Pulmonary Nodules
Matt LandmanResident in Research
Faculty Facilitator – Dr. Eric Grogan
Resident Teaching Conferences - 2010
• Goal is to have a broad-based curriculum and hopefully not just another conference
• Want you to learn something• Mainly case-based with faculty facilitators• Supplemental materials available• SCORE – weekly email reminders
– Weekly questions based on that weeks reading– May or may not relate to RTC
• After January ABSITE review, moving upstairs in Light Hall
www.nccn.org

Fall 2010 Resident Teaching ConferencesSeptember 24, 2010 No Grand Rounds VMS Oral Exams RTC/Skills Labs only
October 1, 2010 title TBA Dr. Addison May Thoracic Trauma
October 8, 2010 title TBA Dr. John Morris, Jr. Hand Lecture
October 15, 2010 title TBA Dr. Jose Diaz Adrenal Masses
October 22, 2010
L.W. Edwards Lecture
“Toward Better Strategies for Improving
Surgical Quality”
Dr. John D. Birkmeyer,
University of Michigan Rocking Chair Conference
October, 29, 2010
Holcomb Lecture title TBA Dr. Brad Warner Pediatric Surgery Case Presentations
November 5, 2010 title TBA Dr. Bryan Collier Disclosure Training - Guillamondegui
November 12, 2010 title TBA
Frederick A. Moore, MD
Chief, General Surgery
Head, Division of Surgical Critical
Care & Acute Care Surgery
The Methodist Hospital
Houston, TX Trauma/EGS Case Presentations
November 19, 2010
Rollin Daniel Lecture Rollin Daniel lecture Rollin Daniel lecture Cardiothoracic Case Presentations
November 26, 2010 No Grand Rounds Thanksgiving Holiday NO RTC
December 3, 2010 MPMMIC Research Meeting
December 10, 2010
title TBA John Alverdy MD FACS
open
December 17, 2010 No Grand Rounds VMS Oral Exams RTC/Skills Labs only
December 24, 2010 No Grand Rounds Christmas Break
NO RTC
December 31, 2010 No Grand Rounds New Year's Eve
NO RTC
Objectives
• Brief intro to lung cancer and screening programs
• Work-up of a pulmonary nodule
– Understand risk of cancer given nodule/patient characteristics
– How long do you follow a nodule? Who get’s additional imaging? Timing of imaging?
– Understand additional work-up and treatment for lung malignancy
How might this appear on the Oral Boards?
• “In a routine pre-op chest x-ray, a 59 year-old smoker was found to have a RUL 3cm pulmonary nodule.”
• What do you do?– Work-up
– Pre-op work-up
– Staging
– Operative considerations
– Post-op treatment
http://articles.cnn.com/2010-05-31/world/indonesia.smoking.baby_1_aldi-anti-smoking-measures-smoke?_s=PM:WORLD
Lung Cancer 101
• Most common cause of cancer deaths in the U.S. – male and female
• 80% - Non-small cell lung cancer
– Adenocarcinoma, SCC, large cell
• Of all presenting with cancer – only 20% surgically resectable
• Stage I with complete surgical resection 70% 5-year survival
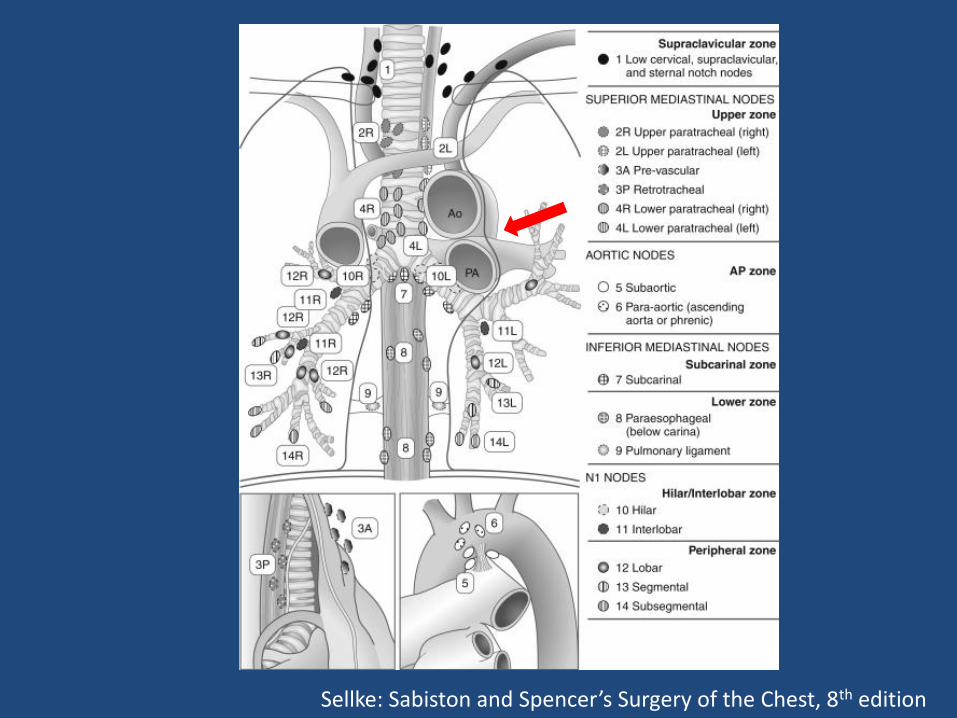
Sellke: Sabiston and Spencer’s Surgery of the Chest, 8th edition
Lung cancer screening programs result in discovery of earlier cancers than the
standard diagnostic methods?
1 2
0%0%
1. True
2. False
Lung cancer screening projects have been shown to decrease lung cancer-related mortality but are prohibitive
due to cost.
1 2
0%0%
1. True
2. False
Lung Cancer Screening
• 1960-1964 – London
– 55K males followed 3 years
• CXR (q3m) vs. CXR at T0 and at 3 years
– Screened – found more cancer, increased resectability
– No difference in lung-cancer related mortality
• 1970s – 3 studies using CXR & sputum cytology
– No differences in lung cancers found and lung-cancer-related mortality
• Low-dose CT scan screening programs– No differences in cancer-related mortality
• Ongoing screening trials
• Other screening methods– Additional sputum evaluation techniques
– Molecular techniques for circulating tumor cells
– Fluorescence bronchoscopy
• Still controversial – most moving to CT scans vs. CXR given sensitivity and specificity
Lung Cancer Screening
Solitary Pulmonary Nodule
• Big question – malignant or not?• Large majority are benign (~80%)• Nodule characteristics predicting malignancy
– Nodule size - #1– Change in nodule size on repeat imaging– Nodule borders (ex. Smooth vs. spiculated)– Solitary vs. multiple nodules– Solid vs. non-solid
• Patient characteristics predicting malignancy– Smoking (# of cigs/day as well as # of years)– Age– Occupational exposures (asbestos, radon, etc.)
