Decision Support Systems 51 (2011) 587–596
Contents lists available at ScienceDirect
Decision Support Systems
j ourna l homepage: www.e lsev ie r.com/ locate /dss
The adoption of mobile healthcare by hospital's professionals:An integrative perspective
Ing-Long Wu a,⁎, Jhao-Yin Li b, Chu-Ying Fu c
a Department of Information Management, National Chung Cheng University, 168 University Road, Ming-Hsiung, Chia-Yi, Taiwanb Institute of Information Science, Academia Sinica, Taiwanc Department of Information Management, WuFeng University of Science and Technology, Chia-Yi, Taiwan
⁎ Corresponding author. Tel.: +886 5 2720411x3462E-mail address: [email protected] (I.-L. Wu).
0167-9236/$ – see front matter © 2011 Elsevier B.V. Aldoi:10.1016/j.dss.2011.03.003
a b s t r a c t
a r t i c l e i n f oArticle history:Received 21 March 2010Received in revised form 7 January 2011Accepted 6 March 2011Available online 10 March 2011
Keywords:Mobile healthcarePersonal service availabilityPersonal innovativeness in ITTAMTPB
The adoption rate of mobile healthcare is relatively low in the hospital. In practice, a study of how healthcareprofessionals adopt mobile services to support their work is imperative. An integration of TAM and TPB,concerning both technological and organizational aspects, is important for understanding the adoption ofmobile healthcare. However, mobile healthcare is a wireless device which is often used in a voluntary motive.Service provisions for pervasive and timely usage and individual psychological states are critical indetermining its use. Accordingly, perceived service availability (PSA) and personal innovativeness in IT (PIIT)may be the important drivers to be included in TAM and TPB. This study thus proposed such a researchframework from a broader and integrative perspective. The empirical examination showed high predictivepower for adoption intention and the influential role of these important variables.
0; fax: +886 5 2721501.
l rights reserved.
© 2011 Elsevier B.V. All rights reserved.
1. Introduction
For the last decade, wireless technologies have been growingpervasively in various applications in the business sector, such asmobile commerce, supply chain management, customer relationshipmanagement, vendor managed inventory and so on. However, it isonly quite recently that a surge of mainstream popularity hasmotivated researchers to acknowledge the healthcare value ofwireless technologies. Hospitals are the places closely related topeople's health and medical professionals are responsible for thepatients' health and life. Medical professionals are always veryconcerned about the risk or uncertainty when using new technologiesto assist in medical treatments. Therefore, medical professionalsusually tend to adopt new technologies later until they have becomemore mature and safety in their use. However, wireless technologiescan be widely applied in many ways to help medical professionalscomplete their work safely and efficiently, for example, electronicpatient records and real-time monitoring systems of heart ratevariability. This creates a great need and importance for mobilehealthcare in the healthcare sector. However, a recent survey by theDepartment of Health in Taiwan in 2008 indicated that the adoptionrate of mobile healthcare for medical professionals is only 16.3%among all hospitals. Moreover, there are only 62 hospitals (13.7%) inTaiwan using mobile phones to perform wireless healthcare.
More specifically, during the last several years, a gradual shift inthe focus of mobile healthcare has taken place in hospitals. More andmore medical professionals are considering using some types ofmobile devices to support their work due to limitations of time andspace [8,27,56,58]. For instance, medical doctors can get patientrecords or the latest medical reports by using Multimedia MessagingService (MMS) on a mobile phone. Some hospitals have adoptedRadio Frequency Identification (RFID) to help medical doctors andnurses identify a large number of patients in emergency room [41,55].Accordingly, a study of how medical professionals adopt mobiledevices is desperately needed to effectively promote the pervasion ofsuch devices in hospitals. In particular, the advent of 3G mobilephones has provided a wide range of application services forperforming mobile healthcare in an easy and convenient manner.
The technology acceptance model (TAM) [14,15], the theory ofplanned behavior (TPB) [4] and their extensions have been widelyapplied in examining the acceptance in various IS contexts[13,23,44,51,67]. TAM focuses more on technological aspect and itsstrengths are its parsimony and high explanatory power. However, itlacks consideration of the effects of individual and organizationalfactors in the adoption process. TPB is used to explain the behavior oftechnology adoption by taking into consideration of the individualrole and organizational system in this process. Moreover, whilemobile devices with wireless features are portable for personal useand provide instant supports for various medical activities anytimeand anywhere, the quality of system services, such as real-timeservice availability, is a major concern for medical professionals. Thisis because the use of mobile healthcare is closely related to the

588 I.-L. Wu et al. / Decision Support Systems 51 (2011) 587–596
patients' health and life and medical professionals need to make surethat system services are able to provide pervasive and timely accessbefore they use these devices. Many studies have indicated the sameconcern about perceived service availability (PSA) when trying tounderstand the adoption of mobile devices [15,25,27,62].
