Ichthyosis prematurity syndrome: A well-definedcongenital ichthyosis subtype
Anette Bygum, MD,a Per Westermark, MD,b and Flemming Brandrup, MDa
Odense, Denmark, and Uppsala, Sweden
Ichthyosis prematurity syndrome is a rare syndrome characterized by the clinical triad of premature birth,thick caseous desquamating epidermis, and neonatal asphyxia. We describe two siblings with ichthyosisprematurity syndrome. The index patient was born at gestational week 34. Immediately after birth hedeveloped respiratory distress and needed intubation. Remarkable skin changes were noticed withuniversal red, edematous and desquamating, spongy skin giving an impression of excessive vernix caseosa.Marked regression of the edema and ichthyotic scaling was observed within a few weeks. The parentsrecalled that his elder sister had similar but milder skin changes and respiratory distress syndrome at birth.Ichthyosis prematurity syndrome was suggested and the diagnosis supported by electron microscopy of askin biopsy specimen showing pathognomonic trilamellar membrane aggregations in the stratum corneumand stratum granulosum. Diagnosing this syndrome is important to reassure parents, obstetricians, andpediatricians about its benign course after complications in the perinatal period. ( J Am Acad Dermatol2008;59:S71-4.)
Ichthyosis prematurity syndrome (IPS) is a rarelyrecognized syndrome belonging to the hetero-geneous group of recessive inherited disorders
of cornification. We describe the clinical characteris-tics of two Danish siblings with IPS where the diag-nosis was confirmed ultrastructurally by electronmicroscopy of a skin biopsy specimen. To our knowl-edge, these are the first two patients given the diag-nosis of IPS in Denmark.
CASE REPORTSCase 1
The proband was a boy born at gestational week34 with a birth weight of 2970 g, after an uneventfulpregnancy and delivery. The parents were unrelated.Immediately after birth he developed respiratorydistress and was intubated for a short time and latertreated by continuous positive airway pressure in aneonatal care department for 1 week. Radiographyshowed bilateral pulmonary infiltrations, possibly asign of aspiration pneumonia. He had a normal cordblood IgE less than 0.1 kU/L (\0.3) but a peripheralblood smear with eosinophilia of 9% (\5%) in hisnewborn period.
From the Department of Dermatology, Odense University Hospital,a
and Department of Genetics and Pathology, Uppsala University.b
Funding sources: None.
Conflicts of interest: None declared.
Reprint requests: Anette Bygum, MD, Department of Dermatology,
Odense University Hospital, 5000 Odense C, Denmark. E-mail:
0190-9622/$34.00
ª 2008 by the American Academy of Dermatology, Inc.
doi:10.1016/j.jaad.2008.06.014
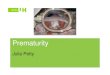
Remarkable skin changes were noticed at birthin the form of an almost universal red, edematousand desquamating, spongy skin. The hyperkeratosiscovering the scalp, face, and upper extremities gavean impression of excessive vernix caseosa (Fig 1).The edema resolved gradually in 1 to 2 weeks but awidespread ichthyotic scaling persisted. The rednessfaded within the next months but the skin stayed drywith minimal superficial scaling. From the age of 6months he developed asthma and signs of atopicdermatitis with fine follicular keratoses on his trunkand proximal upper extremities. Normal develop-mental milestones were recorded and the boy wasotherwise healthy.
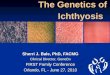
A skin biopsy specimen at the age of 2 monthsexamined by electron microscopy showed trilamel-lar lamellae in swollen corneocytes in stratum cor-neum and stratum granulosum characteristic ofichthyosis congenita type IV (Fig 2).
