www.mhh-unfallchirurgie.de 1 Unfallchirurgische Klinik www.mhh-unfallchirurgie.de Unfallchirurgische Klinik
Schulter im Seniorenalter Proximale Humerus Fraktur
weniger Komplikationen mit weniger Geld? C. Krettek,
U. Wiebking, N. Hawi
www.mhh-unfallchirurgie.de 2 Unfallchirurgische Klinik
Disclaimer / Conflict of Interrest
Co-Editor Skeletal Trauma (Elsevier)
Associate Editor J Bone Joint Surgery
Leitthemenherausgeber Der Unfallchirurg (Springer)
Medizinischer Leiter OTUpdate (medUpdate)
www.mhh-unfallchirurgie.de 3 Unfallchirurgische Klinik
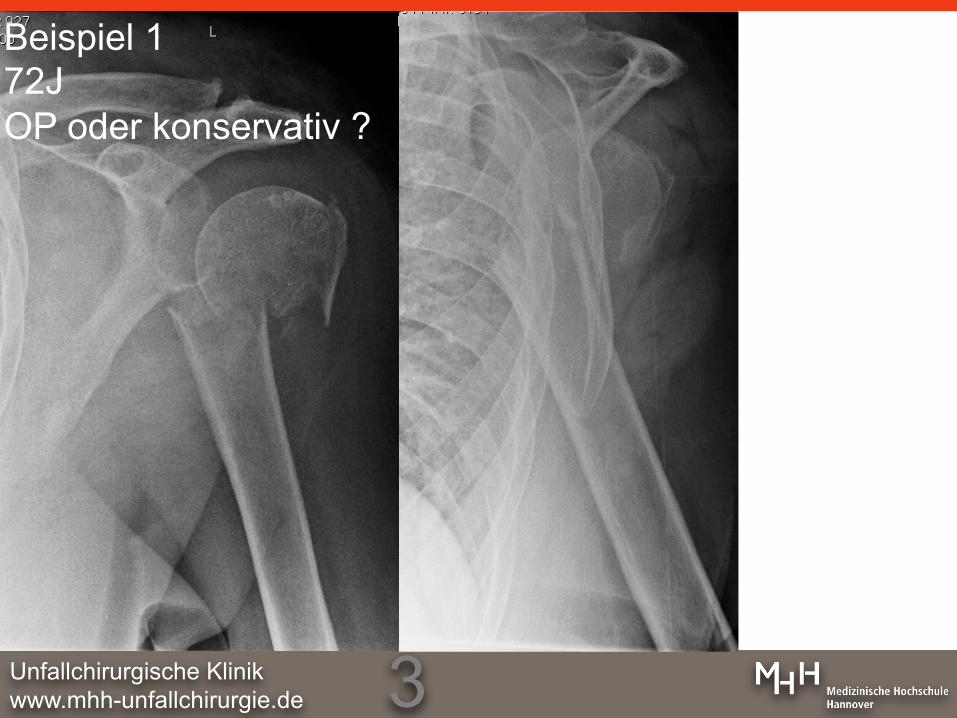
Beispiel 1 72J OP oder konservativ ?

www.mhh-unfallchirurgie.de 4 Unfallchirurgische Klinik
Beispiel 2 58J OP oder konservativ ?

www.mhh-unfallchirurgie.de 5 Unfallchirurgische Klinik
Beispiel 3 NN, > 60J OP oder konservativ ?

www.mhh-unfallchirurgie.de 6 Unfallchirurgische Klinik
Beispiel 1 72J OP oder konservativ ?
4.4.2011
11.4.2011 3.12.2012

www.mhh-unfallchirurgie.de 7 Unfallchirurgische Klinik
auswärts OP Empfehlung
Beispiel 2 58 y B1-2 Neer III.3
6W 3M Constant Score 56
after reduction

www.mhh-unfallchirurgie.de 8 Unfallchirurgische Klinik www.mhh-unfallchirurgie.de Unfallchirurgische Klinik
Beispiel 3 NN, > 60J OP oder konservativ ?
www.mhh-unfallchirurgie.de 9 Unfallchirurgische Klinik
• sensibilisieren • Studienlage • Behandlungsrealität in Deutschland • MHH Behandlungsalgorithmus • offene Fragen
www.mhh-unfallchirurgie.de 10 Unfallchirurgische Klinik
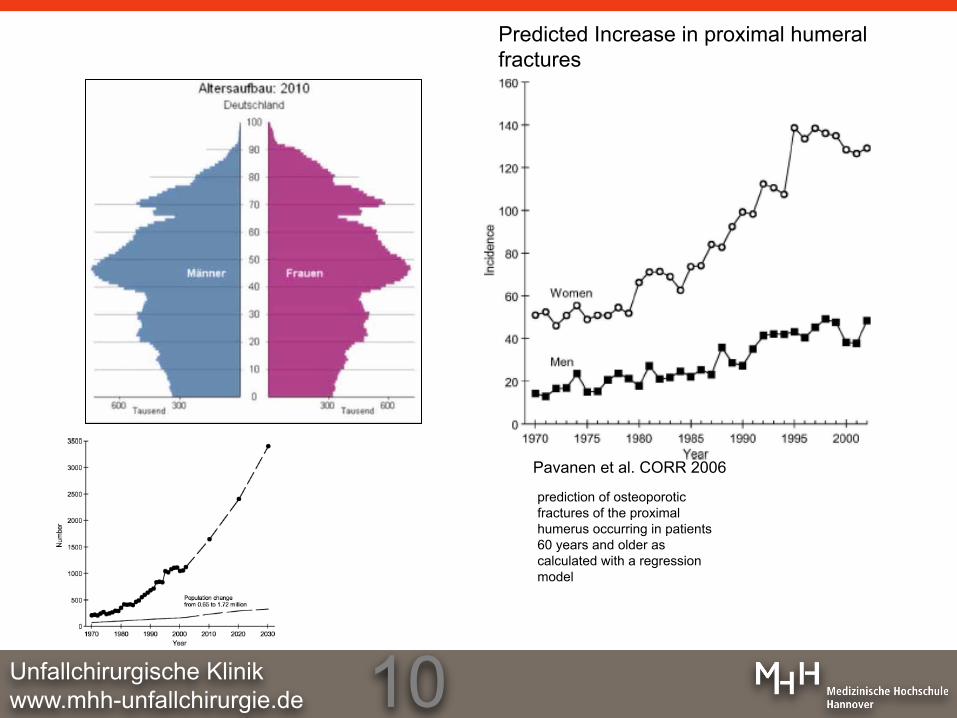
prediction of osteoporotic fractures of the proximal humerus occurring in patients 60 years and older as calculated with a regression model
Pavanen et al. CORR 2006
Predicted Increase in proximal humeral fractures
age-adjusted incidence (per 100,000individuals) of hospital treated osteoporotic fractures of the proximal humerus in patients 60 years and older.
