
Original Investigation
Outcomes of Patients Receiving Maintenance Dialysis AdmittedOver Weekends
Ankit Sakhuja, MD,1 Jesse D. Schold, PhD,1,2 Gagan Kumar, MD,3 Aaron Dall, MD,4
Puneet Sood, MD,5 and Sankar D. Navaneethan, MD, MPH1
Background: Hospital admissions over weekends have been associated with worse outcomes in differentpatient populations. The cause of this difference in outcomes remains unclear; however, different staffingpatterns over weekends have been speculated to contribute. We evaluated outcomes in patients on mainte-nance dialysis therapy admitted over weekends using a national database.
Study Design: Retrospective cohort study.Setting & Participants: We included nonelective admissions of adult patients (�18 years) on maintenance
dialysis therapy (n � 3,278,572) identified using appropriate International Classification of Diseases, NinthRevision, Clinical Modification (ICD-9-CM) codes for 2005-2009 using the Nationwide Inpatient Sampledatabase.
Predictor: Weekend versus weekday admission.Outcomes: The primary outcome measure was all-cause in-hospital mortality. Secondary outcomes
included mortality by day 3 of admission, length of hospital stay, time to death, and discharge disposition.Measurements: We adjusted for patient and hospital characteristics, payer, year, comorbid conditions, and
primary discharge diagnosis common to maintenance dialysis patients.Results: There were an estimated 704,491 admissions over weekends versus 2,574,081 over weekdays.
Unadjusted all-cause in-hospital mortality was 40,666 (5.8%) for weekend admissions in comparison to138,517 (5.4%) for weekday admissions (P � 0.001). In a multivariable model, patients admitted overweekends had higher all-cause in-hospital mortality (OR, 1.06; 95% CI, 1.01-1.10) in comparison to thoseadmitted over weekdays and higher mortality during the first 3 days of admission (OR, 1.18; 95% CI,1.10-1.26). Patients admitted over weekends were less likely to be discharged to home, had longer hospitalstays, and had shorter times to death compared with those admitted over weekdays on adjusted analysis.
Limitations: Use of ICD-9-CM codes to identify patients, defining weekend as midnight Friday to midnightSunday.
Conclusions: Maintenance dialysis patients admitted over weekends have increased mortality rates andlonger lengths of stay compared with those admitted over weekdays. Further studies are needed to identify thereasons for worse outcomes for weekend admissions in this patient population.Am J Kidney Dis. 62(4):763-770. © 2013 by the National Kidney Foundation, Inc.
INDEX WORDS: Dialysis; admissions; mortality.
A growing body of literature demonstrates unfa-vorable outcomes for weekend hospital admis-
sions in comparison to weekdays. This phenomenonhas been highlighted in several patient populations,including those with myocardial infarction,1 stroke,2
intracerebral hemorrhage,3 gastrointestinal bleeding,4
pulmonary embolism,5 ruptured abdominal aortic an-eurysm,5 acute epiglottitis,5 and recently, acute kid-ney injury.6 Although the cause of this phenomenonremains elusive, potential explanations include differ-ential staffing models with limited availability ofclinician expertise, unmeasured differences in sever-ity of illness, and decreased accessibility to diagnosticand therapeutic procedures.
End-stage renal disease (ESRD) defined as kidneyfailure necessitating kidney replacement therapy, mostoften in the form of hemodialysis, is a growingepidemic in the United States. The present population-wide prevalence is estimated to be 1,700 patients permillion, with a projection of more than 700,000 preva-
lent patients by 2015.7 According to the US RenalAm J Kidney Dis. 2013;62(4):763-770
Data System 2012 annual data report, there were 340new cases of ESRD per million population in 2010.8
ESRD constitutes a unique group of patients who arehospitalized frequently, and the in-hospital mortalityis on average 6-8 times greater than that in the generalpopulation (Collins et al,8 volume 2, chapters 1 and5). Given their complex nature and propensity to
From the Departments of 1Nephrology and Hypertension and2Quantitative Health Sciences, Cleveland Clinic, Cleveland, OH;Divisions of 3Pulmonary and Critical Care Medicine and 4Ne-phrology, Department of Medicine, Medical College of Wisconsin,Milwaukee, WI; and 5Renal-Electrolyte Division, University ofPittsburgh Medical Center, Pittsburgh, PA.
Received October 9, 2012. Accepted in revised form March 6,2013. Originally published online May 13, 2013.
Address correspondence to Ankit Sakhuja, MD, Department ofNephrology and Hypertension, Glickman Urological and KidneyInstitute, Cleveland Clinic, Q7, 9500 Euclid Ave, Cleveland, OH44195. E-mail: [email protected]
© 2013 by the National Kidney Foundation, Inc.0272-6386/$36.00
http://dx.doi.org/10.1053/j.ajkd.2013.03.014763
Sakhuja et al
develop volume and metabolic derangements, pa-tients with ESRD, especially those on maintenancedialysis therapy who need hospitalization, likely wouldrequire timely access to expert nephrology consulta-tion and renal replacement therapy.
Worse outcomes for weekend admissions, althoughdemonstrated for many time-sensitive medical condi-tions, have not been studied in maintenance dialysispatients. Thus, we aimed to study whether this phe-nomenon existed for hospital admissions of patientsreceiving maintenance dialysis. We used a large nation-ally representative database (the Nationwide InpatientSample [NIS] database) to describe the mortalitydifferences and other associated outcomes betweenweekday and weekend admissions of patients onmaintenance dialysis therapy.
METHODS
StudyDesign
We designed a retrospective cohort study using the HealthcareCost and Utilization Project-NIS, the largest all-payer inpatientcare database publicly available in the United States. This is anadministrative data set created by the Agency for HealthcareResearch and Quality that contains data from the 20%-stratifiedsample of US community hospitals.9 Each hospitalization is treatedas an individual entry in the database and is coded with oneprincipal diagnosis, up to 14 secondary diagnoses, and 15 proce-dural diagnoses associated with that stay. NIS encompasses infor-mation for all patients regardless of payer, including privateinsurance and the uninsured. It also includes patient informationregardless of type of hospital: teaching or nonteaching, rural orurban, large or small volume, and private or publicly owned. Tofacilitate the projection of national estimates, both hospital anddischarge weights are provided, along with information necessaryto calculate the variance of estimates.