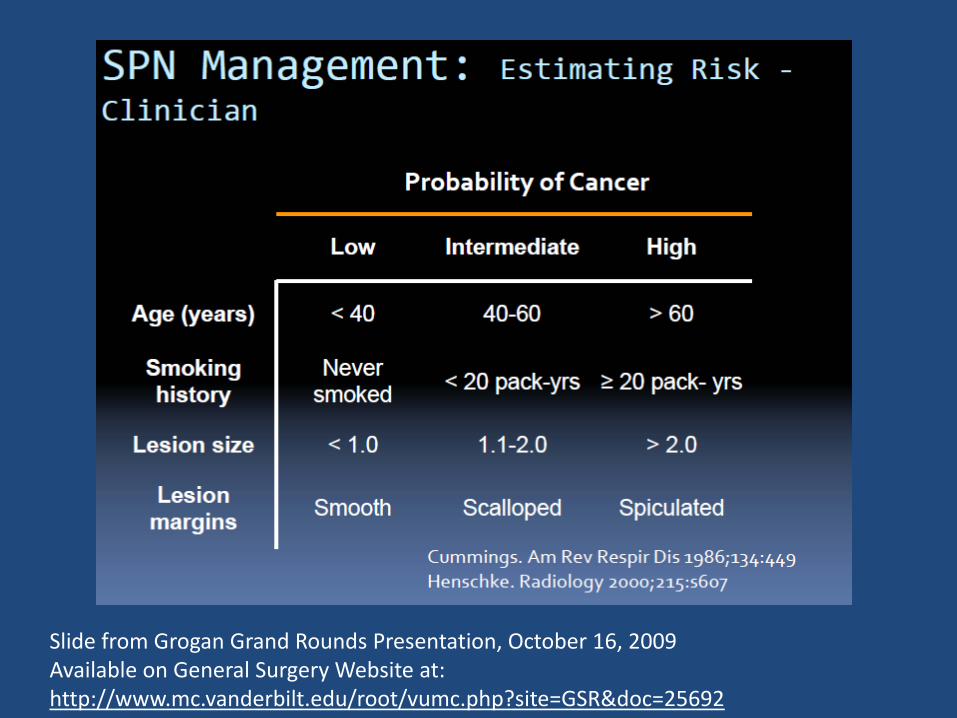
Slide from Grogan Grand Rounds Presentation, October 16, 2009 Available on General Surgery Website at: http://www.mc.vanderbilt.edu/root/vumc.php?site=GSR&doc=25692
Solitary Pulmonary Nodule – Work Up
• History & Physical– Noting cancer, infection risk factors
– Other symptoms, paraneoplastic symptoms
• Old Imaging Baseline Chest CT and upper abdomen
• Nodule Size and repeat imaging
• Concerning Mediastinal/cervical nodes PET/CT and biopsy
• Biopsy (nodule and mediastinum) vs. surgical removal of nodule with mediastinal lymph node dissection/sampling
Imaging
• Limits of detection
– CXR – 7 – 10mm
– CT – < 5 mm
– PET – 1.0 – 1.2 cm
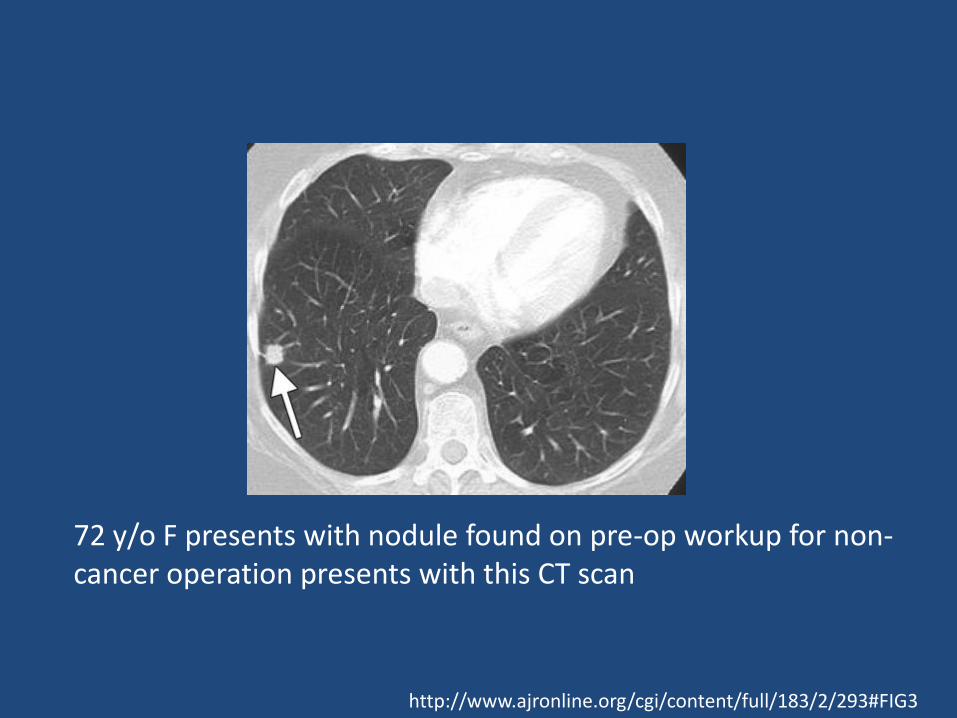
72 y/o F presents with nodule found on pre-op workup for non-cancer operation presents with this CT scan
http://www.ajronline.org/cgi/content/full/183/2/293#FIG3
Solitary Pulmonary Nodules
• <5mm repeat imaging in 12 months
• > 5 – 15 mm repeat imaging in 3 months
– Solid higher risk for cancer than non-solid lesions
• >15mm Early follow up (infectious concerns 1 month) vs. Biopsy
– Patient risk factors may play a role in decision
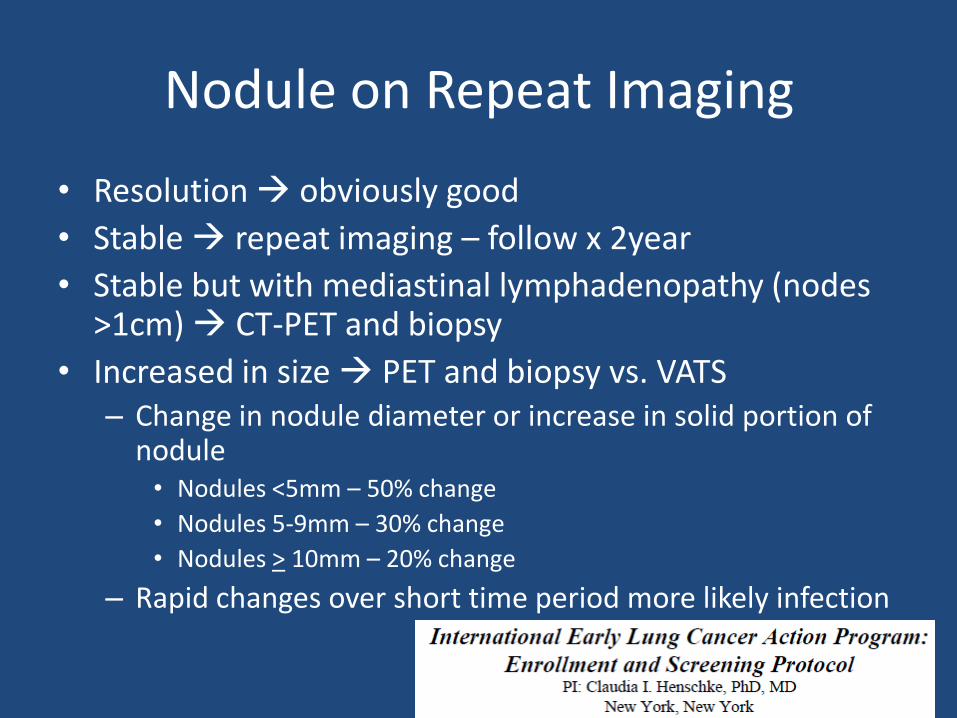
