
Journal of Surgical Oncology 49:253-258 (1992)
Non-lcteric Pancreas Head Carcinoma Fares Worse Than lcteric Pancreas Head Carcinoma
KOJ I YAMAGUCHI, MD, KAZUYOSHI NISHIHARA, MD, AND MASAZUMI TSUNEYOSHI, MD
From the Departments of Surgery I (K.Y.) and Pathology I / (K.N., M.T.), Kyushu University Faculty of Medicine, Fukuoka, lapan
A total of 22 patients with non-icteric pancreas head carcinoma were retrospectively compared with 6 1 patients with icteric pancreas head carci- noma. No significant difference was found regarding age, sex, greatest diameter, macroscopic type, microscopic type, stage, lymphatic perme- ation, perineural infiltration, venous invasion, lymph node metastasis, and the presence of cancer cells at the surgical margins. The main location of pancreas head carcinoma could be divided into two sites: the superior (pericholedochal), and inferior or distal (excholedochal) areas of the pan- creas head. Sixteen (73%) of the 22 non-icteric pancreas head carcinomas were located in the inferior or distal area (excholedochal), while 28 (46%) of the 61 icteric pancreas head carcinomas were situated in the superior portion (pericholedochal) ( P < 0.05). One (5%) of the 22 non-icteric pancreas head carcinomas was small pancreas carcinoma, compared with 1 1 (18%) of the 61 icteric pancreas head carcinomas. The cumulative 2-year and 4-year survival rates of the 22 patients with non-icteric pancreas head carcinoma were significantly worse than those of the 61 patients with icteric pancreas head carcinoma [7.9% vs. 24.6% ( P < 0.05) and 0% vs. 13.4% ( P < O.Ol)] . These findings suggest that non-icteric pancreas head carcinomas normally arise in an area far from the biliary tree, and include a greater number of large tumors. Any resulting difficulty and delay in the diagnosis and treatment of this disease will usually lead to a worsening of the clinical course of non-icteric pancreas head carcinoma. 0 1992 Wiley-Liss, Inc.
KEY WORDS: jaundice, prognostic factor, small pancreas carcinoma
INTRODUCTION Patients with pancreas head carcinoma usually develop
jaundice at the time of clinical diagnosis [ 11. The clinical course of patients with either pancreas body or tail carci- noma is generally worse than that of patients with pan- creas head carcinoma. This is because pancreas body or tail carcinoma rarely leads to jaundice, and widely infil- trates the retroperitoneal structures at the time of detec- tion. There have been some sporadic case reports of non- icteric pancreas head carcinoma [2,3], but there have been very few reports regarding the clinicopathologic characteristics of non-icteric pancreas head carcinoma based on a number of cases. The authors previously re- ported a clinicopathologic study of 96 cases of pancreas exocrine carcinoma [ 11 and also reported that non-icteric
0 1992 Wiley-Liss, Inc.
ampullary carcinoma fared better than icteric ampullary carcinoma because non-icteric ampullary carcinoma in- cluded a greater number of early ampullary carcinoma and papillary adenocarcinoma than icteric ampullary car- cinoma [4]. In our previous series of pancreas carcinoma, 22 patients were non-icteric at the time of clinical diagno- sis and had no history of jaundice. In this paper, we performed a comparative study of the 22 patients with non-icteric pancreas head carcinoma and 6 1 patients with
Accepted for publication January 10, 1992. Address reprints requests to Koji Yamaguchi, MD, Department of Surgery I, Kyushu University Faculty of Medicine, 3-1-1 Maidashi. Higashi-ku, Fukuoka 812, Japan.
