Radiologyof
Pediatric Gastroenterology
Normal Oesophagus
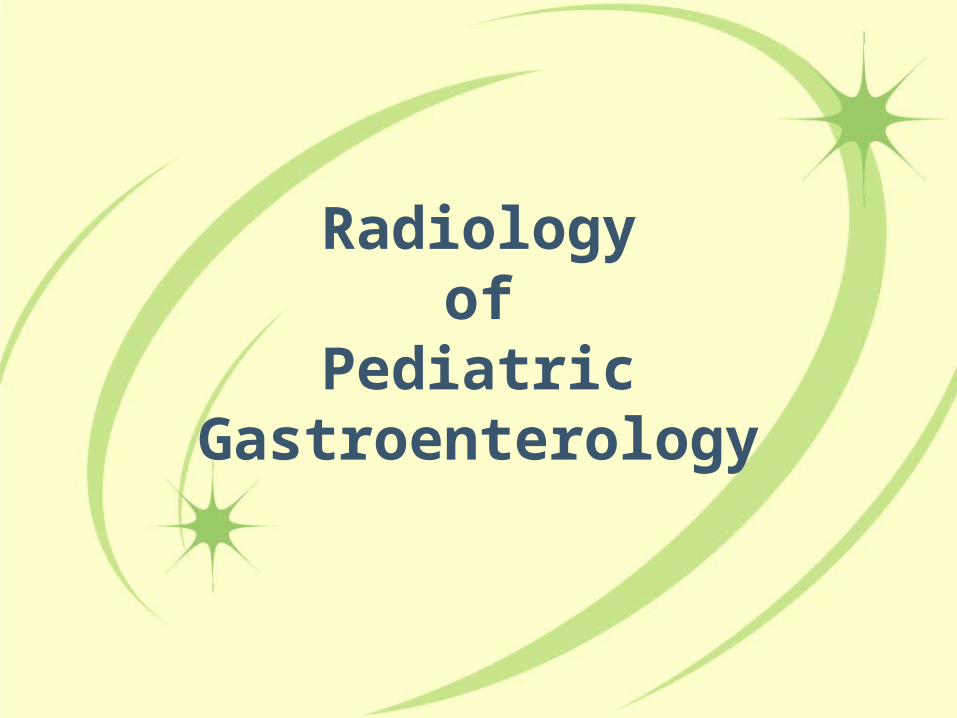
Barium swallow examination: Lateral view: The course and diameter of the esophagus are normal, the longitudinal mucosal folds are regular.
Normal Stomach
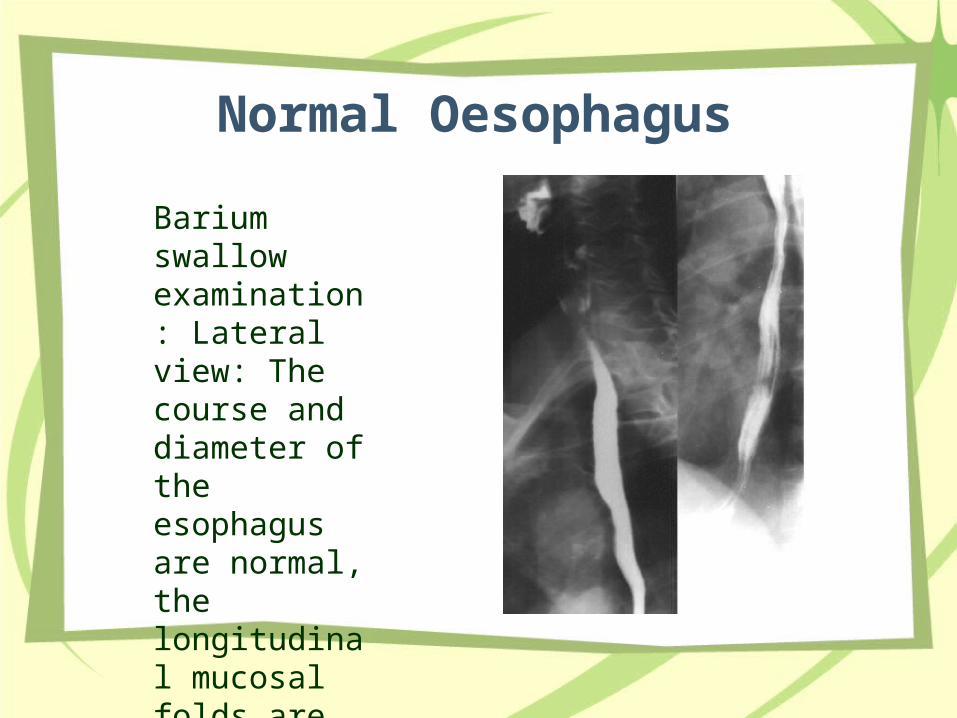
• Postcontrast examination: The stomach is of normal size and shape, its mucosal folds are regular. The fornix is filled with contrast material because of the supine position. The duodenum is normal. Jejunal loops filled with contrast material are visible behind the stomach.
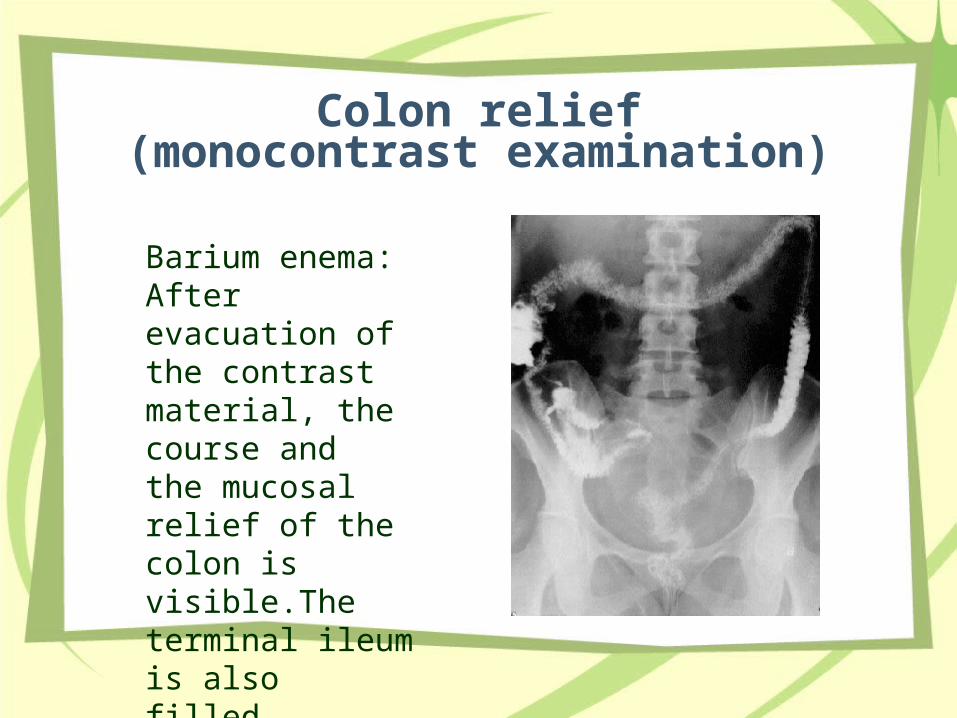
Colon relief(monocontrast examination)
Barium enema: After evacuation of the contrast material, the course and the mucosal relief of the colon is visible.The terminal ileum is also filled.