In addition, while mobile healthcare is an emerging technology forpersonal use which is often used voluntarily, the psychological statesof medical personnel play a critical role in determining system use.Many researchers have considered such a psychological antecedentfor identifying individual differences in the adoption of newtechnology, namely personal innovativeness [19,22,50,54]. It refersto an individual's psychological state of willingness to take a risk bytrying out an innovation. As personal innovativeness is applied inexamining IT acceptance, it is defined as personal innovativeness in IT(PIIT) [1,68].
In summary of the above discussion, while the adoption process ofmobile healthcare involves both technological and organizationalaspects on the level of individual, in this study, we first integratedTAM and TPB in a complementary manner. Many studies haveproposed a unified model primarily based on TAM and TPB for variousIS settings [62,65]. In particular, a similar study worked on exploringPDA acceptance by healthcare professionals with higher explanatorypower [68]. Moreover, while considering the importance of PSA andPIIT in the adoption of mobile healthcare in particular, an enhance-ment of the unified view with the two important antecedents maypositively increase the explanatory power of a proposed model.However, little research has discussed the personal use of mobilehealthcare in a broader view in the hospital context. Therefore, theobjective of this study aims at proposing an integrated model byincluding four components to explore the adoption of mobilehealthcare.
In addition, many researchers have generally argued that theacceptance of an emerging IT in hospitals may be affected by somehospital characteristics other than IT-related attributes, such ashospital size/type and user/provider type [28,33,48,52]. Hospitaltype was defined to include three major types, medical center,regional hospital, and local hospital, based on a combination of somehospital attributes, such as quality of medical service, annual revenue,and number of employees, in Taiwan. Provider type was classified astwo major types of professional users in the mobile healthcarecontext, physicians and nurses. Therefore, we specified hospital typeand provider type as two control variables in this study. Furthermore,empirical examination is conducted to examine the practical validityof the proposed model.
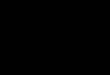
PerceivedEase of use
PersonalInnovativeness
in IT
H11
H12
H7
H6PerceivedService
Availability
PerceivedUsefulness
H10
H5
H8
H9
Fig. 1. Researc
2. Literature review and hypotheses development
Based on the above discussion, Fig. 1 provides a pictorial depictionof this research framework. The following section discusses thetheoretical bases and development of relevant hypotheses.
2.1. Mobile healthcare
With an increasingly mobile society and the worldwide deploy-ment of wireless networks, the wireless infrastructure can providesupport for many current and emerging healthcare applications. Thiscan fulfill the vision of ubiquitous healthcare or healthcare to anyone,anytime, and anywhere. A recent study has pointed out that thewireless requirements for supporting healthcare services are in acomprehensive coverage with readiness, including reliable access andtransmission of medical information, location management, andsupport for patient mobility [58]. A comprehensive wireless architec-ture for location management in a healthcare environment can bedesigned by utilizing one or more location tracking technologies,including GPS, cellular networks, wireless LANs, and RFID [55,57].Specifically, various remote devices have been applied in wirelesshealthcare. Examples include the implementation of infrared andradio-based locator badges [49], long-term health monitoring bywearable devices [29], wireless telemetry systems for EEG epilepsymonitoring [37], wireless sensors for blood oxygen saturationmonitoring [6,43], real-time monitoring of patients in the homeenvironment [32,39], short range blue tooth-based systems fordigitized ECG [31], and several systems for remote heart monitoringusing cellular-type wireless networks [46]. Furthermore, Shermanet al. [47] conducted a case study to understand the usage of mobileincentive care units (MICU) in medical emergency services.