The NIS collects information for common demographic vari-ables, such as age, race, and sex, along with primary and secondaryinsurance and hospital-level characteristics such as teaching status,location (rural vs urban), size of hospital, and hospital region.Facilities are considered to be teaching hospitals if they have anAmerican Medical Association–approved residency program, are amember of the Council of Teaching Hospitals, or have a ratio offulltime-equivalent interns and residents to patients of 0.25 orhigher. Hospital location (rural/urban) and bed size also are de-fined. The bed size cutoff values are chosen so that approximatelyone-third of the hospitals in a given region, location, and teachingstatus combination would fall within each bed size category(small, medium, and large). From 2004 in the NIS, hospitals with acore-based statistical area type of metropolitan were categorized asurban, whereas hospitals with a core-based statistical area type ofrural were categorized as rural. Data from 2005-2009 were usedfor this study.
StudyPopulation
We included all admissions of adult patients (aged �18 years)from the NIS database for 2005-2009 who were on maintenancedialysis therapy. Maintenance dialysis status was defined as pa-tients with an International Classification of Diseases, NinthRevision, Clinical Modification (ICD-9-CM) code for ESRD (585.6)or procedure code for hemodialysis (39.95) or peritoneal dialysis
(54.98), but absence of ICD-9-CM code for acute kidney injury764
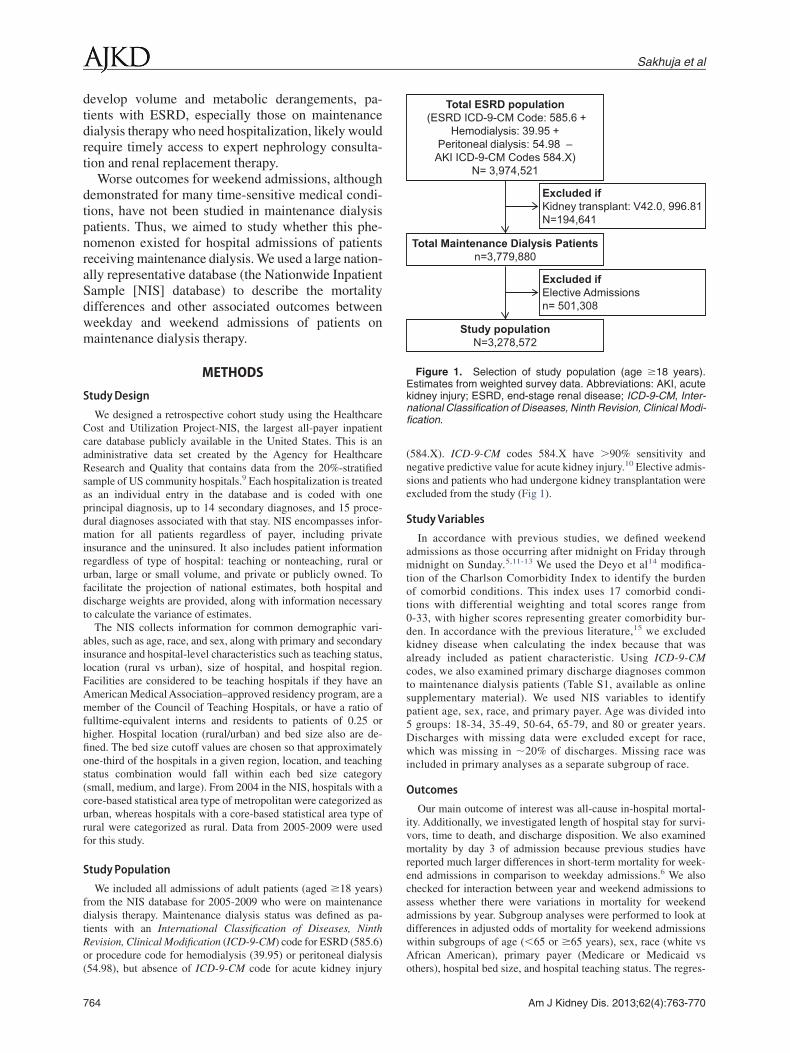
(584.X). ICD-9-CM codes 584.X have �90% sensitivity andnegative predictive value for acute kidney injury.10 Elective admis-sions and patients who had undergone kidney transplantation wereexcluded from the study (Fig 1).
StudyVariables
In accordance with previous studies, we defined weekendadmissions as those occurring after midnight on Friday throughmidnight on Sunday.5,11-13 We used the Deyo et al14 modifica-tion of the Charlson Comorbidity Index to identify the burdenof comorbid conditions. This index uses 17 comorbid condi-tions with differential weighting and total scores range from0-33, with higher scores representing greater comorbidity bur-den. In accordance with the previous literature,15 we excludedkidney disease when calculating the index because that wasalready included as patient characteristic. Using ICD-9-CMcodes, we also examined primary discharge diagnoses commonto maintenance dialysis patients (Table S1, available as onlinesupplementary material). We used NIS variables to identifypatient age, sex, race, and primary payer. Age was divided into5 groups: 18-34, 35-49, 50-64, 65-79, and 80 or greater years.Discharges with missing data were excluded except for race,which was missing in �20% of discharges. Missing race wasincluded in primary analyses as a separate subgroup of race.
