Prophylactic Laser Treatment to Fellow Eyesof Unilateral Retinal Pigment Epithelial Tears
MIRJAM GROSS-JENDROSKA, MD, SARAH L. OWENS, MD, CHRIS J. FLAXEL, MD,ROBYN H. GUYMER, MD, PHD, AND ALAN C. BIRD, MD
● PURPOSE: To evaluate prophylactic laser treat-ment of the macula in reducing the risk of visualloss in the fellow eye of patients with a retinalpigment epithelial tear caused by age-related mac-ular degeneration in the first eye.● METHODS: In a prospective study, 12 patientswith a retinal pigment epithelial tear in one eyecaused by age-related macular degeneration anddrusen in the fellow eye received prophylacticlaser treatment of the retina in their fellow eyesand were followed up for 2 years or more afterprophylactic treatment.● RESULTS: In 12 fellow eyes that received pro-phylactic laser treatment, a reduction in best-corrected visual acuity to 20/80 or worse occurredin one (8%) of 12 eyes in the first year and two(18%) of the remaining 11 eyes in the second yearafter treatment. The cumulative risk of visual lossin the treated fellow eye was 25% in 2 years.● CONCLUSIONS: In historical control subjects in anatural history study of patients with retinal pig-ment epithelial tear in one eye, central visual lossoccurred in 16 (37%) of 43 eyes in the first yearand in seven (30%) of 23 eyes in the second yearfor a cumulative loss of 59% in the first 2 years.Compared with these historical control subjects,our findings suggest that visual loss in the felloweyes of patients with a retinal pigment epithelialtear in the first eye is reduced by prophylactic low
intensity laser photocoagulation of the macula.(Am J Ophthalmol 1998;126:77–81. © 1998 byElsevier Science Inc. All rights reserved.)
I N AGE-RELATED MACULAR DEGENERATION, CEN-
tral vision can be lost because of choroidal neo-vascularization, retinal pigment epithelial de-
tachment, or geographic atrophy. Pigmentepithelial detachments leading to tears have anespecially poor visual prognosis, and patients withthis condition have a particularly high risk ofdeveloping a visual loss in the fellow eye. In a studyof 43 patients with a retinal pigment epithelial tearin one eye, Schoeppner and associates1 reported therisk of central visual loss caused by complications ofage-related macular degeneration in the fellow eye.All patients had an initial visual acuity of 20/40 orbetter in the fellow eye, with loss of vision beingdefined as a reduction of best-corrected visual acuityto 20/80 or worse. Loss of vision occurred in 16(37%) of 43 patients in the first year, seven (30%)of 23 patients in the second year, and eight (50%)of 16 patients in the third year. The cumulative lossof visual acuity was 37% in 1 year, 59% in 2 years,and 80% in 3 years.1
It is believed that retinal pigment epithelialdetachments are caused by reduction of hydraulicconductivity of a thickened Bruch membrane, thusimpeding the outward movement of fluid from theretinal pigment epithelium towards the choroid.2,3
A tear may occur at the edge of the detachmentwhen the tangential stress becomes great enough torupture the detached tissue.4,5 It follows that inthese cases, the impedance to flow would be thegreatest, which is emphasized by the finding that therisk to the second eye is a detachment of the retinal
Accepted for publication Oct 21, 1997.From the Department of Clinical Ophthalmology, Institute of Oph-
thalmology, University of London, Moorfields Eye Hospital, London,United Kingdom (Drs Gross-Jendroska, Owens, Flaxel, Guymer, andBird); and Augenklinik, Klinikum Benjamin Franklin, Free Universityof Berlin, Berlin, Germany (Dr Gross-Jendroska).