254 Yamaguchi et al.
C B D
P D
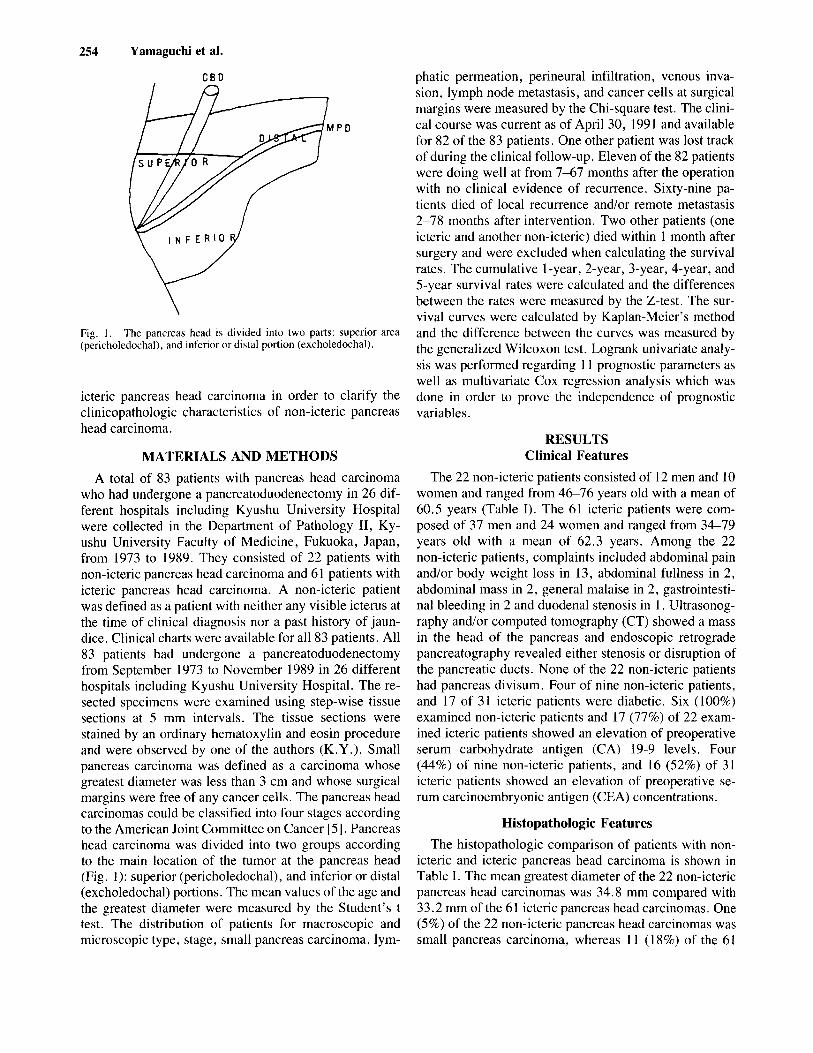
Fig. I . (pericholedochal), and inferior or distal portion (excholedochal).
The pancreas head is divided into two parts: superior area
icteric pancreas head carcinoma in order to clarify the clinicopathologic characteristics of non-icteric pancreas head carcinoma.
MATERIALS AND METHODS A total of 83 patients with pancreas head carcinoma
who had undergone a pancreatoduodenectomy in 26 dif- ferent hospitals including Kyushu University Hospital were collected in the Department of Pathology 11, Ky- ushu University Faculty of Medicine, Fukuoka, Japan, from 1973 to 1989. They consisted of 22 patients with non-icteric pancreas head carcinoma and 61 patients with icteric pancreas head carcinoma. A non-icteric patient was defined as a patient with neither any visible icterus at the time of clinical diagnosis nor a past history of jaun- dice. Clinical charts were available for all 83 patients. All 83 patients had undergone a pancreatoduodenectomy from September 1973 to November 1989 in 26 different hospitals including Kyushu University Hospital. The re- sected specimens were examined using step-wise tissue sections at 5 mm intervals. The tissue sections were stained by an ordinary hematoxylin and eosin procedure and were observed by one of the authors (K.Y.). Small pancreas carcinoma was defined as a carcinoma whose greatest diameter was less than 3 cm and whose surgical margins were free of any cancer cells. The pancreas head carcinomas could be classified into four stages according to the American Joint Committee on Cancer [5]. Pancreas head carcinoma was divided into two groups according to the main location of the tumor at the pancreas head (Fig. 1): superior (pericholedochal), and inferior or distal (excholedochal) portions. The mean values of the age and the greatest diameter were measured by the Student’s t test. The distribution of patients for macroscopic and microscopic type, stage, small pancreas carcinoma, lym-
phatic permeation, perineural infiltration, venous inva- sion, lymph node metastasis, and cancer cells at surgical margins were measured by the Chi-square test. The clini- cal course was current as of April 30, 1991 and available for 82 of the 83 patients. One other patient was lost track of during the clinical follow-up. Eleven of the 82 patients were doing well at from 7-67 months after the operation with no clinical evidence of recurrence. Sixty-nine pa- tients died of local recurrence and/or remote metastasis 2-78 months after intervention. Two other patients (one icteric and another non-icteric) died within 1 month after surgery and were excluded when calculating the survival rates. The cumulative 1-year, 2-year, 3-year, 4-year, and 5-year survival rates were calculated and the differences between the rates were measured by the Z-test. The sur- vival curves were calculated by Kaplan-Meier’s method and the difference between the curves was measured by the generalized Wilcoxon test. Logrank univariate analy- sis was performed regarding 11 prognostic parameters as well as multivariate Cox regression analysis which was done in order to prove the independence of prognostic variables.