Predicted Increase in proximal humeral fractures
www.mhh-unfallchirurgie.de 11 Unfallchirurgische Klinik
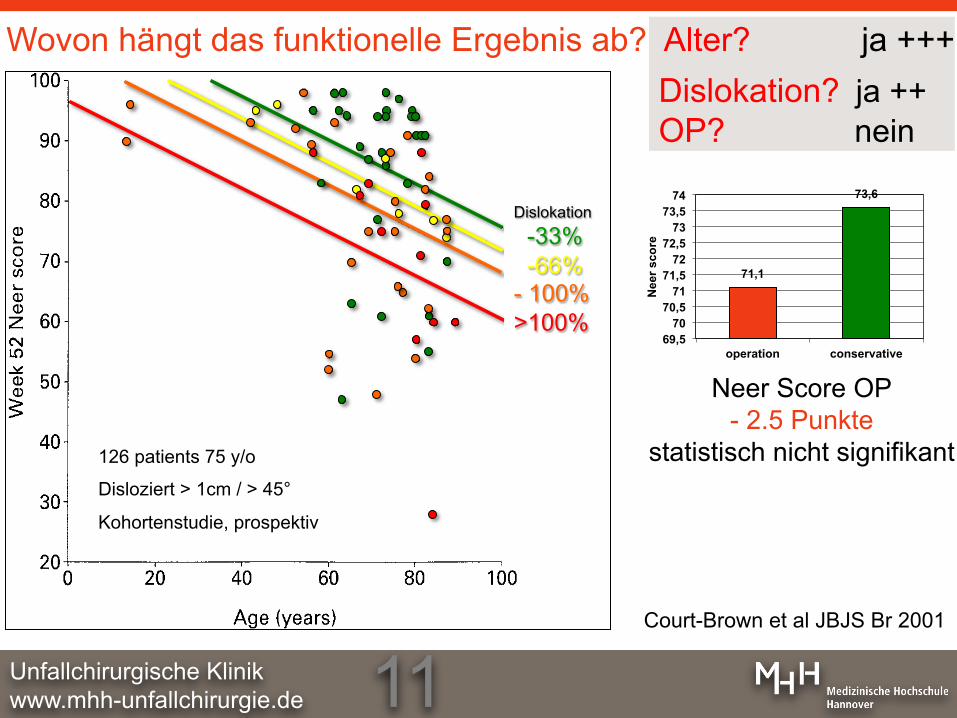
Dislokation? ja ++ OP? nein
Wovon hängt das funktionelle Ergebnis ab? Alter? ja +++
126 patients 75 y/o
Disloziert > 1cm / > 45°
Kohortenstudie, prospektiv
71,1
73,6
69,5 70
70,5 71
71,5 72
72,5 73
73,5 74
operation conservative
Nee
r sco
re
Neer Score OP - 2.5 Punkte
statistisch nicht signifikant
Court-Brown et al JBJS Br 2001
Dislokation
-33% -66% - 100% >100%
www.mhh-unfallchirurgie.de 12 Unfallchirurgische Klinik
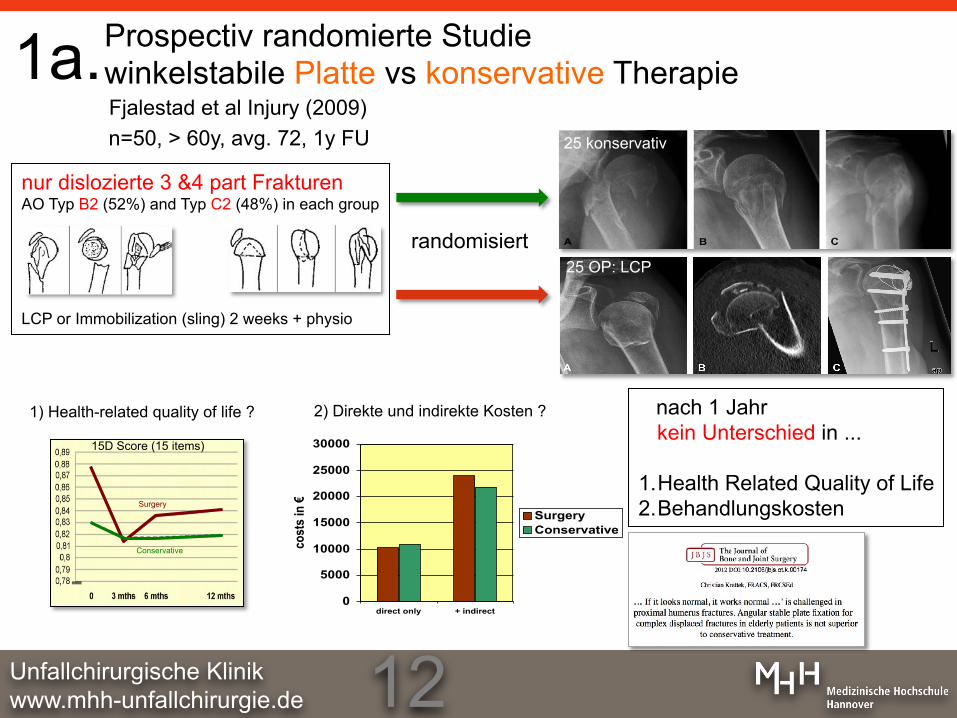
nur dislozierte 3 &4 part Frakturen AO Typ B2 (52%) and Typ C2 (48%) in each group
LCP or Immobilization (sling) 2 weeks + physio
Fjalestad et al Injury (2009) n=50, > 60y, avg. 72, 1y FU
nach 1 Jahr kein Unterschied in ...
1. Health Related Quality of Life 2. Behandlungskosten
0
5000
10000
15000
20000
25000
30000
direct only + indirect
cost
s in
€
SurgeryConservative
Prospectiv randomierte Studie winkelstabile Platte vs konservative Therapie
2) Direkte und indirekte Kosten ? 1) Health-related quality of life ?
25 OP: LCP
25 konservativ
randomisiert
Surgery
Conservative
15D Score (15 items)
1a.