A recent report has shown the importance of health monitoringsystems in reducing the number of readmissions for patients sufferingfrom many chronic health problems [16]. Health monitoring systemscan also help in keeping track of patients with one or more cognitivedisabilities, such as stray prevention system for the elderly withdementia [36]. Many cost-effectiveness analyses for mobile health-care services have been reported for the potential usage [21,64].Lehoux et al. [34] conducted an interview of a small group ofphysicians to point out some problems in using mobile devices forclinics. An economic analysis of health insurance was performed byGravelle and Sicilian [24] and they indicated that if wireless networkscould provide the help to a treatment process of patients in hospitals,the outcome of healthcare would be effectively increased. Moreover,
PerceivedBehavioral Control
BehavioralIntention
SubjectiveNorm
Attitude H1
H2
H3
H4
Technology Acceptance Model
Theory of Planned Behavior
Hospital Type
Provider Type
h model.

589I.-L. Wu et al. / Decision Support Systems 51 (2011) 587–596
the use of wireless technologies can reduce the long-term cost ofhealthcare and result in an increased productivity of healthcareproviders. To support the long-term healthcare needs of patients,comprehensive wireless patient monitoring solutions must bedeveloped for the homes, nursing homes, and hospitals [27,42,56].In summary, these objectives can be well achieved by the features ofwireless technologies: improved coverage and scalability of wirelessnetworks, dependable and reliable operations, implementable andreusable wireless technologies, and expandable and modifiablewireless technologies [57]. We argue that emerging mobile devicesin the hospitals are important tools for improving the quality ofhealthcare in the near future. Therefore, exploring the use of mobiledevices is a major issue for medical personnel, nursing staff, andpatients in hospitals.
2.2. TAM and TPB
Both TAM and TPB were originally based on the efforts of thetheory of reasoned action (TRA) [18]. TRA is a well-established modelthat has been broadly used to predict and explain human behavior invarious domains. According to TRA, a person's behavior towardcertain action is determined by his or her behavioral intention (BI) toperform the behavior and in turn, BI is jointly determined by theperson's attitude (ATT) and subjective norm (SN) concerning thebehavior in question. Behavioral intention is a measure of the strengthof one's willingness to try and exert while performing certainbehavior. Attitude refers to the degree of a person's favorable orunfavorable evaluation or appraisal of the behavior in question.Subjective norm refers to the perceived social pressure to perform ornot to perform the behavior. A person's attitude toward a behavior isdetermined by his or her salient beliefs (sbi) about the consequencesof performing the behavior multiplied by the evaluation (ei) of theseconsequences, that is, A=Σsbiei. An individual's subjective norm (SN)is determined by a multiplicative function of his or her normativebeliefs (nbi), for example, perceived expectations of specific referentindividuals or groups, and his or her motivation to comply (mci) withthese expectations, that is, SN=Σnbimci.
Based on the effort of TRA, TAM is designed for modeling useracceptanceof information technology [15]. Thismodel hypothesizes theserelationships, actual use of a certain technology directly influenced by aperson's behavioral intention to use and in turn, behavioral intention touse determined by perceived usefulness (PU) and attitude toward thetechnology. Furthermore, perceived usefulness and attitude are affectedby perceived ease of use (PEOU). Perceived usefulness refers to theprospective user's subjective assessment of the probability that using aspecific application systemwill increasehis orher jobperformancewithinan organizational context. Perceived ease of use refers to the degree towhich the prospective user expects the target system to be free of effort inuse. TRA has theorized that behavioral intention to use is determined byattitude toward the behavior and subjective norm. However, TAM is onlyconcerned with the effect of attitude and neglects the influence ofsubjective norm on behavioral intention to use. This is due to theuncertainty about theoretical and psychometric status when TAM wasdeveloping [15]. The appeal of this model is that it is both specific andparsimonious. These determinants are easy to understand and can bemanipulated through systemdesign and implementation. They should beable to generalize across various settings [9,51].
Building on TRA, TPB differs from TRA by adding a third component,perceived behavioral control (PBC). Accordingly, behavioral intention touse is jointly determined by a person's attitude, subjective norm, andperceived behavioral control toward the behavior. PBC refers to aperson's perception of ease or difficulty in performing the behavior ofinterest. It is concernedwith the beliefs aboutpresence of control factorsthat may facilitate or inhibit performance of the behavior [5]. Thus,control beliefs about resources and opportunities are the underlyingdeterminants of PBC and it can be depicted as control beliefs (cbi)
weighted by perceived power of the control factor (pi) in question, thatis, PBC=Σcbipi. In sum, TPB proposes to eliminate the limitation of TRAin dealing with the behaviors over which people have incompletevolitional control [4]. Many studies have indicated the need forconsidering control-based beliefs to understand personal behaviorrelated to the adoption of mobile healthcare [10,68]. Control-basedbeliefs can fall into individual categories, such as perceived self-efficacyin using mobile technology, and organizational categories, such asperceived technology support and training and perceivedmanagementsupport.