Outcomes
Our main outcome of interest was all-cause in-hospital mortal-ity. Additionally, we investigated length of hospital stay for survi-vors, time to death, and discharge disposition. We also examinedmortality by day 3 of admission because previous studies havereported much larger differences in short-term mortality for week-end admissions in comparison to weekday admissions.6 We alsochecked for interaction between year and weekend admissions toassess whether there were variations in mortality for weekendadmissions by year. Subgroup analyses were performed to look atdifferences in adjusted odds of mortality for weekend admissionswithin subgroups of age (�65 or �65 years), sex, race (white vsAfrican American), primary payer (Medicare or Medicaid vs
Total ESRD population(ESRD ICD-9-CM Code: 585.6 +
Hemodialysis: 39.95 +Peritoneal dialysis: 54.98 –
AKI ICD-9-CM Codes 584.X)N= 3,974,521
Total Maintenance Dialysis Patientsn=3,779,880
Study populationN=3,278,572
Excluded if Kidney transplant: V42.0, 996.81N=194,641
Excluded ifElective Admissionsn= 501,308
Figure 1. Selection of study population (age �18 years).Estimates from weighted survey data. Abbreviations: AKI, acutekidney injury; ESRD, end-stage renal disease; ICD-9-CM, Inter-national Classification of Diseases, Ninth Revision, Clinical Modi-fication.
others), hospital bed size, and hospital teaching status. The regres-
Am J Kidney Dis. 2013;62(4):763-770

Weekend Maintenance Dialysis Admissions
sion coefficients were compared using a generalized Hausmantest.16,17
Statistical Analysis
Stata IC 11.0 (StataCorp LP) was used for all analyses. We usedweights provided with the NIS to generate national estimates of thenumber of admissions in each age group using the survey com-mands. The �2 test was used to compare categorical variablesbetween patients admitted on the weekend and those admitted onweekdays. Because length of stay of survivors and time to deathwere not normally distributed, t test was performed on log-transformed values.
We examined factors associated with in-hospital mortality bymultivariable logistic regression. Univariable logistic regressionwas used to identify risk factor variables associated with in-hospital mortality. All variables that were significant at P � 0.10were included in the final multivariable model. To control forvariability by year, we used year as a predictor in regressionmodels. We checked variables for multicollinearity using toleranceand variance inflation factor. For variables used in the final model,both tolerance and variation inflation factor were very close tounity. Similarly, for factors associated with length of stay ofsurvivors and time to death, univariable and multivariable linearregressions were performed.
We examined for interactions between weekend admissionsand cardiovascular diseases,2,18-21 gastrointestinal bleed,11 hos-pital bed size,6 or teaching status,22 as has been suggested in theliterature. Significant interaction terms were included in theappropriate final multivariable models. For all-cause in-hospitalmortality, we found significant interactions between weekendadmission and primary discharge diagnosis of cardiovasculardisease and weekend admission and teaching status of thehospital, which were both included in the final regressionmodel. Similarly for length of stay of survivors, significantinteraction with weekend admissions was found only withhospital bed size.
We performed 5 sensitivity analyses to further evaluate therobustness of our results. To account for multiple admissions ofsame patients (readmissions), we identified hospital records withsimilar age, sex, race, primary payer, hospital identification code,and year of admission, as done previously in literature.23 For thefirst sensitivity analysis, we included all unique observations alongwith one of each duplicate observation randomly selected from thedatabase. For the second sensitivity analysis, we included allunique observations along with one of each duplicate admitted inthe first month for that duplicate observation. Similarly for thethird sensitivity analysis, we included all unique observationsalong with one of each duplicate observation admitted in the lastmonth for that duplicate observation. Finally, we did anothersensitivity analysis including only unique observations and exclud-ing any duplicate observations (Table S2). Because race wasmissing for �20% of observations, we performed another sensitiv-ity analysis excluding race.
RESULTS
Patient Characteristics
Using the NIS database, during the 5-year time-frame of our study (2005-2009), there were an esti-mated 3,278,572 (95% confidence interval [CI],3,104,322-3,452,822) discharges on maintenance di-alysis therapy. Of those, an estimated 704,491 (95%
CI, 654,945-754,038) were admitted over weekends.Am J Kidney Dis. 2013;62(4):763-770
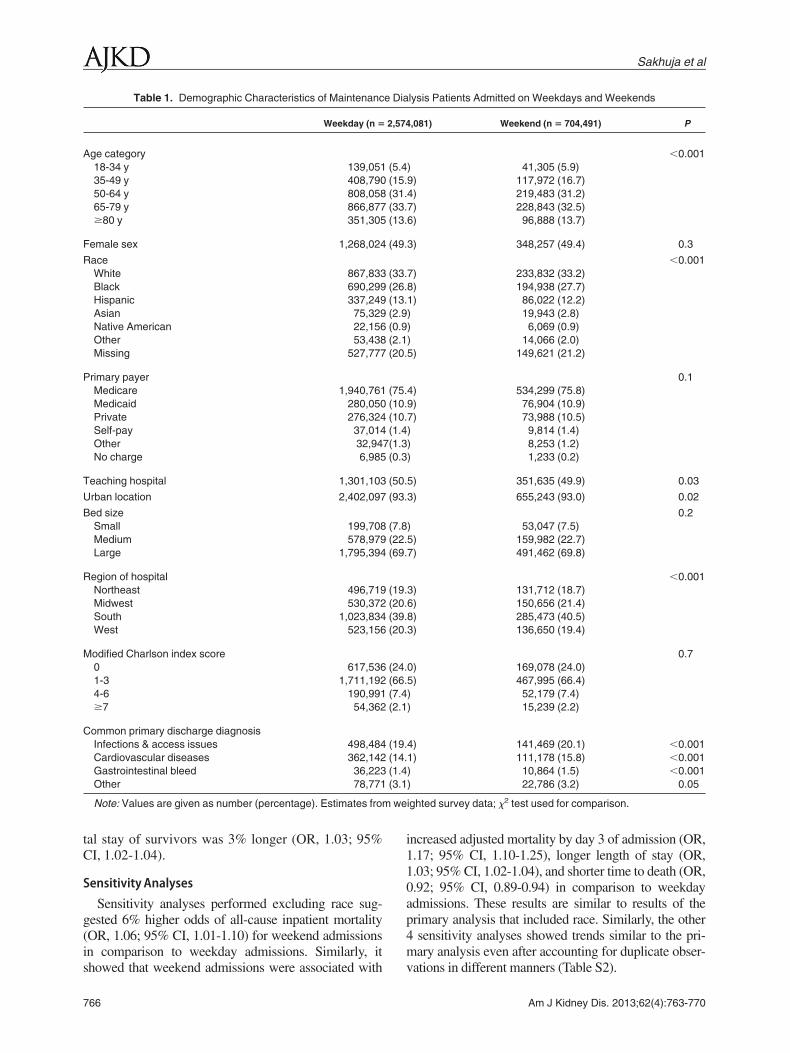
Baseline characteristics of patients in terms of age,sex, other demographics, comorbid conditions, andhospital characteristics are listed in Table 1. Pa-tients admitted over weekends were more likely tobe aged 18-49 or 80 years or older, African Ameri-cans, and admitted less often to teaching hospitals.Primary discharge diagnoses common to mainte-nance dialysis patients included any infection oraccess complication, cardiovascular disease (includ-ing heart failure, acute coronary syndrome, andatrial fibrillation/flutter and stroke), gastrointestinalbleed, and others (including hypertensive emer-gency and hyperkalemia).