Reprint requests to Alan C. Bird, MD, Professorial Unit, MoorfieldsEye Hospital, City Road, London EC1V 2PD, UK; fax: 44-171-2519350; e-mail: [email protected]
© 1998 BY ELSEVIER SCIENCE INC. ALL RIGHTS RESERVED.0002-9394/98/$19.00 77PII S0002-9394(98)00061-0

pigment epithelium that may or may not tear1,6 andcould explain the poor visual outcome. The lack ofeffective treatment for such lesions makes an effec-tive prophylaxis desirable.4,5,7–11
Prophylaxis in age-related macular disease hasbeen reported previously. Several authors havereported a reduction in the number and size ofdrusen after low-intensity photocoagulation ineyes with age-related maculopathy. In 1971,Gass12 was the first to suggest prophylactic lasertreatment for patients with asymptomatic pig-ment epithelial detachments in an attempt totack down the retinal pigment epithelium. Later,he notes the disappearance of drusen in patientstreated for choroidal neovascularization.13 Cleasby andassociates14 were the first to conduct a prospectivetrial of prophylactic photocoagulation in patientswith either bilateral drusen or a disciform lesion inone eye and with drusen in the fellow eye. Theyfound a reduction in the amount of drusen in thetreated group vs the untreated control group. Ofpatients with unilateral disciform lesions, only 4.4%per year developed exudative lesions in the treatedsecond eye. Other investigators have made similarobservations.15–18 The most convincing evidence oftherapeutic effect is from the work of Frennessonand Nilsson,19 who showed in a controlled trial thatthe area occupied by drusen decreased significantlyafter photocoagulation; however, they did not iden-tify a change in central visual acuity as a result ofphotocoagulation.
To lower the risk of central visual loss in thefellow eye of patients with retinal pigment epithelialtear caused by age-related macular degeneration inthe first eye and a particularly poor visual prognosis,we placed low-intensity laser spots in the macularregion of the fellow eye.
PATIENTS AND METHODS
WE PROSPECTIVELY STUDIED 12 PATIENTS WITH AGE-
related macular degeneration who presented with aretinal pigment epithelial tear in one eye and drusenin the fellow eye. The mean patient age was 76 years(range, 62 to 86 years), and there were 10 womenand two men. The initial mean best-corrected visual
acuity of the fellow eye was 20/30 (range, 20/20 to20/40). On fluorescein angiography of the felloweye, four patients showed hypofluorescent drusen(Patients 4, 5, and 8), two patients had delayedchoroidal filling (Patients 8 and 9), three showedhyperpigmentation (Patients 1, 2, and 9), and twohad shallow pigment epithelial detachments with-out signs of occult or well-defined choroidal neovas-cularization on fluorescein angiography (Patients 6and 7; Table).
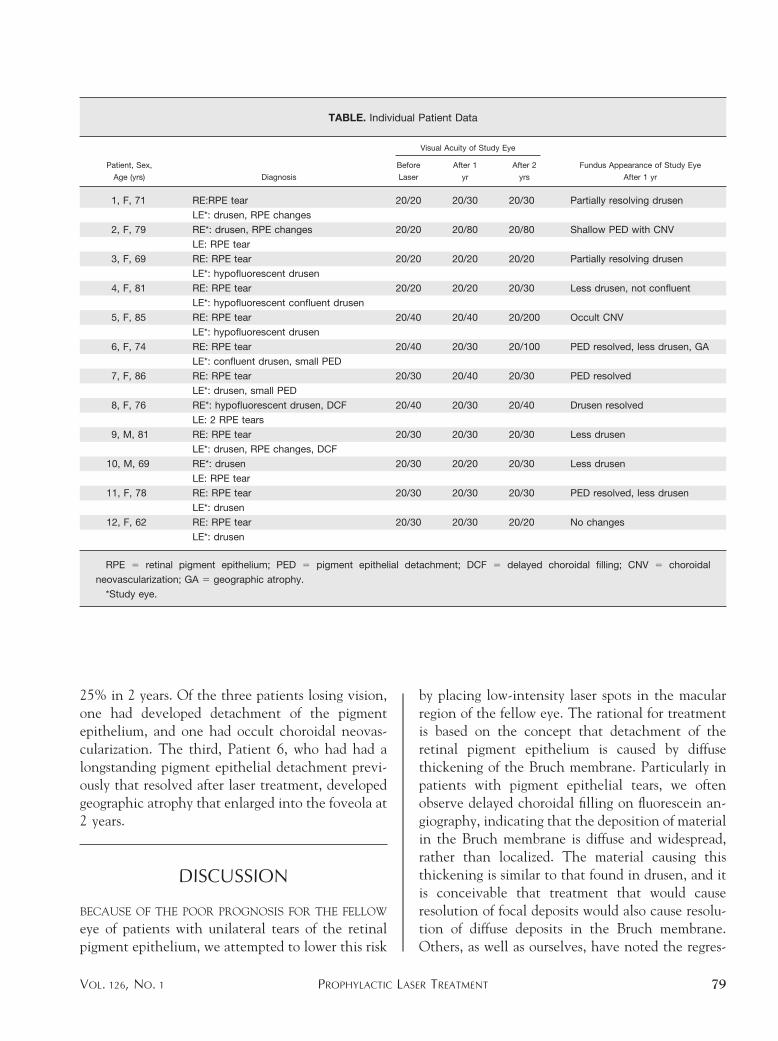
After the patients gave informed consent, photo-coagulation of the fellow eye was carried out withthe argon green or yellow dye laser. All patientsreceived laser treatment consisting of 12 burns at0.2 second and 200 mm size. The lowest possibleintensity for achieving a faint whitening of theneurosensory retina was used, usually between 80 to120 mW. The spots were placed between 600 and1,000 mm in a circle around the foveola (Figure).All patients were monitored at regular intervals.Visual loss was defined as the reduction of best-corrected visual acuity to 20/80 or worse.