Nodule on Repeat Imaging
• Resolution obviously good
• Stable repeat imaging – follow x 2year
• Stable but with mediastinal lymphadenopathy (nodes >1cm) CT-PET and biopsy
• Increased in size PET and biopsy vs. VATS– Change in nodule diameter or increase in solid portion of
nodule • Nodules <5mm – 50% change
• Nodules 5-9mm – 30% change
• Nodules > 10mm – 20% change
– Rapid changes over short time period more likely infection
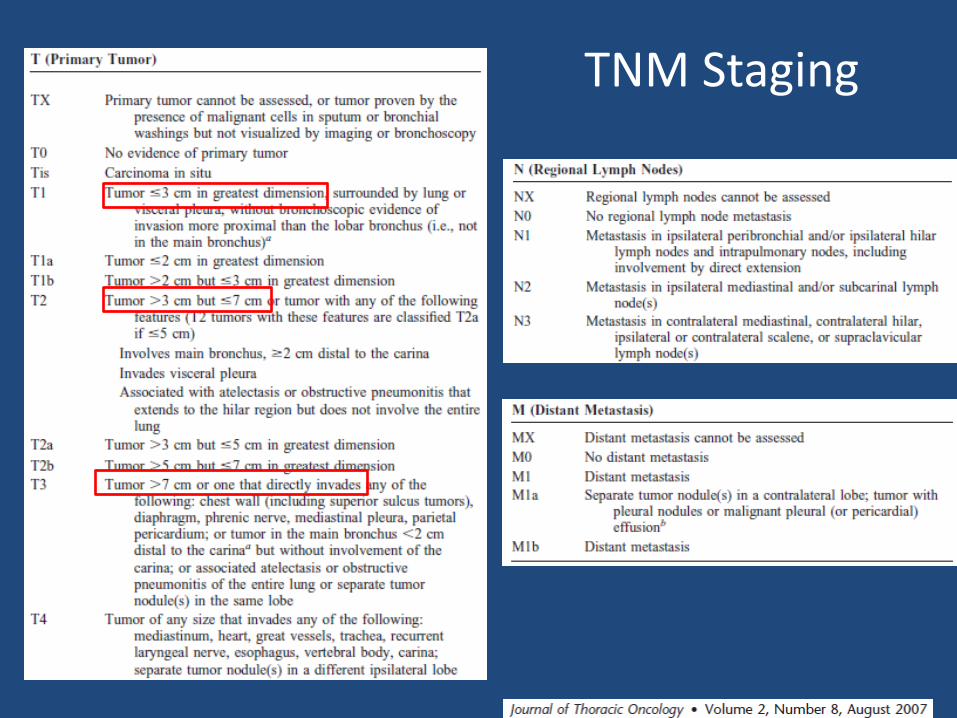
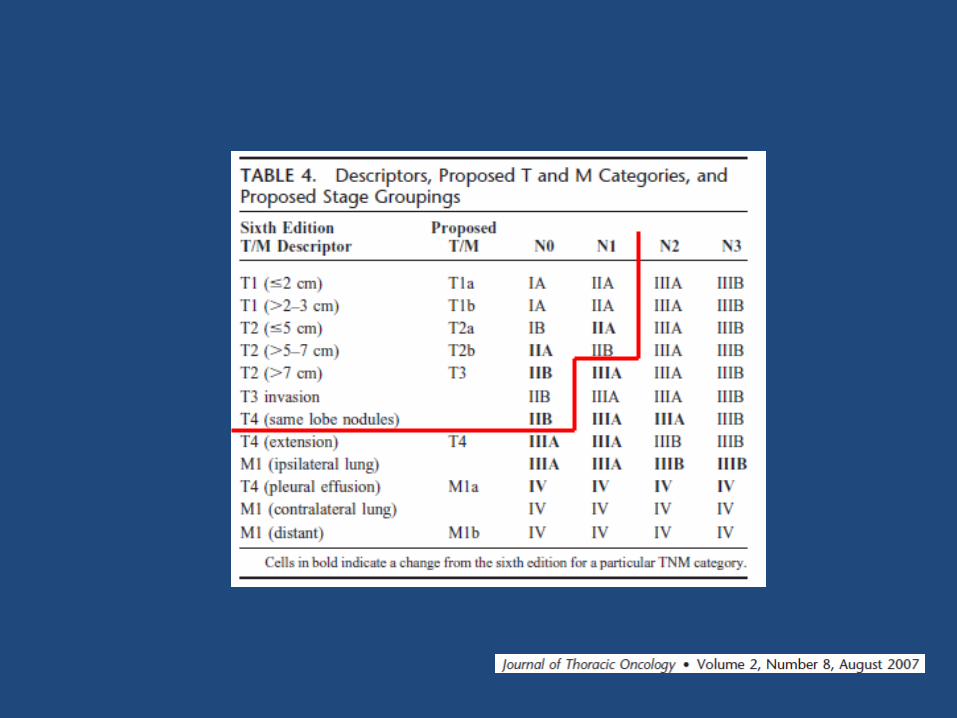
TNM Staging
Case Presentations
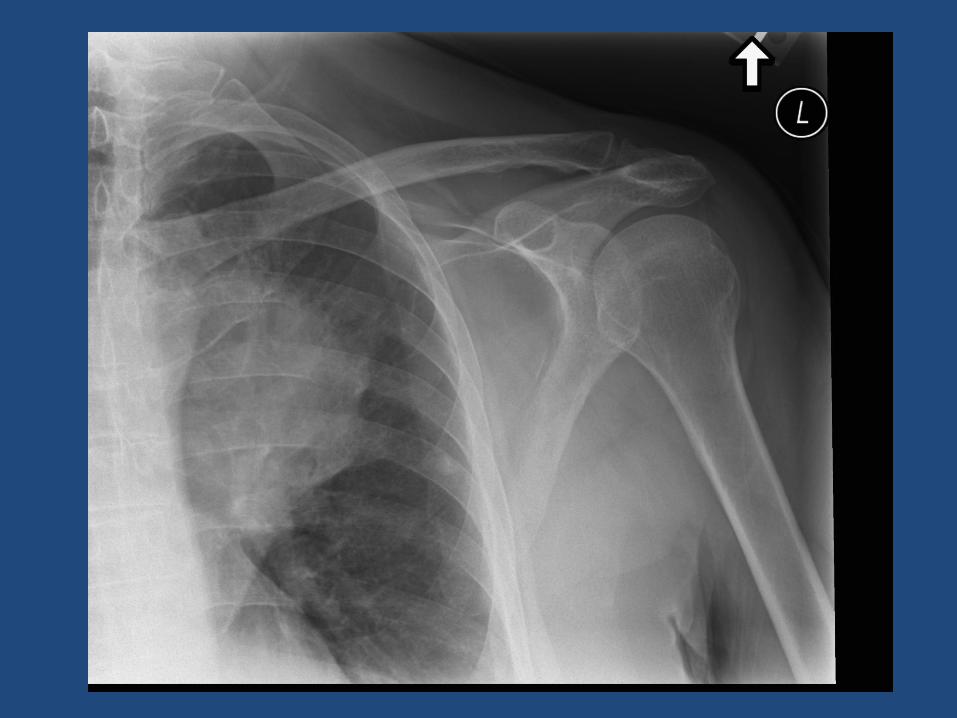
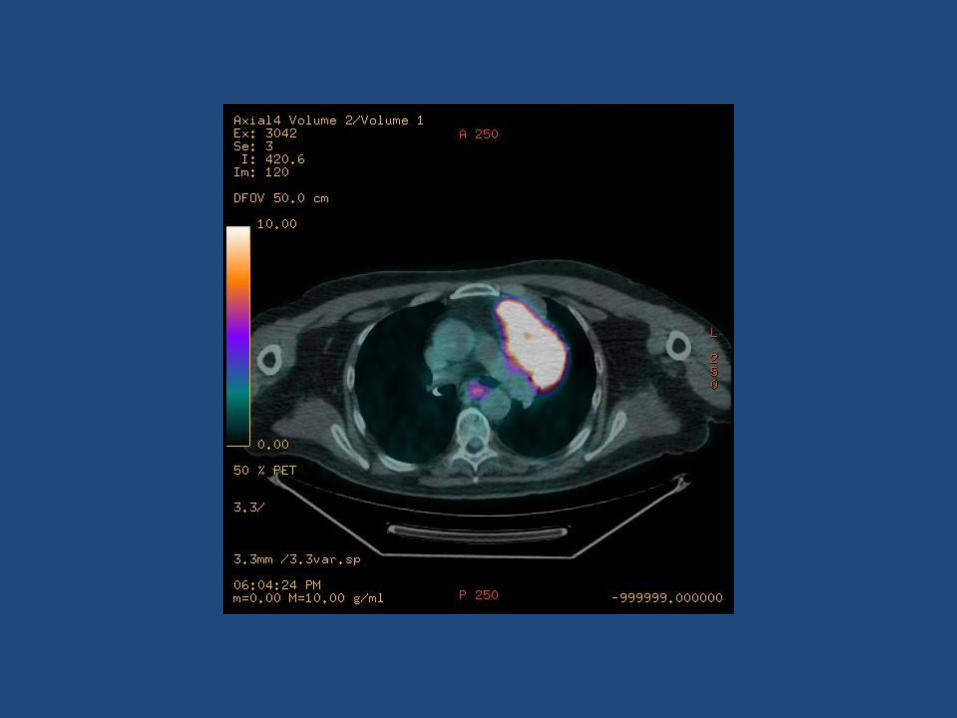
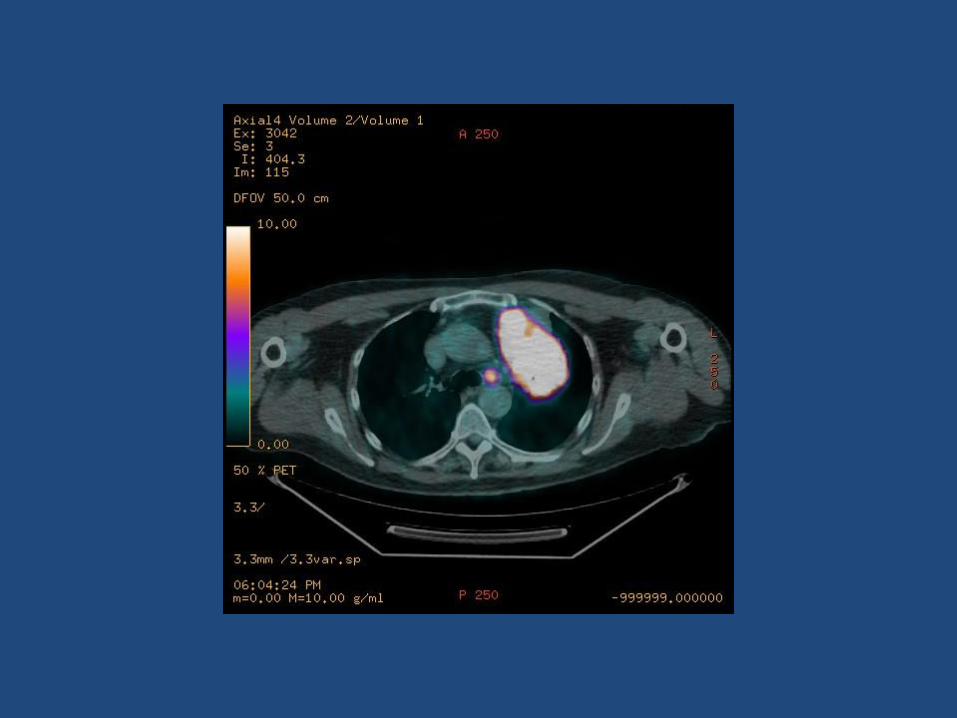
Patient RG67 y/o M presents with left lung mass found in workup for shoulder pain
PMHx – DM, COPD, HTN, Hyperparathyroid, Arthritis
Additional History?smoking history, environmental exposures, cough, hemoptysis, weight changes, infectious disease history, voice changes, cervical lymphadenopathy, weakness, chest pain
Differential DiagnosisCancer (primary or met), infectious (mycoses, TB, abscess), inflammatory, congenital
Patient RG - Next Steps
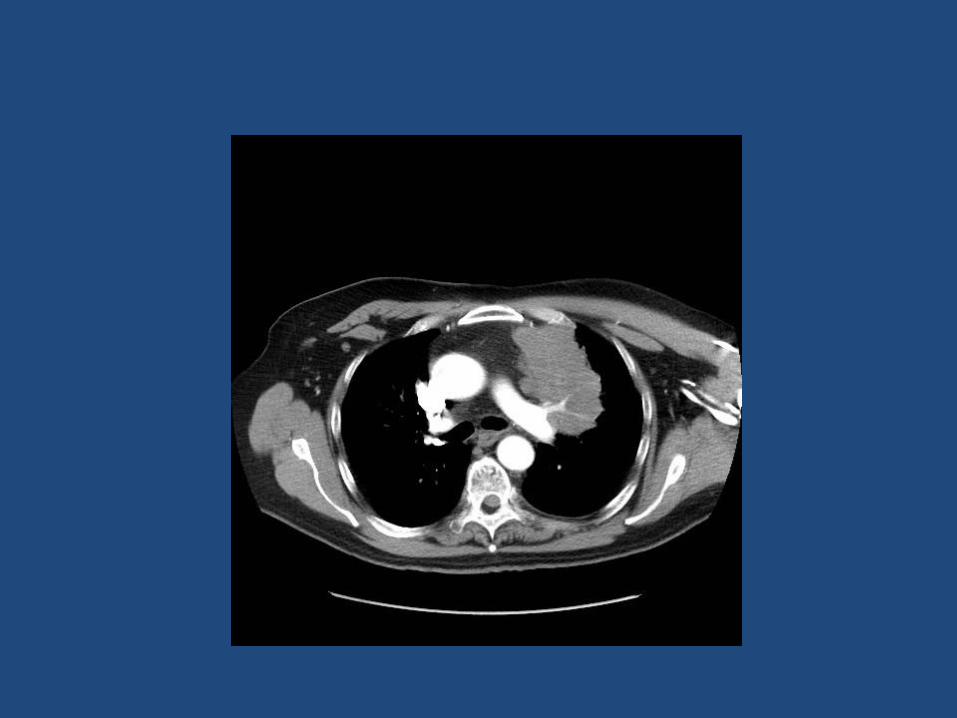
• Risk of malignancy?
