Intravascular Ultrasound Helps Differentiate
Coronary Mural Hematoma from Dissection
Wen-Hsiung Lin, Jui-Peng Tsai, Kuang-Te Wang, Yung-Chih Chen and Hsiao-yang Cheng
Intravascular ultrasound (IVUS) is a safe, accurate, and reproducible method of detecting vessel wall structure and
disease. In this case, we describe a 75-year-old female with hypertension and effort angina. Coronary arteriography
revealed critical stenosis in the distal right coronary artery (RCA), and intravascular ultrasound (IVUS)
demonstrated spontaneous dissection flap. A significant dissection-like lesion developed at the distal part of the
lesion after ballooning and stenting. Another stent was used to cover the edge dissection. The dissection-like lesion
extended proximally and distally and was complicated with inferior wall myocardial infarction. IVUS revealed
coronary mural hematoma which compromised the vessel lumen. We used stents to maintain adequate coronary
lumen and flow. One week later, follow-up angiography demonstrated patent RCA. The patient was discharged and
has had no symptom until now. Using angiography, it is difficult to differentiate coronary mural hematoma from
dissection. IVUS can provide valuable information in this situation.
Key Words: Intravascular ultrasound � Coronary mural hematoma
INTRODUCTION
Contrast coronary arteriography is limited in its abil-
ity to quantify the extent or distribution of atherosclero-
sis or to identify changes within the vessel wall over
time. Intravascular ultrasound (IVUS) lends insight into
dynamic changes before and after percutaneous coronary
intervention (PCI). IVUS is an imaging modality that
can bring a tomographic perspective to PCI and is capa-
ble of showing the arterial wall and the lumen of the cor-
onary arteries with high spatial resolution across the full
360-degree circumference of the vessel. Thus, it pro-
vides additional information beyond what is obtained
from angiography. The use of IVUS in cardiac catheteri-
zation laboratory has continued to evolve since its intro-
duction almost 15 years ago.1
IVUS may be used for several purposes during PCI:
(1) to assess plaque morphology and composition, quan-
tify vessel and plaque size and select the best devices for
PCI;2 (2) to confirm angiographic estimates of stenosis
severity; (3) to assess anatomical results and detect com-
plications, including dissections and residual minimal
cross-sectional area, after PCI;3 and (4) to assess stent
deployment and in-stent restenosis. In addition, IVUS
also can help differentiate between true and false coro-
nary aneurysm and between coronary dissection and mu-
ral hematoma like this case.
CASE REPORT
A 75-year-old female with a history of regularly
controlled hypertension and chronic obstructive pulmo-
nary disease for 20 years was admitted with effort an-
gina. Echocardiography had not shown obvious regional
wall motion abnormality, and patient could not tolerate
39 Acta Cardiol Sin 2009;25:39�42
Case Report Acta Cardiol Sin 2009;25:39�42
Received: December 5, 2007 Accepted: April 11, 2008
Division of Cardiology, Department of Internal Medicine, Mackay
Memorial Hospital, Taitung, Taiwan.
Address correspondence and reprint requests to: Dr. Jui-Peng Tsai,
Division of Cardiology, Department of Internal Medicine, Mackay
Memorial Hospital, 1, Lane 303, Changsha Street, Taitung, Taiwan.
Tel: 886-89-310150 ext. 543; E-mail: [email protected]
stress test due to degenerative disease of legs and mark-
ed exertional dyspnea. Coronary arteriography revealed
significant type B1 lesion on the distal right coronary ar-
tery (RCA) (Figure 1A) and insignificant lesion at the
left coronary artery.