Mortality
Unadjusted all-cause in-hospital mortality was5.4% for dialysis patients admitted during the week-days in comparison to 5.8% for weekend admis-sions (Table 2). Even after adjusting relevant cova-riates, weekend admissions were associated with a6% higher odds of death compared with those whowere admitted during the weekdays (odds ratio[OR], 1.06; 95% CI, 1.01-1.10; Fig 2; Table 3).Unadjusted mortality by day 3 of admission simi-larly was higher on weekends (5.4% vs 4.5%; P �0.001) compared with weekdays. After adjustingfor relevant covariates, dialysis patients admittedover the weekends had an 18% higher odds of deathby day 3 of admission than those who were admit-ted on weekdays (OR, 1.18; 95% CI, 1.10-1.26).
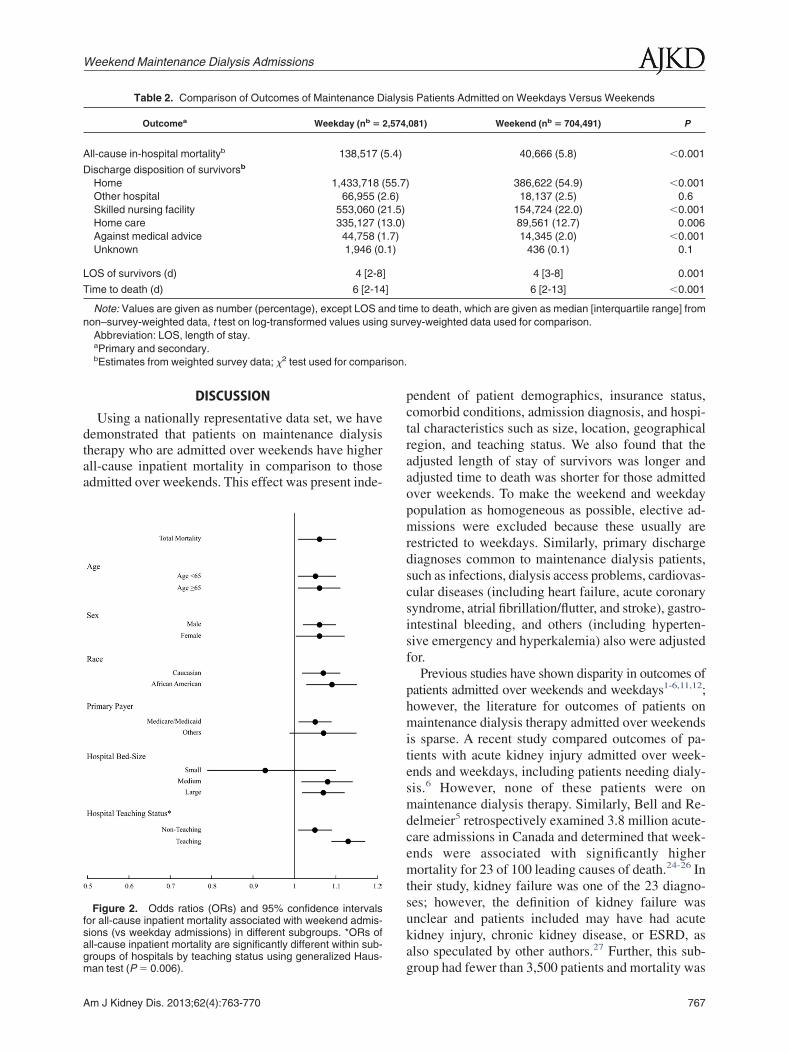
We did not find a significant difference in ad-justed odds of mortality for weekend admissionswithin subgroups of age (�65 or �65 years), sex,race (white vs African American), primary payer(Medicare or Medicaid vs others), or hospital bedsize, but the adjusted odds of mortality in weekendadmissions was significantly higher in teachinghospitals in comparison to nonteaching hospitals(Fig 2). To assess whether the relationship changesover time, we also checked for interaction betweenyear and weekend admissions, which was not sig-nificant.
Disposition andLengthof Stay
Patients admitted over weekends were less likely tobe discharged to home and more likely to be trans-ferred to skilled nursing facilities in comparison tothose admitted over weekdays (P � 0.001 for both;Table 2). We also found that time to death was shorterand length of stay of survivors was longer for week-end admissions in comparison to weekday admissions(Table 2). Similarly, in comparison to those admittedover weekdays, the adjusted time to death of patientsadmitted over weekends was 9% shorter (OR, 0.91;
95% CI, 0.89-0.94), and the adjusted length of hospi-765
m we
Sakhuja et al
tal stay of survivors was 3% longer (OR, 1.03; 95%CI, 1.02-1.04).