RESULTS Clinical Features
The 22 non-icteric patients consisted of 12 men and 10 women and ranged from 4 6 7 6 years old with a mean of 60.5 years (Table I). The 61 icteric patients were com- posed of 37 men and 24 women and ranged from 34-79 years old with a mean of 62.3 years. Among the 22 non-icteric patients, complaints included abdominal pain and/or body weight loss in 13, abdominal fullness in 2, abdominal mass in 2, general malaise in 2, gastrointesti- nal bleeding in 2 and duodenal stenosis in 1. Ultrasonog- raphy and/or computed tomography (CT) showed a mass in the head of the pancreas and endoscopic retrograde pancreatography revealed either stenosis or disruption of the pancreatic ducts. None of the 22 non-icteric patients had pancreas divisum. Four of nine non-icteric patients, and 17 of 31 icteric patients were diabetic. Six (100%) examined non-icteric patients and 17 (77%) of 22 exam- ined icteric patients showed an elevation of preoperative serum carbohydrate antigen (CA) 19-9 levels. Four (44%) of nine non-icteric patients, and 16 (52%) of 31 icteric patients showed an elevation of preoperative se- rum carcinoembryonic antigen (CEA) concentrations.
Histopathologic Features The histopathologic comparison of patients with non-
icteric and icteric pancreas head carcinoma is shown in Table I. The mean greatest diameter of the 22 non-icteric pancreas head carcinomas was 34.8 mm compared with 33.2 mm of the 6 1 icteric pancreas head carcinomas. One (5%) of the 22 non-icteric pancreas head carcinomas was small pancreas carcinoma, whereas 1 1 (1 8%) of the 6 1
Pancreas Head Carcinoma 255
TABLE I. Clinicopathologic Features of Non-Icteric Pancreas Head Carcinoma and Icteric Pancreas Head Carcinoma*
Statistical Icteric Non-icteric significance"
No. of cases
Sex (M/F) Diameter (mm) Small pancreas carcinoma Location of tumor
Pericholedochal Excholedochal
Age
Inferior Distal
Macroscopic type Expansive Mixed Infiltrative
Stage I I1 111 IV
Well differentiated Moderately differentiated Poorly differentiated Others
Lymphatic permeation Yes
Perineural invasion Yes
Venous invasion Yes
Lymph node metastasis Yes
Cancer cells at surgical margins Yes
Microscopic type (adenocarcinoma)
61 62.3 f 9.6
37/24 33.2 f 9.8
I 1 (18%)
33 28 23
5
44 (72%) 9 (15%) 8 (13%)
14 (23%)
47 (77%) 0
0
34 (56%) 15 (25%) 6 (10%) 6 (10%)
52 (85%)
59 (97%)
37 (61%)
46 (75%)
34 (56%)
22 60.5 k 9.7
12/10 34.8 * 8.4
1(1%)
6 16 12 4
11 (50%) 7 (32%) 4 (18%)
4 (18%) 0
18 (88%) 0
9 (41%) 7 (32%) 2 (9%) 4 (18%)
20 (91%)
21 (95%)
13 (59%)
15 (68%)
1 1 (50%)
N.S. N.S. N.S. N.S.