The RCA was engaged with a 6 Fr JR5 guiding cath-
eter, and a floppy guidewire (Runthrough NS�) was in-
serted into the posterior lateral branch (PLV) of the
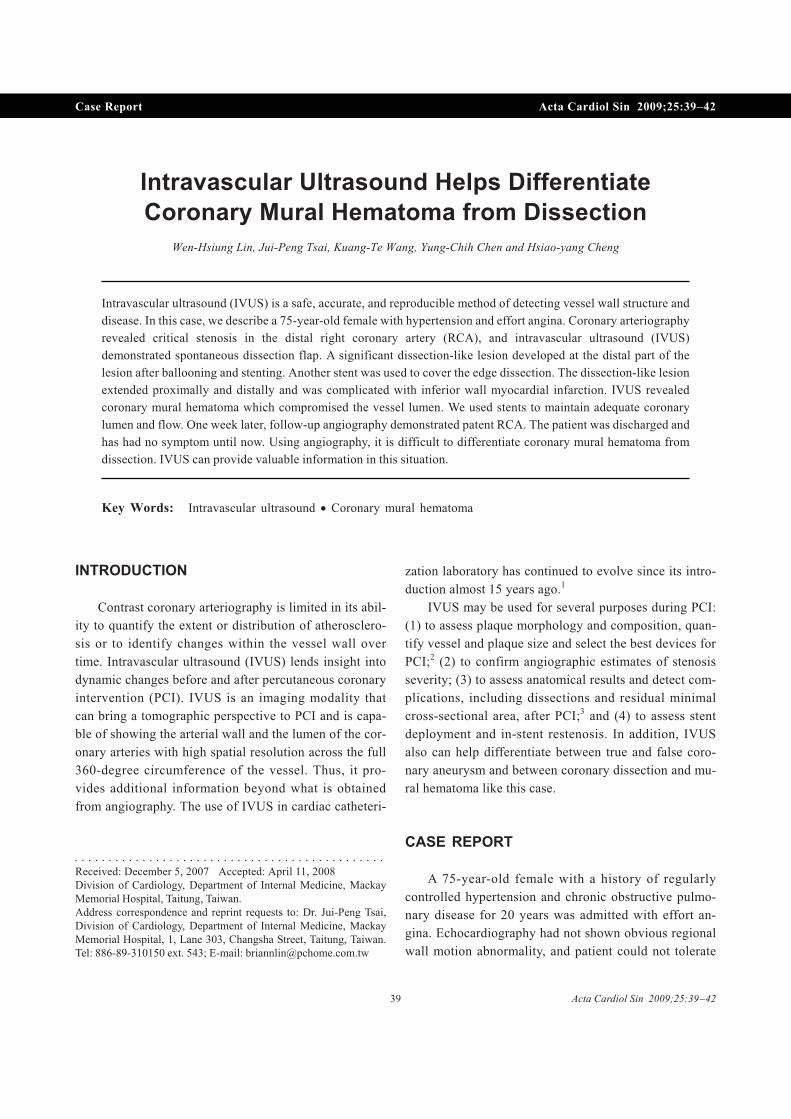
RCA. IVUS imaging of the lesion showed a cross-sec-
tional diameter of about 4.5~5.0 mm, and eccentric large
atheroma with 78� stenosis, and spontaneous plaque
dissection (Figure 1B) was noticed. The culprit lesion
was dilated with a Fortis� (non-compliance balloon 4.0
� 13 mm) at 14 atm. After balloon angioplasty, there was
46� residual stenosis, and a Driver� stent (4.0 � 15 mm
Medtronic�) was deployed at 14 atm in the distal RCA.
Post- dilatation was done with a Fortis� (non-compli-
ance balloon 4.0 � 13 mm) at 18 atm. Angiography re-
vealed a significant dissection-like lesion in the distal
stent area (Figure 1C), so we put another Driver� stent
(4.0 � 12 mm Medtronic�) at 9 atm and post-dilated with
a Fortis� (non-compliance balloon 4.0 � 13 mm) at 20
atm. Unfortunately, a new proximal lesion happened and
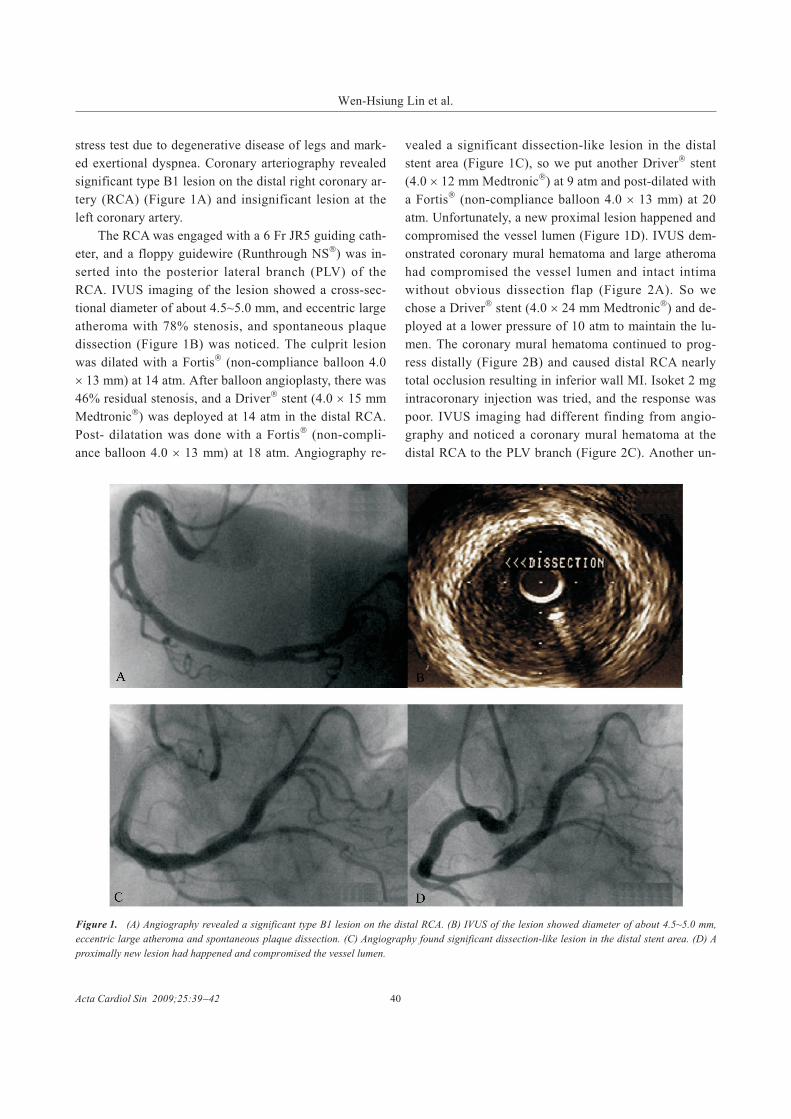
compromised the vessel lumen (Figure 1D). IVUS dem-
onstrated coronary mural hematoma and large atheroma
had compromised the vessel lumen and intact intima
without obvious dissection flap (Figure 2A). So we
chose a Driver� stent (4.0 � 24 mm Medtronic�) and de-
ployed at a lower pressure of 10 atm to maintain the lu-
men. The coronary mural hematoma continued to prog-
ress distally (Figure 2B) and caused distal RCA nearly
total occlusion resulting in inferior wall MI. Isoket 2 mg
intracoronary injection was tried, and the response was
poor. IVUS imaging had different finding from angio-
graphy and noticed a coronary mural hematoma at the
distal RCA to the PLV branch (Figure 2C). Another un-
Acta Cardiol Sin 2009;25:39�42 40
Wen-Hsiung Lin et al.
Figure 1. (A) Angiography revealed a significant type B1 lesion on the distal RCA. (B) IVUS of the lesion showed diameter of about 4.5~5.0 mm,
eccentric large atheroma and spontaneous plaque dissection. (C) Angiography found significant dissection-like lesion in the distal stent area. (D) A
proximally new lesion had happened and compromised the vessel lumen.
dersize Driver� stent (3.0 � 30 mm Medtronic�) was de-
ployed at lower pressure of 9 atm in the RCA (D- >