The following section discusses the development of relevanthypotheses. While the acceptance of mobile healthcare generallyinvolves both technological and behavioral aspects for personal use,TAM is not complete in its coverage of both aspects, includingperceived usefulness, perceived ease of use, and attitude. Manystudies have therefore proposed the concept of integrating TPB in acomplementary manner, including subjective norm and perceivedbehavioral control, in many business applications [38,44,62,65]. Morespecifically, some researchers have also applied the integrationconcept to explore the use of telemedicine technologies by healthcareprofessionals, for example, WAP-based telemedicine systems [10,26].Additionally, other studies have shown that the integration of TAMand TPB should lead to higher power to explain technologyacceptance in both business and healthcare applications [62,68].Therefore, we simply integrated TAM with two belief structures,subjective norm and perceived behavioral control, and ignored theirdecomposed attributes in this study.
Based on the above discussion, there are three direct antecedents,attitude, perceived behavioral control, and subjective norm, fordetermining behavioral intention to use. We argue that there arethree potential linkages between these three antecedents andbehavioral intention to use in the usage context of mobile healthcare.Three hypotheses are thus proposed.
H1. Attitude has a positive effect on behavioral intention to usemobile healthcare.
H2. Perceived behavioral control has a positive effect on behavioralintention to use mobile healthcare.
H3. Subjective norm has a positive effect on behavioral intention touse mobile healthcare.
Moreover, according to the TAM structure, as discussed previously,perceived usefulness has a direct impact on behavioral intention to use,perceived usefulness and perceived ease of use are two antecedents ofattitude, and perceived ease of use has a direct effect on perceivedusefulness. We argue that these potential linkages exist in the usagecontext of mobile healthcare. Four hypotheses are thus proposed.
H4. Perceived usefulness has a positive effect on behavioral intentionto use mobile healthcare.
H5. Perceived usefulness has a positive effect on attitude towardusing mobile healthcare.
H6. Perceived ease of use has a positive effect on attitude towardusing mobile healthcare.
H7. Perceived ease of use has a positive effect on perceived usefulnessfor mobile healthcare.
2.3. Personal innovativeness and IT adoption
Personal innovativeness represents the degree to which anindividual is willing to take a risk by trying out an innovation[19,40]. People with this trait tend to launch a new idea in a system byimporting the innovation from outside of the system's boundaries.

590 I.-L. Wu et al. / Decision Support Systems 51 (2011) 587–596
According to innovation diffusion theory (IDT), people react differ-ently due to differences in personal innovativeness, which is apredisposed tendency toward adopting an innovation [45]. Personalinnovativeness can be classified into five types: innovators, earlyadopters, early majority, late majority, and laggards. The applicationof personal innovativeness in information technology has beenreferred to as personal innovativeness in IT [1,2]. PIIT has been widelyused to examine the adoption of various IS settings [3,22,50,53,54,68].PIIT is conceptualized as a trait, which is a relatively stable descriptorof an individual and invariant across situations. As also noted byWebster and Martochhio [65], traits are generally not influenced byenvironmental or internal variables. When individuals have greatpower to decide to either use an innovation or not in an organization,we can base PIIT on analyzing their psychological states to furtherunderstand human behavior intention to use the innovation.
The following section presents the development of relevanthypotheses. Many studies have examined the relationship betweenPIIT and attitude in many IS settings. One study investigated thepersonal acceptance of Internet-based public grid computing softwarewith a PC-based device among voluntary participators and argued alinkagebetweenPIIT andattitude towardusing this device [50]. Anotherstudy analyzed individual's Internet anxiety, an attitude toward theInternet use, when individual may experience perceived unreliability,risk, and vulnerability from using the Internet. Thus, the authorssuggested a relationship between PIIT and Internet anxiety [53].Additional study discussed the potential relationship between softwaredevelopers' innovativeness and their attitude toward an innovation interms of the redesign of software development process in theirorganization [22]. Other studies have identified the indirect effect ofPIIT on attitudes toward using various information technologies[54,63,68]. Accordingly, while healthcare professionals usually work inan independent decision-making manner for patients' treatment andthe early use of mobile healthcare is considered in a voluntary mode,PIIT is argued to be an important determinant of attitude toward usingmobile healthcare. The following hypothesis is thus proposed.