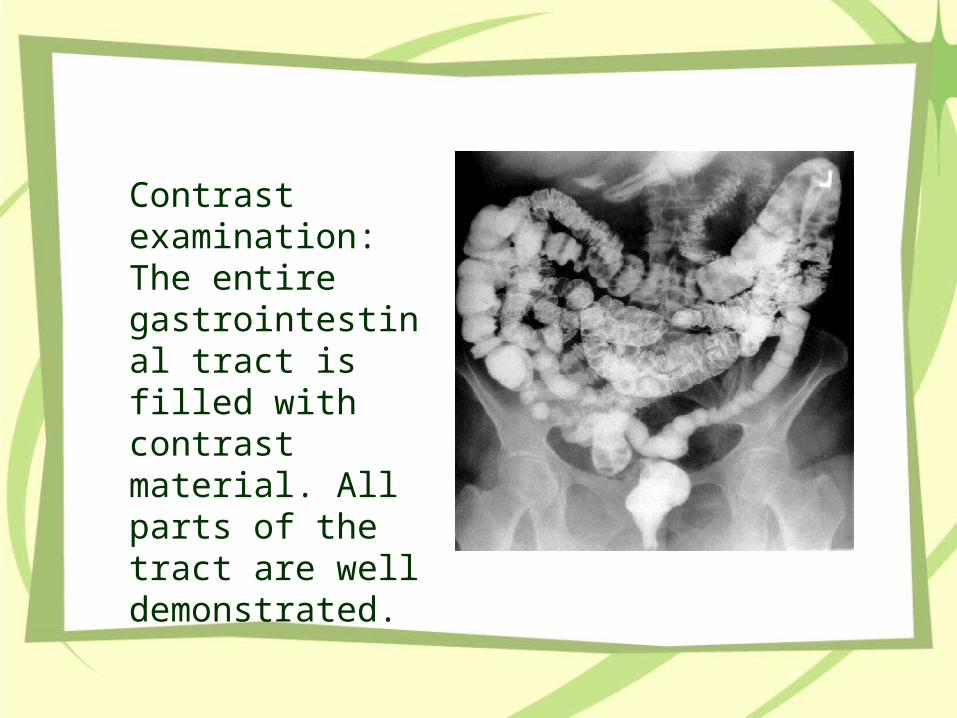
Contrast examination: The entire gastrointestinal tract is filled with contrast material. All parts of the tract are well demonstrated.
CASE I
ACALASIA
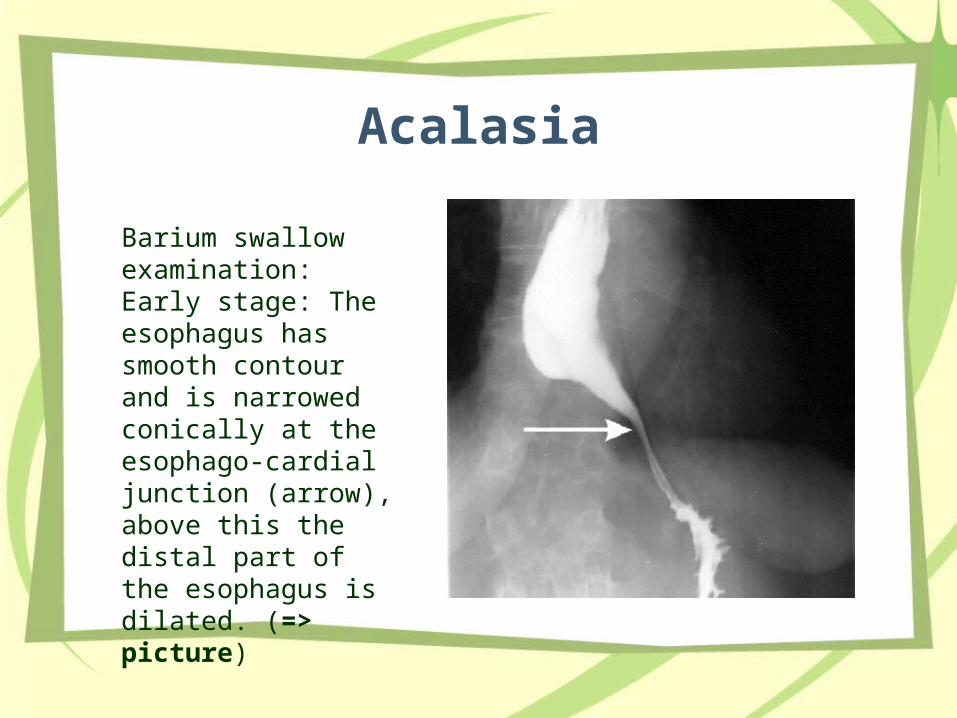
Acalasia
• Barium swallow examination: Early stage: The esophagus has smooth contour and is narrowed conically at the esophago-cardial junction (arrow), above this the distal part of the esophagus is dilated. (=> picture)
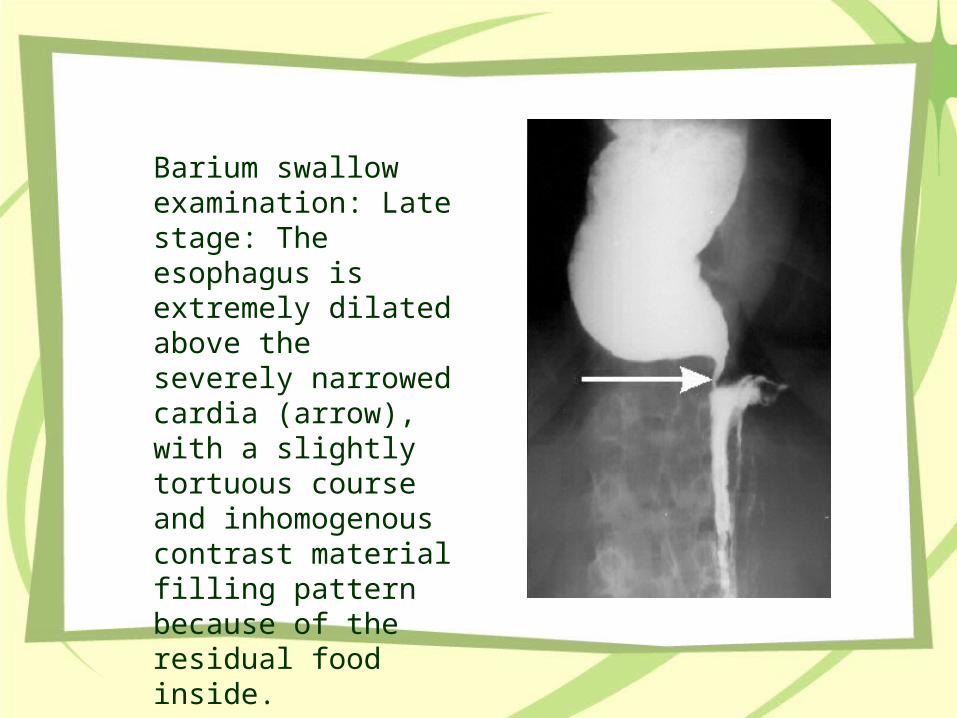
Barium swallow examination: Late stage: The esophagus is extremely dilated above the severely narrowed cardia (arrow), with a slightly tortuous course and inhomogenous contrast material filling pattern because of the residual food inside.
Case 2
ESOPHAGEAL ATRESIA