PLV) to keep the lumen patent (Figure 2D). After the
procedure, the patient’s symptoms improved and electro-
cardiogram revealed resolution of ST segments. The pa-
tient’s peak cardiac enzymes were CK: 354 U/L, CK-
MB: 37.7 U/L and troponin I: 11.2 ng/ml. One week
later, follow-up angiography and IVUS demonstrated
patent RCA with mild absorption and organization of
coronary mural hematoma. This patient was then dis-
charged, and has had no symptoms until now.
DISSCUSSION
Intermediate lesion presents a challenging task in
decision-making for revascularization and can be partic-
ularly troublesome in patients whose symptomatic status
is difficult to evaluate. This patient had typical effort an-
gina, but her echocardiography revealed normal wall
motion. In this situation, stress test was a good option.
Because she suffered from degenerative disease of the
legs and marked exertional dyspnea, the patient could
not tolerate treadmill test, and myocardial perfusion scan
is not available in Taitung. In addition to coronary
angiography, IVUS can assist decision-making, and in
combination with fractional flow reserve (FFR) is better
to detect significant stenosis than IVUS image alone.
Measurements of FFR and coronary flow reserve using
miniaturized sensors have proved useful in identifying
lesions of hemodynamic significance.4,5 We did not have
FFR, but the patient’s IVUS image had significant steno-
sis and vulnerable plaque, so angioplasty was indicated.
We treated her culprit lesion with balloon angio-
41 Acta Cardiol Sin 2009;25:39�42
Coronary Mural Hematoma or Dissection
Figure 2. (A) IVUS demonstrated mural hematoma and large atheroma had compromised vessel lumen. (B) Mural hematoma had progressed and
compressed distal lumen. (C) IVUS noticed mural hematoma at the distal RCA to PLV branch. (D) Angiography showed patent RCA and normal
coronary flow.

plasty and stenting. Coronary angiography extremely
mimiked coronary residual dissection after the first
stenting. IVUS did not found dissective intima, but we
still treated the new finding of angiography as edge dis-
section, covering it with another stent and post-dilatated
with high pressure for full expansion of stent. Unfortu-
nately, a new proximal lesion happened and compro-
mised the vessel lumen.