P < 0.05
N.S.
N.S.
N.S.
N.S.
N.S.
N.S.
N.S.
N.S.
* dif.: differentiated adenocarcinoma, ly: lymphatic permeation, pn: perineural invasion, v: venous invasion, n: lymph node metastasis. ew: cancer cells at surgical margins. a N.S.: not significant.
icteric pancreas head carcinomas were small pancreas head carcinomas. The majority of non-icteric and icteric pancreas head carcinomas were well-circumscribed and expansive in margin and were tubular adenocarcinomas of a differentiated type. Non-icteric pancreas head carci- noma showed invasion to the lymphatic (91%), perineu- ral (95%), and venous (59%) spaces, compared with 8.596, 97%, and 6 1 % of icteric pancreas head carcinoma, respectively. Non-icteric pancreas head carcinoma me- tastasized to the lymph nodes in 15 (68%) of the 22 cases, while icteric pancreas head carcinoma did so in 46 (75%) of the 61 cases. The resected margins mainly in the retro- peritoneal aspects were affected by malignant cells in 11 (50%) of the 22 non-icteric pancreas head carcinomas, compared with 34 (56%) of the 61 cases of icteric pan- creas head carcinomas. Sixteen (73%) of the 22 non- icteric pancreas head carcinomas were located in excho-
ledochal areas (12 in inferior and 4 in distal), while 33 (54%) of the 61 icteric pancreas head carcinomas were situated in the pericholedochal region (P < 0.05). Eight of the 22 non-icteric pancreas head carcinomas were 10- cated in the uncinate process of the pancreas head.
Clinical Course The cumulative 2-year and 4-year survival rates of the
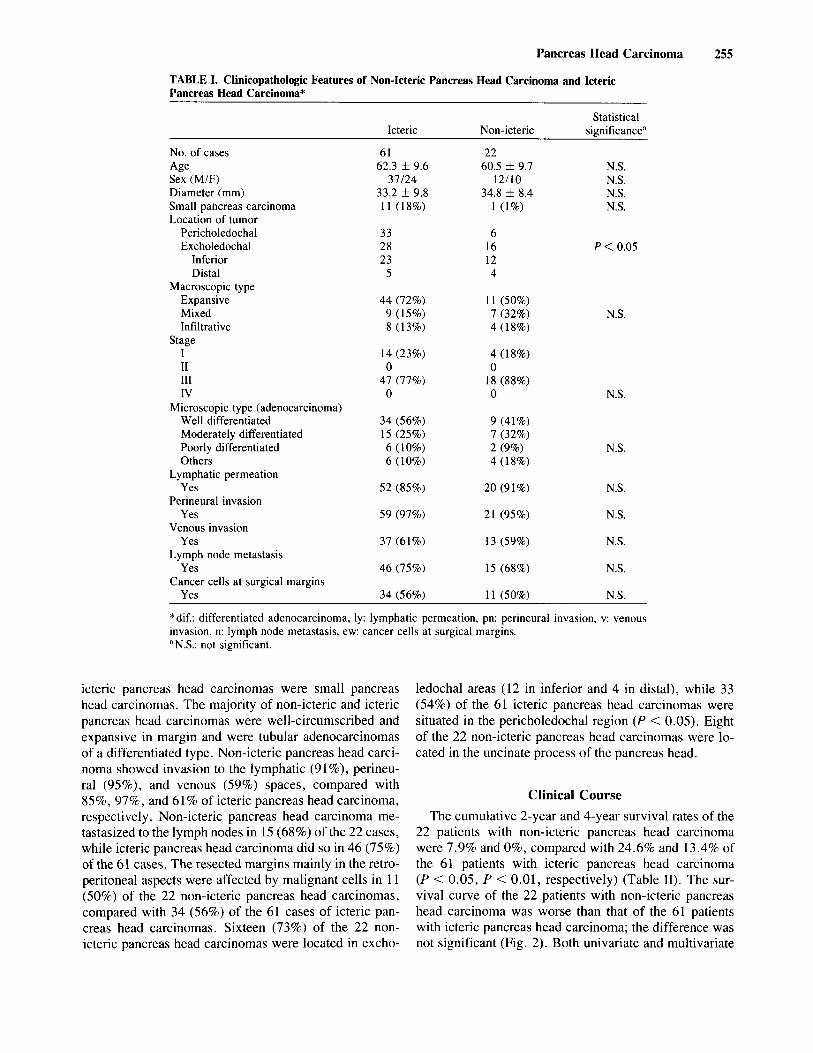
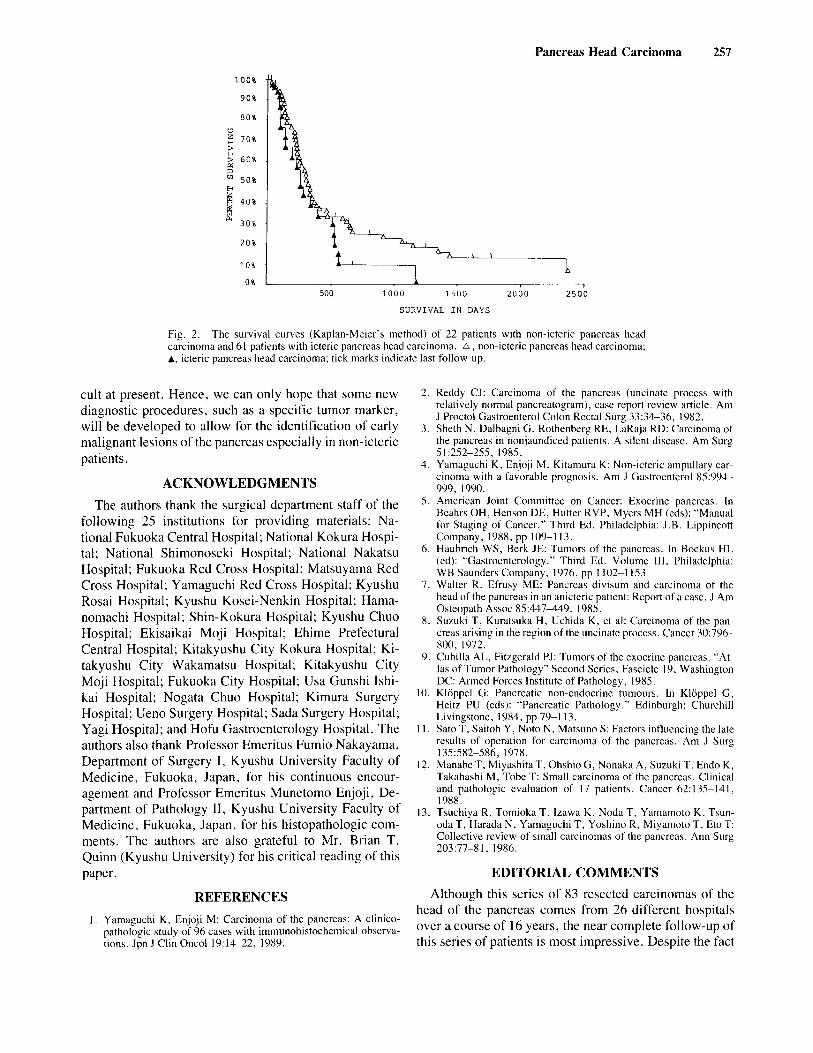
22 patients with non-icteric pancreas head carcinoma were 7.9% and 0%, compared with 24.6% and 13.4% of the 61 patients with icteric pancreas head carcinoma (P < 0.05, P < 0.01, respectively) (Table 11). The sur- vival curve of the 22 patients with non-icteric pancreas head carcinoma was worse than that of the 61 patients with icteric pancreas head carcinoma; the difference was not significant (Fig. 2). Both univariate and multivariate