– High given size of lung mass, enlarged mediastinalnodes
• If lung cancer – probable clinical stage?
– 9.5 cm with mediastinal nodes, no mets
– If includes pleural effusion?
• Next steps?
– PET/CT
– Biopsy – both primary lesion and mediastinal nodes
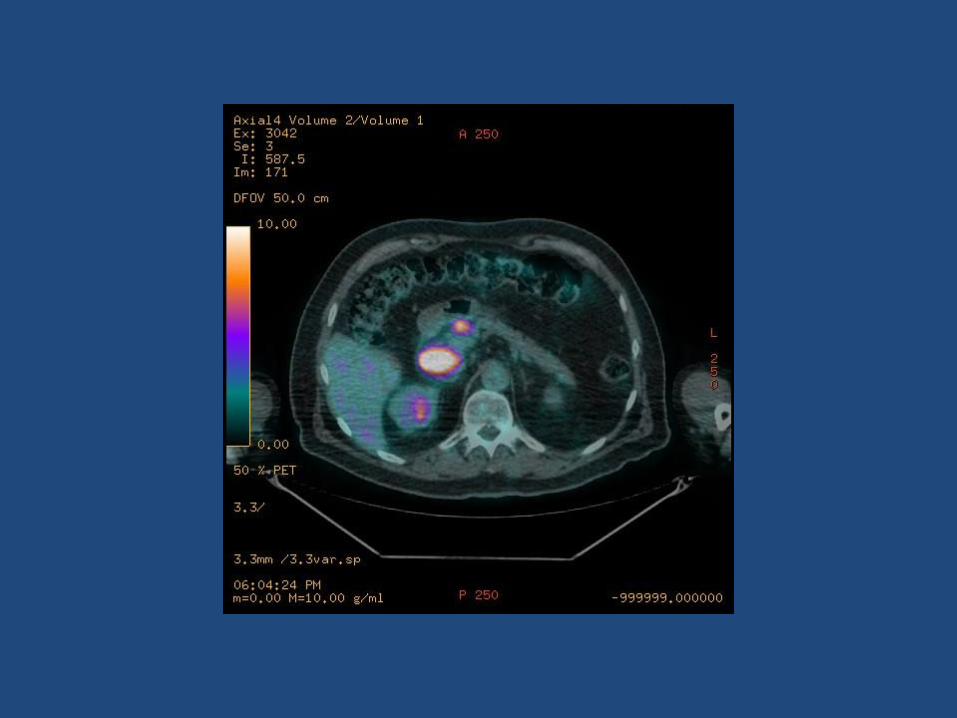
Biopsy 11/24/08
• CT-guided core needle biopsy – approached from left anterior chest
• Diffuse Large B-cell lymphoma
• Referred to Hematology for treatment
– CHOP and Rituxan
Sellke: Sabiston and Spencer’s Surgery of the Chest, 8th edition
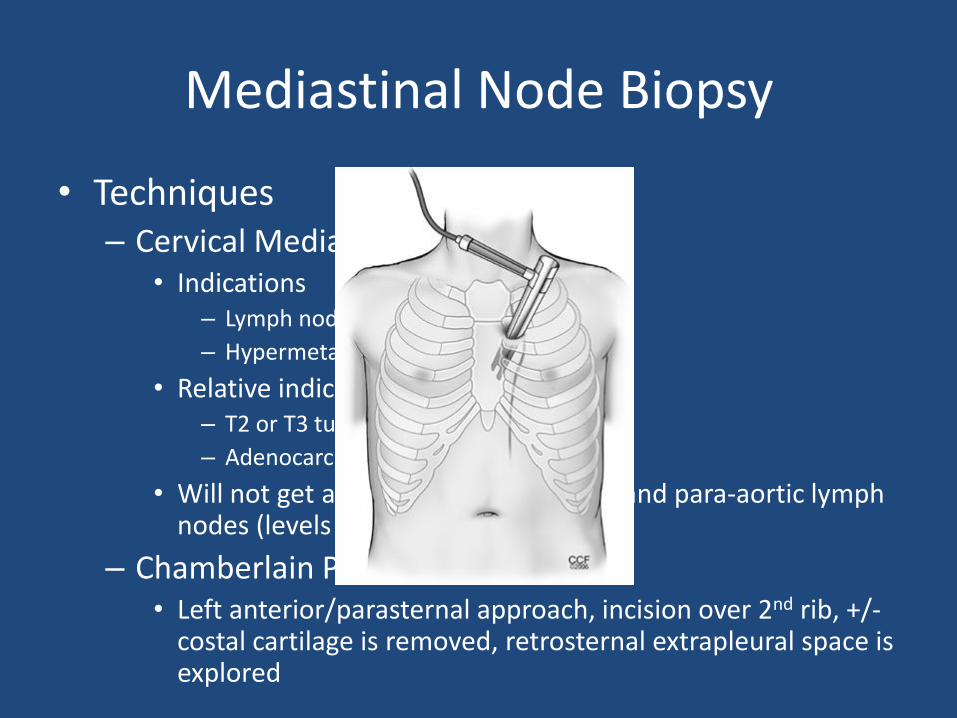
Mediastinal Node Biopsy
• Techniques– Cervical Mediastinoscopy
• Indications– Lymph node enlargement >1cm on CT
– Hypermetabolic lymph nodes on PET
• Relative indications– T2 or T3 tumors
– Adenocarcinoma or large cell carcinoma
• Will not get aortopulmonary window and para-aortic lymph nodes (levels 5 and 6)
– Chamberlain Procedure• Left anterior/parasternal approach, incision over 2nd rib, +/-
costal cartilage is removed, retrosternal extrapleural space is explored
Learning Points – Patient RG
• Predictors of malignancy – nodule characteristics
• Enlarged mediastinal lymph nodes on CT additional staging with PET/CT
• Biopsy for diagnosis and staging – both primary tumor and mediastinal nodes
Patient GB75 y/o F LUL 5mm mass found by PCP (unknown
reason for imaging)PMHx: HTN, CAD, COPD, TAH in 1977, left thigh mass
Additional History?smoking history, environmental exposures, cough, hemoptysis, weight changes, infectious disease history, voice changes, cervical lymphadenopathy, weakness, chest pain**Old images**
Additional imaging/next step?Baseline CT and planned repeat imaging in 3 months
Patient GB
• Repeat CT scan 1 year later
– Nodule size is 1cm
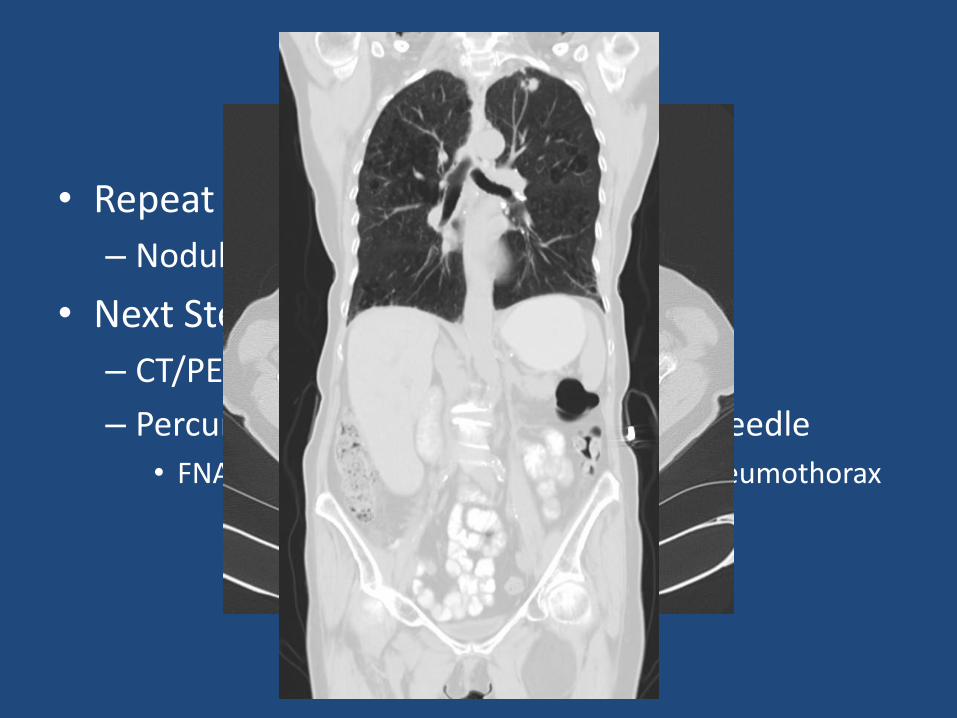
• Next Step?
