centre of Research Excellence in Translating Nutritional Science to Good Health (2013-17). Elements and expertise of the team The project capitalises on the complimentary expertise and skills of the CIs. CIA Rayner is a gastroenterologist with an interest in nutrient-gut interactions, and in particular, the stimuli that drive gut peptide secretion. CIC Horowitz an endocrinologist who pioneered the notion of upper gut function being of central importance to glycaemic control, while CID Jones trained in Nuclear Medicine and is a leading authority on the measurement and manipulation of gastric emptying. These three CIs have developed the concept of macronutrient preloads as a means of harnessing nutrient-gut interactions to reduce the glycaemic response to a subsequent meal, based on the physiology of gastric emptying and gut hormone release. CIB Clifton is a metabolic physician with a distinguished record of devising, and evaluating, nutritional treatments for metabolic disease. He has led over 100 clinical research trials in this area, with a particular emphasis on the effects of high protein diets for weight loss and glycaemic control. He was a co-author with the other CIs on a paper describing the acute effects of whey protein preloads on postprandial glycaemia in type 2 diabetes (Ma et al. Diabetes Care 2009; 32: 1600-02). This team is now optimally placed to translate the knowledge derived from acute physiological studies to a larger scale, longer-term trial. All the CIs are experienced at recruiting and screening patients with type 2 diabetes for inclusion in clinical trials, and CIB, in particular, has led numerous trials of a size and duration comparable to the current proposal. The CIs have expertise in the required techniques, all of which are established in their laboratory. They will also draw on the biostatistical expertise of Ms Kylie Lange, who is employed full-time by their CRE. Productivity of team members All the CIs are in the top tier of research productivity, with a combined output of more than 700 peer-reviewed papers, > 190 of which have been cited ≥ 50 times, and they publish regularly in the highest ranking journals in the fields of diabetes, nutrition, and gastroenterology. They have a record of being able to translate the physiological principles of disease management into practical strategies suitable for widespread implementation, such as CIB Clifton’s CSIRO Total Well Being Diet books. Influence in this field of research CIs A, C, and D are recognised as members of a world-leading group in the area of gut function in diabetes, as reflected in regular invitations to speak at international forums and contribute reviews and practice guidelines. CIB is an authority on nutritional interventions to combat chronic disease, and his research has been instrumental, eg. in the withdrawal of trans fatty acids from Australian margarine. CIA’s acute dietary intervention studies generated substantial media interest, while CIB is regularly sought for comment on television and radio on nutritional issues. His CSIRO Total Well Being Diet books 1 and 2, based on the outcome of 5 high protein weight loss studies, have sold over one million copies in Australia and been translated into multiple foreign languages. How the team will work together All the CIs are co-located in, or in close proximity to, the Royal Adelaide Hospital campus and meet at least weekly, having shared CI status on a highly productive CCRE (2007-12) and now on their newly established CRE. CIA Rayner will take overall responsibility for the project, with close assistance from CIB Clifton. CID Jones will supervise the collection and analysis of gastric emptying data, and CIC Horowitz will contribute to data analysis and overall intellectual input. AI Lange has been involved in designing the study, including determination of the sample size and analysis plan, and will be closely involved in the management of data collection and storage, as well as the final statistical analysis.