256 Yamaguchi et al.
TABLE 11. Cumulative Survival Rates of Non-Icteric and Icteric Pancreas Head Carcinoma
Cumulative survival rates
1-year 2-year 3-year 4-year 5-year
lcteric 41% 2 5 W 19% 13%’ 13% (61)
(22) Non-icteric 38% 8%a 5% O%b 0%
aP < 0.05. h P < 0.01.
analyses failed to reveal evidence that icterus was an independent prognostic variable of pancreas head carci- noma.
DISCUSSION Early specific symptoms and signs pointing toward the
diagnosis of pancreas cancer are normally absent or un- recognized in the majority of cases until jaundice appears [ 11. According to Haubrich and Berk [6] jaundice is ab- sent in at least 50% of patients when they are first seen, and never ensues in approximately 20% of patients. Pa- tients with pancreas head carcinoma develop icterus ear- lier than patients with pancreas body or tail carcinoma. The symptoms and signs of pancreas body or tail carci- noma are nonspecific and the diagnosis of pancreas body or tail carcinoma is rarely made until the tumor has ad- vanced substantially. Patients with pancreas head carci- noma usually fare better than those with pancreas body or tail carcinoma. Most patients with pancreas head carci- noma are icteric at the time of clinical diagnosis but some patients remain non-icteric even in advanced stages. Very few authors have reported the clinicopathologic features of non-icteric pancreas head carcinoma [2,3,7].
We previously reported that non-icteric ampullary car- cinoma fared better than icteric ampullary carcinoma be- cause non-icteric ampullary carcinoma included a greater number of early ampullary carcinoma and papillary ade- nocarcinoma than icteric ampullary carcinoma [4]. We first expected that non-icteric pancreas head carcinoma would include a large number of early pancreas head carcinoma. One (5%) of the 22 non-icteric pancreas head carcinomas was small pancreas carcinoma, whereas 11 (18%) of the 61 icteric pancreas head carcinomas were small pancreas head carcinomas. Non-icteric pancreas head carcinoma originated far from the biliary tree and included a larger number of large pancreas carcinomas, while icteric pancreas head carcinoma arose near the common bile duct and included a larger number of small tumors.
Suzuki et al. [8] previously reported six cases of carci- noma arising in the uncinate process of the pancreas head with a poor prognosis. Five of the six patients did not
develop jaundice. The uncinate process is a hook-like extension of the lower part of the head of the pancreas and is located very near the vital structures such as the hepatic artery, portal vein, and vena cava. Therefore, carcinoma of the uncinate process easily invades the vital organs and the clinical course of the patients is dismal, even if the tumor is resectable. In the present series, 8 of the 22 non-icteric tumors (8 of the 12 non-icteric tuniors in the inferior area) corresponded to carcinoma of the uncinate process. In the four non-icteric pancreas head carcinomas in the distal portion, the tumors were located just above the portal vein and the retroperitoneal aspects of the resected specimens were affected by malignant cells.
Walter and Efrusy [7] reported a case of a combination of pancreas divisum and carcinoma of the pancreas head in a non-icteric patient, which reflected the unusual ana- tomic drainage of the pancreas divisum. In the present study, none of the 22 non-icteric patients had pancreas divisum.
The patients with pancreas head carcinoma associated with obstructive jaundice can be diagnosed much earlier than those in whom jaundice is absent. In cases of non- icteric pancreas head carcinoma, the symptoms and signs are so vague that they can often be confused with those of other conditions. Routine laboratory tests aid little in the definitive diagnosis of the disease. Sophisticated new modalities of diagnosis such as ultrasonography, endo- scopic retrograde cholangiography, and CT scanning fre- quently can lead to a correct diagnosis, but tests are seldom performed unless there is a strong suspicion that carcinoma of the pancreas may exist. Most patients with non-icteric pancreas head carcinoma suffer from persis- tent unexplained abdominal pain, marked anorexia, and weight loss. Clinicians should consider non-icteric pancreas head carcinoma whenever patients present with abdominal pain or general malaise and they should be subjected to sophisticated diagnostic testing.