– CT/PET
– Percuntaneous Biopsy – FNA vs. Core Needle
• FNA indeterminate and complicated by pneumothorax
Patient GB
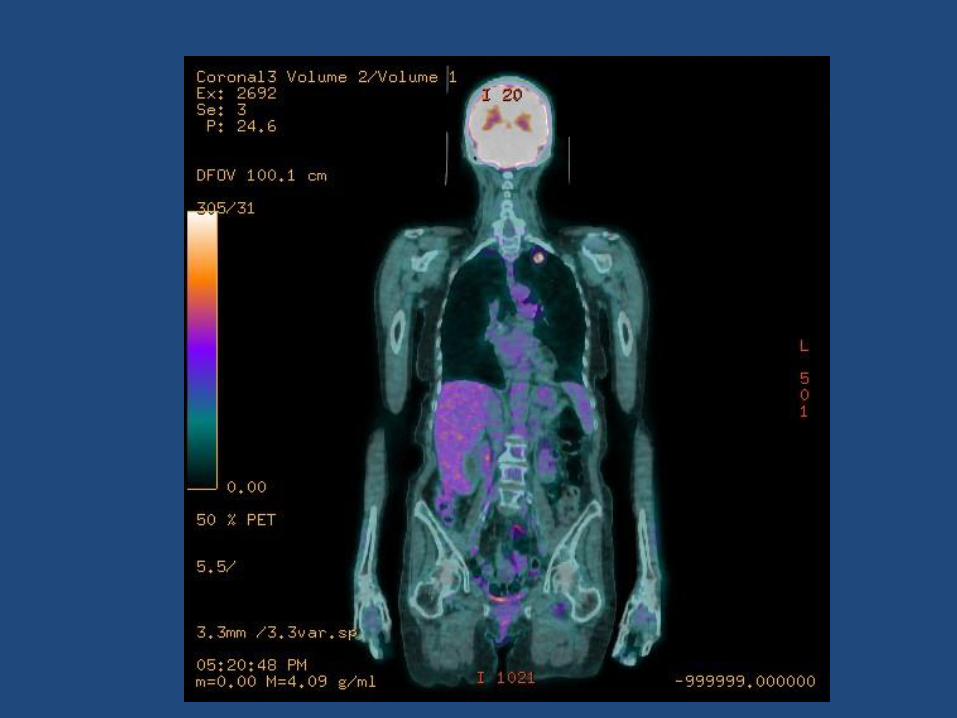
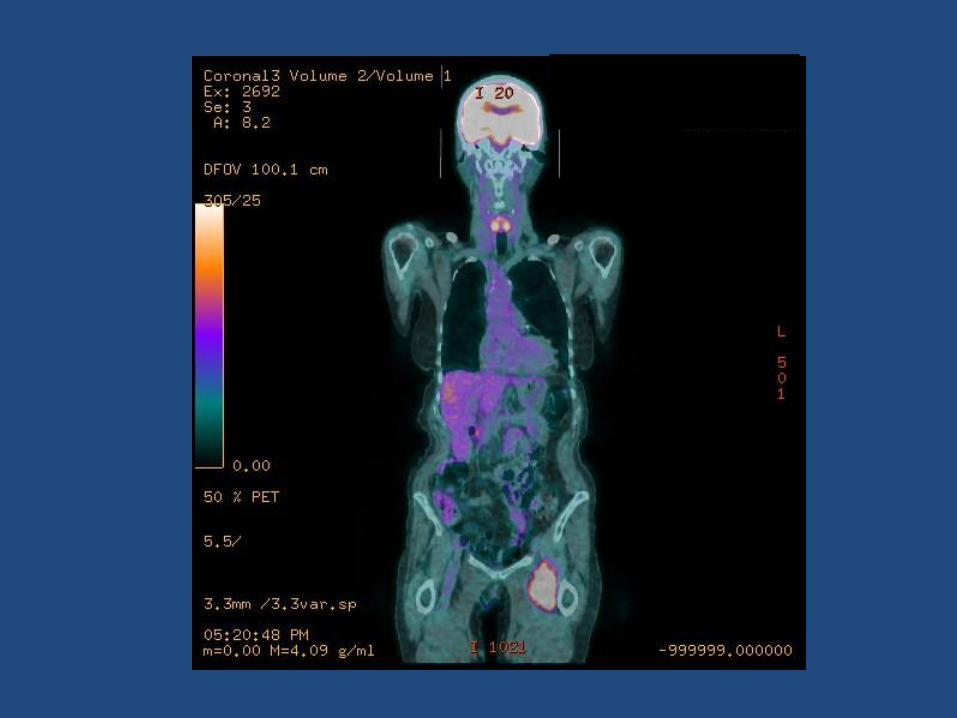
• PET/CT Scan– 2.1 x 1.3 spiculated Left upper lobe mass
– Intensely FDG avid
– 1.1 cm right paratracheal lymph node, not FDG avid and “likely benign”
– Left medial thigh mass 5.1 x 5.1cm, FDG avid
• Next Step?– Thigh mass work-up
– Excised – 9.5 cm hibernoma (benign tumor of brown fat)
Patient GB
• She seeks second opinion after indeterminate lung biopsy results and benign leg lesion
• Options?
– Repeat percutaneous biopsy
– Bronchoscopic biopsy
• Not amenable given location
– Surgical Biopsy with formal resection if cancer
Patient GB – Next Step
• PET positive 2.1 cm LUL lesion, PET negative mediastinal nodes, no metastatic disease noted, thigh mass benign
• Clinical Stage?– T1bN0M0 – Stage I
• Next Step?– Pre-op work up including PFTs, Cardiac Stress Test
– OR for Bronchoscopy and VATS, possible Left Upper Lobectomy
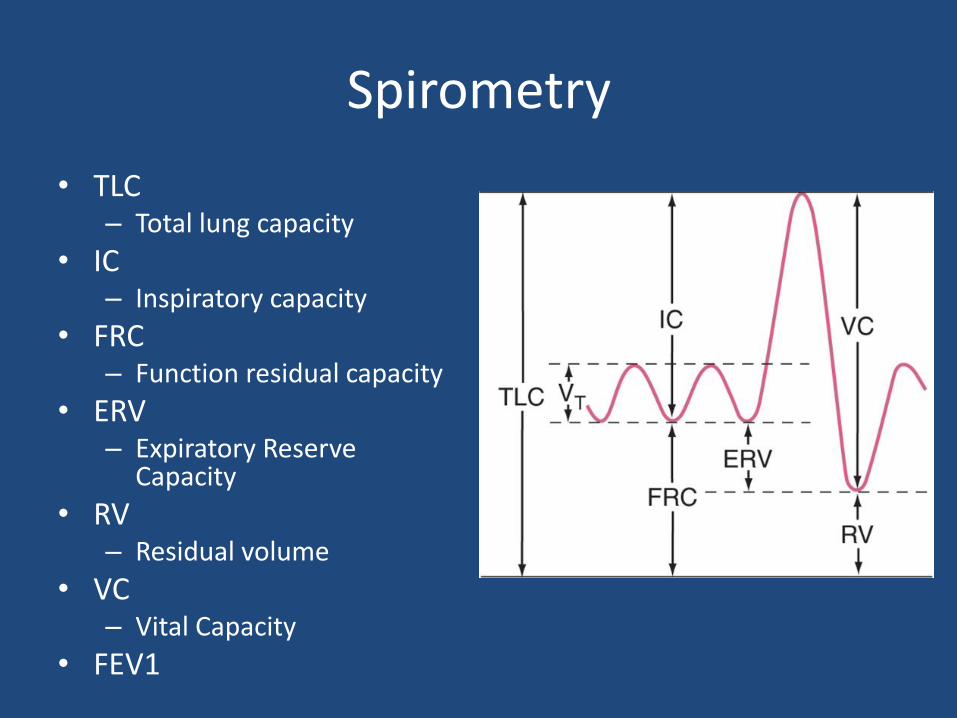
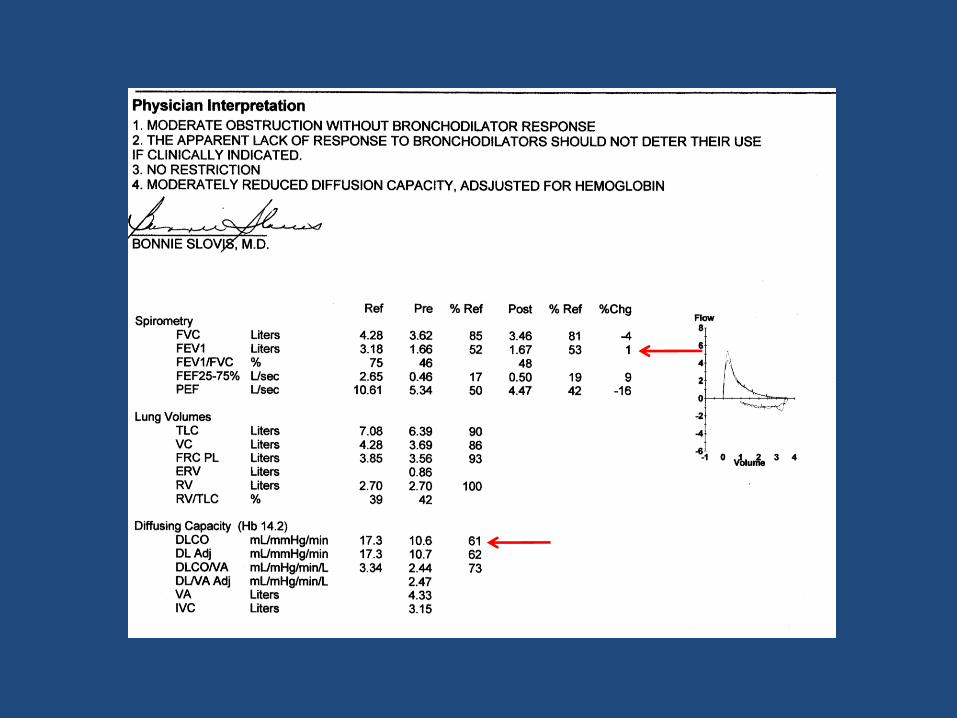
Spirometry
• TLC– Total lung capacity
• IC– Inspiratory capacity
• FRC– Function residual capacity
• ERV– Expiratory Reserve
Capacity
• RV– Residual volume
• VC– Vital Capacity
• FEV1
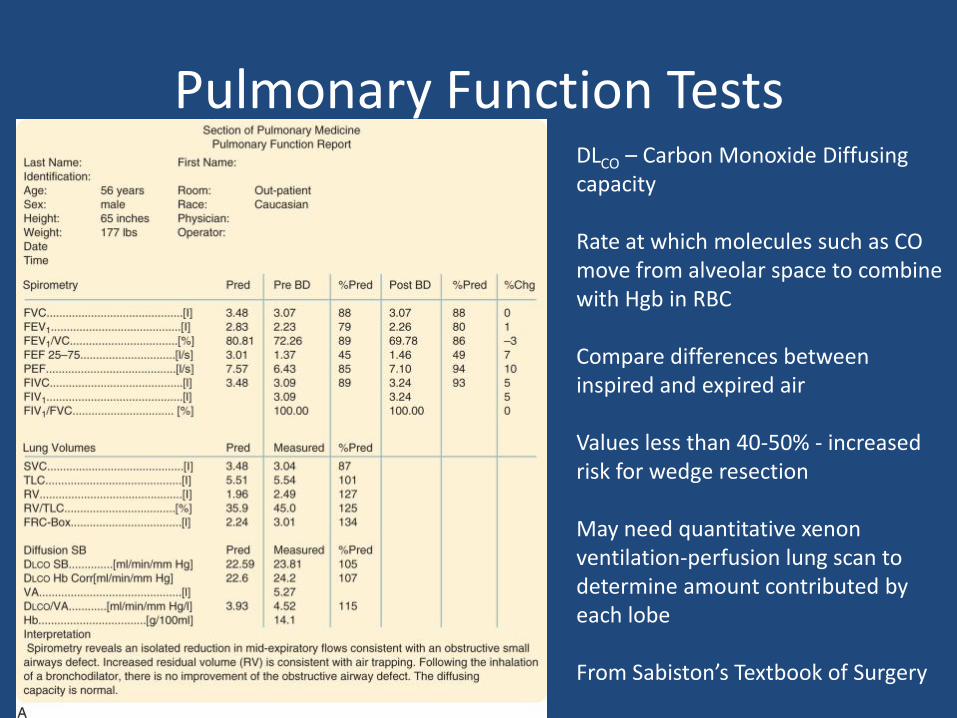
Pulmonary Function TestsDLCO – Carbon Monoxide Diffusing capacity
Rate at which molecules such as CO move from alveolar space to combine with Hgb in RBC
Compare differences between inspired and expired air
Values less than 40-50% - increased risk for wedge resection
May need quantitative xenon ventilation-perfusion lung scan to determine amount contributed by each lobe
From Sabiston’s Textbook of Surgery
Operative Course
• Bronchoscopy – normal bronchial anatomy, no endobronchial masses
• Right Lateral Decubitus position– VATS – wedge resection of mass for pathology– Path – non-small cell lung ca– Video-assisted formal left upper lobectomy