• EA is a condition in which the proximal and distal portions of the esophagus do not communicate
Clinical signs • The first clinical sign of an infant with EA is
maternal polyhydramnios resulting from the infant's inability to swallow and absorb amniotic fluid through the gut.
• Excess salivation and fine, frothy bubbles in the mouth and sometimes nose result from an inability to swallow. Any attempts at feeding result in choking, coughing, cyanotic episodes, and food regurgitation.
•
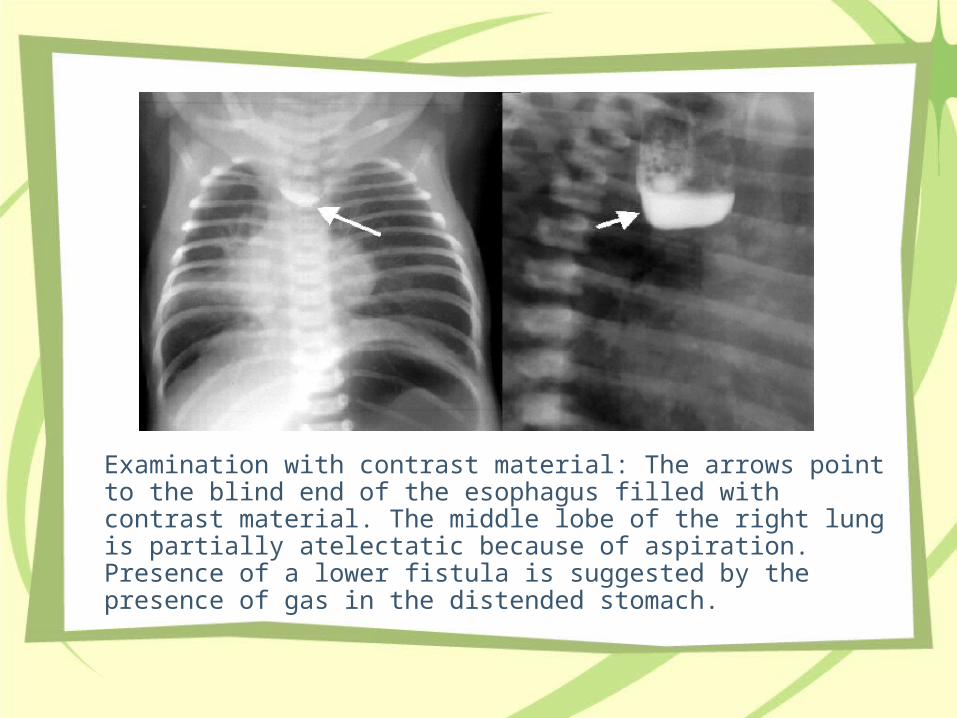
Examination with contrast material: The arrows point to the blind end of the esophagus filled with contrast material. The middle lobe of the right lung is partially atelectatic because of aspiration. Presence of a lower fistula is suggested by the presence of gas in the distended stomach.