Various prognostic parameters have been reported re- garding pancreas carcinoma, i.e., site of tumor [9,10], size of tumor [ 1 11, histopathologic type [9, lo], histo- pathologic stage [9,10], and so forth. We now add an- other prognostic factor: the presence or absence of ic- terus, regarding pancreas head carcinoma.
Some cases of small pancreas carcinoma (less than 3 cm in the largest diameter) have been reported recently [12,13]. However, most of them are symptomatic (ic- teric) clinically, and infiltrative in nature and the clinical course is not always favorable. Small pancreas carcinoma does not always mean early pancreas carcinoma. Only minute pancreas carcinoma in the asymptomatic (non- icteric) phase can be expected to yield a favorable prog- nosis which is worth calling “early pancreas head carci- noma.” Despite the advances of diagnostic modalities, the early diagnosis of pancreas carcinoma remains diffi-
Pancreas Head Carcinoma 257
1 0 0 %
90%
8 0 %
7 0 %
2 60% 3
5 0 %
6 40%
30%
20%
1 0 %
(3
z
ej !&
0 % L 1 i
500 1 0 0 0 1 5 0 0 2 0 0 0 2 5 0 0
SURVIVAL IN DAYS
Fig. 2. The survival curves (Kaplan-Meier’s method) of 22 patients with non-icteric pancreas head carcinoma and 61 patients with icteric pancreas head carcinoma. a, non-icteric pancreas head carcinoma; A, icteric pancreas head carcinoma; tick marks indicate last follow-up.
cult at present. Hence, we can only hope that some new diagnostic procedures, such as a specific tumor marker, will be developed to allow for the identification of early malignant lesions of the pancreas especially in non-icteric patients.
ACKNOWLEDGMENTS The authors thank the surgical department staff of the
following 25 institutions for providing materials: Na- tional Fukuoka Central Hospital; National Kokura Hospi- tal; National Shimonoseki Hospital; National Nakatsu Hospital; Fukuoka Red Cross Hospital; Matsuyama Red Cross Hospital; Yamaguchi Red Cross Hospital; Kyushu Rosai Hospital; Kyushu Kosei-Nenkin Hospital; Hama- nomachi Hospital; Shin-Kokura Hospital; Kyushu Chuo Hospital; Ekisaikai Moji Hospital; Ehime Prefectural Central Hospital; Kitakyushu City Kokura Hospital; Ki- takyushu City Nakamatsu Hospital; Kitakyushu City Moji Hospital; Fukuoka City Hospital; Usa Gunshi Ishi- kai Hospital; Nogata Chuo Hospital; Kimura Surgery Hospital; Ueno Surgery Hospital; Sada Surgery Hospital; Yagi Hospital; and Hofu Gastroenterology Hospital. The authors also thank Professor Emeritus Fumio Nakayama, Department of Surgery I, Kyushu University Faculty of Medicine, Fukuoka, Japan, for his continuous encour- agement and Professor Emeritus Munetomo Enjoji, De- partment of Pathology 11, Kyushu University Faculty of Medicine, Fukuoka, Japan, for his histopathologic com- ments. The authors are also grateful to Mr. Brian T. Quinn (Kyushu University) for his critical reading of this paper.
REFERENCES I , Yamaguchi K, Enjoji M: Carcinoma of the pancreas: A clinico-
pathologic study of 96 cases with immunohistochemical observa- tions. Jpn J Clin Oncol 19:14-22, 1989.
2. Reddy CJ: Carcinoma of the pancreas (uncinate process with relatively normal pancreatogram), case report review article. Am J Proctol Gastroenterol Colon Rectal Surg 33:34-36, 1982.
3. Sheth N , Dalbagni G, Rothenberp RE, LaRaja RD: Carcinoma of the pancreas in nonjaundiced patients. A silent disease. Am Surg 51:252-255, 1985.