www.mhh-unfallchirurgie.de 13 Unfallchirurgische Klinik
OP
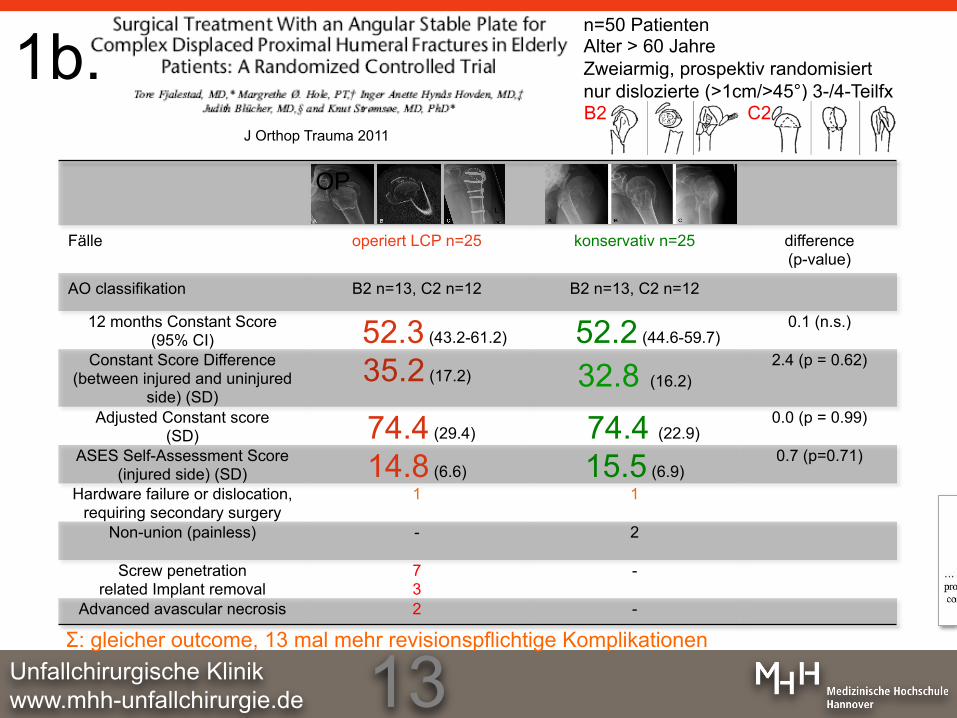
Fälle operiert LCP n=25 konservativ n=25 difference (p-value)
AO classifikation B2 n=13, C2 n=12 B2 n=13, C2 n=12
12 months Constant Score (95% CI) 52.3 (43.2-61.2) 52.2 (44.6-59.7)
0.1 (n.s.)
Constant Score Difference (between injured and uninjured
side) (SD) 35.2 (17.2) 32.8 (16.2)
2.4 (p = 0.62)
Adjusted Constant score (SD) 74.4 (29.4) 74.4 (22.9)
0.0 (p = 0.99)
ASES Self-Assessment Score (injured side) (SD) 14.8 (6.6) 15.5 (6.9)
0.7 (p=0.71)
Hardware failure or dislocation, requiring secondary surgery
1 1
Non-union (painless) - 2
Screw penetration related Implant removal
7 3
-
Advanced avascular necrosis 2 -
n=50 Patienten Alter > 60 Jahre Zweiarmig, prospektiv randomisiert nur dislozierte (>1cm/>45°) 3-/4-Teilfx
J Orthop Trauma 2011 B2 C2
1b.
Σ: gleicher outcome, 13 mal mehr revisionspflichtige Komplikationen
www.mhh-unfallchirurgie.de 14 Unfallchirurgische Klinik
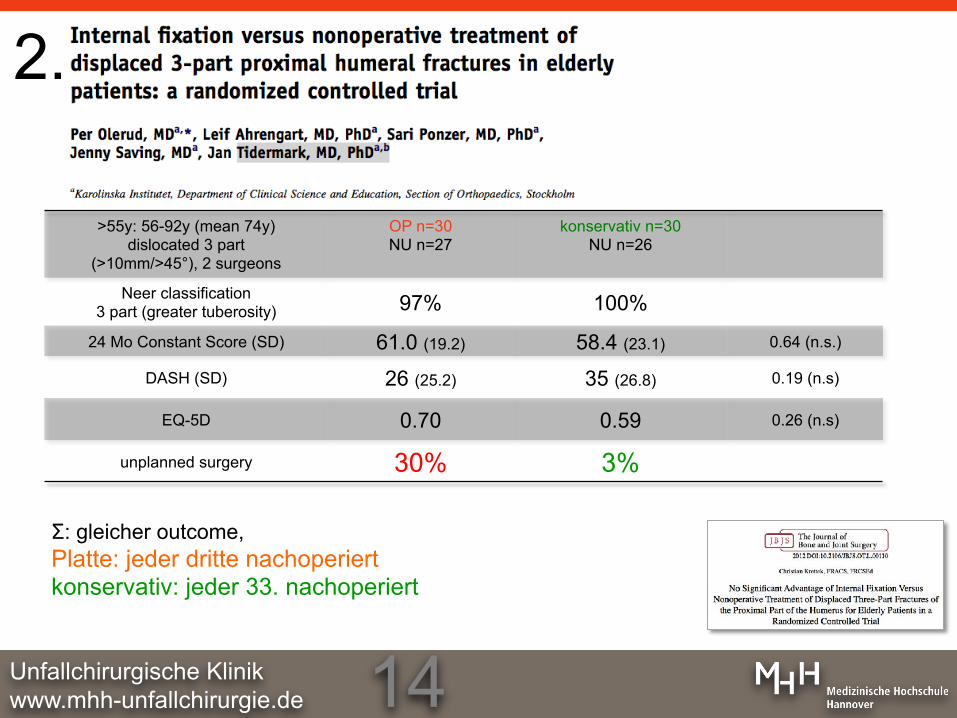
>55y: 56-92y (mean 74y) dislocated 3 part
(>10mm/>45°), 2 surgeons
OP n=30 NU n=27
konservativ n=30 NU n=26
Neer classification 3 part (greater tuberosity) 97% 100%
24 Mo Constant Score (SD) 61.0 (19.2) 58.4 (23.1) 0.64 (n.s.)
DASH (SD) 26 (25.2) 35 (26.8) 0.19 (n.s)
EQ-5D 0.70 0.59 0.26 (n.s)
unplanned surgery 30% 3%
2.
Σ: gleicher outcome, Platte: jeder dritte nachoperiert konservativ: jeder 33. nachoperiert
www.mhh-unfallchirurgie.de 15 Unfallchirurgische Klinik
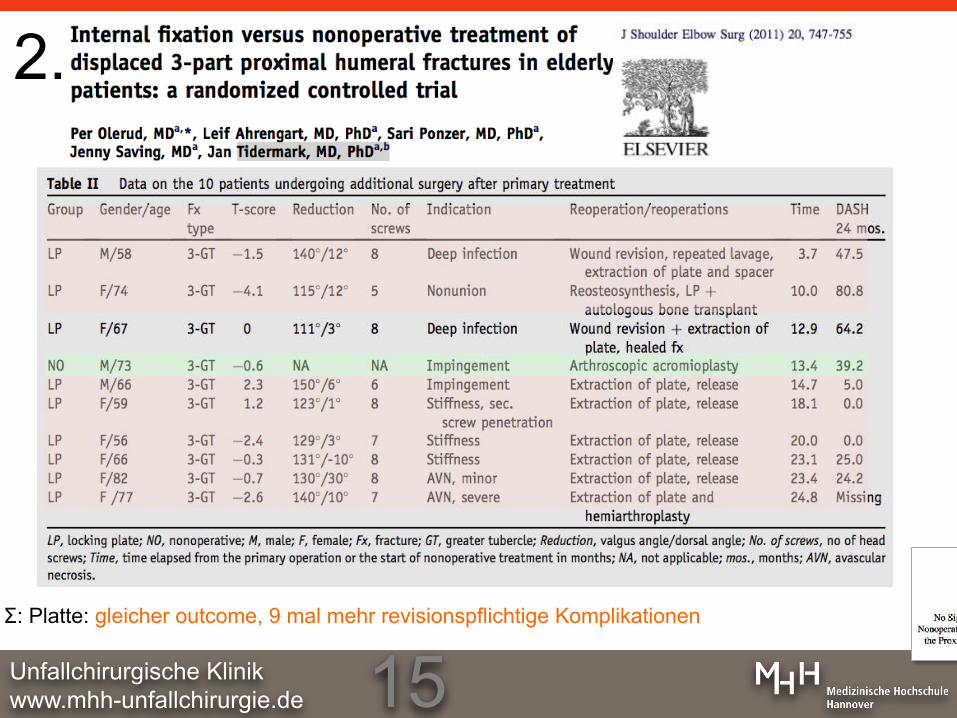
2.