Track Record APP1066835 Rayner
22
CIA: Associate Professor Chris Rayner A/Prof Rayner is the Gwendolyn Michell Associate Professor in the Discipline of Medicine, University of Adelaide, and a Consultant Gastroenterologist at the Royal Adelaide Hospital. Since his return in 2004 from postdoctoral training at St Mark’s Hospital, London, he has been building an international profile in the field of nutrient-gut interactions, with an emphasis on the role of upper gut function in the pathophysiology and management of diabetes mellitus. He has taken the leadership role in the group investigating this area at the University of Adelaide, established by Prof Michael Horowitz. Funding: A/Prof Rayner is a Chief Investigator on two current NHMRC Project Grants, and played a major role in securing 10 years of NHMRC funding for an NHMRC Centre of Clinical Research Excellence (CCRE) in Nutritional Physiology (2007-12) and subsequently a CRE in Translating Nutritional Science to Good Health (2012- 17), on both of which he is a Chief Investigator. He has been CIA on a NHMRC Project Grant (627139, 2010-12) investigating relationships between upper gastrointestinal function and glycaemic control in diabetes mellitus, and a CI on 3 previous NHMRC project grants. He has also received competitive funding from Diabetes Australia, the University of Adelaide, the Royal Adelaide Hospital, the Rebecca L Cooper Foundation, and the Intensive Care Foundation, and has been a CI on grants that have generated over $9.4 million in funding. Publications: He has published over 100 peer-reviewed papers and 7 book chapters, the majority as either first or senior author. His ‘h-index’ is 25. Key publications have included a review in Diabetes Care (cited over 200 times) and an invited editorial for the Journal of Clinical Investigation, which have expressed the fundamental philosophy of his group, that the gut is central to glycaemic control. A seminal paper with Dr R Young, published in Gut in 2009, marks the initiation of an exciting basic science collaboration examining carbohydrate sensing in the gut. International and national profile: His scholarship was recognised by selection as an “emerging leader in gastroenterology” by AstraZeneca in 2002, and the award of Hanson Institute New Clinical Science Investigator in 2005. His research has been enhanced by forming and maintaining extremely productive collaborations with senior international colleagues, including Prof Andre Smout (The Netherlands), Prof James Meyer (USA), Prof Trygve Hausken (Norway), and recently, Profs Michael Nauck and Juris Meier (Germany). In addition to local and national presentations, he has given international invited presentations for the Joint International Neurogastroenterology and Motility Meeting (Switzerland), St Mark’s Hospital (London, UK), and the University of Essen (Germany). Research translation: Formal collaboration with other investigators from basic science and dietary intervention backgrounds through the CRE has created unprecedented opportunities for A/Prof Rayner to translate molecular mechanisms to human pathophysiology (particularly in the area of small intestinal glucose sensing, with Dr R Young in the Royal Adelaide Hospital Nerve Gut laboratory); this approach is now being extended to patients with critical illness and to identification of intestinal fat sensors and their modulation in obesity and with dietary changes, in collaboration with emerging young investigators in the group. A/Prof Rayner is also developing dietary strategies, based on emerging principles of gut physiology, for subsequent evaluation in clinical trials – for example, the use of defined “preloads” to stimulate gut feedback mechanisms in advance of a main meal, and thereby attenuate the subsequent glycaemic excursion. Training: He is currently supervising four PhD students, who are all medical graduates with subspecialty training in gastroenterology, endocrinology, and paediatric endocrinology. He has previously supervised a further 4 PhD students (one awarded a University Doctoral Research Medal in 2010) and an Honours student. He coordinates a structured Honours Program for the School of

Track Record APP1066835 Rayner
23
Medicine, University of Adelaide, and through the CRE is increasingly involved in mentoring postdoctoral researchers in the establishment phase of their careers. He has supervised several clinical fellows from the Asia-Pacific region, and has extensive involvement in the undergraduate medical curriculum and the postgraduate training of physicians. Contributions to profession relating to research: A/Prof Rayner has served as an external reviewer of NHMRC Project Grants (2008, 2010, 2011), and on NHMRC Grant Review Panels (2010, 2011). He has reviewed grants for the Diabetes Australia Research Trust, Sheffield Hospitals Charitable Trust, Ophthalmic Research Institute of Australia, Women's and Children's Hospital Foundation, and the Foundation for High Blood Pressure Research. He has served as a peer reviewer for 40 different journals. Commercial: A/Prof Rayner is responsible for a number of investigator-initiated trials with pharmaceutical companies involved in gut hormone-related therapies (Lilly, Merck); some of these represent collaborations with small pharma companies to establish proof-of-concept in phase I studies (Satiogen, Meyer Nutriceuticals).