4. Yamaguchi K, Enjoji M, Kitamura K: Non-icteric ampullary car- cinoma with a favorable prognosis. Am J Gastroenterol 85:994- 999, 1990.
5 . American Joint Committee on Cancer: Exocrine pancreas. In Beahrs OH, Henson DE, Hutter RVP, Myers MH (eds): “Manual for Staging of Cancer.” Third Ed. Philadelphia: J .B. Lippincott Company, 1988, pp 109-1 13.
6. Haubrich WS, Berk JE: Tumors of the pancreas. In Bockus HL (ed): “Gastroenterology.” Third Ed. Volume I l l , Philadelphia: WB Saunders Company, 1976, pp 1102-1 153.
7. Walter R, Efrusy ME: Pancreas divisum and carcinoma of the head of the pancreas in an anicteric patient: Report of a case. J Am Osteopath Assoc 85:447449, 1985.
8. Suzuki T, Kuratsuka H, Uchida K, et al: Carcinoma of the pan- creas arising in the region of the uncinate process. Cancer 30:796- 800, 1972.
9. Cubilla AL, Fitzgerald PJ: Tumors of the exocrine pancreas. “At- las of Tumor Pathology” Second Series, Fascicle 19, Washington DC: Armed Forces Institute of Pathology, 1985.
10. Kloppel G: Pancreatic non-endocrine tumours. In Kloppel G, Heitz PU (eds): “Pancreatic Pathology.” Edinburgh: Churchill Livingstone, 1984, pp 79-1 13.
1 I . Sato T, Saitoh Y, Noto N , Matsuno S: Factors influencing the late results of operation for carcinoma of the pancreas. Am J Surg 135:582-586, 1978.
12. Manabe T, Miyashita T, Ohshio G, Nonaka A, Suzuki T, Endo K, Takahashi M, Tobe T: Small carcinoma of the pancreas. Clinical and pathologic evaluation of 17 patients. Cancer 62: 135-141, 1988.
13. Tsuchiya R, Tomioka T , lzawa K , Noda T, Yamamoto K, Tsun- oda T, Harada N , Yamaguchi T , Yoshino R, Miyamoto T, Eto T: Collective review of small carcinomas of the pancreas. Ann Surg 203:77-8 I , 1986.
EDITORIAL COMMENTS Although this series of 83 resected carcinomas of the
head of the pancreas comes from 26 different hospitals over a course of 16 years, the near complete follow-up of this series of patients is most impressive. Despite the fact

258 Yamaguchi et al.
that it is hard to consider the operative treatment approach employed as uniform over time and throughout such a heterogenous group of institutions, the distribution of various characteristics of the patients in this series was amazingly similar for the icteric and non-icteric groups. The only real difference, beside the location of lesions in the head of the pancreas, was the higher proportion of small pancreatic carcinomas in the icteric group.
We usually think of non-icteric carcinomas of the head and body of the pancreas as having an unusually poor prognosis because they tend to become non-resectable prior to our ability to establish the diagnosis. This poten- tial reason for a difference in prognosis between these non-icteric patients and carcinomas producing obstruc- tive jaundice is actually eliminated by the design of their study-including only patients who have undergone total gross resection of their disease. Their data do demon- strate, however, that obstructive jaundice is a more effi-
cient way to trigger appropriate diagnostic measures while the cancer is relatively small.
Although the authors seemed impressed by the fact that these results were opposite to those from their own study with ampullary carcinoma, this does not seem too sur- prising. Ampullary carcinomas that do not produce jaun- dice must be quite small, when originating at this specific site. In contrast to patients with cancers located in the pancreatic head, icteric patients have larger lesions than non-icteric patients with ampullary cancer. Overall, these results are not surprising but this may be the first time this issue has been as carefully studied as it has been by this group.
Walter Lawrence, Jr., MD
Medical College of Virginia Richmond, Virginia 23298
Recommended

