SensitivityAnalyses
Sensitivity analyses performed excluding race sug-gested 6% higher odds of all-cause inpatient mortality(OR, 1.06; 95% CI, 1.01-1.10) for weekend admissionsin comparison to weekday admissions. Similarly, it
Table 1. Demographic Characteristics of Maintenanc
Weekday (n �
Age category18-34 y 139,05135-49 y 408,79050-64 y 808,05865-79 y 866,877�80 y 351,305
Female sex 1,268,024
RaceWhite 867,833Black 690,299Hispanic 337,249Asian 75,329Native American 22,156Other 53,438Missing 527,777
Primary payerMedicare 1,940,761Medicaid 280,050Private 276,324Self-pay 37,014Other 32,94No charge 6,985
Teaching hospital 1,301,103
Urban location 2,402,097
Bed sizeSmall 199,708Medium 578,979Large 1,795,394
Region of hospitalNortheast 496,719Midwest 530,372South 1,023,834West 523,156
Modified Charlson index score0 617,5361-3 1,711,1924-6 190,991�7 54,362
Common primary discharge diagnosisInfections & access issues 498,484Cardiovascular diseases 362,142Gastrointestinal bleed 36,223Other 78,771
Note: Values are given as number (percentage). Estimates fro
showed that weekend admissions were associated with
766
increased adjusted mortality by day 3 of admission (OR,1.17; 95% CI, 1.10-1.25), longer length of stay (OR,1.03; 95% CI, 1.02-1.04), and shorter time to death (OR,0.92; 95% CI, 0.89-0.94) in comparison to weekdayadmissions. These results are similar to results of theprimary analysis that included race. Similarly, the other4 sensitivity analyses showed trends similar to the pri-mary analysis even after accounting for duplicate obser-
lysis Patients Admitted on Weekdays and Weekends
,081) Weekend (n � 704,491) P
�0.001) 41,305 (5.9)9) 117,972 (16.7)4) 219,483 (31.2)7) 228,843 (32.5)6) 96,888 (13.7)
3) 348,257 (49.4) 0.3
�0.0017) 233,832 (33.2)8) 194,938 (27.7)1) 86,022 (12.2)) 19,943 (2.8)) 6,069 (0.9)) 14,066 (2.0)5) 149,621 (21.2)
0.14) 534,299 (75.8)9) 76,904 (10.9)7) 73,988 (10.5)) 9,814 (1.4)) 8,253 (1.2)) 1,233 (0.2)
5) 351,635 (49.9) 0.03
3) 655,243 (93.0) 0.02
0.2) 53,047 (7.5)5) 159,982 (22.7)7) 491,462 (69.8)
�0.0013) 131,712 (18.7)6) 150,656 (21.4)8) 285,473 (40.5)3) 136,650 (19.4)
0.70) 169,078 (24.0)5) 467,995 (66.4)) 52,179 (7.4)) 15,239 (2.2)
4) 141,469 (20.1) �0.0011) 111,178 (15.8) �0.001) 10,864 (1.5) �0.001) 22,786 (3.2) 0.05
ighted survey data; �2 test used for comparison.
e Dia
2,574
(5.4(15.(31.(33.(13.
(49.
(33.(26.(13.(2.9(0.9(2.1(20.
(75.(10.(10.(1.4
7(1.3(0.3
(50.
(93.
(7.8(22.(69.
(19.(20.(39.(20.
(24.(66.(7.4(2.1
(19.(14.(1.4(3.1
vations in different manners (Table S2).
Am J Kidney Dis. 2013;62(4):763-770
ison.
Weekend Maintenance Dialysis Admissions
DISCUSSION
Using a nationally representative data set, we havedemonstrated that patients on maintenance dialysistherapy who are admitted over weekends have higherall-cause inpatient mortality in comparison to thoseadmitted over weekends. This effect was present inde-
Table 2. Comparison of Outcomes of Maintenance D
Outcomea Weekday (nb �
All-cause in-hospital mortalityb 138,517 (
Discharge disposition of survivorsb
Home 1,433,718 (Other hospital 66,955 (2Skilled nursing facility 553,060 (2Home care 335,127 (1Against medical advice 44,758 (1Unknown 1,946 (0
LOS of survivors (d) 4 [2-8
Time to death (d) 6 [2-14
Note: Values are given as number (percentage), except LOS anon–survey-weighted data, t test on log-transformed values usin
Abbreviation: LOS, length of stay.aPrimary and secondary.bEstimates from weighted survey data; �2 test used for compar
Figure 2. Odds ratios (ORs) and 95% confidence intervalsfor all-cause inpatient mortality associated with weekend admis-sions (vs weekday admissions) in different subgroups. *ORs ofall-cause inpatient mortality are significantly different within sub-groups of hospitals by teaching status using generalized Haus-
man test (P � 0.006).Am J Kidney Dis. 2013;62(4):763-770
pendent of patient demographics, insurance status,comorbid conditions, admission diagnosis, and hospi-tal characteristics such as size, location, geographicalregion, and teaching status. We also found that theadjusted length of stay of survivors was longer andadjusted time to death was shorter for those admittedover weekends. To make the weekend and weekdaypopulation as homogeneous as possible, elective ad-missions were excluded because these usually arerestricted to weekdays. Similarly, primary dischargediagnoses common to maintenance dialysis patients,such as infections, dialysis access problems, cardiovas-cular diseases (including heart failure, acute coronarysyndrome, atrial fibrillation/flutter, and stroke), gastro-intestinal bleeding, and others (including hyperten-sive emergency and hyperkalemia) also were adjustedfor.
Previous studies have shown disparity in outcomes ofpatients admitted over weekends and weekdays1-6,11,12;however, the literature for outcomes of patients onmaintenance dialysis therapy admitted over weekendsis sparse. A recent study compared outcomes of pa-tients with acute kidney injury admitted over week-ends and weekdays, including patients needing dialy-sis.6 However, none of these patients were onmaintenance dialysis therapy. Similarly, Bell and Re-delmeier5 retrospectively examined 3.8 million acute-care admissions in Canada and determined that week-ends were associated with significantly highermortality for 23 of 100 leading causes of death.24-26 Intheir study, kidney failure was one of the 23 diagno-ses; however, the definition of kidney failure wasunclear and patients included may have had acutekidney injury, chronic kidney disease, or ESRD, asalso speculated by other authors.27 Further, this sub-
is Patients Admitted on Weekdays Versus Weekends
,081) Weekend (nb � 704,491) P
40,666 (5.8) �0.001
) 386,622 (54.9) �0.00118,137 (2.5) 0.6
154,724 (22.0) �0.00189,561 (12.7) 0.00614,345 (2.0) �0.001
436 (0.1) 0.1
4 [3-8] 0.001
6 [2-13] �0.001
e to death, which are given as median [interquartile range] fromey-weighted data used for comparison.
