Parasitology Today, vol. 4, no. I O, 1988 279
Loa I o a - a Neglected Filaria M, Pinder
There has been considerable research on the biochemistry and immunology of many human, veterinary and laboratory animal filariae, with a view to understanding pathogenic and protective immune mechanisms and developing ways to boost them 1-3. But, apart from a few isolated reports (eg. Refs .4, 5), these aspects have been largely ignored for the human filarial parasite Loa loa. Obviously not all filariae can be studied in equal depth - almost 100 different life cycle patterns are documented 6 - but, as Margaret Pinder shows here, L. loa/s an important human pathogen of considerable biological interest.
One reason for the paucity of studies on L. loa is that apart from the ocular mani- festations, reports of which abound in the literature, the disease it induces is not considered dramatic (see Box 1). As in other filarial infections, the disease shows a wide spectrum of symptoms and although many subjects are asympto- matic, some may show debilitating clinical signs. Endemic areas can show high inci- dence of disease (see Box 2), and in some regions this is the second most common reason for medical consrdtation (after mal- aria) (A. Sail6, pers. corrLmun.). Currently available drugs are far from ideal and vector control is considered impractical ll. The subject seems ripe for studies on immune mechanisms of parasite control.
Controlled microfilaraemia It has been estimated that in hyper-
endemic zones inhabitants may receive one infective fly bite every five days 1°. In one hyperendemic zone, 95% of inhab- itants had antibodies reacting with L. loa antigens by the age of two years 4. In con- trast, the prevalence of microfilaraemic individuals in an exposed population rarely exceeds 35%, which has led many investigators to propo:se that acquired immunity may eliminate circulating microfilariae (mf) in certain individ- uals l°'21. There are a few published case histories that describe amicrofilaraemic individuals with subconjunctival migra- tion of adult worms. These individuals are described as having 'occult' infections 22.
It has been claimed that the frequency of occult loiasis exceeds that of the micro- filaraemic form l°, and in Gabon we recently obtained evidence supporting this claim 2z. Gabonese adults reporting at hospitals in the Haut-Ogoou6 with an ocular involvement and who had not taken diethylcarbamazine (DEC) within the past year were examined clinically and microfilaraemia was estimated (no. mf per 1 ml blood). Only 15 of 47 (33%) had L.
loa microfilaraemia and the remainder had occult infections (ie. amicrofilaraemic). This suggests that in the endemic area only one of three subjects infected with L. Ioa shows microfilaraemia.
Immune mechanisms The mechanism by which these sub-
jects control their microfilaraemia may be immunological and, since the intensity of microfilaraemia is a crucial determinant in disease transmission (see Box 3), it is of practical importance to investigate this further. One of the best-studied host defense mechanisms against parasitic worms is that responsible for the control and suppression of microfilaraemia during filarial infection. In many cases antibody- mediated mechanisms have been impli- cated 1,26-2s.
Sera from 15 subjects with parasitologi- cally verified occult loiasis were compared with sera from ten subjects with high levels of circulating L./oa microfilariae for their ability to react with living homol- ogous microfilariae in an immunofluor- escence antibody test (IFAT) 29. Sera from highly microfilaraemic subjects did not react or reacted very weakly, whereas most sera from people with occult loiasis reacted strongly - most of the serum anti- bodies were of the IgG class. These sera were also tested against living microfil- ariae in an antibody-dependent cell- mediated cytotoxicity test using normal leucocytes. Approximately 50% of sera active in IFAT were also active in the cytotoxicity test, and all sera that did not react in IFAT were inactive in cytotox- icity. As has been described for other filariae 27'2s there was strong cellular ad- hesion along the length of the microfil- ariae, which eventually became completely surrounded, immobile and unrecognizable.
This reaction was obtained using sera from individuals able to control their microfilaraemia in vivo. This correlation
~) 1988, Elsevier Publications, Cambridge 0169'47581881502.00
Centre International de Recherches Medicales
BP 769 Franceville Gabon
In areas endemic for loiasis, 23-70% of inhabitants show symptoms indicative of the disease (F. Noireau and A. Dupont, pets. commun.) and symptomatic infections are common in temporary residents. However, life- threatening complications are rare.