RESULTS
AFTER WE PERFORMED PROPHYLACTIC LASER TREAT-
ment on 12 fellow eyes of eyes with retinal pigmentepithelial tears caused by age-related macular de-generation, we retreated Patient 4 after 14 monthsand Patient 11 after 4 months because the appear-ance of their large confluent drusen had notchanged. Patient 8 had received relatively intenselaser treatment initially. After 4 months, her drusenhad completely disappeared, but she had developedchoroidal neovascularization at one laser scar withdistortion of vision. As she declined further lasertreatment, the lesion was only observed. Twomonths later, evidence of choroidal neovasculariza-tion had disappeared on fluorescein angiography,and visual acuity had improved slightly 1 year aftertreatment.
All 12 patients were followed up for 2 years. Ofthe 12 patients, one (8%) had a reduced visualacuity of 20/80 in the fellow eye at 1 year. In thesecond year, two (18%) of 11 patients had reducedvisual acuity at 14 and 18 months. The cumulativerisk of visual loss to the fellow eye was, therefore,
AMERICAN JOURNAL OF OPHTHALMOLOGY78 JULY 1998
25% in 2 years. Of the three patients losing vision,one had developed detachment of the pigmentepithelium, and one had occult choroidal neovas-cularization. The third, Patient 6, who had had alongstanding pigment epithelial detachment previ-ously that resolved after laser treatment, developedgeographic atrophy that enlarged into the foveola at2 years.
DISCUSSION
BECAUSE OF THE POOR PROGNOSIS FOR THE FELLOW
eye of patients with unilateral tears of the retinalpigment epithelium, we attempted to lower this risk
by placing low-intensity laser spots in the macularregion of the fellow eye. The rational for treatmentis based on the concept that detachment of theretinal pigment epithelium is caused by diffusethickening of the Bruch membrane. Particularly inpatients with pigment epithelial tears, we oftenobserve delayed choroidal filling on fluorescein an-giography, indicating that the deposition of materialin the Bruch membrane is diffuse and widespread,rather than localized. The material causing thisthickening is similar to that found in drusen, and itis conceivable that treatment that would causeresolution of focal deposits would also cause resolu-tion of diffuse deposits in the Bruch membrane.Others, as well as ourselves, have noted the regres-
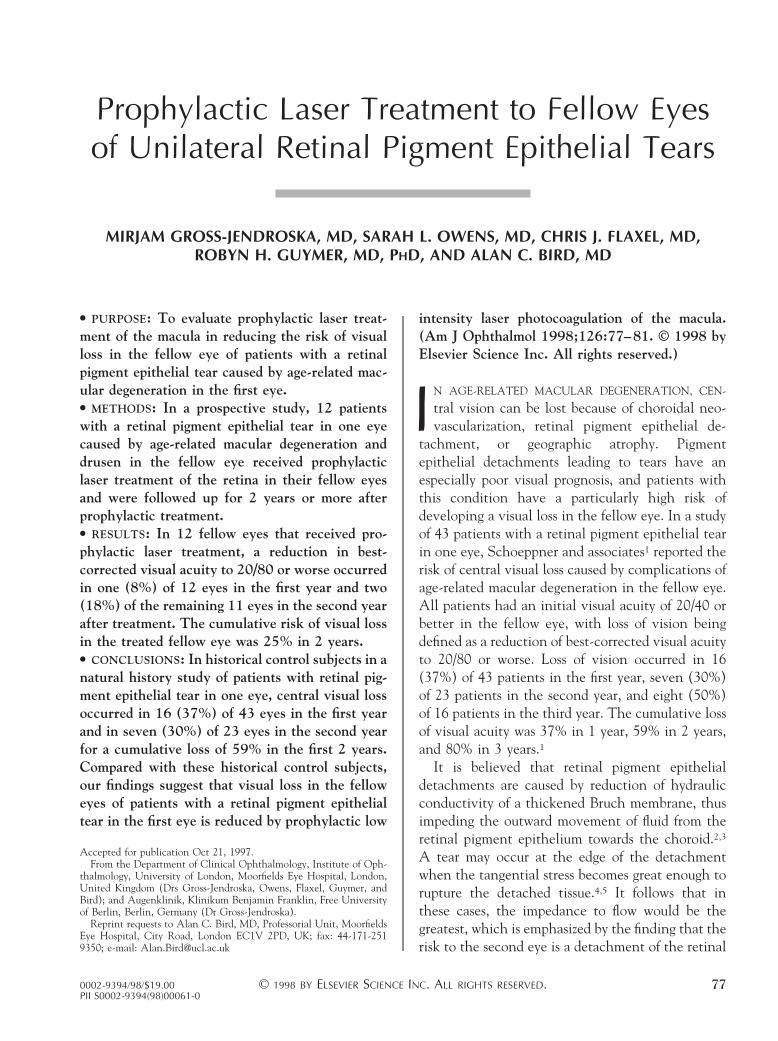
TABLE. Individual Patient Data
Patient, Sex,
Age (yrs) Diagnosis
Visual Acuity of Study Eye
Fundus Appearance of Study Eye
After 1 yr
Before
Laser
After 1
yr
After 2
yrs
1, F, 71 RE:RPE tear 20/20 20/30 20/30 Partially resolving drusen
LE*: drusen, RPE changes