Track Record APP1066835 Rayner
24
CIB: Professor Peter Clifton Qualifications MBBS Melbourne University 1975 B Med Sci, Melbourne University 1975 Membership Royal College of Physicians (UK) 1979 PhD Department of Medicine, Flinders University of South Australia 1988 Fellowship Royal Australasian College of Physicians 1986 Awards: Fellowship of the Nutrition Society of Australia 2009 Distinguished Alumnus of Flinders University 2006 CSIRO Medal for Scientific Excellence 2005 CSIRO Medal for Business Excellence 2005 Current Appointments: NHMRC Senior Research Fellow 2012 - 2017 Baker IDI Heart and Diabetes Institute Laboratory head, Nutritional Interventions, July 2009 to Feb 2013 Professor of Nutrition, University of South Australia Feb 2013 Clinical Positions: Physician (Senior Lecturer) at Flinders Medical Centre responsible for the Lipid Disorders Clinic 1987 to date Physician (Professor of Medicine) at Royal Adelaide Hospital in Endocrine Clinic 1998 to date Affiliate Positions: Professor, Department of Medicine, Royal Adelaide Hospital 1998 to date Professor, Department of Physiology, University of Adelaide 2005 to date Professor, School of Pharmacy & Medical Sciences & Sansom Health Research Institute, University of South Australia 2011 to date Track Record: Prof Clifton is an NHMRC Principal Research Fellow, general physician and endocrinologist with a major interest in the nutritional treatment of lipid disorders and CVD and its antecedents type 2 diabetes and obesity. He has affiliate professorial titles at all 3 universities in Adelaide and clinical appointments at the Royal Adelaide Hospital and Flinders Medical Centre. He is recognised in Australia as an expert in clinical nutrition, lipids & chronic disease prevention & treatment. He was made a Fellow of the Nutrition Society of Australia in 2009. Prof Clifton is frequently sought by the media to comment on nutritional issues and has regular ABC radio slots. From 1990 to 1999 he led the nutritional research effort at CSIRO guiding 13 scientists in Adelaide and 6 on other CSIRO sites. He has been responsible for designing, funding and leading over 100 clinical trials in the last 23 years with a clear logical hypothesis driven pathway from lipid composition to macronutrient manipulation and weight loss for global risk reduction. The contributions with the most impact include the demonstration of the effect of trans fatty acids on Lp(a) levels (world first), the relationship between trans fatty acid intake and first heart attack (the only study in Australia), the effect of weight loss on CRP levels (world first), the effect of Atkins style weight loss diets on LDL cholesterol levels and flow mediated dilatation (very convincingly negative) and the effect of high salt diets on flow mediated dilatation (world first). One of the most direct effects of his research was the withdrawal of trans fatty acid containing margarines in Australia by Goodman Fielder following the results of his “First Heart Attack Study”. He also contributed to the evidence base for the effectiveness of plant sterols with 3 trials for Australian companies and 5 trials for international companies. After performing 5 high protein weight loss studies he co-authored the CSIRO Total Well Being Diet books 1 and 2 which have sold over one million copies in Australia and has led to over 400,000 Australians over 45 following the diet and losing an average of 6Kg over 6 months (Wyld et al 2010). A CSIRO Healthy Heart Book was published in 2008 and a combined Baker IDI/CSIRO Diabetes book appeared in 2011. His research group published the largest body of work on the effects of a high protein diet for weight loss (over 100 publications) and are highly cited in this area. Target groups of interest have included groups

Track Record APP1066835 Rayner
25
with insulin resistance, metabolic syndrome, type 2 diabetes and polycystic ovary syndrome. His current research is on the effect of high protein weight loss diets on bone density in post-menopausal women and renal function in people with type 2 diabetes and early renal disease. He is also actively researching diet choice and efficacy of weight loss. Research Output: Prof Clifton has a large body of primary research papers (>200), an H index of 44, and >5000 citations with an average of 28 citations per research publication with 450 citations/year over the last 3 years. His review articles have an average citation of 62 with >100 citations in 2010. Grant Success: CSIRO became eligible for NHMRC project grants in 2004. Since then he has been CIA on 2 grants and CI on 3 others. He obtained 6 NHF grants and 2 DART grants and one Hoechst diabetes grant. In addition he has had industry grants worth a total of over $10m. Research supervision and mentoring: He has mentored 20 PhD students (5 of whom are current, 15 to completion) and the majority are continuing actively in research, some at Associate Professor level and have published 2-3 papers from their PhD. He also supervises 2-3 Honours students/year from the Flinders University Dietetics course for their research placement which frequently leads to publications for them. Contribution to NHMRC/scientific community: He has been a NHMRC grant reviewer for over 20 years and has been invited to be on grant review panels over the last 3 years. He has also been a grant reviewer for the National Heart Foundation and for national funding bodies in Israel and Austria. He reviews about 50 papers per year for a wide variety of scientific journals and provides regular nutritional update sessions for general practitioners, dietitians, diabetes educators and cardiac rehabilitation nurses. Relevant skills: His skills relevant to this project include clinical epidemiology, the design and analysis of a wide range of trials in which biomarkers play a significant role for patients with diabetes and/or CVD in clinical practice