280 Parasitology Today, vol. 4, no. I O, 1988
of in vitro with in vivo results suggests that an antibody-dependent mechanism could be important in natural infections, although this does not preclude the pos- sible involvement of other mechanisms. In particular, IgE has not been examined, and previous workers have reported that rat IgE anti-Acanthocheilonema (= Dipet- alonema ) viteae can kill L. loa microfilariae in the presence of platelets 3°.
Individuals with parasitologically ver- ified occult loiasis did not differ from microfilaraemic subjects either in severity
of symptoms or in eosinophil c o u n t 24. The occult state is thus not necessarily associ- ated with increased pathology and fur- thermore, some subjects with high levels of microfilariae-specific IgG antibodies were asymptomatic. This contrasts strongly with Wuchereria bancrofti and Brugia malayi infections where occult filariasis is frequently symptomatic with enlargement of the lymph nodes and respiratory com- plaints - such patients show high levels of antibody against microfilariae and marked eosinophilia 31 .
iiiii~ili~i
ii!~!!!il
! iiiii!iii!! iiiiiii~ii
!!i~!iill
ii!i!:~!i!i
i~iii~iiii iiii!:i~il
E
~ ~ p t o m and few ~5 of 25:~ ~u!t~ wi~ ocular

Parasitology Today, val. 4, no. 10, 1988 281
In lymphatic filarial[ infections how- ever, asymptomatic occult infections often remain undetected and such sub- jects may be classified as 'resistant'. This emphasizes the need for serological tests to detect these individuals. Tests for cir- culating parasite antigen have been developed for certain human and animal filarial infections but detection is often hindered by the masking of antigen by antibody in immune complexes 3z,33.
Occult loiasis is not always asympto- matic and a hyper-responsive syndrome has recently been described in temporary residents of the endemic zone 7. The syn- drome is characterized by frequent and severe 'Calabar swellings' (see Fig. 1) with pruritis, pronounced eosinophifia and high antibody titres to unspecified heter- ologous filarial antigens. Microfilariae could be detected in only 7 of 20 subjects.
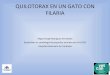
In other filarial infections there have been many studies to identify surface molecules using iodination followed by gel electrophoresis 2. Fewer studies have attempted to identify surface antigens recognized by sera from subjects that have cleared microfilaraemia, even in animal model systems. Some authors have re- ported a lack of correlation between recognition of surface ~mtigens and clini- cal s t a t u s 34 but our recent studies on loia- sis gave remarkably clear-cut results 29 (Fig. 5). We iodinated live microfilariae using iodogen as the catalyst and sub- sequently immunoprecipitated the extracted antigens using individual patients' sera. Several, but not all, occult loiasis sera that were )highly reactive in
IFAT and in cytotoxicity tests, precipi- tated a 23 kDa molecule that was not precipitated by sera from highly micro- filaraemic subjects (Fig. 1). This 23 kDa molecule was also recognized by sera from a mandrill, Papio (Mandrillus) sphinx, experimentally infected with L. loa. Molecules of 33 kDa, 48 kDa and 75-84 kDa were also immunoprecipitated by sera from loiasic patients but the recog- nition of these molecules did not correlate with the clinical picture. As with other microfdariae 2, human albumin was the predominantly labelled surface molecule.
The 23 kDa molecule is a protein with- out N-linked glycans or interchain disul- phide linkages 3s. It is thought to be located on the outer microfilarial sheath. This sheath is not a cellular plasma mem- brane and little is known of its structure, although under the electron microscope the surface appears rough with granular deposits 36.