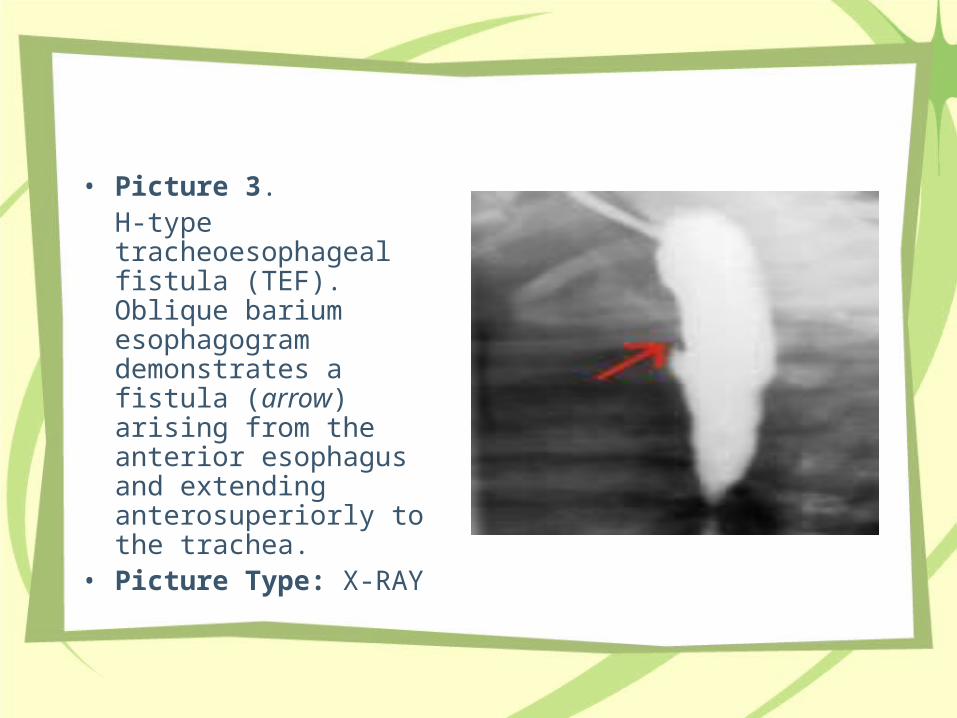
• Picture 3. H-type tracheoesophageal fistula (TEF). Oblique barium esophagogram demonstrates a fistula (arrow) arising from the anterior esophagus and extending anterosuperiorly to the trachea.
• Picture Type: X-RAY
CASE 3
Hypertrophic Pyloric Stenosis
•Clinical History: 2 month old male with a history of recurrent vomiting after meals.
•Findings: Thickening and elongation of the pyloric canal. The muscle wall thickness is 5-6 mm. The pyloric canal measures approximately 21 mm.
X-RAY
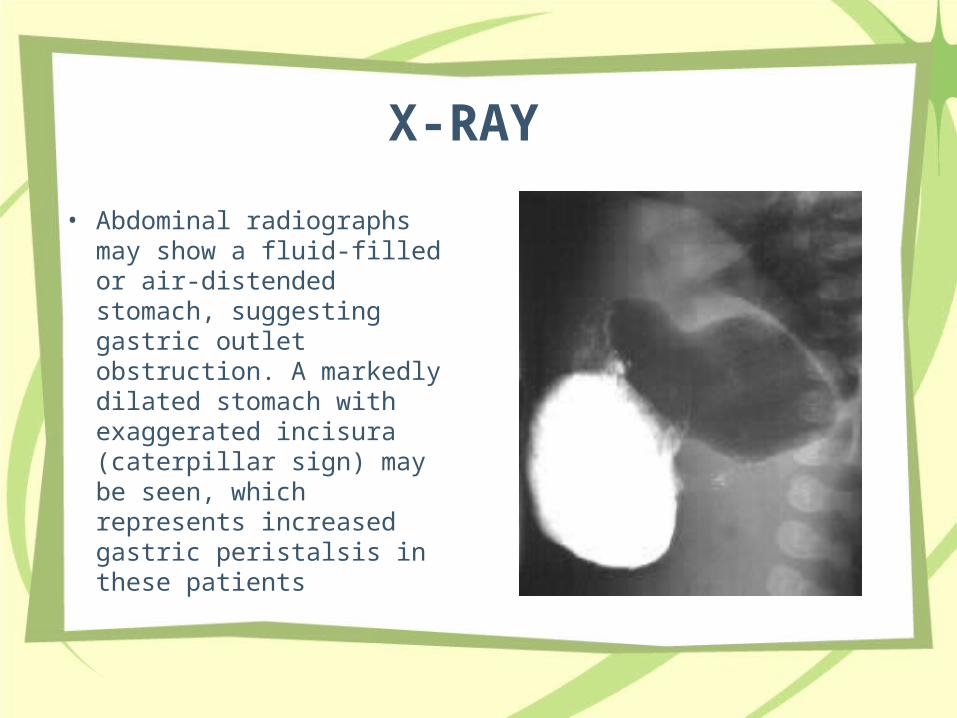
• Abdominal radiographs may show a fluid-filled or air-distended stomach, suggesting gastric outlet obstruction. A markedly dilated stomach with exaggerated incisura (caterpillar sign) may be seen, which represents increased gastric peristalsis in these patients
Findings on UGI include the following: • Delayed gastric emptying (if severe, this may prevent
barium from passing into the pylorus and severely limit the study)
• Cephalic orientation of the pylorus • Shouldering (ie, filling defect at the antrum created by
prolapse of the hypertrophic muscle) • Mushroom or umbrella sign (ie, thickened muscle
indenting the duodenal bulb (refers to the impression made by the hypertrophic pylorus on the duodenum)
• Double track (ie, redundant mucosa in the narrowed pyloric lumen, which results in separation of the barium column into two channels)
• String sign (ie, barium passing through the narrowed channel creating a single, markedly attenuated and elongated track)
• Pyloric tit (ie, outpouching created by distortion of the lesser curve by the hypertrophied muscle)
• Retained secretions and retrograde peristalsis
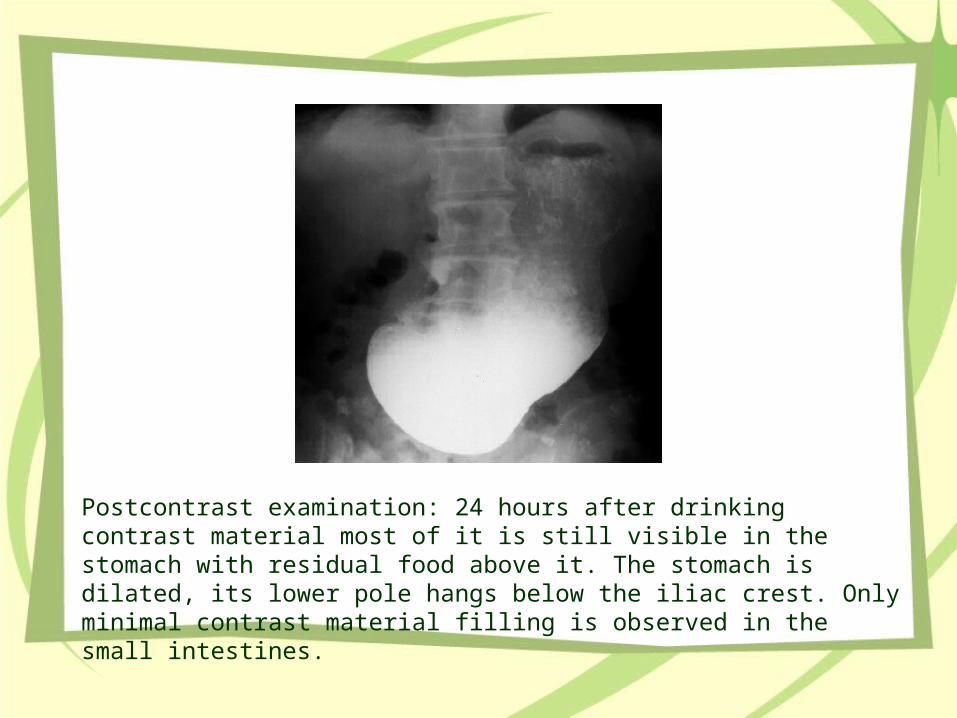
Postcontrast examination: 24 hours after drinking contrast material most of it is still visible in the stomach with residual food above it. The stomach is dilated, its lower pole hangs below the iliac crest. Only minimal contrast material filling is observed in the small intestines.