ialys
2,574
5.4)
55.7.6)1.5)3.0).7).1)
]
]
nd timg surv
group had fewer than 3,500 patients and mortality was
767
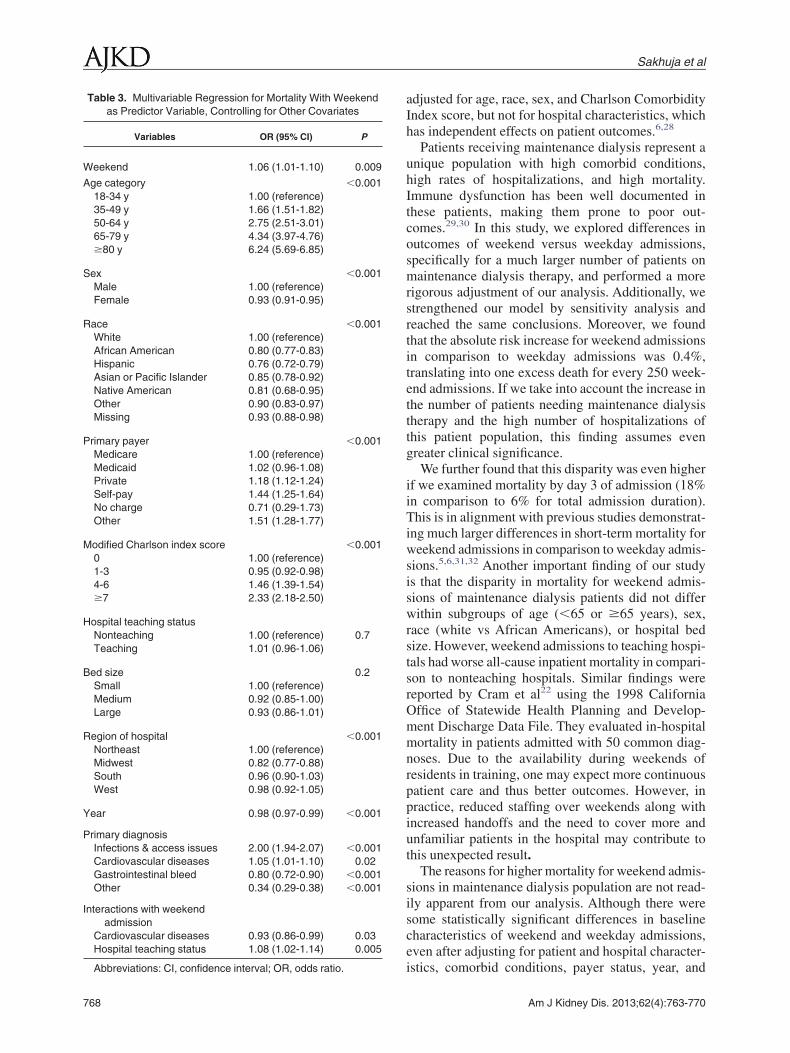
Abbreviations: CI, confidence interval; OR, odds ratio.
768
Sakhuja et al
adjusted for age, race, sex, and Charlson ComorbidityIndex score, but not for hospital characteristics, whichhas independent effects on patient outcomes.6,28
Patients receiving maintenance dialysis represent aunique population with high comorbid conditions,high rates of hospitalizations, and high mortality.Immune dysfunction has been well documented inthese patients, making them prone to poor out-comes.29,30 In this study, we explored differences inoutcomes of weekend versus weekday admissions,specifically for a much larger number of patients onmaintenance dialysis therapy, and performed a morerigorous adjustment of our analysis. Additionally, westrengthened our model by sensitivity analysis andreached the same conclusions. Moreover, we foundthat the absolute risk increase for weekend admissionsin comparison to weekday admissions was 0.4%,translating into one excess death for every 250 week-end admissions. If we take into account the increase inthe number of patients needing maintenance dialysistherapy and the high number of hospitalizations ofthis patient population, this finding assumes evengreater clinical significance.
We further found that this disparity was even higherif we examined mortality by day 3 of admission (18%in comparison to 6% for total admission duration).This is in alignment with previous studies demonstrat-ing much larger differences in short-term mortality forweekend admissions in comparison to weekday admis-sions.5,6,31,32 Another important finding of our studyis that the disparity in mortality for weekend admis-sions of maintenance dialysis patients did not differwithin subgroups of age (�65 or �65 years), sex,race (white vs African Americans), or hospital bedsize. However, weekend admissions to teaching hospi-tals had worse all-cause inpatient mortality in compari-son to nonteaching hospitals. Similar findings werereported by Cram et al22 using the 1998 CaliforniaOffice of Statewide Health Planning and Develop-ment Discharge Data File. They evaluated in-hospitalmortality in patients admitted with 50 common diag-noses. Due to the availability during weekends ofresidents in training, one may expect more continuouspatient care and thus better outcomes. However, inpractice, reduced staffing over weekends along withincreased handoffs and the need to cover more andunfamiliar patients in the hospital may contribute tothis unexpected result.