Σ: Platte: gleicher outcome, 9 mal mehr revisionspflichtige Komplikationen
www.mhh-unfallchirurgie.de 16 Unfallchirurgische Klinik
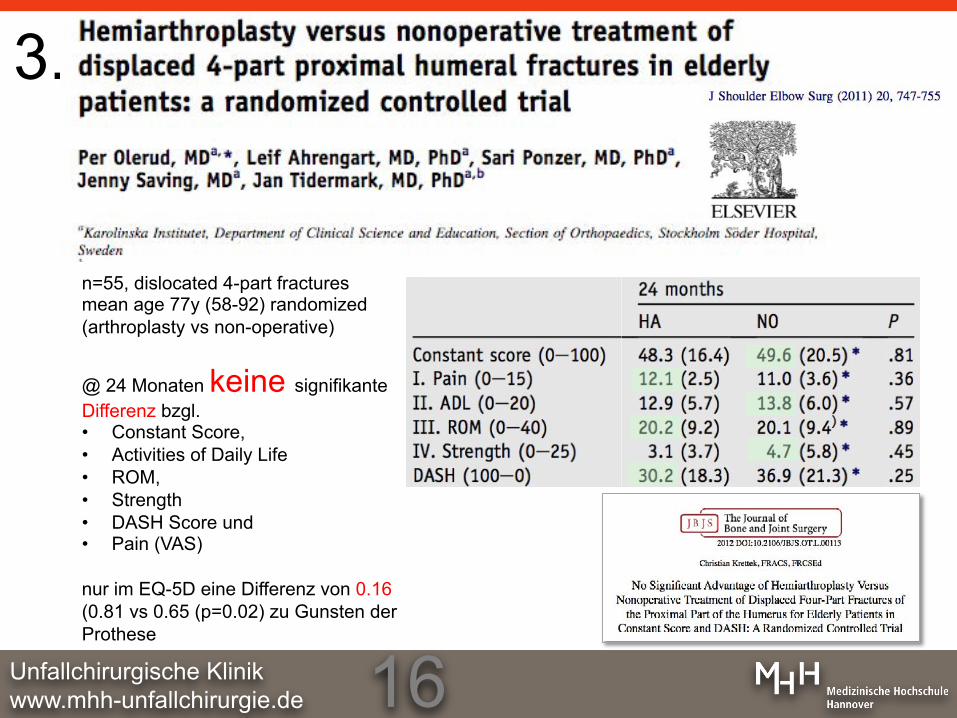
n=55, dislocated 4-part fractures mean age 77y (58-92) randomized (arthroplasty vs non-operative)
@ 24 Monaten keine signifikante Differenz bzgl. • Constant Score, • Activities of Daily Life • ROM, • Strength • DASH Score und • Pain (VAS)
nur im EQ-5D eine Differenz von 0.16 (0.81 vs 0.65 (p=0.02) zu Gunsten der Prothese
3.
www.mhh-unfallchirurgie.de 17 Unfallchirurgische Klinik
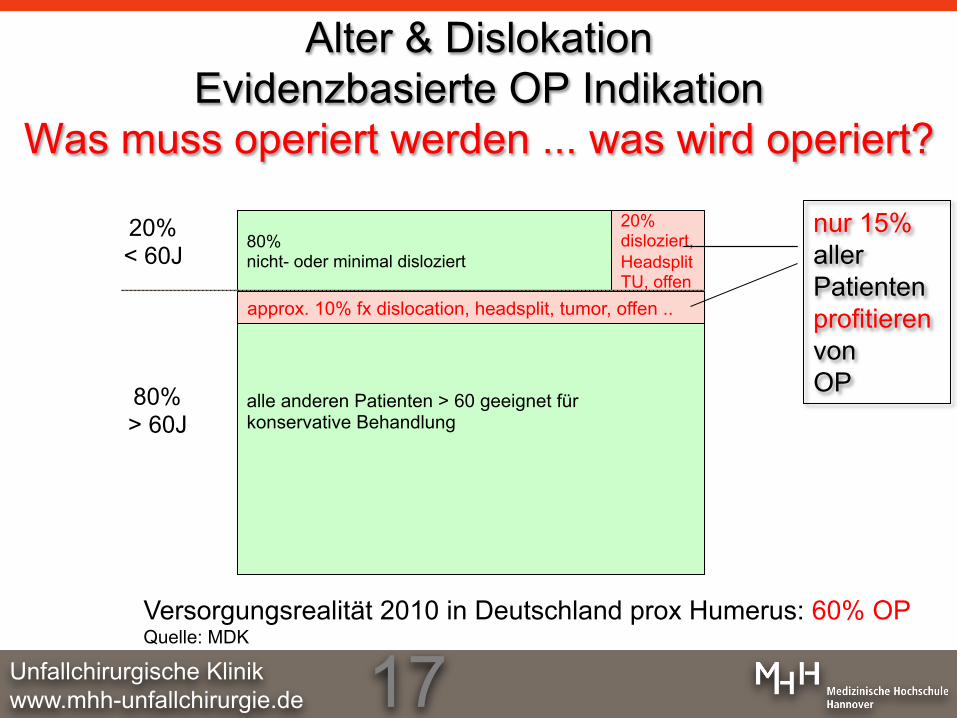
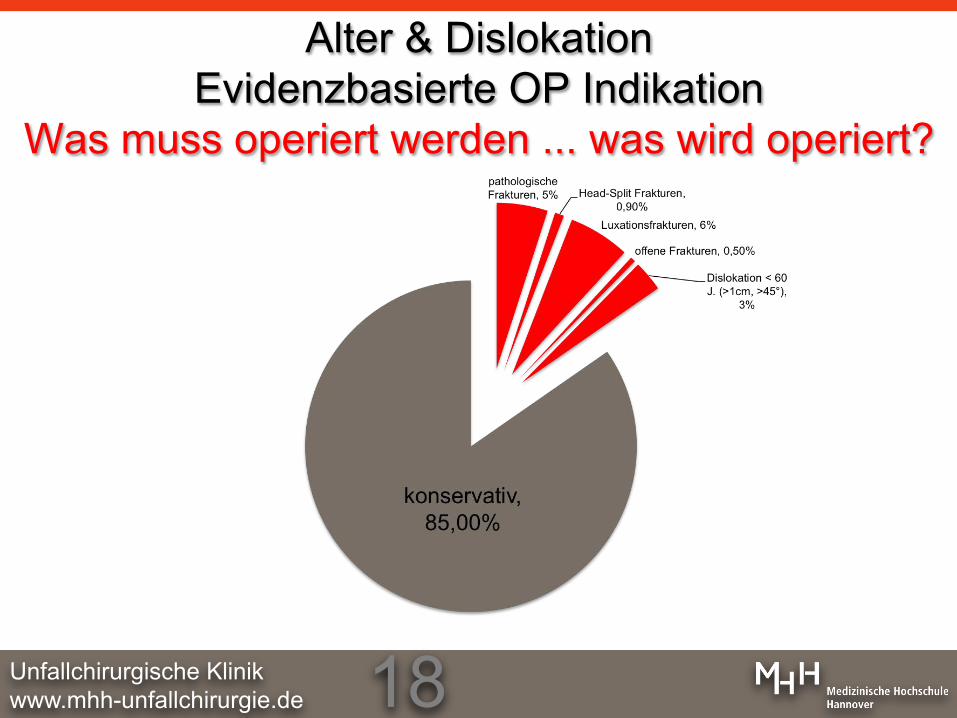
alle anderen Patienten > 60 geeignet für konservative Behandlung
80% nicht- oder minimal disloziert
approx. 10% fx dislocation, headsplit, tumor, offen ..