CASE 4
Duodenal Atresia
• Duodenal atresia represents complete obliteration of the duodenal lumen
• The etiology of duodenal atresia and stenosis is unknown
• Anatomy: In most cases, duodenal atresia occurs below the ampulla of Vater. In a very few cases, the atresia occurs proximal to the ampulla.
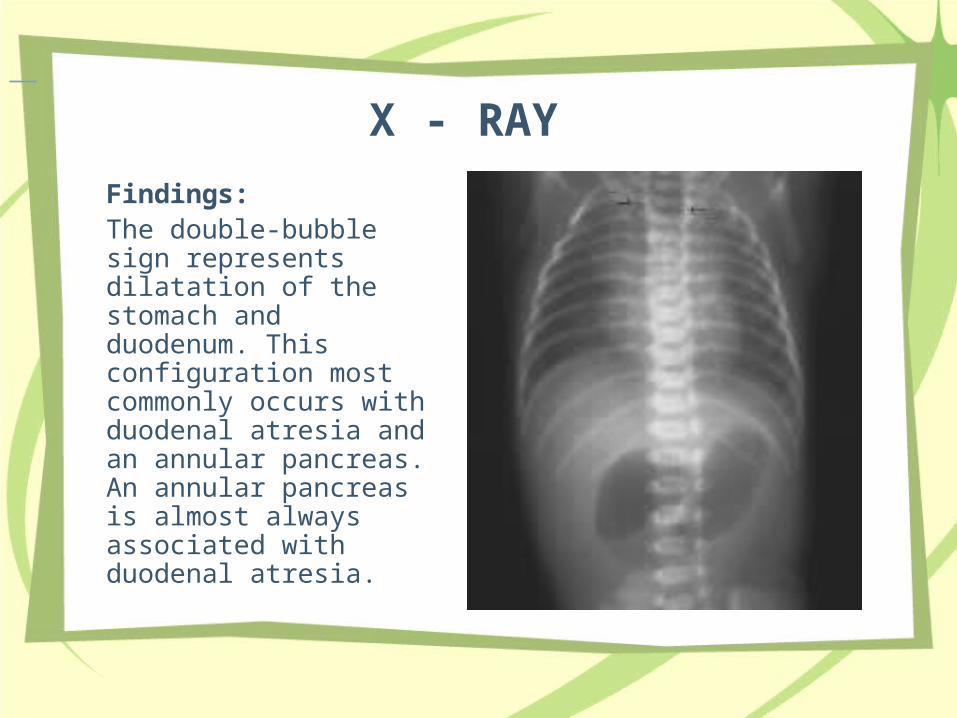
X - RAY Findings: The double-bubble sign represents dilatation of the stomach and duodenum. This configuration most commonly occurs with duodenal atresia and an annular pancreas. An annular pancreas is almost always associated with duodenal atresia.
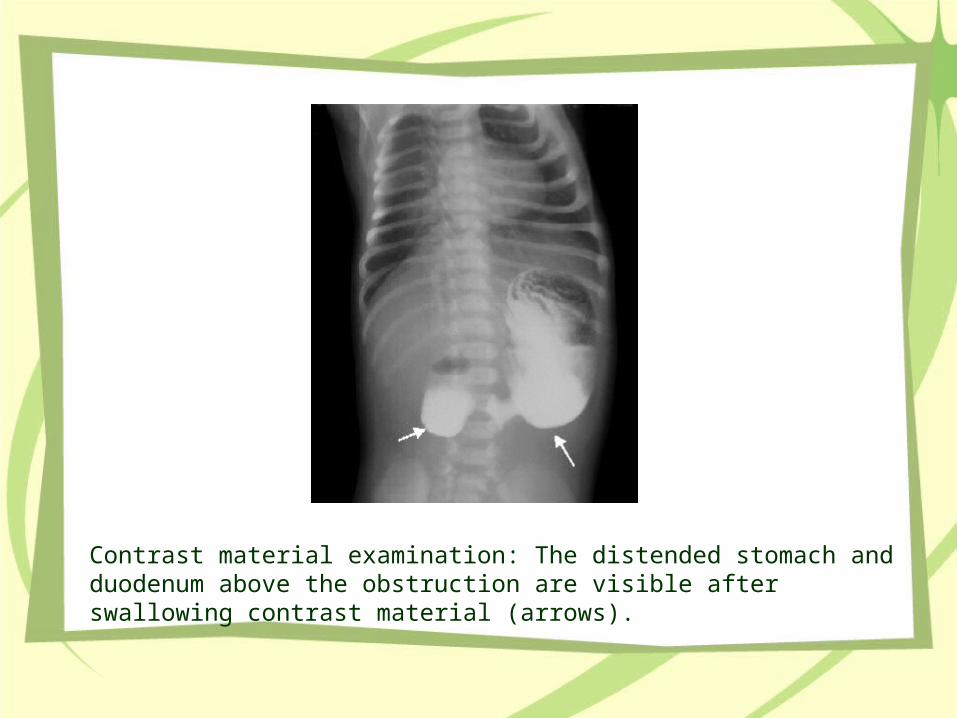
Contrast material examination: The distended stomach and duodenum above the obstruction are visible after swallowing contrast material (arrows).
