American Journal of Medical Genetics 120A:289–291 (2003)
Research Letter
Re-Evaluation of Kyphomelic Dysplasia
To the Editor:
The heterogeneity of kyphomelic syndromes has beenalready suggested by Cisarik et al. [1999] and severalother authors. The Internationnal Nomenclature ofSkeletal Dysplasia committee has considered, duringthe last meeting, that this entity was too confusing to beincluded in the new classification [Hall et al., 2002].However, before concluding that there is real hetero-geneity in cases reported so far under this name, itwould be necessary to exclude all misdiagnosis.
When a new entity is described, it is tempting to de-scribe as a same disease, cases presenting with similarfeatures, but which are clearly distinct. There areseveral examples in the skeletal dysplasia field, asin the spectrum of ateleosteogenesis or of congenitalbowing of the limbs. In this last group, campomelic dy-splasia has been often over-diagnosed. Indeed, severalcaseswith short and stubby limbshave been proposed ascampomelic dysplasia although the thin aspect of thelong bones seems to be a major distinctive feature in theoriginal description [Khajavi et al., 1976].
On the other hand, kyphomelic dysplasia was definedby Maclean et al. [1983] as a bent-bone dysplasia butwith short and stubby long bones. For a time, cases withshortened, stubby, and bowed long bones were gatheredunder this term.However after a reviewof the publishedcases, some cases are clearly other distinct chondrodys-plasias. Three syndromes have to be recognized and notconfused.
The first one is the Schwartz–Jampel syndrome:Spranger et al. [2000] drew the attention to this con-fusion and showed that the previous case described byMaclean et al. [1983] resembled to Schwartz–Jampelsyndrome as demonstrated by the photographs.
The second misdiagnosis could be the Stuve–Wiedeman syndrome which was also described as asevere form of Schwartz–Jampel type II syndrome[Cormier-Daire et al., 1998; Superti-Furga et al., 1998].
The third type of confusion concerns the autosomalrecessive metaphyseal dysplasia McKusick type (carti-lage hair hypoplasia, CHH) [McKusick et al., 1965]. Theobservation described by Corder et al. [1995], withsevere combined immune defect, seemed to be a typicalexample of a neonatal form of CHH: the radiographsshowed a round aspect of the inferior femoral epiphysisand irregularities of the metaphyses. This aspect wasalready described under the name of Glasgow syndrome[Connor et al., 1985] or dysplasia with round epiphyses[Maroteaux et al., 1988]. All these descriptions havebeen demonstrated as being, in fact, severe CHH[Turnpenny et al., 1990; Le Merrer and Maroteaux,1991].
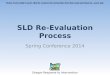
We report here a girl, observed at birth, with meta-physeal abnormalities and shortened and bowed longbones (Fig. 1a). At 9 years of age, she was very short(92 cm, �6 SD) and had low levels of IgA and severalcurrent infections. The hair was blond but normal. Theradiographs were suggestive of CHH: during growth,the bowing of the long bones disappeared progressively,the metaphyseal irregularities were very mild on the
Fig. 1. Case 1, a: Lower limbs at 6months: note the round distal femoralepiphyses, the shortening and bowing of the long bones, with mildmetaphyseal flaring. b: Hands at 9-years-old: note the short phalangesand the metaphyseal widening of the phalanges and the radius. c: Lowerlimbs at 9-years-old: note the mild coxa vara, the irregularities of themetaphyses specially on the knee.
*Correspondence to: Dr. Martine Le Merrer, INSERM U 393,Departement de Genetique, Hopital Necker-Enfants Malades,149, rue de Sevres, 75015 Paris, France.E-mail: [email protected]
Received 23 July 2002; Accepted 2 December 2002
DOI 10.1002/ajmg.a.20035
� 2003 Wiley-Liss, Inc.

femoral neck whereas the radiological aspect of thehand (Fig. 1b) and the knee (Fig. 1c), and the mildimmunological defect confirmed this diagnosis. Unfor-tunately no DNA samples were available for testing theCHH gene.
We suggest, therefore, that all cases published askyphomelic dysplasia with metaphyseal abnormalities[Fryns et al., 1983; Rezza et al., 1984; O’Reilly and Hall,1994; Pallotta et al., 1999] need to be reevaluated and, ifit is possible, to be tested for Nrase MRP mutationsresponsible for CHH [Ridanpaa et al., 2001]. This mole-cular screening could be done also, in case 4 of Cisariket al. [1999], based on the clinical manifestation of thischild and the radiographic analysis at birth.
Nevertheless, after exclusion of all of the differentialdiagnosis of kyphomelic dysplasia, some patients withsevere bowing belong certainly to a separate entity,which should be still called by this name.
We report here another child seen soon after birth,first child of healthy and consanguineous parents. Thelength was 41 cm, and the weight was 2680 g. This girlhad a flat face, a high forehead, and a severemicromelia(photographs of the patient are unavailable). Theproximal segment was extremely short with clinicallyangulation of the femora. Jointmovements were limitedwith multiple webs. The elbows were clenched.
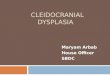
The radiographs showed very stubby femora, whichwere extremely curved. The iliac wings were short andwidened; the acetabular roof was completely horizontaland the iliac anglewas closed (Fig. 2a). The humeriwerealso short and had a dumbbell shape (Fig. 2b). Withtime, she grew slowly (at 10 years, her heightwas 99 cm,�6 SD), the angulation of the femora regressed, but theapexof the femora ’s curvewereasymmetric. Thegrowthof the tibia was also asymmetric (Fig. 2c). Her psycho-
motor development was quite normal. Chromosomalexamination was normal.