The reasons for higher mortality for weekend admis-sions in maintenance dialysis population are not read-ily apparent from our analysis. Although there weresome statistically significant differences in baselinecharacteristics of weekend and weekday admissions,even after adjusting for patient and hospital character-
Table 3. Multivariable Regression for Mortality With Weekendas Predictor Variable, Controlling for Other Covariates
Variables OR (95% CI) P
Weekend 1.06 (1.01-1.10) 0.009
Age category �0.00118-34 y 1.00 (reference)35-49 y 1.66 (1.51-1.82)50-64 y 2.75 (2.51-3.01)65-79 y 4.34 (3.97-4.76)�80 y 6.24 (5.69-6.85)
Sex �0.001Male 1.00 (reference)Female 0.93 (0.91-0.95)
Race �0.001White 1.00 (reference)African American 0.80 (0.77-0.83)Hispanic 0.76 (0.72-0.79)Asian or Pacific Islander 0.85 (0.78-0.92)Native American 0.81 (0.68-0.95)Other 0.90 (0.83-0.97)Missing 0.93 (0.88-0.98)
Primary payer �0.001Medicare 1.00 (reference)Medicaid 1.02 (0.96-1.08)Private 1.18 (1.12-1.24)Self-pay 1.44 (1.25-1.64)No charge 0.71 (0.29-1.73)Other 1.51 (1.28-1.77)
Modified Charlson index score �0.0010 1.00 (reference)1-3 0.95 (0.92-0.98)4-6 1.46 (1.39-1.54)�7 2.33 (2.18-2.50)
Hospital teaching statusNonteaching 1.00 (reference) 0.7Teaching 1.01 (0.96-1.06)
Bed size 0.2Small 1.00 (reference)Medium 0.92 (0.85-1.00)Large 0.93 (0.86-1.01)
Region of hospital �0.001Northeast 1.00 (reference)Midwest 0.82 (0.77-0.88)South 0.96 (0.90-1.03)West 0.98 (0.92-1.05)
Year 0.98 (0.97-0.99) �0.001
Primary diagnosisInfections & access issues 2.00 (1.94-2.07) �0.001Cardiovascular diseases 1.05 (1.01-1.10) 0.02Gastrointestinal bleed 0.80 (0.72-0.90) �0.001Other 0.34 (0.29-0.38) �0.001
Interactions with weekendadmission
Cardiovascular diseases 0.93 (0.86-0.99) 0.03Hospital teaching status 1.08 (1.02-1.14) 0.005
istics, comorbid conditions, payer status, year, and
Am J Kidney Dis. 2013;62(4):763-770

Weekend Maintenance Dialysis Admissions
primary discharge diagnoses common to maintenancedialysis patients, higher mortality for weekend admis-sions persisted. There are some unique in-hospitalcircumstances that likely affect patients on mainte-nance dialysis therapy more than other groups. Theweekends usually have fewer available staff and re-sources and, depending on the structure of the hospitalstaff working over weekends, may not be familiarwith patients and may be less experienced. Decreasednurse staffing has been shown to be associated withworse outcomes.33,34 In addition, many long-termcare facilities do not admit patients on weekends, thusstretching the already scant available resources overweekends in hospitals.
Although we have used a database with representa-tive sample, our study has some limitations. We usedICD-9-CM codes for ESRD, dialysis, and acute kid-ney injury to identify our study population. Althoughdialysis and acute kidney injury codes have been usedpreviously, the ICD-9-CM codes for ESRD have notbeen validated.35 However, the same inclusion algo-rithm has been used in the literature before.15 Addition-ally, coding may vary among different hospitals andcoding errors may have resulted in some degree ofselection bias. However, we believe that such codingpractices are unlikely to differ between weekdays andweekends. We classified weekend admissions as thoseoccurring from midnight Friday to midnight Sunday.This does not take into account that health careservices on Friday evenings, early mornings on Mon-days, and holidays likely are similar to those providedover weekends. We therefore may have underesti-mated the worse outcomes over weekends. Becausemaintenance dialysis facilities are open on Saturdays,there may be a difference in outcomes of Saturday andSunday admissions. However, we were unable todifferentiate between Saturday and Sunday admis-sions. Further, despite multivariable adjustment, wecannot exclude other unmeasured confounding fac-tors that may have influenced our results. Addition-ally, we were not able to determine whether thepatients being admitted came from home or anotherhealth care facility. The database does not provideunique patient identifiers; therefore, it is not possibleto accurately distinguish readmissions of the samepatient. However, using patient characteristics, pri-mary payer, hospital ID, and year of admission, weattempted to identify duplicate observations and per-formed 4 different sensitivity analyses based on thedifferent ways of selecting unique observations, withcontinued robustness of our results.
In summary, this study, which included a represen-tative sample of nonelective inpatient admissions,provides evidence of worse outcomes for mainte-
nance dialysis patients who were admitted over week-Am J Kidney Dis. 2013;62(4):763-770
ends. Future studies are needed to explore reasons thatmight explain such findings and consider strategies tostrengthen staffing and resources over weekends thatmight improve the quality of health care delivery formaintenance dialysis patients.
ACKNOWLEDGEMENTSSupport: This publication was made possible by grant RR024990
(Dr Navaneethan) from the National Center for Research Re-sources (NCRR), a component of the National Institutes of Health(NIH), and NIH Roadmap for Medical Research. Dr Schold issupported by the NIH/National Institute of Diabetes and Digestiveand Kidney Diseases (R01 DK085185) and investigator-initiatedgrant support from The PhRMA Foundation, Genzyme, and RocheOrgan Transplant Research Foundation. Its contents are solely theresponsibility of the authors and do not necessarily represent theofficial view of the NCRR or NIH.
Financial Disclosure: The authors declare that they have noother relevant financial interests.
SUPPLEMENTARY MATERIALTable S1: ICD-9-CM codes for primary discharge diagnosis.Table S2: Sensitivity analyses and effect on various outcomes.Note: The supplementary material accompanying this article
(http://dx.doi.org/10.1053/j.ajkd.2013.03.014) is available atwww.ajkd.org.
REFERENCES1. Magid DJ, Wang Y, Herrin J, et al. Relationship between
time of day, day of week, timeliness of reperfusion, and in-hospitalmortality for patients with acute ST-segment elevation myocardialinfarction. JAMA. 2005;294(7):803-812.
2. Saposnik G, Baibergenova A, Bayer N, Hachinski V. Week-ends: a dangerous time for having a stroke? Stroke. 2007;38(4):1211-1215.
3. Crowley RW, Yeoh HK, Stukenborg GJ, Medel R, KassellNF, Dumont AS. Influence of weekend hospital admission onshort-term mortality after intracerebral hemorrhage. Stroke. 2009;40(7):2387-2392.
4. Shaheen AA, Kaplan GG, Myers RP. Weekend versus week-day admission and mortality from gastrointestinal hemorrhagecaused by peptic ulcer disease. Clin Gastroenterol Hepatol. 2009;7(3):303-310.
5. Bell CM, Redelmeier DA. Mortality among patients admit-ted to hospitals on weekends as compared with weekdays. N EnglJ Med. 2001;345(9):663-668.
6. James MT, Wald R, Bell CM, et al. Weekend hospitaladmission, acute kidney injury, and mortality. J Am Soc Nephrol.2010;21(5):845-851.