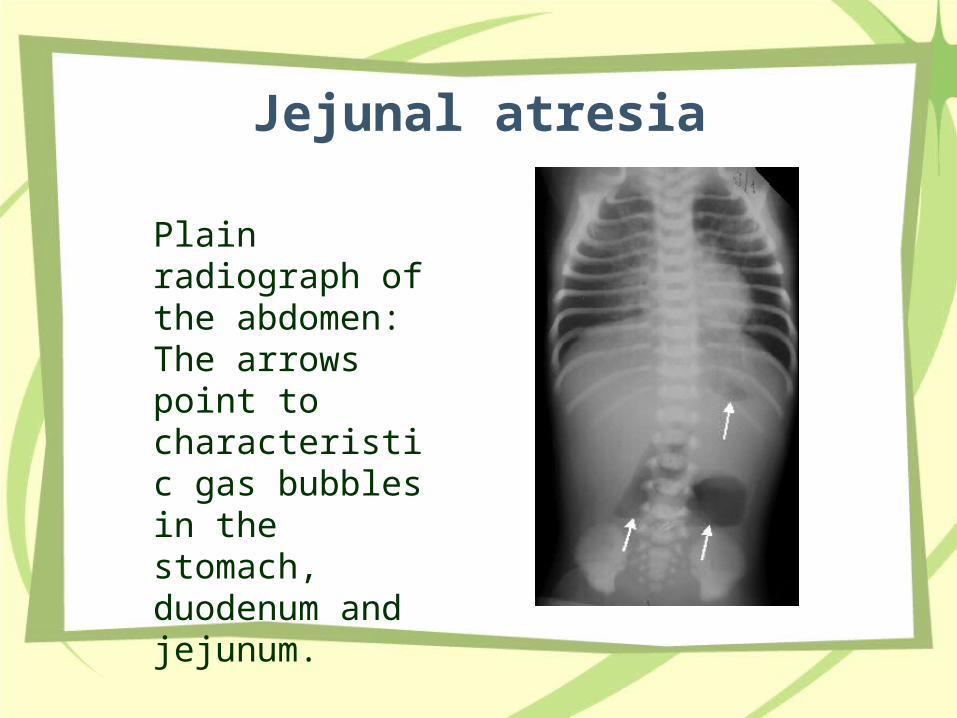
Jejunal atresia
Plain radiograph of the abdomen: The arrows point to characteristic gas bubbles in the stomach, duodenum and jejunum.
CASE 5
Hirschsprung Disease
• Synonyms and related keywords: congenital megacolon, aganglionic megacolon, aganglionosis, HD
• HD is characterized by the absence of myenteric and submucosal ganglion cells in the distal alimentary tract. The disease results in decreased motility in the affected bowel segment.
Clinical Details:Newborns with HD come to medical attention with the
following symptoms: • Failure to pass meconium within the first 48 hours of life • Abdominal distension that is relieved by rectal
stimulation or enemas • Vomiting • Neonatal enterocolitis
Symptoms in older children and adults include thefollowing: • Severe constipation • Abdominal distension • Bilious vomiting • Failure to thrive
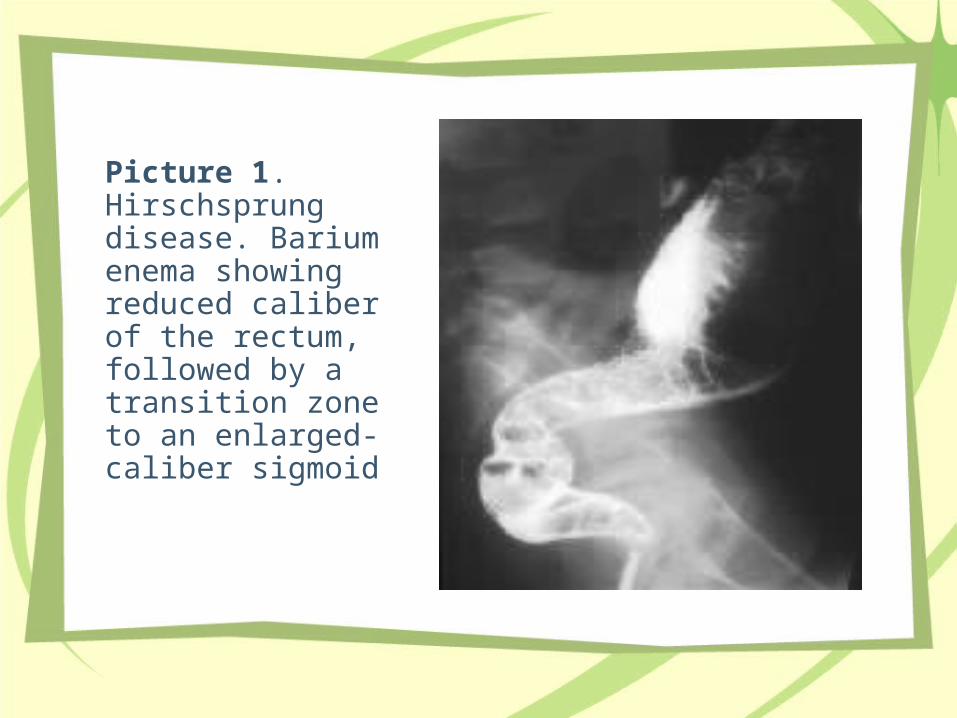
Picture 1. Hirschsprung disease. Barium enema showing reduced caliber of the rectum, followed by a transition zone to an enlarged-caliber sigmoid