80% > 60J
20% < 60J
Alter & Dislokation Evidenzbasierte OP Indikation
Was muss operiert werden ... was wird operiert?
Versorgungsrealität 2010 in Deutschland prox Humerus: 60% OP Quelle: MDK
20% disloziert, HeadsplitTU, offen
nur 15% aller Patienten profitieren von OP
www.mhh-unfallchirurgie.de 18 Unfallchirurgische Klinik
Alter & Dislokation Evidenzbasierte OP Indikation
Was muss operiert werden ... was wird operiert?
www.mhh-unfallchirurgie.de 19 Unfallchirurgische Klinik
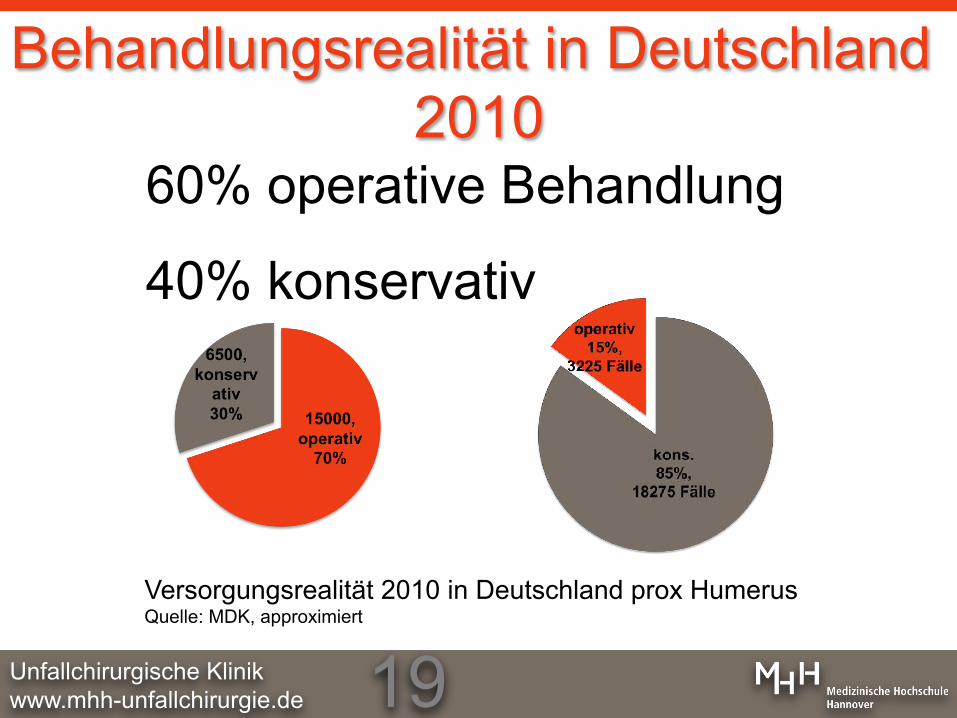
Behandlungsrealität in Deutschland 2010
60% operative Behandlung
40% konservativ
Versorgungsrealität 2010 in Deutschland prox Humerus Quelle: MDK, approximiert
www.mhh-unfallchirurgie.de 20 Unfallchirurgische Klinik
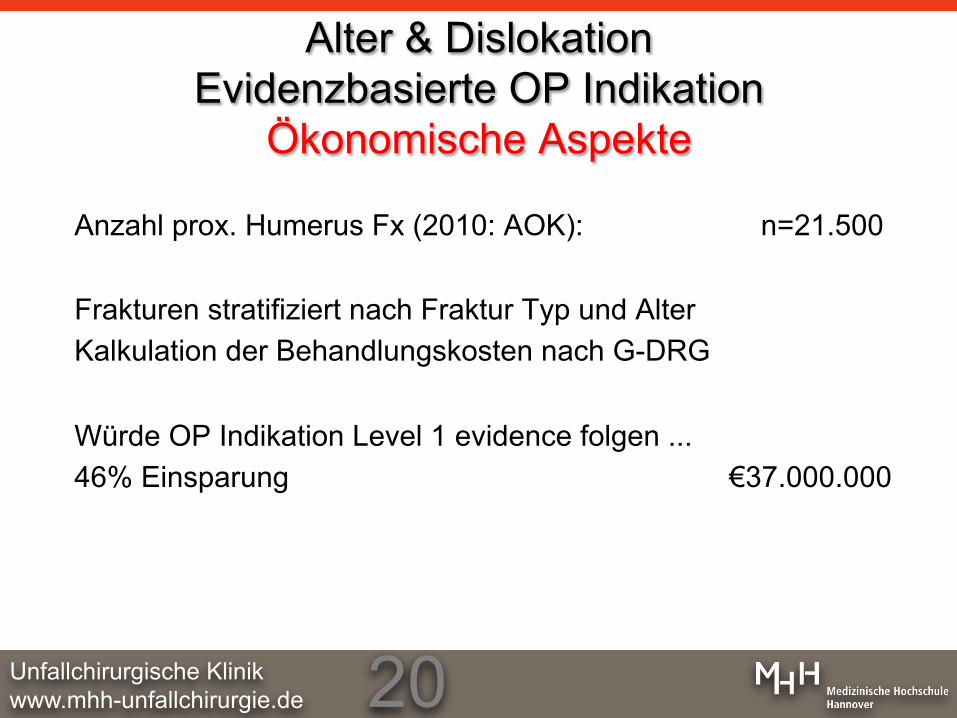
Anzahl prox. Humerus Fx (2010: AOK): n=21.500 Frakturen stratifiziert nach Fraktur Typ und Alter Kalkulation der Behandlungskosten nach G-DRG Würde OP Indikation Level 1 evidence folgen ... 46% Einsparung €37.000.000
conomic Aspects
Alter & Dislokation Evidenzbasierte OP Indikation
Ökonomische Aspekte

www.mhh-unfallchirurgie.de 21 Unfallchirurgische Klinik
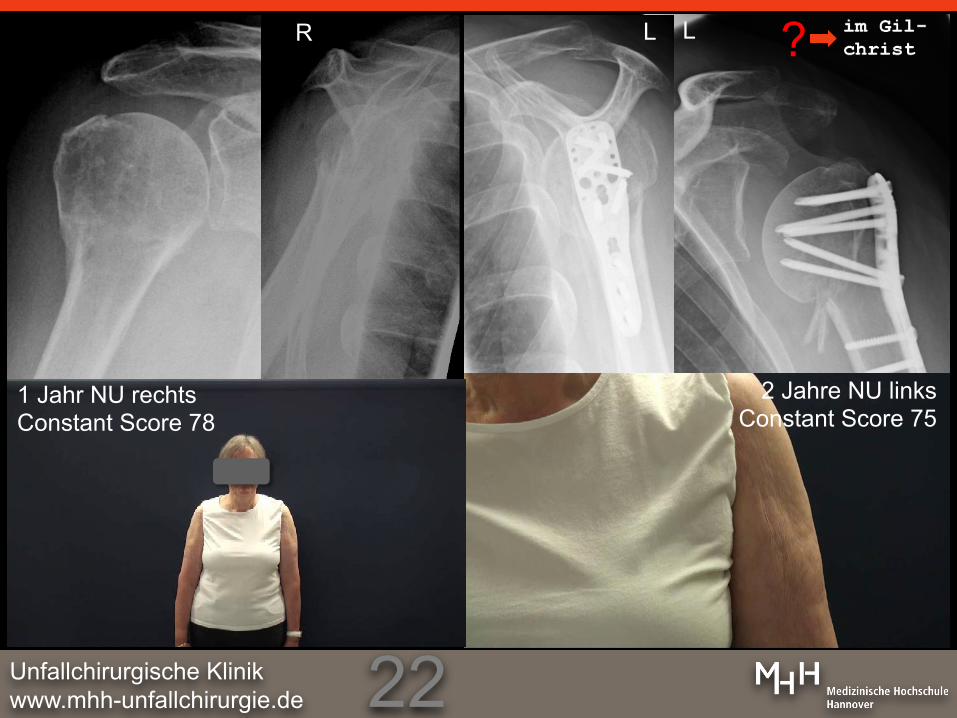
76 Jahre, weiblich AO B1 re, AO A3 links
R L L
eine Patientin, zwei Behandlungen eine Seite OP, die andere konservativ
wo?-was?