The case 3 published by Cisarik et al. [1999] isextremely similar, and case 1 and 2 of the same pub-lication belong probably to the same entity aswell as thecase reported by Temple et al. [1989]. We suggest thatthe severity of the major angulation of the femora is theclue for the diagnosis of this type of chondrodysplasia.Anautosomal recessivemodeof inheritance seems likelybased on the consanguinity observed in our case.
Finally, several other reports in the literature[Khajavi et al., 1976; Hall and Spranger, 1979] arecompletely distinct from the four entities presentedhere. Further observations with a long term follow upwill be helpful for a better delineation of the group ofbent-bone chondrodysplasias.
REFERENCES
Cisarik F, Koslowski K,Masel J, Sillence D. 1999. Variability in kyphomelicdysplasia. Pediatr Radiol 29:551–557.
Connor JM, Connor RAC, Sweet EM, Gibson AAM, Patrick WJA,McNay MB, Redford DHA. 1985. Lethal neonatal chondrodysplasias inthe west of Scotland 1970–1983 with a description of a thanatophoric,dysplasia like, autosomal recessive disorder,Glasgowvariant.AmJMedGenet 22:243–253.
Corder WT, Hummel M, Miller C, Wilson NW. 1995. Association of kypho-melic dysplasia with severe combined immunodeficiency. Am J MedGenet 57:626–629.
Cormier-Daire V, Superti-Furga A, Munnich A, Lyonnet S, Rustin P,Delezoide AL, De Lonlay P, Giedion A,Maroteaux P, LeMerrerM. 1998.Clinical homogeneity of the Stuve–Wiedemann syndrome and overlapwith the Schwartz–Jampel syndrome type 2. Am J Med Genet 78:146–149.
Fryns JP, Annicq P, UlrixM, van den Berghe H. 1983. Congenital bowing ofthe long bones. Acta Paediatr Scand 72:789–791.
Hall CM, The international nomenclature Group on ConstitutionalDisorders of Bone. 2002. International nosology and classification ofconstitutional disorders of bone, 2001. Am J Med Genet 113:65–77.
Hall BD, Spranger JW. 1979. Familial congenital bowing with short bones.Radiology 132:611–614.
Khajavi A, Lachman R, Rimoin D, Schmike N, Dorst J, Handemaker S,Ebbi A, Pereault G. 1976. Heterogeneity in the camptomelic syndromes:Long and short bone varieties. Radiology 120:641–647.
Le Merrer M, Maroteaux P. 1991. Cartilage hair hypoplasia in infancy: Amisleading chondrodysplasia. Eur J Pediat 150:847–851.
Maclean RN, Prater WK, Lozzio CB. 1983. Skeletal dysplasia with short,angulated femora (kyphomelic dysplasia). Am J Med Genet 14:373–380.
Maroteaux P, Stanescu R, Stanescu V, Cousin J. 1988. Recessive lethalchondrodysplasia ‘‘round femoral inferior epiphysis type.’’ Eur J Pediatr147:408–411.
McKusick VA, Eldridge R, Hostetler JA, Egeland JA, Ruangwit U. 1965.Dwarfism in the amish. II. Cartilage-hair hypoplasia. Bull JohnsHopkins Hosp 116:285–326.
O’Reilly MAR, Hall CM. 1994. Kyphomelic dysplasia. (Letter) J Med Genet31:423–427.
PallottaR,EhresmanT,RogginiMM,Fusilli P. 1999.Kyphomelic dysplasia:Clinical and radiologic long-term follow-up of one case and review of theliterature. Radiology 212:847–852.
Rezza E, Iannaccone G, Lendvai D. 1984. Familial congenital bowing withshort thick bones and metaphyseal changes, a distinct entity: Report ofthe clinical and radiological findings in two siblings. Pediatr Radiol14:323–327.
Ridanpaa M, van Eenennaam H, Pelin K, Chadwick R, Johnson C, Yuan B,vanVenrooijW,PruijnG, SalmelaR, Rockas S,MakitieO,Kaitila I, de laChapelleA. 2001.Mutations in theRNAcomponent ofRNaseMRPcausea pleiotropic human disease, cartilage-hair hypoplasia. Cell 104:195–203.
Fig. 2. Case 2, a: Lower limbs at birth: note the spread iliac wings andthe short, stubby, and strongly curved femora. The metaphyses of the tibiaareflaredwhereas the diaphyse is straight.b: Upper limbs at birth: enlargeddistal part of the humeri, flared metaphyses of the long bones, shortmetacarpals. c: Lower limbs at 12-years-old: curved and asymmetric femoraenlargedmetaphyses and irregular shaft of thediaphyses of the tibia and thefibula.
290 Le Merrer et al.

Spranger J, Hall BD, Hane B, Srivastava A, Stevenson RE. 2000. Spectrumof Schwartz–Jampel syndrome includes micromelic chondrodysplasia,kyphomelic dysplasia, and Burton disease. Am J Med Genet 94:287–295.
Superti-FurgaA, Tenconi R,ClementiM,EichG, SteinmannB,BoltshauserE, Giedion A. 1998. Schwartz–Jampel syndrome type 2 and Stuve–Wiedemann syndrome: A case for ‘‘lumping.’’ Am J Med Genet 78:150–154.
Temple IK, Thompson EM, Hall CM, Bridgeman G, Pembrey ME. 1989.Kyphomelic dysplasia. J Med Genet 26:457–468.
Turnpenny PD, Dakwar RA, Boulos FN. 1990. Kyphomelic dysplasia: Thefirst 10 cases. J Med Genet 27:269–272.
Martine Le Merrer*Valerie Cormier DairePierre MaroteauxDepartement de Genetique et INSERM U393Hopital Necker Enfants MaladesParis, France
Research Letter 291
Recommended