• Final Pathology– 1.4 cm non-small cell carcinoma, favor squamous– All nodes negative– Pathologic Stage?
• T1aN0M0 – Stage I
Learning Points – Patient GB
• Enlarging mass needs tissue diagnosis
• R/o metastatic disease
• Pre-op Spirometry and PFTs
• Lung Cancer Staging
Patient MG
75 y/o F left-sided chest pain, concern for PE pulmonary nodules on CT
PMHx – CAD s/p PTCA & stents, hysterectomy (1985), hypercholesterolemia
Additional History?
smoking history, environmental exposures, cough, hemoptysis, weight changes, infectious disease history, voice changes, cervical lymphadenopathy, weakness, chest pain
CT scan

Patient MG
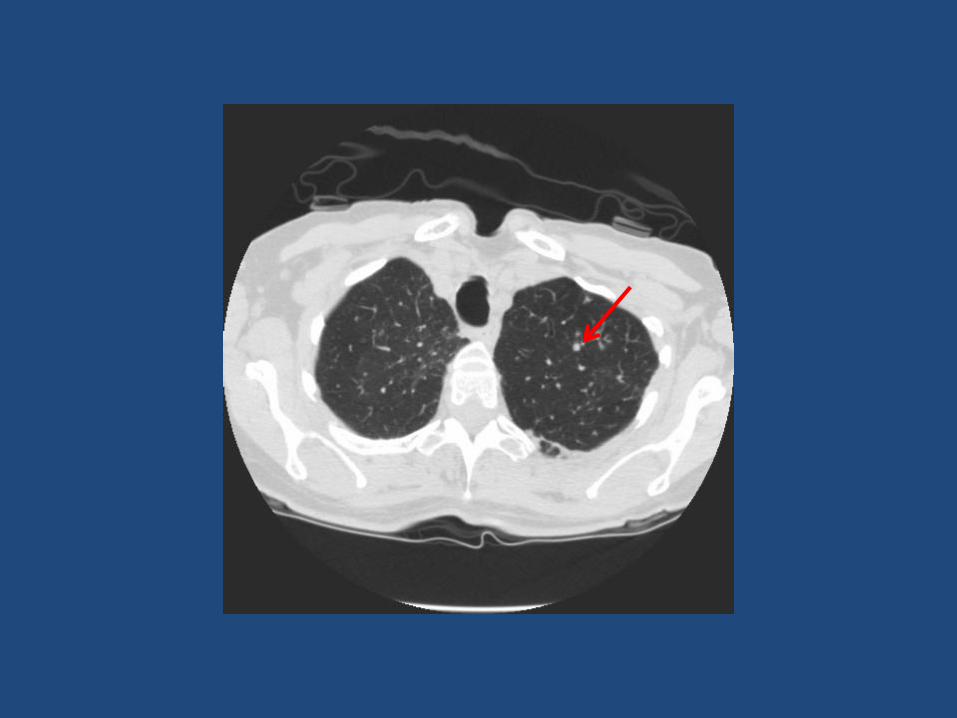
• CT Scan findings:– Airspace opacity in the superior lingula and to a lesser
degree in the right middle lobe associated with multiple ground-glass pulmonary nodules and mediastinaladenopathy – largest node in LUL approximately 6.5mm
• Risk for malignancy?– Low – multiple nodules likely infectious
• Next Step?– Sputum cultures
– Bronchoscopy with biopsy/culture
– Short follow-up with repeat imaging after course of abx
Patient MG
• Unable to submit sputum sample for culture
• Bronchoscopy
– Mycobacterium avium complex
– Started on extended course of Azithromycin and Rifampin (Avelox later added)
• Next step?
– Follow up imaging – specifically examining largest nodule (6.5mm nodule)
Learning Points – Patient MG
• Nodule Characteristics and risk of malignancy
• Use of bronchoscopy for diagnosis
• Follow-up imaging
Patient JB82 y/o M presents with a 13mm LUL nodule
PMHx: COPD on 2L NC, CAD s/p CABGx4 1997, cryptococcal pneumonia 1970s, 4.2 cm AAA s/p EVAR, GERD, HTN
Additional History?smoking history, environmental exposures, cough, hemoptysis, weight changes, infectious diseases history, voice changes, cervical lymphadenopathy, weakness, chest pain**Prior Imaging**
Risk of Malignancy?Next Step?