www.mhh-unfallchirurgie.de 22 Unfallchirurgische Klinik
R L L
2 Jahre NU links Constant Score 75
1 Jahr NU rechts Constant Score 78
?

www.mhh-unfallchirurgie.de 23 Unfallchirurgische Klinik
64y Rheumatoid arthritis AO 11 C2 Neer III.3

www.mhh-unfallchirurgie.de 24 Unfallchirurgische Klinik
64y Rheumatoid arthritis 2005: AO 11 C2 Neer III.3 2y Constant Score 74 2013: Dekompensation ... Prothese ... wie vorher
www.mhh-unfallchirurgie.de 25 Unfallchirurgische Klinik
Primär Prothese nach Trauma Revisionsrate 17%
Prothese nach Versagen kons. Therapie Revisionsrate 7% P. Habermeyer Schulterchirurgie, 2010 Elsevier, München
Prothese nach Versagen operativer Therapie ‚... massive Probleme ...‘ Gohlke Schulterkurs Tegernsee 2012
Optimal Timing for Total Shoulder Arthroplasty after Fracture ? Is secondary Arthroplasty really worse?
Hepp 2011 Frakturprothese auf dem Rückzug, inverse Prothese Ausnahme
www.mhh-unfallchirurgie.de 26 Unfallchirurgische Klinik
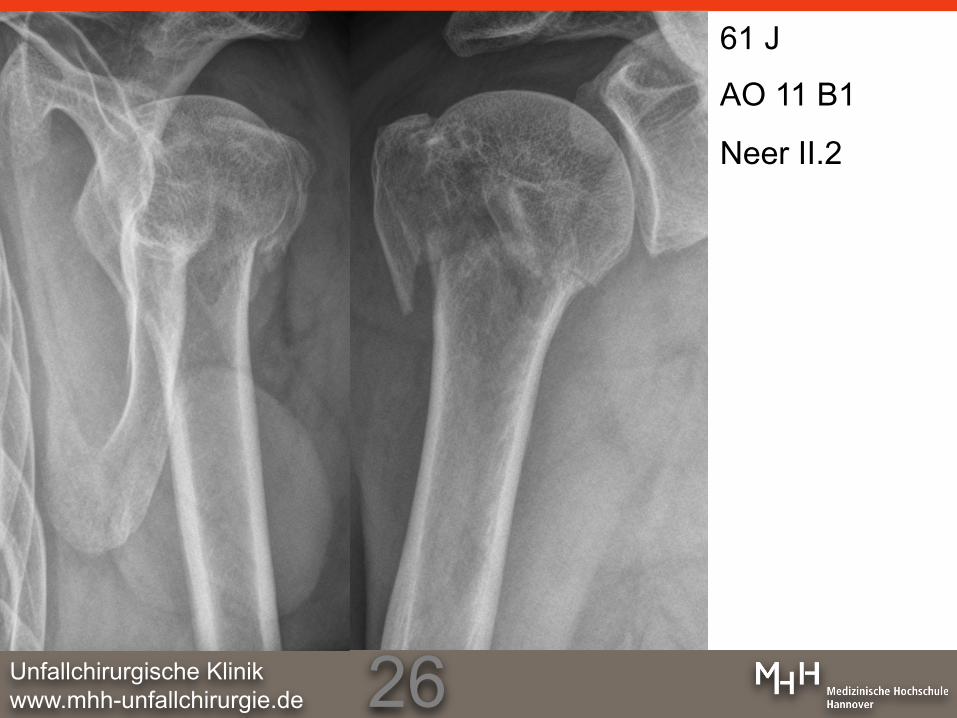
61 J
AO 11 B1
Neer II.2
www.mhh-unfallchirurgie.de 27 Unfallchirurgische Klinik
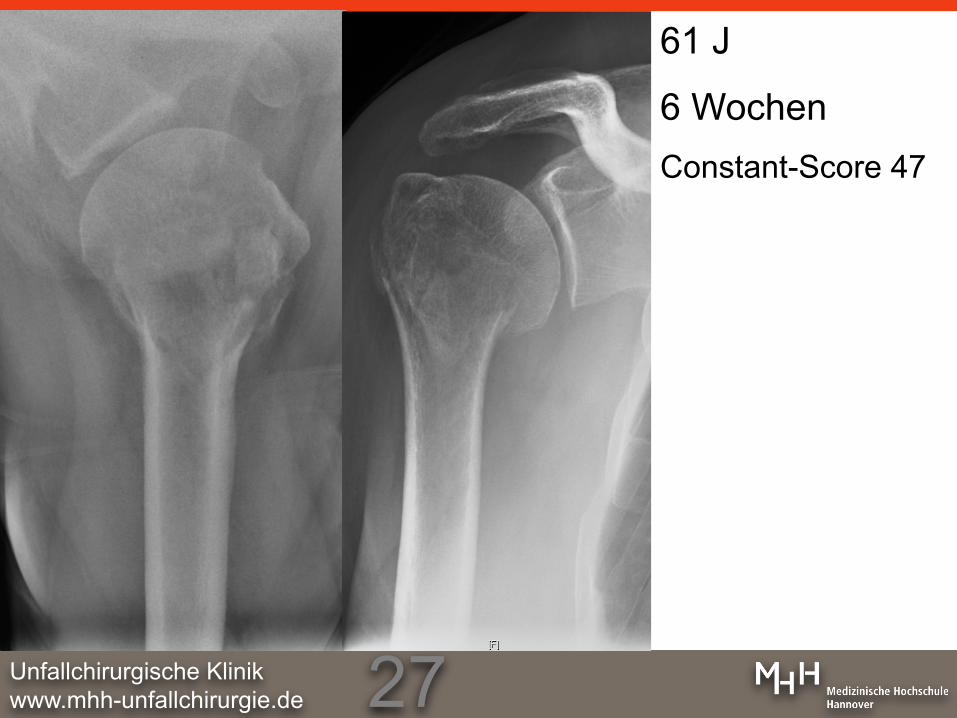
61 J
6 Wochen Constant-Score 47

www.mhh-unfallchirurgie.de 28 Unfallchirurgische Klinik
61 J, 3 Monate
Constant-Score 80
www.mhh-unfallchirurgie.de 29 Unfallchirurgische Klinik
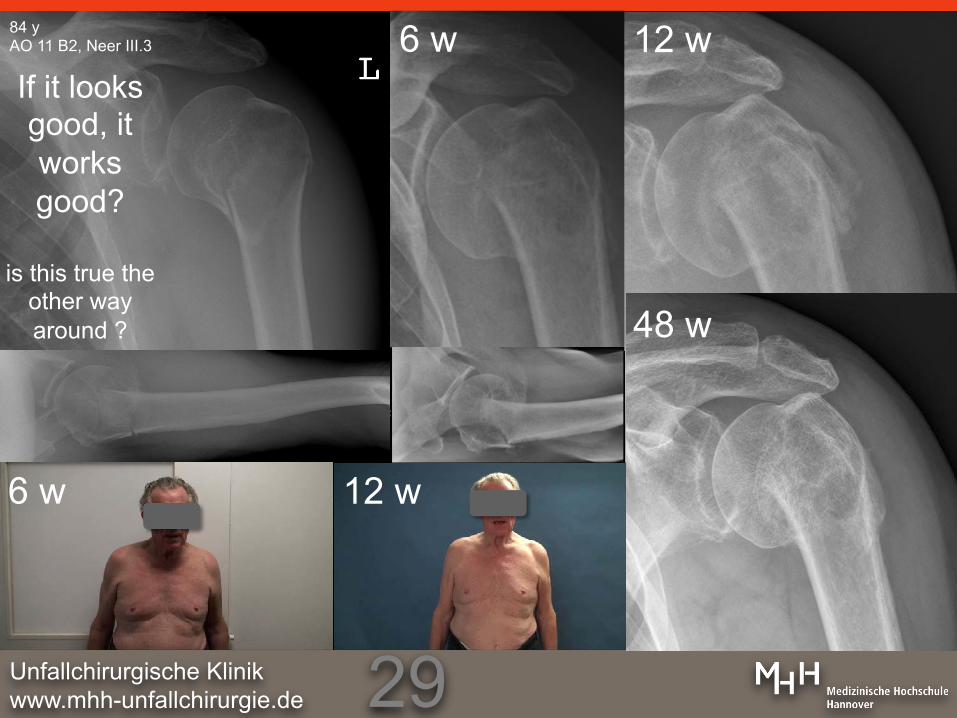