H8. Personal innovativeness in IT has a positive effect on attitudetoward using mobile healthcare.
According to IDT, individualswith high innovativeness aremore likelyto try out new things and have greater ability to control uncertainty andrisk [45].Many studieshavediscussed thedirect and indirect effects of PIITon perceived behavioral control on adoption behavior of variousinformation technologies [3,68]. In the study by Yi et al. [68], in terms ofthe acceptance of PDA bymedical professionals, the PIIT was posited as adirect antecedent of perceived behavioral control toward the behavior ofadopting PDA. Another study proposed PIIT as a determinant of computerself-efficacy with respect to the use of Window or Lotus software [3].Moreover, the decomposed TPB identifies computer self-efficacy as adeterminant of perceived behavioral control toward the behavior of usinga new technology [51]. Therefore, PIIT has the indirect impact onperceived behavioral control toward the behavior. Accordingly, we arguethat there is a potential linkage between PIIT and perceived behavioralcontrol toward the behavior of using mobile healthcare. The followinghypothesis is thus proposed.
H9. Personal innovativeness in IT has a positive effect on perceivedbehavior control with respect to using mobile healthcare.
Individuals with more innovativeness in IT are more technicallycompetent than others in using new technology. They tend to beearlier adopters of new technology while compared to later adopters.They consider the complexity of using new technology less trouble-some than others [30]. Perceived ease of use is considered as themajor technical feature in initiating the use of new technology for newusers [14]. Much research has discussed the direct relationshipbetween PIIT and perceived ease of use in various IS settings
[35,63,68]. A prior study indicated that PIIT is a significant antecedentof perceived ease of use in terms of knowledge of workers in their useof IT [35]. Extending these findings, Yi et al. [68] theorized the directeffect of PIIT on perceived ease of use while testing the acceptance ofPDA by healthcare professionals. Another study indicated that higherPIIT leads to higher perceived ease of use for financial service software[63]. In addition, Agarwal et al. [3] proposed an indirect relationshipbetween PIIT and perceived ease of use with a moderating role ofcomputer self-efficiency for using Window or Lotus software. Basedon the above arguments, we assume that there is a linkage betweenPIIT and perceived ease of use for mobile healthcare. The followinghypothesis is thus proposed.
H10. Personal innovativeness in IT has a positive effect on perceivedease of use for mobile healthcare.
2.4. Perceived service availability and IT adoption
Wireless technologies can provide high availability of medicalresources for healthcare professionals anytime and anywhere andtherefore, enable employees to significantly improve the quality ofpatient care and their working practice. The final challenge for usingmobile healthcare is to achieve the dream of ubiquitous healthcare.However, the use of mobile healthcare is closely related to thepatients' health and life. Healthcare professionals are usually hesitantto adopt a new system service, such as mobile healthcare, when it isstill in the early development stage of its regular use. Among theconcerns regarding mobile service, there is a specific perception thatrelates to the unique features of wireless devices and their particularusage context for patient safety. Perceived service availability refers tothe degree to which an innovation is perceived as being able tosupport pervasive and timely usage. It is considered as an importantdeterminant for use in mobile healthcare.
The following section discusses the development of relevanthypotheses. Many studies have generally highlighted the importanceof service provisions in determining the personal use of a new mobileservice [17,25,27]. More specifically, one study indicated that PSA isexpected to have a direct effect on perceived usefulness for a mobiledata service and in turn, behavioral intention to use [25]. Accordingly,we posit a potential linkage between PSA and perceived usefulness formobile healthcare. The following hypothesis is thus proposed.
H11. Perceived service availability has a positive effect on perceivedusefulness for mobile healthcare.
The same study, as discussed above, also argued that PSA has adirect influence on perceived ease of use for amobile data service [25].Another study proposed that facilitating conditions are determinantsof perceived ease of use for a new technology [59]. Facilitatingconditions are defined as the provision factors in the user environ-ment to support the use of a new technology [62]. Thus, facilitatingconditions can be considered as certain forms of PSA based on theabove definition, such as the readiness of a wireless service. Inconclusion, PSA has an influence on perceived ease of use in themobile healthcare context. Based on the above discussion, we arguethat there is a potential linkage between PSA and perceived ease ofuse for mobile healthcare. The following hypothesis is thus proposed.