CT-PETBiopsy
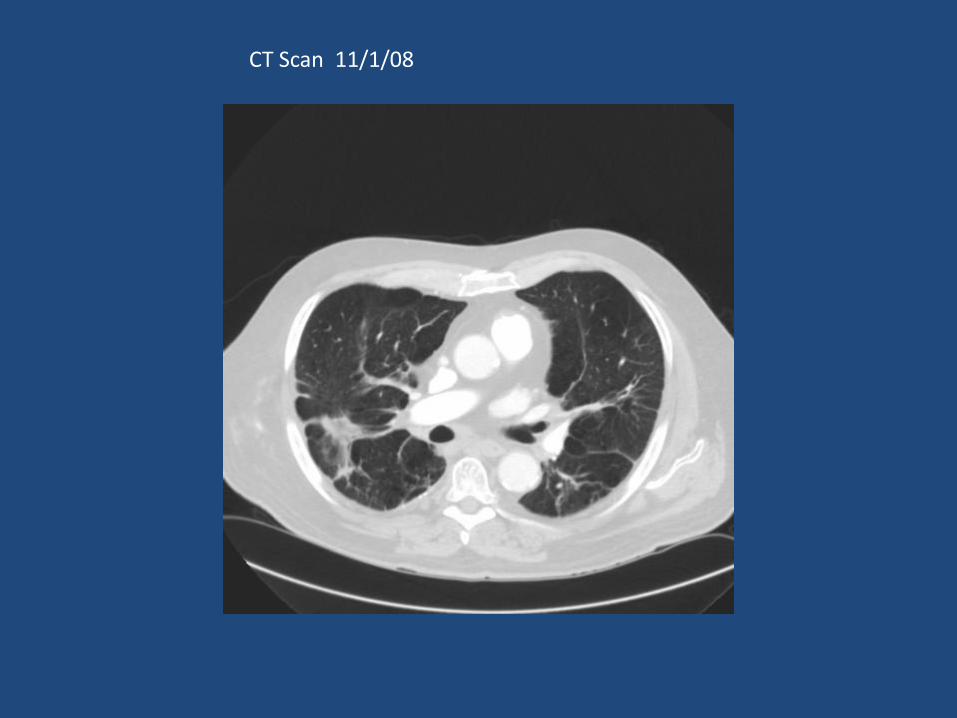
CT Scan 11/1/08
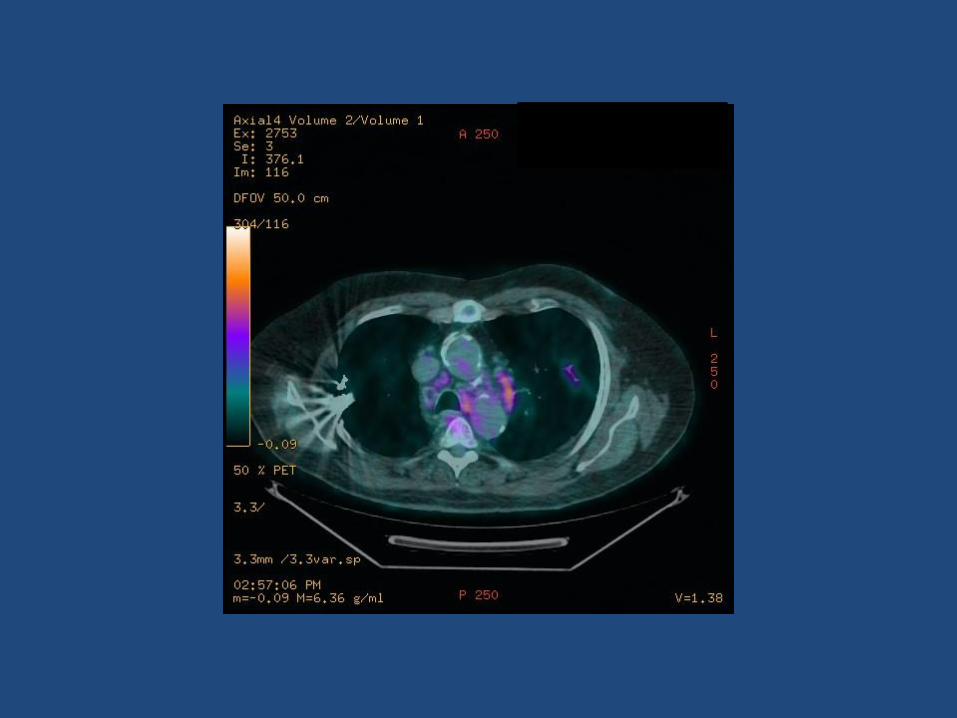
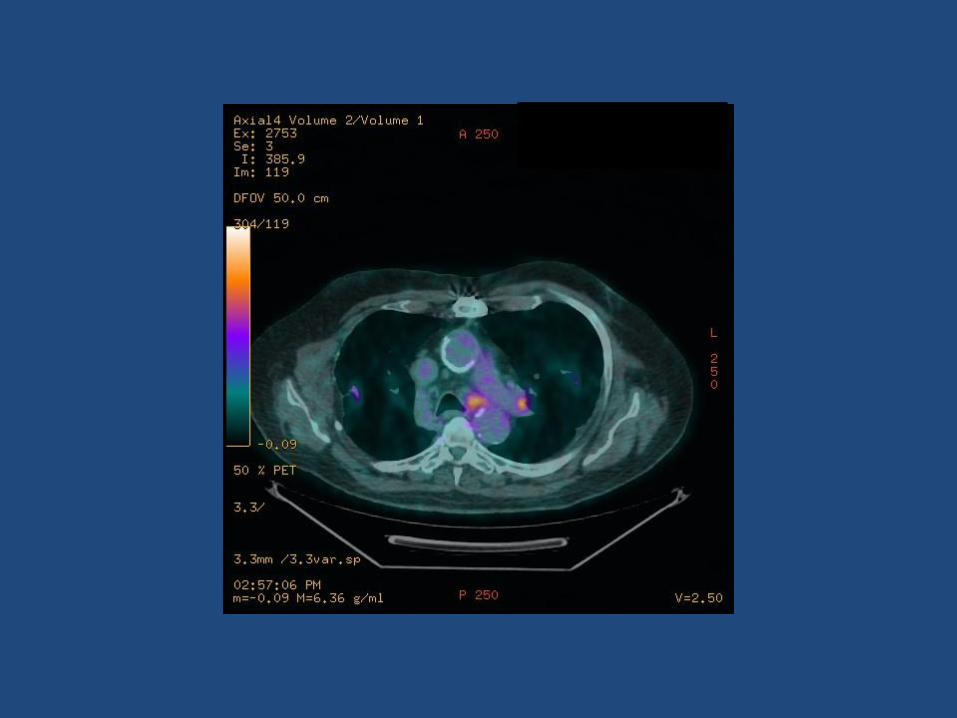
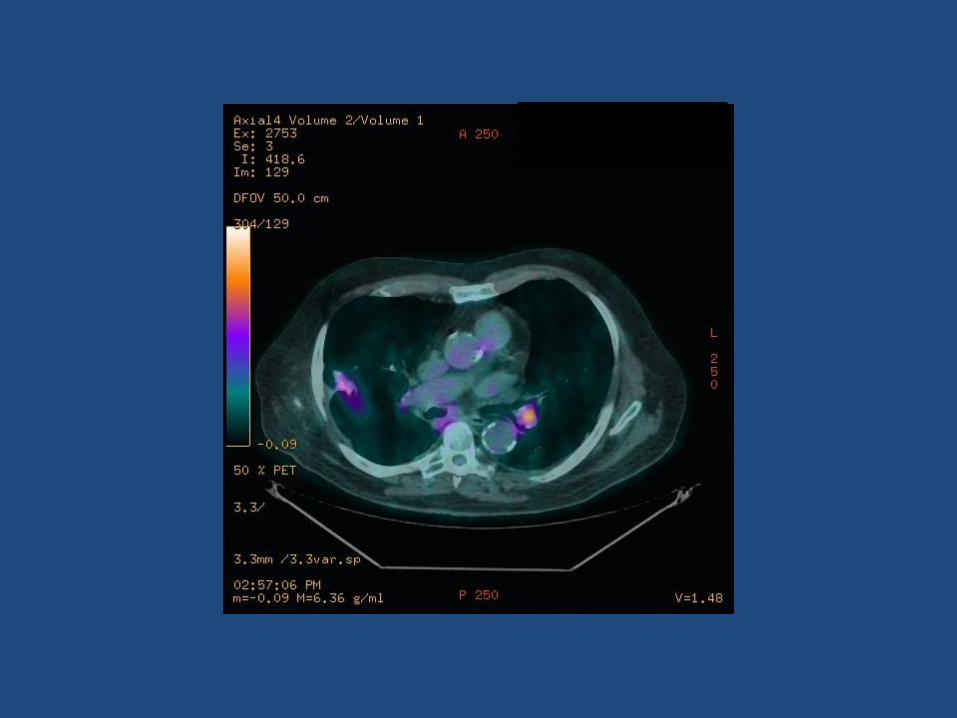
Patient JB
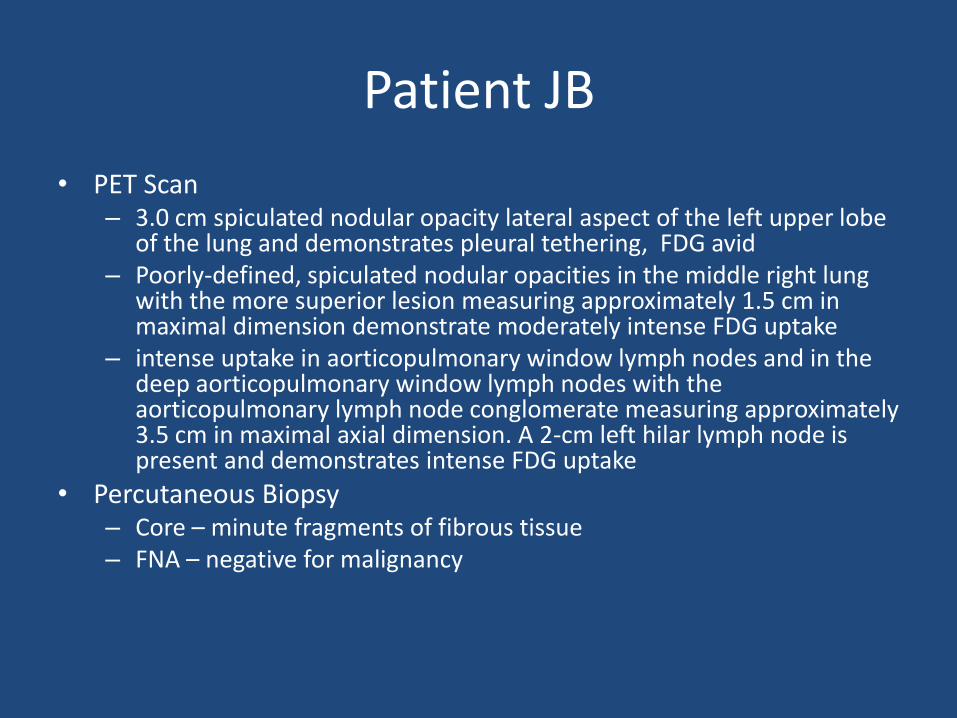
• PET Scan– 3.0 cm spiculated nodular opacity lateral aspect of the left upper lobe
of the lung and demonstrates pleural tethering, FDG avid– Poorly-defined, spiculated nodular opacities in the middle right lung
with the more superior lesion measuring approximately 1.5 cm in maximal dimension demonstrate moderately intense FDG uptake
– intense uptake in aorticopulmonary window lymph nodes and in the deep aorticopulmonary window lymph nodes with the aorticopulmonary lymph node conglomerate measuring approximately 3.5 cm in maximal axial dimension. A 2-cm left hilar lymph node is present and demonstrates intense FDG uptake
• Percutaneous Biopsy– Core – minute fragments of fibrous tissue– FNA – negative for malignancy
Patient JB
• Next Step?