It seems possible that in loiasis this 23 kDa protein may be the target antigen of host-protective antibody-dependent responses. Antigens of similar molecular mass may be important in immunity to lymphatic filariae: pooled sera from W. bancrofti patients immunoprecipitate a 22 kDa surface molecule from B. malayi 37, and a somatic antigen of 25 kDa elicits protective IgG responses in jirds (Meriones unguiculatus) 38. This also correlates well with the observation that in vitro antibody synthesis using lymphocytes from loiasis patients and fractionated B. malayi anti- gens can only be stimulated by a low molecular mass fraction (22-45 kDa) 39.

282 Parasitology Today, voL 4, no. I O, 1988
phatics and pulmonary circulation, and removal of the spleen leads to an increase in microfilaraemia. In primates that con- trol their microfilaraemia, the spleen becomes hypertrophied and covered with granulomata.
In the absence of longitudinal studies on infected people it is difficult to assess how appropriate is the primate model. The primate infection appears to differ in symptoms (no Calabar swellings or eye involvement have been reported) while the splenic granulomata shown by the infected primates are not characteristic of human loiasis. However, there does appear to be an inverse correlation in pri- mates between microfilaraemia and anti-L. /oa antibodies 44, as might be expected from the human studies. More- over, sera from both mandrill and man recognize a 23 kDa molecule on micro- f i l a r i a e 29 .
Animal models Attempts to infect laboratory animals
with L . / o a have been largely unsuccess- ful. However, inoculation of adult L. loa, but not the infective form (L3), into jirds did lead to microfilaraemia in four of six animals tested, and microfilariae were eliminated only after some months 4°.
Certain primates can be experimentally infected with L3 stages ofL. loa- suitable hosts include drills (Mandrillus leuco- phaeus) 41, baboons (Papio anubis), patas monkeys (Erythrocebus patas), rhesus monkeys (Macaca mulatta) 42 and man- drills 29. Cynomolgus monkeys (Macaca fascicularis) do not appear to be suitable (H. Flockhart, unpublished).
In general, similar results were obtained from all the susceptible species. Infective larvae take almost two months to become young adults and female worms start releasing microfilariae after four months. At first, microfilariae are con- fined to the lymphatics and pulmonary circulation and subsequently, at 5-6 months, they are found in the peripheral blood. During rising microfilaraemia the daily output of a single female worm aver- ages 10-22x 103 mf/day 43. Microfilarae- mia increases to high levels in many individuals, persisting for different periods (from a few weeks in drills to up to two years in rhesus monkeys), and subse- quently declines to a low level - less than 200 mf/ml. At this time, microfilarial numbers are not reduced in the lym-
Immunity Epidemiological studies on L . /oa show
a proportion of inhabitants in endemic areas with neither clinical nor parasito- logical signs of infection. This may indicate some level of resistance. In a study in the Haut-Ogoou6, Gabon, out of 162 perma- nent adult residents, 33 'resistant' indi- viduals with neither symptoms nor parasites were identified (A. Dupont , unpublished). The possible importance of such individuals in assessing immunologi- cal correlates of resistance has long been recognized, as has the need to conduct examinations at regular intervals to con- firm their resistance status 3. Again, specif- ic serological tests to confirm the absence of adult worms would be a great advantage.
The ability of sera from 16 of the resistant individuals to immunoprecipi- tate surface antigens of the homologous adult worm was compared with that of sera from the previously mentioned microfilaraemic and occult loiasis sub- jects. All resistant sera immunoprecipi- tated a 29-31 kDa antigen although some were more strongly reactive than others. The amicrofilaraemic sera also strongly immunoprecipitated this 29-31 kDa anti- gen, whereas microfilaraemic sera reacted weakly or not at alps. This antigen appears to be a glycoprotein, but its role in resistance is questionable because anti- bodies are present in individuals harbour- ing adult worms. The possible cross-reaction with L3 antigens and other stages needs further study. Again there seems to be close similarity between Bru- g/a spp and L. loa because adult Brugia

Parasitology Today, vol. 4, no. I O, 1988 283
also have a major surface antigen of 29 kDa that reacts with sera of L. loa patients 46.