•
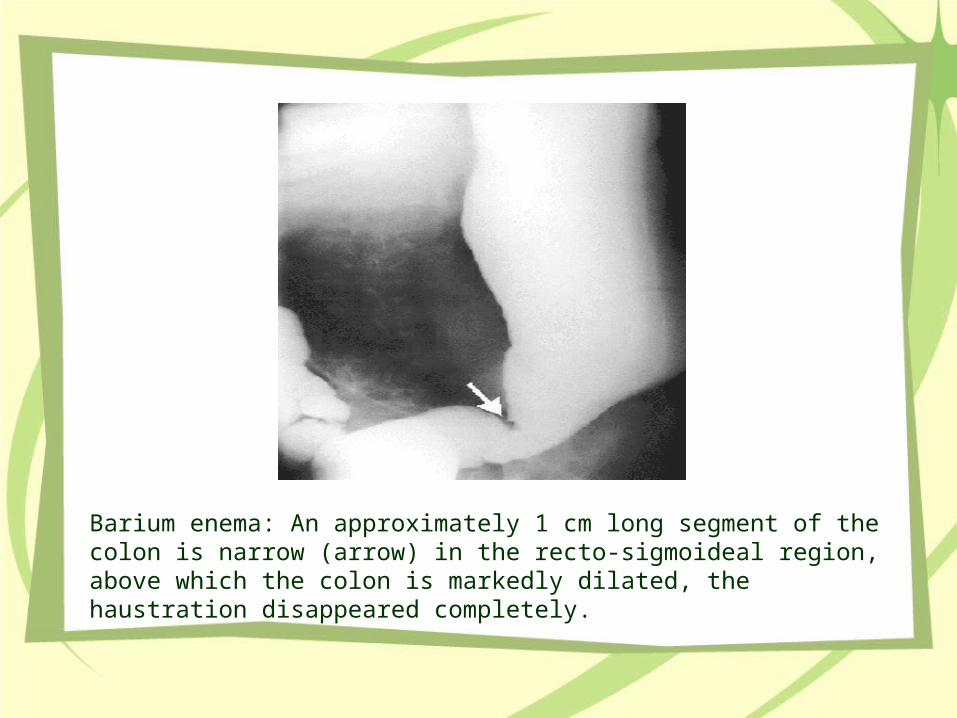
Barium enema: An approximately 1 cm long segment of the colon is narrow (arrow) in the recto-sigmoideal region, above which the colon is markedly dilated, the haustration disappeared completely.
•
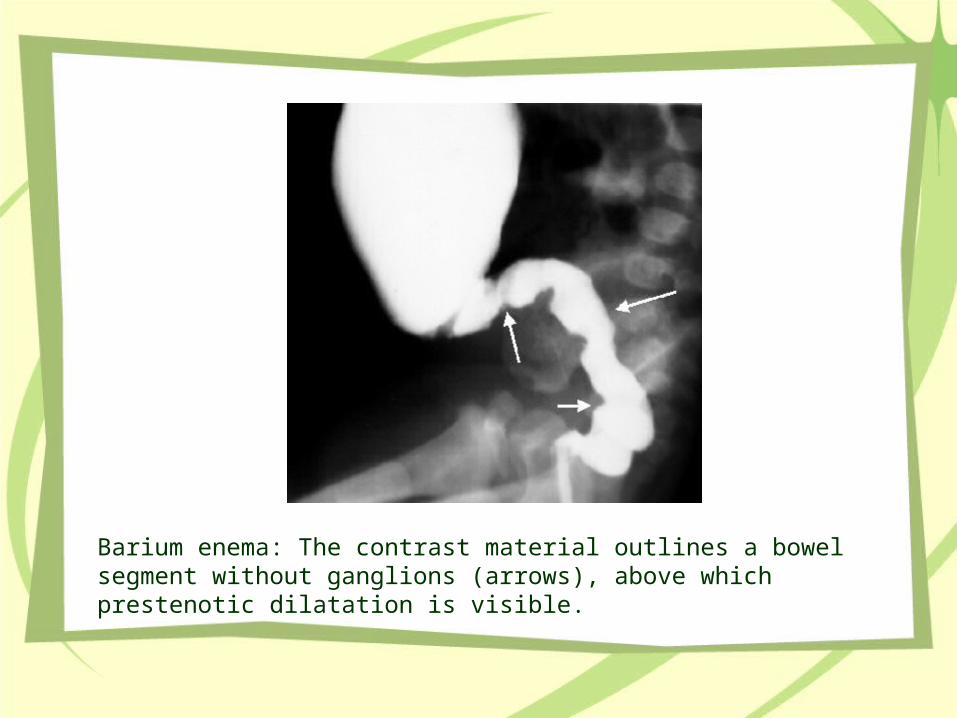
Barium enema: The contrast material outlines a bowel segment without ganglions (arrows), above which prestenotic dilatation is visible.
CASE 6
Intussusception
• Invagination of a bowel segment (usually small bowel) into the lumen of the more distal bowel (usually colon) occurs
• Venous congestion is a major factor both in symptomatology and in the characteristic presence of blood in the stool.
Clinical Details
Most intussusceptions are acute andpresent in a well-nourished infant with
signsand symptoms of bowel obstruction asfollows: • Cramping abdominal pain • Poor feeding • Vomiting
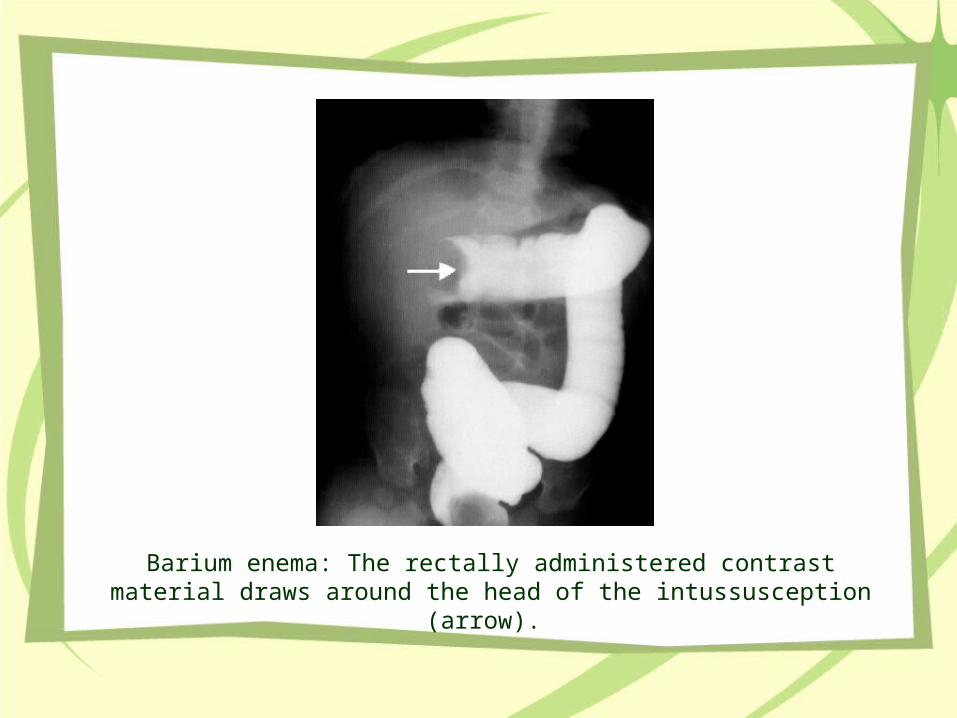
Barium enema: The rectally administered contrast material draws around the head of the intussusception (arrow).