Case 2The parents could tell that his 4-year-old sister
presented strange reptilelike skin changes at birth,especially at the distal extremities (Fig 3, A) andtransient respiratory distress syndrome treated in apediatric care department, which was elucidatedretrospectively through a survey of the case notes.She was a twin born at gestational week 33 with abirth weight of 1587 g (the dizygotic twin had a birthweight of 2199 g). At birth her skin was described asdry and ichthyotic. It was noticed that the amnioticfluid was greenish discolored in an unusual way.Because of respiratory insufficiency she was intu-bated and treated on a respirator for 2 days and after
S71

J AM ACAD DERMATOL
NOVEMBER 2008
S72 Bygum, Westermark, and Brandrup
that treated with continuous positive airway pres-sure for a further 10 days. Aspiration pneumonia wassuggested because of a radiograph showing severebilateral pulmonary infiltrates (Fig 4). As a newbornshe had blood eosinophilia of 13% in differentialcount (\5%). This value has not been checked sinceand we have no information about IgE. Her skin hasbeen persistently dry with a tendency to prurigo andperiodic flexural dermatitis that suggests atopic der-matitis. When evaluated at the age of 4 years, dry skinwith a texture like sandpaper caused by follicularkeratoses was found on her trunk and proximalextremities. The skin on her hands was dry andlichenified (Fig 3, B). She has had lifelong eye prob-lems with slight photophobia, epiphora, and frequentpurulent conjunctivitis.
Both children have fair skin and light hair withfine white scaling on the scalp. Light and polarizationmicroscopy results of hair shafts have been normal inboth children. They both have a tendency for accu-mulation of cerumen and detritus in the externalauditory canals requiring frequent visits to anotologist.
In addition to the proband and his sister there areseveral family members with atopy and dry skin.Both parents have dry skin and the father had asthmain childhood. The other dizygotic twin is completelyhealthy.
Fig 1. Case 1. A, Red, edematous, and caseous skin on theface at birth. B, Edematous, desquamating, spongy skin onthe scalp and upper arm at birth.
DISCUSSIONIPSwas suspected in theboybecauseof the clinical
triad: premature birth, thick caseous desquamatingepidermis, and neonatal asphyxia. The diagnosis wasconfirmed by ultrastructural analysis of a skin biopsyspecimen. Furthermore, linkage to a locus on chro-mosome9q34was established in the affected childrenin a study of Scandinavian cases of IPS with identicallinkage.1 Haplotype analysis confirmed a strongfounder effect for the disorder.1 However, it has notbeen possible to trace the ancestry of this family backto the other Scandinavian kindred although we haveinformation on the family 6 generations back.
IPS belongs to the heterogeneous group of auto-somal recessive congenital ichthyoses. However, theliterature with regard to the clinical findings in IPS isvery sparse. The first descriptions were published asichthyosis congenita type IV identifying IPS as aseparate entity by its characteristic ultrastructuralfeatures.2,3 In fact, the ultrastructural findings seemto be pathognomonic with conspicuous membraneinclusions in the stratum corneum, although thesubcellular origin for these membrane structureshas not been determined. In 1993, Niemi et al4
published the clinical features in two Finnish childrenwith recessive ichthyosis congenita type IV, one ofthese died at age 2 days old in respiratory distress.The descriptive name of the syndrome was given byGedde-Dahl5 in 1996 according to Klar et al.6 Thefrequency of IPS is probably underestimated becauseof insufficient knowledge of this specific disease. In arecent French article, the condition was descriptivelyreported as ‘‘self-healing congenital verruciform hy-perkeratosis’’ and published as a new phenotype.7
The initial finding of a thick caseous desquamatingepidermis in IPS seem to be rather specific in the
Fig 2. Electron microscopy: note curved multilamellarmembranous structure in corneocyte.

J AM ACAD DERMATOL
VOLUME 59, NUMBER 5
Bygum, Westermark, and Brandrup S73
spectrum of autosomal recessive congenital ichthyo-ses. However, vernix caseosa-like covering has beenfound occasionally in KID syndrome. The finding isdistinct from the collodion membrane in, for in-stance, lamellar ichthyosis and the massive constric-tive scales in harlequin ichthyosis. The specificity ofthe IPS phenotype is supported by linkage analysis incases with identical phenotype.1
In IPS, the pregnancy is complicated by polyhy-dramnion and an opaque amnion fluid because ofthe shedding of large amounts of epidermal cells(described as starry-sky appearance by ultrasound7).Ultrasound descriptions from the pregnancies werenot available in our cases. The birth is always prema-ture and delivery typically takes place at gestationalweeks 30 to 34. Asphyxia is characteristically foundafter delivery probably because of aspiration of am-niotic debris. The skin is covered by a thick, caseous,desquamating epidermis at birth. Soon after thecritical neonatal period the child’s health improvesrapidly, changing to dryness of the skin, follicularhyperkeratosis, and fine white scaling at the scalp thatpersists into adulthood. The clinical features weredescribed by Brusasco et al,8 who noted hypereosin-ophilia and a strongly positive Darier sign as well. Infact, both our children showed positive urticarialdermographism and slight blood eosinophilia in asingle blood test. Flexural dermatitis and an associa-tion with atopic dermatitis has been found. In thearticles by Niemi et al4 and Brusasco et al,8 the verycharacteristic persistent follicular goose-skin-like
Fig 3. Neonatal cobblestone ichthyosis (A) and currentskin status (B) of patient 2.