Track Record APP1066835 Rayner
26
CIC: Professor Michael Horowitz Professor Michael Horowitz (age 59) was appointed to a Personal Chair at the University of Adelaide in 1995, and has been the Director of the Endocrine and Metabolic Unit at the Royal Adelaide Hospital since 1997. His research activities are almost exclusively clinically based and relate primarily to gastrointestinal motor, sensory and hormonal function, particularly in the context of diabetes mellitus/glycaemic control, critical illness, aging and appetite regulation. He led the NHMRC Centre of Clinical Research Excellence (CCRE) in Nutritional Physiology (2007-12) and the subsequent NHMRC Centre of Research Excellence (CRE) in Translating Nutritional Science to Good Health (2012 – 17). Prof Horowitz has, accordingly, effectively integrated his clinical career with a comprehensive, clinically-based, research programme and has a proven leadership record in both the management of research teams and service delivery. Funding: His research programmes have been supported by the NHMRC on a continuous basis since 1984 (as CI on 32 project grants) to a total of $14,183,663. During the last five years he has also had support from the NIH, Diabetes Australia Research Trust, the Rebecca L. Cooper Medical Research Foundation and the Clive and Vera Ramaciotti Foundations. Publications: He is a co-author of 525 peer-reviewed papers and 37 book chapters and publishes consistently in the top ranking journals relating to gastroenterology (Gastroenterology, Gut, American Journal of Physiology), diabetes (Diabetes Care, Diabetologia), endocrinology (Journal of Clinical Endocrinology and Metabolism) and nutrition (American Journal of Clinical Nutrition). At least 152 of these papers have been cited ≥ 50 times, placing him in the top 1% of cited authors in clinical medicine world-wide. His ‘h’ index is 79. He is co-editor (with Professor M Samsom) of as multi-author book entitled: ‘Gastrointestinal function in diabetes mellitus’, which represents the most comprehensive treatise on this subject. International and national profile: He has had extensive involvement as speaker at international and national scientific meetings, and has been an invited Plenary, or Symposium, speaker at international conferences on 75 occasions, including the annual meetings of the American Diabetes Association, American Gastroenterological Association, European Association for the Study of Diabetes, Scandinavian Society for the Study of Diabetes, World Congresses of Gastroenterology, World Diabetes Congress, Swedish Diabetes Society and the American Motility Society. A particular highlight was the invitation to present one of four ‘State of the Art’ lectures at the European Association for the Study of Diabetes Meeting in Vienna (1996). He has also been the recipient of a number of awards relating to research, including the Elder Prize for Scholarship at the University of Adelaide (1995), the Distinguished Research Prize of the Gastroenterological Society of Australia (1999), the Eric Susman Prize of the Royal Australasian College of Physicians (2000), the Dintenfass Award of the Rebecca L. Cooper Medical Research Foundation (2000, 2005), the Kellion Award for outstanding contribution to diabetes research of the Australian Diabetes Society (2009) and a Masters Award provided by the American Gastroenterological Association for Sustained Achievement in Digestive Sciences (2010). He has active international research collaborations with colleagues in Los Angeles and St Louis, USA, Bochum, Germany and Bergen, Norway. He was a member of the Toronto Diabetic Neuropathy Expert Group (2010), which was responsible for the development of consensus guidelines. Research translation: Prof Horowitz has shown consistent ability to translate applied science into clinical outcomes. He is recognised as the leading authority in the area of disordered gastrointestinal motility in type 1 and type 2 diabetes and the author of current guidelines for itsinvestigation and management in the on-line text ‘Up to Date’. An increasing focus of this work, which is now directed primarily by A/Prof Chris Rayner, has related to the impact of gastric emptying on glycaemic control in diabetes, which has hitherto been essentially ignored and now shown to be of great importance. In collaboration with Prof John Dent, Prof Horowitz performed a series of studies focussing on normal and disordered gastric motility which contributed to the recognition that chronic gastroparesis is a common, and clinically important, condition. This lead to the development of techniques (eg radionuclide and manometric) for diagnostic purposes and resulted in improved

Track Record APP1066835 Rayner
27