2, F, 79 RE*: drusen, RPE changes 20/20 20/80 20/80 Shallow PED with CNV
LE: RPE tear
3, F, 69 RE: RPE tear 20/20 20/20 20/20 Partially resolving drusen
LE*: hypofluorescent drusen
4, F, 81 RE: RPE tear 20/20 20/20 20/30 Less drusen, not confluent
LE*: hypofluorescent confluent drusen
5, F, 85 RE: RPE tear 20/40 20/40 20/200 Occult CNV
LE*: hypofluorescent drusen
6, F, 74 RE: RPE tear 20/40 20/30 20/100 PED resolved, less drusen, GA
LE*: confluent drusen, small PED
7, F, 86 RE: RPE tear 20/30 20/40 20/30 PED resolved
LE*: drusen, small PED
8, F, 76 RE*: hypofluorescent drusen, DCF 20/40 20/30 20/40 Drusen resolved
LE: 2 RPE tears
9, M, 81 RE: RPE tear 20/30 20/30 20/30 Less drusen
LE*: drusen, RPE changes, DCF
10, M, 69 RE*: drusen 20/30 20/20 20/30 Less drusen
LE: RPE tear
11, F, 78 RE: RPE tear 20/30 20/30 20/30 PED resolved, less drusen
LE*: drusen
12, F, 62 RE: RPE tear 20/30 20/30 20/20 No changes
LE*: drusen
RPE 5 retinal pigment epithelium; PED 5 pigment epithelial detachment; DCF 5 delayed choroidal filling; CNV 5 choroidal
neovascularization; GA 5 geographic atrophy.
*Study eye.
PROPHYLACTIC LASER TREATMENTVOL. 126, NO. 1 79
sion of drusen far away from the laser scars, suggest-ing a widespread effect rather than a local reac-tion.15,17,18 We believe that the effect ofprophylactic treatment in reducing the risk of visualloss can work only by initiating a widespread changein this system of deposition and removal of material.
The mechanism of resorption of drusen is uncer-tain. It was concluded from a study on monkeys thatphotocoagulation was followed by invasion of theBruch membrane by macrophages that led to regres-sion of drusen.20 This is a local phenomenon, butthe drusen resolve in areas distant from the photo-coagulation. Alternatively, laser treatment couldlead to a partial destruction of debris deposited inthe Bruch membrane, thereby increasing its hydrau-lic conductivity.21 Additionally, a reduction in thenumber of retinal pigment epithelial cells could leadto a decrease in the production of material depositedinto the Bruch membrane.
The number of patients enrolled in this study wassmall, and there were no control patients. However,with the risk for visual loss of the fellow eye beingreduced from 37% (in historical control subjects) to8% in the first year and from 59% (in historicalcontrol subjects) to 25% in the second year, in this
pilot study, we believe that for this subset ofage-related macular degeneration, low-intensity la-ser photocoagulation of the posterior pole may bewarranted. Admittedly, the experience of a con-trolled trial would be needed to draw firm conclu-sions, but tears of the retinal pigment epithelium areuncommon, and a trial may be impracticable.