7. Gilbertson DT, Liu J, Xue JL, et al. Projecting the number ofpatients with end-stage renal disease in the United States to theyear 2015. J Am Soc Nephrol. 2005;16(12):3736-3741.
8. Collins AJ, Foley RN, Herzog C, et al. US Renal DataSystem 2012 annual data report. Am J Kidney Dis. 2013;61(1)(suppl 1):e1-e480.
9. Introduction to the HCUP Nationwide Inpatient Sample 2010.http://www.hcup-us.ahrq.gov/db/nation/nis/NISIntroduction2010.pdf. Accessed January 5, 2013.
10. Waikar SS, Wald R, Chertow GM, et al. Validity of Interna-tional Classification of Diseases, Ninth Revision, Clinical Modifi-cation codes for acute renal failure. J Am Soc Nephrol. 2006;17(6):
1688-1694.769

Sakhuja et al
11. Ananthakrishnan AN, McGinley EL, Saeian K. Outcomesof weekend admissions for upper gastrointestinal hemorrhage: anationwide analysis. Clin Gastroenterol Hepatol. 2009;7(3):296-302, e291.
12. Aujesky D, Jimenez D, Mor MK, Geng M, Fine MJ,Ibrahim SA. Weekend versus weekday admission and mortalityafter acute pulmonary embolism. Circulation. 2009;119(7):962-968.
13. Crowley RW, Yeoh HK, Stukenborg GJ, Ionescu AA,Kassell NF, Dumont AS. Influence of weekend versus weekdayhospital admission on mortality following subarachnoid hemor-rhage. Clinical article. J Neurosurg. 2009;111(1):60-66.
14. Deyo RA, Cherkin DC, Ciol MA. Adapting a clinicalcomorbidity index for use with ICD-9-CM administrative data-bases. J Clin Epidemiol. 1992;45(6):613-619.
15. Kumar G, Sakhuja A, Taneja A, et al. Pulmonary embolismin patients with CKD and ESRD. Clin J Am Soc Nephrol. 2012;7(10):1584-1590.
16. svy postestimation—postestimation tools for svy. SurveyData Reference Manual Release 11. College Station, TX: StataPress; 2009:101-105.
17. Kim HM, Eisenberg D, Ganoczy D, et al. Examining therelationship between clinical monitoring and suicide risk amongpatients with depression: matched case-control study and instrumen-tal variable approaches. Health Serv Res. 2010;45(5, pt 1):1205-1226.
18. Gallerani M, Boari B, Manfredini F, Mari E, Maraldi C,Manfredini R. Weekend versus weekday hospital admissions foracute heart failure. Int J Cardiol. 2011;146(3):444-447.
19. Horwich TB, Hernandez AF, Liang L, et al. Weekendhospital admission and discharge for heart failure: association withquality of care and clinical outcomes. Am Heart J. 2009;158(3):451-458.
20. Kostis WJ, Demissie K, Marcella SW, Shao YH, WilsonAC, Moreyra AE. Weekend versus weekday admission and mortal-ity from myocardial infarction. N Engl J Med. 2007;356(11):1099-1109.
21. Deshmukh A, Pant S, Kumar G, Bursac Z, Paydak H,Mehta JL. Comparison of outcomes of weekend versus weekdayadmissions for atrial fibrillation. Am J Cardiol. 2012;110(2):208-211.
22. Cram P, Hillis SL, Barnett M, Rosenthal GE. Effects ofweekend admission and hospital teaching status on in-hospital
mortality. Am J Med. 2004;117(3):151-157.770
23. Chung L, Krishnan E, Chakravarty EF. Hospitalizations andmortality in systemic sclerosis: results from the Nationwide Inpa-tient Sample. Rheumatology (Oxford). 2007;46(12):1808-1813.
24. Ensminger SA, Morales IJ, Peters SG, et al. The hospitalmortality of patients admitted to the ICU on weekends. Chest.2004;126(4):1292-1298.
25. Laupland KB, Shahpori R, Kirkpatrick AW, Stelfox HT.Hospital mortality among adults admitted to and discharged fromintensive care on weekends and evenings. J Crit Care. 2008;23(3):317-324.
26. Barnett MJ, Kaboli PJ, Sirio CA, Rosenthal GE. Day of theweek of intensive care admission and patient outcomes: a multisiteregional evaluation. Med Care. 2002;40(6):530-539.
27. Halm EA, Chassin MR. Why do hospital death rates vary?N Engl J Med. 2001;345(9):692-694.
28. Ananthakrishnan AN, McGinley EL, Saeian K. Higherhospital volume is associated with lower mortality in acute non-variceal upper-GI hemorrhage. Gastrointest Endosc. 2009;70(3):422-432.
29. Hauser AB, Stinghen AE, Kato S, et al. Characteristics andcauses of immune dysfunction related to uremia and dialysis. PeritDial Int. 2008;28(suppl 3):S183-S187.
30. Kato S, Chmielewski M, Honda H, et al. Aspects of immunedysfunction in end-stage renal disease. Clin J Am Soc Nephrol.2008;3(5):1526-1533.
31. Marco J, Barba R, Plaza S, Losa JE, Canora J, Zapatero A.Analysis of the mortality of patients admitted to internal medicinewards over the weekend. Am J Med Qual. 2010;25(4):312-318.
32. Barba R, Losa JE, Velasco M, Guijarro C, Garcia deCasasola G, Zapatero A. Mortality among adult patients admittedto the hospital on weekends. Eur J Intern Med. 2006;17(5):322-324.
33. Needleman J, Buerhaus P, Mattke S, Stewart M, ZelevinskyK. Nurse-staffing levels and the quality of care in hospitals. N EnglJ Med. 2002;346(22):1715-1722.
34. Sasichay-Akkadechanunt T, Scalzi CC, Jawad AF. Therelationship between nurse staffing and patient outcomes. J NursAdm. 2003;33(9):478-485.
35. Parikh DS, Swaminathan M, Archer LE, et al. Perioperativeoutcomes among patients with end-stage renal disease followingcoronary artery bypass surgery in the USA. Nephrol Dial Trans-
plant. 2010;25(7):2275-2283.Am J Kidney Dis. 2013;62(4):763-770
Recommended

