One unexplored area ofL. loa immunol- ogy, and perhaps the most relevant for host resistance, is the antigenicity of the infective L3 form. In the absence of a successful in vitro culture system, L3 must be obtained from the insect vectors (Chry- sops) infected either naturally or ex- perimentally by feeding on highly microfilaraemic primates. There seems to be only one report on the immunology of L. loa L3, which demonstrates that, like other helminth larval stages, they can acti- vate the alternative coraplement pathway; this leads to eosinophils binding to the cuticle but does not seem to affect larval viability 47.
Immunomodulation and future research L. loa poses an iunnunological puzzle
that is also apparent with the other filariae - why do certain individuals produce anti- body to microfiladal surface antigen(s) whereas others do not? It is difficult even to speculate on this in the absence of studies on the natural history of infection. It has not been detemfined whether the various clinical and parasitological mani- festations seen reflect different, perhaps genetically determined, individual reac- tions, or whether these', are stages through which all patients progress.
In the primate model, animals given a single infection always seem to control the wave of microfilaraemia - this may be correlated with the appearance of IgG specific for the 23 kDa surface antigen 3]. Perhaps in individuals that are constantly reinfected, the load o:f adult worms and released microfilariae gradually increases and parasite-induced immunosuppres- sion 3~ starts to play a role. In this context, it is interesting that lymphocytes from loiasic patients synthesize antibody in response to low doses of B. malayi adult antigens but not to high doses 5. The alternative possibility of neonatal toler- ance requires investigation. Transplacen- tal passage of microfilariae is reported for some other animal and human filariae, but is unclear for L. /oa. One study reports 3 of 112 newborns with microfilaraemia 4s and another found no microfilariae in 111 umbilical cord blood samples 4. Trans- placental passage ofL. loa antigens has not been studied.
In summary, although our understand- ing of clinical and pathological aspects of loiasis has improved - ]both for permanent and temporary residents of endemic
MrxlO -a 200 . . . . . ~ ,
Y ~ +~+~;;: +i ~ .+~
6 8 . 2 - -
4 2 . 7 - - + . . . . . . . + ++o++++ ~ + ° . - + e m
31 - -
21.5--
1~4--
I 2 3 4 5 6 7 O 9 1 0 Fig. 5. Immunoprecipitates of iodogen-iodinated surface microfilarial molecules by Ioiasic sera and protein A-sepharose, analysed by 5DS-PAGE electrophoresis. Lane I, total profile; lane 2, normal European serum; lanes 3-6, sera f rom occult Ioiasic subjects; lanes 7-10, sera from microfilaraemic subjects; arrow marks the 23 kDa antigen. (~ American Association of Immunologists.
regions - the immunological processes remain unclear. Antigens of immunologi- cal importance have been identified on adult worms and microfilariae (but not yet on the infective L3 stage), and some aspects of both humoral and cellular immunity have been studied in vitro. Research is hampered by the paucity of parasite material and there is an evident need to use recombinant DNA technology to produce substantial quantities of the relevant antigens. Several groups are already using this technology with other filaria (eg. Ref. 49). The substantial cross- reactivity among filarial species suggests that this could prove a fruitful area for international collaboration.
References 1 Haque, A. and Capron, A. (1986) Parasite Antigens
(Pearson, T.W., ed.), pp 317-402, Marcel Dekkar 2 Selkirk, M.E. et al. (1986) Parasitology 91 (Suppl.),
15-38 3 Anonymous(1987)Reportofthe13thWorkingGroupon
Protective Immunity and Vaccination in Onchocerciasis and Lymphatic Filariasis WHO TDR/FIL-SWG 13/87.3
4 Goussard, B. et al. (1984) Microbiol. Immunol. 28, 787-792
5 Nurmmn, T.B., Withers, A. and Ottesen, E.A. (1985) J . Iraraunol. 135, 2794-2799
6 Schacher, J.F. (1973)Southeast Asian J. Trop. Med. Public Health 4, 336-349
7 Nutman, T.B. etal. (1986)ff. Infect. Dis. 154, 10-18 8 Eveland, L.K., Yermakov, V. and Kenney, M. (1975)
Trans. R. Soc. Trap. Med. Hyg. 69, 354-355 9 Clarke, V. de V. et al. (1971) Cent. Aft. J. Med. 17,
1-11 10 Fain, A. (1978)Bull. Organ. Mond. Santd 56, 155--167

284 Parasitology Today, vol. 4, no. I O, 1988
Acknowledgement The photographs in Boxes I and 3 were generously provided by Professor D. Richard- Lenoble, CUSS, Libreville, Gabon. CIRMF is supported bythe State of Gabon and by funds provided by Elf-Gabon.
