Letter to the Editor
Further Family With Possible AutosomalRecessive Inheritance of Adams-Oliver Syndrome
To the Editor:
In a recent issue, Klinger and Merlob [1998] reportedon 2 sibs with Adams-Oliver syndrome and possibleautosomal recessive inheritance. They note that mostreports on Adams-Oliver syndrome demonstrate auto-somal dominant pedigrees. Three families includingtheir family suggest autosomal recessive inheritance[Kahn and Olmedo, 1950; Koiffmann et al., 1988]. Inthe report by Koiffmann et al. [1988] parental consan-guinity provided additional support for an autosomalrecessive pattern. Autosomal dominant inheritancewith clear vertical transmission and many examples ofmale-to-male transmission has been well documentedin Adams-Oliver syndrome [Whitley and Gorlin, 1991].However, reduced penetrance with variable clinical ex-pressivity has been described in several families withautosomal dominant inheritance [Bamforth et al.,1994; Scribanu and Temtamy, 1975; Sybert, 1985].
We would like to report on a Turkish family with 2affected sibs and unaffected consanguineous parents asfurther evidence of recessive inheritance in at leastsome families.
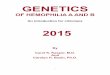
The proposita was the fifth child of a 33-year-oldmother and a 40-year-old father who were second cous-ins. The mother did not have prenatal care. The femaleinfant was born by normal vaginal delivery at term.Birth weight, length, and head circumference were2650 g (25%), 50 cm (50%), and 35 cm (50%), respec-tively. The patient was diagnosed as having Adams-Oliver syndrome because of a large scalp defect withabsence of underlying skull, prominent scalp veinswith a tortuous pattern, cutis marmorata, and termi-nal transverse limb defects in four limbs (Fig. 1, 2).Cranial CT did not show any abnormality other thanthe skull defect. Abdominal ultrasound and echocardi-ography did not demonstrate any abnormalities. Thepatient’s scalp defect covered itself almost completelywith granulation tissue by 2 months. She died at homeat 4 months. Autopsy was declined. Examination of theparents and 4 sibs showed an 8-year-old brother who
had a short left hallux and an atrophic area of skinwith alopecia on the vertex presenting since birth. Hisfindings were consistent with the diagnosis of Adams-Oliver syndrome. There were no other individuals withthese types of findings in the family.
Three families with Adams-Oliver syndrome havebeen reported previously in which autosomal recessiveinheritance is more likely than autosomal dominantinheritance. In the report by Kahn and Olmedo [1950],2 affected sibs and normal parents were presented.However, because physical examination of parents wasnot reported, subtle findings in them cannot be ex-cluded. In the report by Koiffmann et al. [1988], 3brothers with unaffected first-cousin parents from Bra-zil were presented. Although this report strongly sug-gests autosomal recessive inheritance because of con-sanguineous parents, the general consanguinity rate inBrazil should be considered. The last report by Klingerand Merlob [1998] included 2 affected sibs with unaf-fected nonconsanguineous parents. Autosomal domi-
*Correspondence to: Mustafa Tekin, M.D., Department of Hu-man Genetics, 1101 East Marshall Street, P.O. Box 980033, Rich-mond, VA 23298. E-mail: [email protected]
Received 8 December 1998; Accepted 4 February 1999
Fig. 1. Cutis marmorata and terminal transverse limb defect in theproposita.
American Journal of Medical Genetics 86:90–91 (1999)
© 1999 Wiley-Liss, Inc.

nant inheritance with incomplete penetrance in theparents or gametic mosaicism is possible in the fami-lies that suggest autosomal recessive inheritance. Al-though our observation strongly suggests autosomalrecessive inheritance with consanguineous parents,the high rate of consanguineous marriages in Turkeyshould also be considered. Congenital skin defects ofthe body with limb defects are an extremely heterog-enous group among which there may be inherited dis-
orders of all Mendelian types as well as sporadic andnongenetic causes [Sybert, 1989]. Our report, togetherwith previous reports of possible recessively inheritedfamilies, suggests that similar heterogeneity might oc-cur in cases with congenital scalp defects with limbdefects. We need to better understand the basic mecha-nisms underlying this potential heterogeneity to pro-vide the most-accurate genetic counseling.
REFERENCES
Bamforth JS, Kaurah P, Byrne J, Ferreira P. 1994. Adams-Oliver syn-drome: A family with extreme variability in clinical expression. Am JMed Genet 49:393–396.
Kahn EA, Olmedo L. 1950. Congenital defect of scalp with a note on theclosure of scalp defects in general. Plast Reconstr Surg 6:435–440.
Klinger G, Merlob P. 1998. Adams-Oliver syndrome: autosomal recessiveinheritance and new phenotypic–anthropometric findings. Am J MedGenet 79:197–199.
Koiffman CP, Wajntal A, Huyke BJ, Castro RM. 1988. Congenital scalpdefects with distal limb anomalies (Adams-Oliver syndrome McKusick10030): further suggestion of autosomal recessive inheritance. Am JMed Genet 29:263–268.
Scribanu N, Temtamy SA. 1975. The syndrome of aplasia cutis congenitawith terminal, transverse defects of limbs. J Pediatr 87:79–82.
Sybert VP. 1985. Aplasia cutis congenita: A report of 12 new families andreview of the literature. Pediatr Dermatol 3:1–14.
Sybert VP. 1989. Congenital scalp defects with distal limb anomalies (Ad-ams-Oliver syndrome-McKusick 10030): Further suggestion of autoso-mal recessive inheritance. Am J Med Genet 32:266–267.
Whitley CB, Gorlin RJ. 1991. Adams-Oliver syndrome revisited. Am JMed Genet 40:319–326.
Mustafa Tekin*Joann BodurthaDepartment of Human GeneticsVirginia Commonwealth UniversityRichmond, Virginia
Ergin C* iftc* iSaadet ArsanDepartment of PediatricsAnkara University School of MedicineAnkara, Turkey
Fig. 2. The large scalp defect in the proposita.
Letter to the Editor 91
Recommended