REFERENCES
1. Schoeppner G, Chuang EL, Bird AC. The risk of fellow eyevisual loss with unilateral retinal pigment epithelial tears.Am J Ophthalmol 1989;108:683–685.
2. Bird AC, Marshall J. Retinal pigment epithelial detach-ments in the elderly. Trans Ophthalmol Soc UK 1986;105:674–682.
3 Moore DJ, Hussain AA, Marshall J. Age-related variation inthe hydraulic conductivity of Bruch’s membrane. InvestOphthalmol Vis Sci 1995;36:1290–1297.
4. Gass JDM. Serous retinal pigment epithelial detachmentwith a notch. Retina 1984;4:205–220.
5. Bird AC. Doyne lecture: pathogenesis of retinal pigmentepithelial detachment in the elderly; the relevance ofBruch’s membrane change. Eye 1991;5:1–12.
6. Chuang EL, Bird AC. Bilaterality of tears of the retinalpigment epithelium. Br J Ophthalmol 1988;72:417.
7. Moorfields Macular Study Group. Retinal pigment epithe-lial detachments in the elderly: a controlled trial of argonlaser photocoagulation. Br J Ophthalmol 1982;66:1–16.
8. Chisholm IH. The recurrence of neovascularization andlate failure in senile disciform lesions. Trans OphthalmolSoc UK 1983;103:354–359.
9. Macular Photocoagulation Group. Argon laser photocoag-ulation for neovascular maculopathy: three year results forrandomized clinical trials. Arch Ophthalmol 1986;224:493–501.
10. Maguire JI, Benson WE, Brown GC. Treatment of fovealpigment epithelial detachments with contiguous extrafo-veal choroidal neovascular membranes. Am J Ophthalmol1990;109:523–529.
11. Yannuzzi LA, Slalkter JS, Sorensen JA, Guyer DR, OrlockDA. Digital indocyanine green videoangiography and cho-roidal angiography. Retina 1992;12:191–223.
12. Gass JMD. Photocoagulation of macular lesions. Trans AmAcad Ophthalmol Otolaryngol 1971;75:580–608.
13. Gass JMD. Drusen and disciform macular detachment anddegeneration. Arch Ophthalmol 1973;90:206–217.
14. Cleasby GW, Nakanishi AS, Norris JL. Prophylactic pho-tocoagulation of the fellow eye in exudative senile macu-lopathy. A preliminary report. Mod Probl Ophthalmol1979;20:141–147.
15. Wetzig PC. Treatment of drusen-related ageing maculardegeneration by photocoagulation. Trans Am OphthalmolSoc 1988;86:276–290.
16. Haut J, Renard Y, Kraiem S, Bensoussan C, Moulin F.Preventive treatment using laser of age-related maculardegeneration of the contralateral eye after age-relatedmacular degeneration in the first eye. J Fr Ophthalmol1991;14:473–476.
FIGURE. Fundus photograph of a macula with drusenillustrating the pattern of photocoagulation therapy.Twelve burns were placed between 600 and 1,000 mmin a circle around the foveola (diagrammatically illus-trated by black dots).
AMERICAN JOURNAL OF OPHTHALMOLOGY80 JULY 1998

17. Sigelman J. Foveal drusen resorption one year after perifo-veal laser photocoagulation. Ophthalmology 1991;98:1379–1383.
18. Figueroa MS, Regueras A, Bertrand J. Laser photocoagula-tion to treat macular soft drusen in age-related maculardegeneration. Retina 1994;14:391–396.
19. Frennesson IC, Nilsson SEG. Effects of argon (green) lasertreatment of soft drusen in early age-related maculopathy: a
6 months’ prospective study. Br J Ophthalmol 1995;79:905–909.
20. Duvall J, Tso MOM. Cellular mechanisms of resolution ofdrusen after laser coagulation: an experimental study. ArchOphthalmol 1985;103:694–703.
21. Bird AC. Treatment of pigment epithelial detachmentsin the elderly patient. Current Opin Ophthalmol 1993;4:25–32.
Authors InteractivetWe encourage questions and comments regarding this article via theInternet on Authors Interactivet at http://www.ajo.com/ Questions, com-ments, and author responses are posted.
PROPHYLACTIC LASER TREATMENTVOL. 126, NO. 1 81
Recommended