approaches to management, including the use of novel pharmacotherapy, including cisapride, domperidone and erythromycin. Prof Horowitz has made important contributions to an ongoing research programme, directed by Prof Ian Chapman, focussing on the so-called ‘anorexia of aging’. The outcome of these studies has lead to the development and application of novel strategies for the prevention and management of impaired nutrition, and its concomitant adverse sequelae, in this group. Prof Horowitz has played an important role in an ongoing research programme, directed primarily by Prof Christine Feinle-Bisset focussing on the gastrointestinal determinants of appetite in health and the obese. The outcome of these studies has resulted in novel strategies for the management of obesity, which are under current evaluation. Prof Horowitz has made important contributions to an ongoing research programme, directed by Prof Karen Jones, focussing on the relevance of gastric and small intestinal function to the regulation of postprandial blood pressure. The insights derived from this work have resulted in the development of novel strategies for the management of postprandial hypotension, a common and clinically important condition, postprandial fall in blood pressure. Prof Horowitz has made important contributions to an ongoing research programme, directed primarily by A/Prof Marianne Chapman and Dr Adam Deane, focussing on the impact of critical illness on gastrointestinal function, nutritional status, and glycaemic control. Recent studies indicate that the hormone, glucagon-like-peptide-1, has the potential to be useful in the management of hyperglycaemia in this group. Training: Prof Horowitz has extensive experience in clinical research training/mentoring and it is in this area that he has arguably made his major contribution to research. He has supervised 33 PhD or MD candidates from medical, science, nuclear medicine, nursing and dietetic backgrounds and 16 postdoctoral research fellows (the latter have been from the UK, the Netherlands, Germany and Singapore as well as Australia). A number of his former PhD students now occupy senior positions and have obtained independent research funding including: (i) Prof R Fraser, Director of Gastroenterology, Flinders Medical Centre; (ii) A/Prof G Hebbard, Director of Gastroenterology, University of Utrecht, the Netherlands; and (iii) A/Prof Chris Rayner, the University of Adelaide. He plays a pivotal role in the CRE to support the training of clinical researchers. He also played a major role in establishing a research project as part of the 4th year medical (MBBS) curriculum at the University of Adelaide and in training doctors working in South East Asia in the clinical and research relevance of gastrointestinal motility. Contributions to profession relating to research: He has made major contributions to the Gastroenterological Society of Australia, the Australian Diabetes Society, the Endocrine Society of Australia, the Royal Australasian College of Physicians, the Royal Adelaide Hospital and the University of Adelaide. Prof Horowitz is currently Chairman of the Research Advisory Committee of the Royal Australasian College of Physicians, a member of its Research and Education Foundation and Chairman of the Royal Adelaide Hospital Project Grants Committee, as well as a member of its Research Committee. He is also a member of the Research Committees of the Faculty of Health Sciences, University of Adelaide and the Queen Elizabeth Hospital. He was Chairman of the CSIRO Division of Human Nutrition Human Ethics Committee from 2002-9. Prof Horowitz has been a regular member of the NHMRC Grant Review Panels and was Chairman of Panel 3e in 2007. He is currently a member of the Editorial Boards of 11 international journals, Editor-in-Chief of The Open Physiology Journal and has reviewed manuscripts for 64 scientific journals. Commercial: Prof Horowitz is a member of a number of national and international Advisory Boards relating to the pharmaceutical industry and has been a regular invitee to the annual Merck Diabetes Global Therapeutic Expert Forum. He has been primarily responsible for the conduct of ~22 investigator-initiated trials, relating particularly to the pharmacological management of diabetic gastroparesis.

Track Record APP1066835 Rayner
28
Professor Karen Jones Professor Karen Jones (age 42) has had a substantial involvement in clinical research for ~21 years. Her initial training was as a nuclear medicine technologist in which she was awarded the prize for the top nuclear medicine student in 1991. She subsequently graduated with a PhD in 1998 (the first nuclear medicine technologist in Australia to do so). Between 1999 and 2002, she held the Dr Paul Janssen Senior Lectureship in the Department of Medicine, University of Adelaide, prior to being the recipient of an NHMRC/Diabetes Australia Career Development Award in 2003 and was subsequently awarded an NHMRC Senior Clinical Career Development Award in 2010, for which she received a prestigious NHMRC Achievement Award as the highest ranked candidate in her category that year. Professor Jones’ primary research interests relate to the relevance of upper gastrointestinal function to (i) postprandial hypotension (PPH) and (ii) diabetes mellitus. PPH occurs in ~50% of nursing home residents and increases the risk of falls, stroke and mortality. The pathophysiology is poorly defined and current therapies less than optimal. She has been primarily responsible for seminal observations that the hypotensive response to a meal is triggered by the interaction of nutrients with the small intestine and that, conversely, gastric distension attenuates the fall in blood pressure, which have major therapeutic implications. Her