– Bronchscopy and FNA of mediastinal nodes
– Bronchial washings - negative
– FNA – no evidence of malignancy
• Other Staging options?
– Mediastinoscopy – contraindicated given previous CABG and calcified aorta
– Wedge Biopsy – difficult due to live LIMA graft
– Follow-up imaging – 3 months
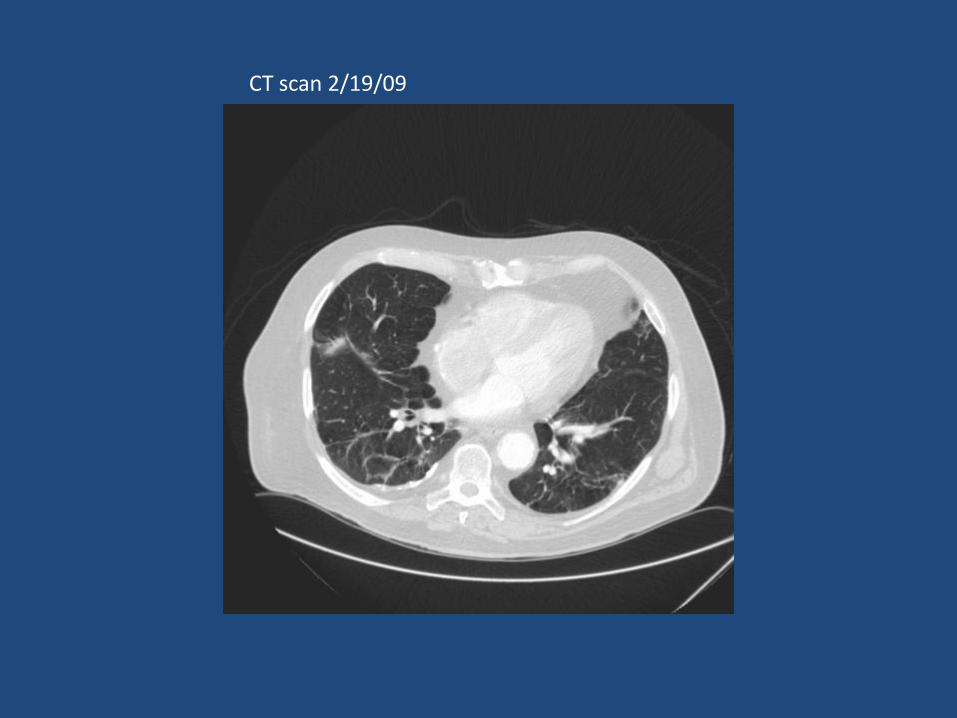
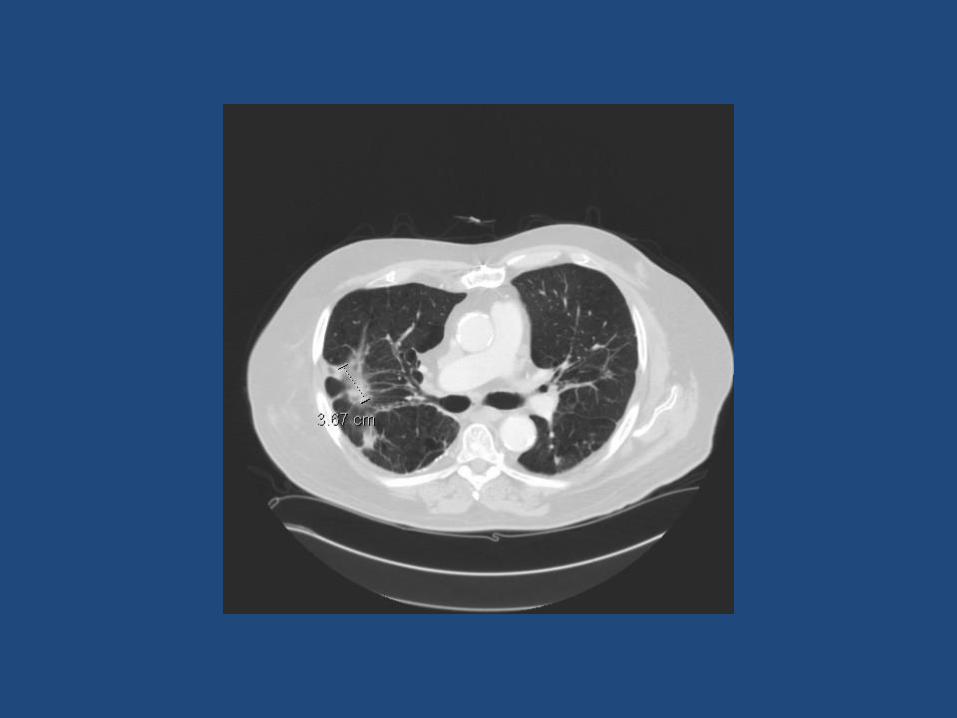
CT scan 2/19/09
Patient JB
• 3-month CT scan – Nodules smaller
– 1.9 cm in the anterior segment of the right upper lobe, 3.5 cm in the posterior segment of the right upper lobe, 0.8 cm in the apicoanterior segment of the left upper lobe
• Continued work-up?
– Repeat imaging at 6 months
A 56 year old patient with a long history of smoking presents with a three month history of multiple seemingly random clots. There is also significant pain that radiates down his left arm and dryness of his eyes. In addition to the sympathetic chain, what
other structure is most likely involved?
1 2 3 4 5
0% 0% 0%0%0%
1. Radial nerve
2. Median nerve
3. Axillary nerve
4. Ulnar nerve
5. Intercostobrachial nerve
What is the correct TNM classification for a lung cancer that is 4 cm in size that invades into the mediastinum, has several positive ipsilateral mediastinal lymph nodes, and has no
evidence of invasion into the great vessels?
1 2 3 4 5
0% 0% 0%0%0%
1. T4N1
2. T4N2
3. T2N3
4. T2N1
5. T3N1
A patient with a suspicious finding on a CT scan requires a wedge resection. What is the minimum
preoperative FEV1 required on a PFT for this patient to be eligible for an operation?
1 2 3 4 5
0% 0% 0%0%0%
1. 2L
2. 1L
3. 0.8L
4. 0.3L
5. 0.6L
A popcorn lesion is found on a chest x-ray in a 36 year old patient with a 5 pack year history of smoking. This is most likely an early finding in lung adenocarcinoma.
1 2
0%0%
1. True
2. False
A 71 year old female diagnosed with lung cancer has difficulty getting out of bed in the morning and always
feels excessively fatigued. What is the most likely diagnosis?
1 2 3 4 5 6
0% 0% 0%0%0%0%
1. Horner syndrome
2. Eaton-Lambert syndrome
3. SIADH
4. Trousseau syndrome
5. SVC syndrome
6. Pancoast tumor
A 78 year old male diagnosed with lung cancer also has SIADH. Describe
this sodium abnormality.
1 2 3 4
0% 0%0%0%
1. Euvolemichyponatremia
2. Hypernatremia
3. Hypovolemichyponatremia
4. Hypervolemichyponatremia
Recommended

![Accurate Pulmonary Nodule Detection in Computed Tomography ... · Pulmonary cancer, causing 1.3 million deaths annually, is a leading cause of cancer death worldwide [8]. Detection](https://img.pdfslide.net/doc/110x75/5f9882f757fdde3a4377a39c/accurate-pulmonary-nodule-detection-in-computed-tomography-pulmonary-cancer.jpg)