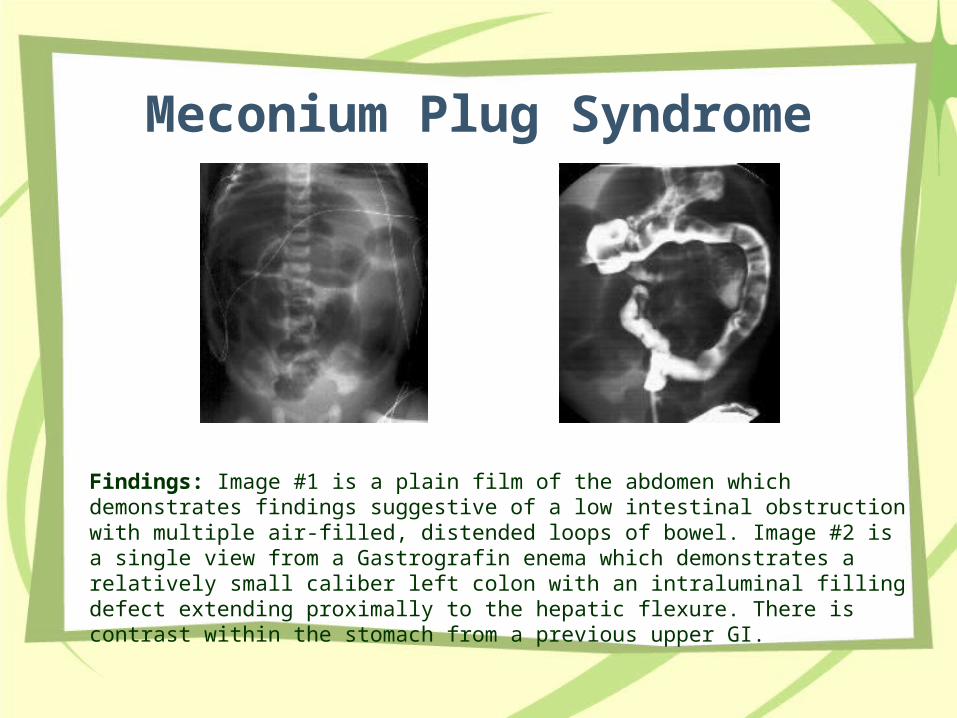
Meconium Plug Syndrome
Findings: Image #1 is a plain film of the abdomen which demonstrates findings suggestive of a low intestinal obstruction with multiple air-filled, distended loops of bowel. Image #2 is a single view from a Gastrografin enema which demonstrates a relatively small caliber left colon with an intraluminal filling defect extending proximally to the hepatic flexure. There is contrast within the stomach from a previous upper GI.
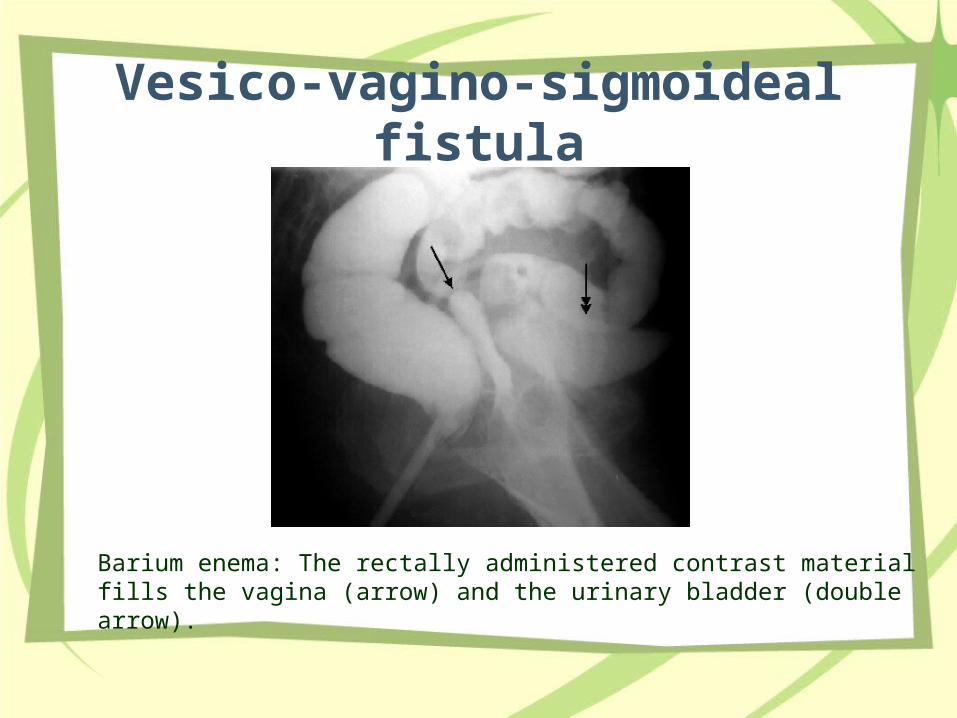
Vesico-vagino-sigmoideal fistula
•
Barium enema: The rectally administered contrast material fills the vagina (arrow) and the urinary bladder (double arrow).
…………… terima kasih
Recommended