accentuation of the follicles is illustrated. Thesefollicular hyperkeratoses seem to be more wide-spread and monomorphous than ordinary keratosispilaris.
IPS is very rare, except in a region of Norway andSweden with an estimated heterozygote carrier fre-quency of 1 in 50.6 In 2004, a Scandinavian groupperformed a genomewide linkage analysis in 16families with IPS from Norway and Sweden. The IPSlocus was mapped to chromosome 9q34.6 A refinedmappingof this regionwaspublished in2006. Linkagewas confirmed to chromosome 9q and the IPS haplo-type refined to a 76-kilobase core region (9q33.3-34.13).1 The gene and gene-product is unknown, butmay be related to a disturbed lipid metabolism in theskin. It is tempting to speculate that the atopic man-ifestations develop secondary to an impaired skinbarrier similar to the association between atopic der-matitis and ichthyosis vulgaris based on filaggrinmutations. However, this cannot be the entire story,as in some of the severe variants such as lamellarichthyosis, atopy is not an associated feature. Thebackground of preterm birth is still an enigma.
IPS has obstetric, pediatric, and dermatologicimplications. The syndrome is potentially fatal, asunrecognized cases might have a high risk of deathfrom asphyxia.
Diagnosing this syndrome is also important toreassure parents and pediatricians about the benigncourse of the disease after complications in theperinatal period and to offer genetic counseling.
We thank radiologist Bo Elle for his description andradiographic image of aspiration pneumonia.
Fig 4. Bilateral pulmonary infiltrates on radiograph inpatient 2 at birth.

J AM ACAD DERMATOL
NOVEMBER 2008
S74 Bygum, Westermark, and Brandrup
REFERENCES
1. Melin M, Klar J, Gedde-Dahl T Jr, Fredriksson R, Hausser I,
Brandrup F, et al. A founder mutation for ichthyosis prematurity
syndrome restricted to 76 kb by haplotype association. J Hum
Genet 2006;51:864-71.
2. Anton-Lamprecht I. Pranatale Diagnostik von Genodermatosen.
Hautarzt 1988;39(Suppl):16-8.
3. Anton-Lamprecht I. The skin. In: Papadimitriou JM, Henderson
DW, Spagnolo DV, editors. Diagnostic ultrastructure of non-
neoplastic diseases. Edinburgh: Churchill and Livingstone; 1992.
pp. 459-550.
4. Niemi KM, Kuokkanen K, Kanerva L, Ignatius J. Recessive
ichthyosis congenita type IV. Am J Dermatopathol 1993;15:
224-8.
5. Gedde-Dahl T Jr. The ichthyosis-prematurity syndrome (IPS).
Abstract presented at: Syndromdiagnostikk, Departments of
Medical Genetics and Pediatrics, Ulleval Hospital, Oslo, Norway;
August 28, 1996.
6. Klar J, Gedde-Dahl T Jr, Larsson M, Pigg M, Carlsson B, Tentler D,
et al. Assignment of the locus for ichthyosis prematurity
syndrome to chromosome 9q33.3-34.13. J Med Genet 2004;
41:208-12.
7. Leaute-Labreze C, Boralevi F, Cony M, Maleville J, Lacombe D,
Surleve-Bazeille JE, et al. Self-healing congenital verruciform
hyperkeratosis. Am J Med Genet 2004;130A:303-6.
8. Brusasco A, Gelmetti C, Tadini G, Caputo R. Ichthyosis congenita
type IV: a new case resembling diffuse cutaneous mastocytosis.
Br J Dermatol 1997;136:377-9.
Recommended