11 Sasa, M. (1976) Human Filariasis pp 122-132, Univer- sity Park Press
12 Cesbron, J-V. etal. (1987)Nature 325,533-536 13 Richard-Lenoble, D. et al. (1985) Bull. Soc. Pathol.
Exot. 78,485-491 14 Van Hoegarden, M. et al. (1987) Ann. Trap. Med.
Parasitol. 81,275-282 15 Burchard, C.D. and Kern, P. (1987) Trans. R. Soc.
Trop. Med. Hyg. 81,420 16 Richard-Lenoble, D. et al. (1988) Congr. Soc. Ouest
Africaine Parasitol. p. 104 17 Rhodian, F. and Rodhain-Rebourg, F. (1973) Med.
Mal. Infect. 3,429-436 18 Pampiglione, S. et al. (1979) Riv. Parasitol. 40, 187-
234 19 Udonsi, J.K. (1986) Ann. Trap. Med. Parasitol. 80,
425-432 20 Richard-Lenoble, D. et al. (1980) Bull. Soc. Pathol.
Exot. 73,192-199 21 Van Hoegarden, M. et al. (1987) Trans. R. Soc. Trap.
Med. Hyg. 81,441-446 22 Dupont, A., Zue-N'dong, J. and Pinder, M. Trans. R.
Soc. Trap. Med. Hyg. (in press) 23 Maudlin, I. and Welbum, S.C. (1988) Parasitology
Today 4, 98-105 24 Duke, B.O.L. (1972)J. Linn. Soc. 51, 97-107 25 Gouteux, J.P., Noirean, F. and Staak, C. (1988)
Congr. Soc. Ouest Africaine Parasitol. p. 88 26 Kwa, B.H. and Mak, J.W. (1987) in Immune
Responses in Parasitic Infections. Immunology, I mmuno- pathology and Immunopraphylaxis Vol. I Nematodes (Soulsby, E.J.L., ed.), pp 233-249, CRC Press
27 Greene, B.M., Taylor, H.R. and Aikawa, M. (1981) J . Immunol. 127,1611-1618
28 Aiyar, S., Zaman, V. and Chan, S.H. (1982) Acta Trap. 39,225-236
29 Pinder, M., Dupont, A. and Egwang, T.G.
J. Immunol. (in press) 30 Haque, A. etal. (1985) Parasite lmmunol. 7, 517-526 31 Ottesen, E.A. (1980)SpringerSeminarslmmunopathol.
2,373-385 32 Weil, G.J. etal. (1987)J. Infect. Dis. 156,350-355 33 Ottesen, E.A. (1984) Trans. R. Soc. Trap. Med. Hyg.
78 (Suppl.), 9-18 34 Denham, D.A. and Fletcher, C. (1987) Filahasis.
Ciba Foundation Symposium (Evered, D. and Clark, S., eds), pp 225-234, Wiley
35 Egwang, T.G. et al. Mol. Biochem. Parasitol. (in press) 36 Kozek, W.J. and Orihel, T.C. (1983) Int.J. Parasitol.
13, 19-43 37 Egwang, T.G. and Kazura, J.W. (1987) Mol. Bio-
chem. Parasitol. 22,159-168 38 Kazura, J.W., Cicirello, H. and McCall, J.W. (1986)
J. Immunol. 136,1422-1426 39 Lal, R.B., Lynch, T.J. and Nutman, T.B. (1987)
J. Immunol. 139,1652-1657 40 MacKenzie, C.D., Suswillo, R.R. and Denham, D.A.
(1982) Trans. R. Soc. Trap. Med. Hyg. 76,778-782 41 Duke, B.O.L. (1960) Ann. Trap. Med. Parasitol. 54,
15-31 42 Orihel, T.C. and Eberhard, M.L. (1985) Trapenrned.