84 y AO 11 B2, Neer III.3 6 w
3M
If it looks good, it works good?
is this true the
other way around ?
6 w 12 w
12 w
48 w
www.mhh-unfallchirurgie.de 30 Unfallchirurgische Klinik
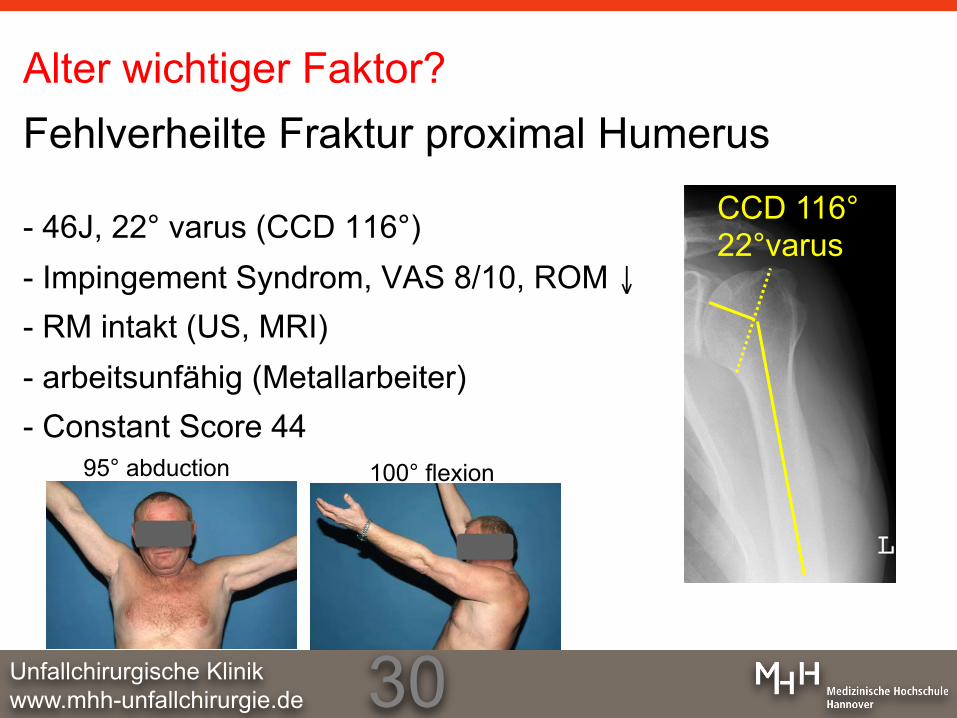
Alter wichtiger Faktor? Fehlverheilte Fraktur proximal Humerus
- 46J, 22° varus (CCD 116°) - Impingement Syndrom, VAS 8/10, ROM ↓ - RM intakt (US, MRI) - arbeitsunfähig (Metallarbeiter) - Constant Score 44
CCD 116° 22°varus
95° abduction 100° flexion
www.mhh-unfallchirurgie.de 31 Unfallchirurgische Klinik
www.mhh-unfallchirurgie.de 32 Unfallchirurgische Klinik
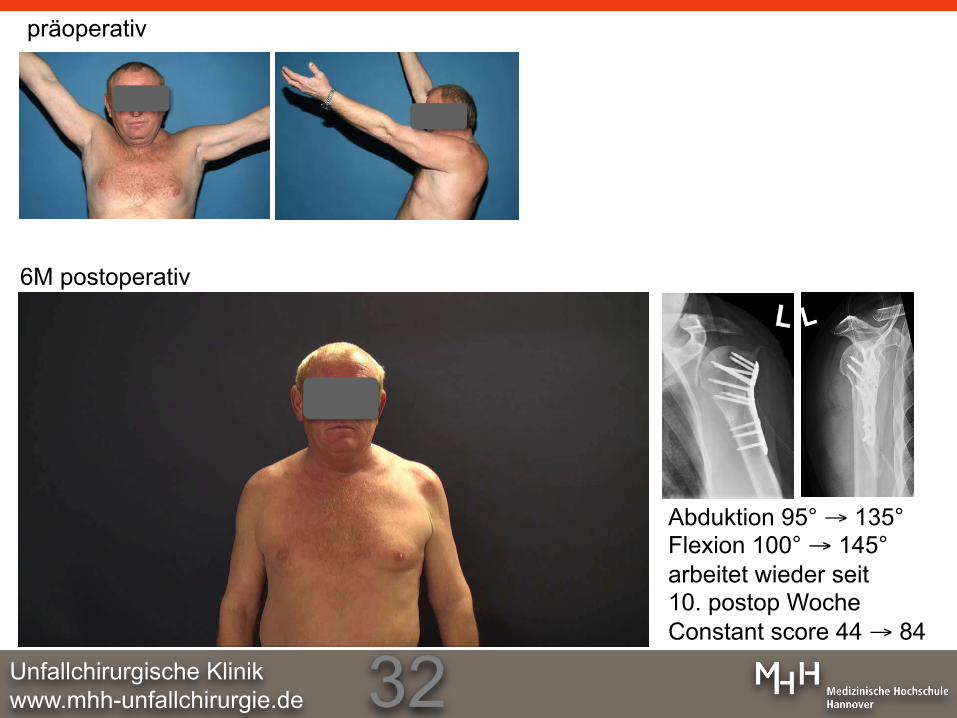
6M postoperativ
präoperativ
Abduktion 95° → 135° Flexion 100° → 145° arbeitet wieder seit 10. postop Woche Constant score 44 → 84

www.mhh-unfallchirurgie.de 33 Unfallchirurgische Klinik
Krettek et al 2011 Der Unfallchirurg
Technik der konservativen Behandlung
Schaftdislokation > 50% geschlossene Reposition Distales Fragment folgt dem proximalen bei Medialversatz des Schaftes proximale Rolle bei Tuberkulumhochstand: Abduktionsschiene Gilchrist-Verband/Schultertasche, Eigenbeübung (schmerzadaptiert) ab 1W: Pendelübungen ab 3W geführte Bewegungen in der Sagitalebene/Frontalebene <90° ab 6W >90° Dehnen mit Stabübungen, Umlenkrolle, leichte Gewichte Schmerz-!-adaptiert Rö:: 3, 6, 12 W (Studie) Bildverstärker Stabilitäts Untersuchung spielt keine Rolle