research relating to diabetes has yielded numerous important insights – arguably the most important of these is that disordered gut function occurs frequently and is both a determinant of, as well as determined by, the blood glucose concentration. This research group is generally recognised as the world leader in this area. During the last 5 years Professor Jones has assumed a leadership role, including primary responsibility for her own research programme, while continuing to work as part of an internationally recognised research group. This has been achieved despite the pressures of raising her 4 young children and two periods of maternity leave in the past 3 years. Funding: Professor Jones is currently a CIA on one NHMRC project grant (NHMRC 627189: 2010-2013), focussing on the role of gastric and small intestinal mechanisms in postprandial blood pressure regulation and another (CIE) relating to optimising nutrient delivery and absorption in the critically ill (NHMRC 1025186: 2012-2014). All areas of research have capitalised on the development of state-of-the-art radioisotopic and ultrasound (2D, 3D, Doppler) techniques to evaluate gastric motor function, and have attracted international recognition. Professor Jones was also a CI on the NHMRC CCRE in Nutritional Physiology, Interventions and Outcomes (NHMRC 453557: 2007-2011) and is a current CI on the NHMRC CRE - Translating Nutritional Science to Good Health (NHMRC 1041687: 2012-2017). In the last decade Professor Jones has been involved in attracting over $6,000,000 in research funds from peer-reviewed sources including the NHMRC, Diabetes Australia Research Trust, the Rebecca L. Cooper Medical Research Foundation and the Royal Adelaide Hospital Research Foundation. Publications: Professor Jones is a co-author of 114 original peer-reviewed papers, 28 reviews, 3 letters and 7 book chapters. She publishes consistently in the top ranking journals relating to gastroenterology (Gastroenterology, Gut, American Journal of Physiology), diabetes (Diabetes Care, Diabetologia), endocrinology (Journal of Clinical Endocrinology and Metabolism) and nutrition (American Journal of Clinical Nutrition). At least 34 of her papers have been cited at least 50 times, she has a total of 4798 citations and her ‘h’ index is 40. International and national profile: Professor Jones has made presentations at local, national and international meetings. In 1998, she was an invited plenary lecturer at the 7th World Congress of Nuclear Medicine and Biology, Berlin and was the keynote speaker at the Victorian Nuclear Medicine Technologist Seminar Programme in 2007. In 2008 she was an invited speaker at the 6th World Congress on The Aging Male, Tampa, Florida, USA, in January 2009, an invited speaker at the AGA Institute course on Gastroparesis and Functional dyspepsia, Orlando, Florida, USA and in June 2009 an invited speaker at the 40th Nordic Gastroenterology meeting in Stavanger, Norway. In 1999, she was the recipient of the ANSTO Award, for ‘outstanding research yielding new and significant data’ (the only nuclear medicine technologist to receive the award) and in 2010 received an NHMRC Achievement Award. She was promoted to full Professor in 2011.

Track Record APP1066835 Rayner
29
Research translation: Professor Jones’ research focussing on gastric and small intestinal function to the regulation of postprandial blood pressure has resulted in the development of novel strategies for the management of postprandial hypotension, a common and clinically important condition. In particular she is performing studies in patients with postprandial hypotension to investigate the therapeutic benefits of acarbose and gastric distension to attenuate the magnitude of the postprandial fall in blood pressure. She hopes to translate her acute to chronic, studies designed to address issues of fundamental clinical significance in this patient group. Training: Professor Jones has hitherto supervised 8 honours and 7 completed PhD students; two of her PhD students were awarded the University of Adelaide Postdoctoral Medal for outstanding work in their PhD thesis. She currently supervises 2 PhD students. She plays a major role in supporting the training of future clinical researchers and plays a pivotal role in identifying and training individuals, particularly those with a medical imaging (nuclear medicine/ultrasound) background, who have excellent research potential. This is facilitated by her established links with the Australian and New Zealand Society of Nuclear Medicine (ANZSNM) and the School of Medical Imaging, University of South Australia. Contributions to profession relating to research: Professor Jones has reviewed applications for NHMRC postgraduate training scholarships (in 2007 and 2008 she was the chairperson of her panel), NHMRC Career Development Fellowships and grant applications for the University of South Australia. She was a member of the Editorial board of The Open Geriatric Medicine Journal and has reviewed manuscripts for at least 13 journals. She has made major contributions to the nuclear medicine profession and believes that she is a role model for other nuclear medicine technologists; several of her former Honours and PhD students have a background in medical imaging. Commercial: Professor Jones has been primarily responsible for several investigator-initiated trials, relating particularly to the pharmacological management of patients with diabetes.
Recommended