Parasitol. 36, 215-224 43 Eberhard, M.L. and Orihel, T.C. (1986) Tropenmed.
Parasitol. 37, 369-374 44 Grieve, R.B. et al. (1985) Tropenmed. Parasitol. 36,
225-229 45 Egwang, T.G. et ul. M ol. B iochem. P arasitol. (in press) 46 Maizels, R.M. et ul. (1985) Tropenmed. Parasitol. 36,
233-237 47 Yates, J.A. etal. (1985)Acta Trap. 42,157-163 48 Zanetti, V. and Lambrecht, F.L. (1948) Ann. Soc.
Belge Med. Trap. 28,355-370 49 Nilsen, T.W. et ul. (1988) Proc. Natl Acad. Sci. USA
85, 3604-3607
Parasitic Diarrhoeas in China Wang Cheng-i
Parasitic diseases associated with diarrhoea are increasingly recognized as important public health problems in China. They range from well-known intestinal infections such as giardiasis, to infections better known for other symptoms- such as mahgnant malaria and schistosomiasis. In this review, Dr Wang Cheng-i discusses recent Chinese studies on giardiasis and amoebiasis, which have been somewhat neglected in the past, and on cryptosporidiosis and infantile hookworm infection which have only recently been recognized as a health problem in China.
Giardiasis
In the suburbs of Beijing, Tianjing and Shanghai, and in rural districts of Liao- ning, Gansu and Zhejiang provinces, fae- cal examination of 3121 people revealed an overall prevalence for Giardia lamblia of 1,2% for adults (range 0,5-5.6), and 6. I% for children (range 2.3-7.8) I-3. By contrast, ELISA tests for Giardia anti- bodies 4 and faecal counter-immuno- electrophoresis for Giardia antigens 5 indicated a much higher prevalence of infection (I 2.6-13.4% in adults; 7.0-15.6% in children).
By direct faecal examination, a signifi- cant sex bias was revealed in the infec- tion rates - averaging 4.2% in 155 I males, compared with 2.8% in 1581
females. Prevalence peaked in the 5-9- year-olds (Table I ).
In adults, diardia infection is generally asymptomatic, but in children the infec- tion is frequently accompanied by clinical symptoms - often leading to severe complications, as illustrated by our re- port of a familial infection 6. In a family of five, all were infected except the father who, as a railway worker, was frequently
out of the home. The mother, a cyst carrier, was asymptomatic but consti- tuted a source of infection for her three daughters. All three showed severe clini- cal manifestations with prolonged recur- rent diarrhoea, nutritional oeclema and hepatomegaly. The youngest (4 years old) was underdeveloped both physi- cally and mentally. The eldest ( 12 years old) had recurrent diarrhoea episodes for ten years, and her chest was pigeon- shaped. Cysts and trophozoites of G. lamblia were identified in stool and duodenal drainage specimens from the daughters, whose sera also showed high titres of Giardia antibodies by ELISA (I/320-1/640) and by IHA (indirect haemagglutination antibody) ( I/I 6).
Table I. Age-related prevalence of Giardia (by faecal examination) and Entamoeba histolytica (by ELISA) in various parts of China
Age Giardia E. histolytica group No.examined % Positive No. examined % Positive
0-4 171 2.3 86 2.3 5-9 372 7.0 41 7.3
I 0-14 1006 5.8 556 12.2 15+ 1583 1.3 452 8.8
~) 1988, Elsevier Publications, Cambridge 0169-4758/88/$02.00
Recommended