Coronary dissection is the most common reason for
acute arterial closure during PCI and can result in seri-
ous complications including death, myocardial infarc-
tion, and emergent bypass surgery. In addition, residual
dissection after stenting remains a risk factor for sub-
acute stent thrombosis in the DES era.6 For detection of
dissections, IVUS is a more sensitive imaging modality
than angiography. The circumferential and the longitudi-
nal extent of coronary dissections can be better appreci-
ated by IVUS. Whenever there is an indication for
stenting, IVUS imaging usually reveals involvement of a
longer arterial segment than can be appreciated angio-
graphically. This additional involvement may be particu-
larly important in cases of bailout stenting for threatened
acute closure, in which it is critical to cover the entirety
of the dissected segment.
In present case, if we still believed empirical dissec-
tion on angiography and had not been alert to check
IVUS after stenting, the mural hematoma would have
progressed to compromise coronary flow and the worst
result would have been acute closure of coronary flow
threatening the patient’s life. Management between coro-
nary dissection and mural hematoma is very different.
The treatment of dissection is used appropriate-size stent
and apposition to cover dissection, but the goal of mural
hematoma is use of stent to keep patent lumen and main-
tain adequate coronary flow.
The other problem is that plaque burden had not
been accurately evaluated when we chose the stent size.
After high pressure balloon dilatation, the massive
plaque burden had migrated to the proximal part and in-
duced mural hematoma due to barotrauma. Mural hema-
toma in this case results from large amount of atheroma
and treatment with high-pressure dilatation. Cross-sec-
tional area stenosis of IVUS is distinct from diameter
stenosis obtained by angiography because it does not use
reference segments, unlike angiography.7,8 IVUS can
more accurately evaluate plaque burden than angio-
graphy.
In conclusion, if there is massive atheroma detected
by IVUS, the stent should be mildly undersized and ap-
propriate pressure should be used to prevent plaque
shifting and mural hematoma. In addition, if angio-
graphy reveals atypical dissection-like lesion, IVUS
should be done to exclude mural hematoma. If mural
hematoma has happened and coronary flow is normal,
observation may be a good option. If a lesion is not well
assessed before PCI, the result of angioplasty can be
worse than with conservative treatment by medication.
REFERENCES
1. St. Goar FG, Pinto FJ, Alderman EL, et al. Intravascular ultra-
sound imaging of angiographically normal coronary arteries: an
in vivo comparison with quantitative angiography. J Am Coll
Cardiol 1991;18:952-8.
2. Fitzgerald PJ, St. Goar FG, Connolly AJ, et al. Intravascular ultra-
sound imaging of coronary arteries. Is three layers the norm? Cir-
culation 1992;86:154-8.
3. Dangas G, Ambrose J, Rehmann D, et al. Balloon optimization
versus stent study (BOSS): provisional stenting and early recoil
after balloon angioplasty. Am J Cardiol 2000;85:957.
4. Pijls NH, De Bruyne B, Peels K, et al. Measurement of fractional
flow reserve to assess the functional severity of coronary-artery
stenoses. N Engl J Med 1996;334:1703-8.
5. Miller DD, Donohue TJ, Younis LT, et al. Correlation of pharma-
cological 99mTc-sestamibi myocardial perfusion imaging with
poststenotic coronary flow reserve in patients with angiographi-
cally intermediate coronary artery stenoses. Circulation 1994;
89:2150-60.
6. Regar E, Lemos PA, Saia F, et al. Incidence of thrombotic stent
occlusion during the first three months after sirolimus-eluting
stent implantation in 500 consecutive patients. Am J Cardiol
2004;93:1271-5.
7. Mintz GS, Nissen SE, Anderson WD, et al. American College of
Cardiology Clinical Expert Consensus Document on Standards
for Acquisition, Measurement and Reporting of Intravascular Ul-
trasound Studies (IVUS). A report of the American College of
Cardiology Task Force on Clinical Expert Consensus Documents.
J Am Coll Cardiol 2001;37:1478-92.
8. Robbins RC, McManus RP, Mitchell RS, Latter DR, Moon MR,
Olinger GN, et al. Management of patients with intramural he-
matoma of the thoracic aorta. Circulation 1993;88(5 Pt 2):II1-10.
9. Hsin HT, Chiu YW, Liau CS, et al. “Inter-lacing” of Stents:
13-Month Follow-up by Intravascular Ultrasound after Primary
Simultaneous Kissing Stenting. Acta Cardiol Sin 2007;23:
277-81.
Acta Cardiol Sin 2009;25:39�42 42
Wen-Hsiung Lin et al.
Recommended
