www.mhh-unfallchirurgie.de 34 Unfallchirurgische Klinik
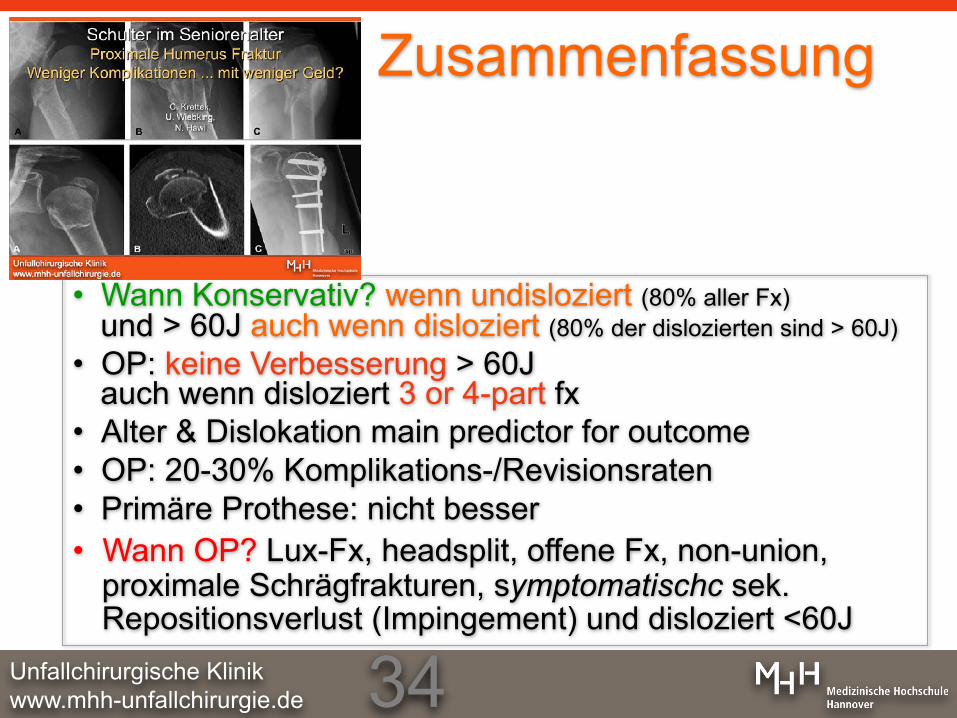
Zusammenfassung
• Wann Konservativ? wenn undisloziert (80% aller Fx) und > 60J auch wenn disloziert (80% der dislozierten sind > 60J)
• OP: keine Verbesserung > 60J auch wenn disloziert 3 or 4-part fx
• Alter & Dislokation main predictor for outcome • OP: 20-30% Komplikations-/Revisionsraten • Primäre Prothese: nicht besser • Wann OP? Lux-Fx, headsplit, offene Fx, non-union,
proximale Schrägfrakturen, symptomatischc sek. Repositionsverlust (Impingement) und disloziert <60J
www.mhh-unfallchirurgie.de 35 Unfallchirurgische Klinik
Diskussion
sehen Patienten nicht mehr Daten werden angezweifelt, Gültigkeit für Deutschland (OP Technik in D besser als Skandinavien) was brauchen wir ... bessere Daten Unklarheit bei jungen Patienten was passiert im längeren Follow up? Studien Registerdaten mit klinischem FU
Recommended




![Anlage 3 zur Honorarvereinbarung 2013 - kvsh.de · M84.41 Schulterregion [Klavikula, Skapula, Akromioklavikular-, Schulter-, Sternoklavikulargelenk] M84.42 Oberarm [Humerus, Ellenbogengelenk]](https://img.pdfslide.net/doc/110x75/5cada6f788c9933f078da1f9/anlage-3-zur-honorarvereinbarung-2013-kvshde-m8441-schulterregion-klavikula.jpg)