H12. Perceived service availability has a positive effect on perceivedease of use for mobile healthcare.
3. Research design
3.1. Instrumentation
A survey was conducted to collect data. The instrument wasdesigned with a two-part questionnaire. The first part uses a nominal

Table 1Demographics of the respondents.
Frequency Percent (%)
Type of hospitalMedical center 15 18.7Regional hospital 45 56.2Local hospital 20 25.1
Bed sizeb500 18 22.5500–1000 45 56.21000–1500 10 12.5N1500 3 8.8
PositionPhysician 50 35.7Nurse 90 64.3
GenderFemale 88 62.9Male 52 37.1
Work experienceb5 years 30 21.45–15 years 62 44.315–25 years 36 25.7N25 years 12 8.6
Education levelHigh school 21 15.0College 48 34.3Graduate 21 15.0M.D. 50 35.7
Ageb30 years 25 17.831–40 years 54 38.641–50 years 43 30.7N50 years 18 12.9
591I.-L. Wu et al. / Decision Support Systems 51 (2011) 587–596
scale and the second part uses 7-point Likert scales, as shown in theAppendix A.
3.1.1. Basic informationThis part of the questionnaire collects basic information about
organizational characteristics including hospital type and bed size aswell as respondent characteristics including position, gender, workexperience, education level, and age.
3.1.2. TAM constructsThe measuring items for TAM constructs, including perceived
usefulness, perceived ease of use, attitude, and behavioral intention touse, were adapted from the measurement developed by Venkateshand Davis [60,61]. They contain 4 items, 4 items, 4 items, and 3 itemsrespectively.
3.1.3. TPB constructsThe measuring items for TPB constructs, including perceived
behavior control and subjective norm, were adapted from themeasurements developed by Taylor and Todd [51] and Bhattacherjee[7]. They contain 3 items and 3 items, respectively.
3.1.4. PIIT and PSAThemeasuring items for personal innovativeness in IT are based on
the recommendations of Agarwal and Prasad [1] and Yi et al. [68],including 3 items. The measuring items for perceived serviceavailability were adapted from the measurements developed byVenkatesh [59] and Hong and Tam [25], including 4 items.
3.1.5. Control variableHospital type is indicated as three types, medical center, regional
hospital, and local hospital and provider/user type is clustered as twotypes, physicians and nurses, as discussed previously.
3.2. Sample design
This survey was conducted to examine the acceptance of mobilehealthcare by healthcare professionals in hospitals. Mobile healthcareis still in an early stage of use and is considered to be a new technologyby medical professionals. It was assumed that larger hospitals wouldbe more likely to have early experience. Three types of hospitals arequalified for this study, including medical centers, regional hospitals,and district hospitals, as classified by the Taiwan Joint Commission onHospital Accreditation. 450 hospitals of these three types wereaccredited by the above-mentioned organization in 2007. Werandomly selected 80 hospitals for the study sample from thepopulation of 450 hospitals. Furthermore, physicians and nurses inthe hospitals were the major respondents since they are the majorusers of mobile healthcare. Afterwards, we first sent an invitationletter to one designated person in each selected hospital and askedthem to help distribute questionnaires to their colleagues, includingphysicians and nurses. After that, 10 questionnaires were sent to eachhospital through the designated person. The designated person foreach hospital was also responsible for the collection of thequestionnaires. In order to improve survey return, a follow-upprocedure was carried out with a phone call made to the designatedperson from each hospital after 3 weeks.
3.3. Demographics
A pretest was conducted for the scale. The scale was carefullyexamined for translation, wording, structure, and content by selectedpractitioners (i.e., physicians and nurses) and scholars in this area.Initial reliability and content validity of the scale should be acceptable.After the questionnaire was finalized, 800 questionnaires were sentout to the potential respondents in terms of 10 potential respondents
for each hospital and 80 sample hospitals. A total of 140 validquestionnaires were received. The response rate was 17.5%. Theseemingly low response rate raised possible concerns about non-response bias. To check non-response bias, the responding samplewas divided into two subsamples, that is, early and late subsamples,including 95 and 45 respondents, respectively. The two groups werecompared using various demographic characteristics, includinghospital type, bed size, position, gender, and age, for their correlationwith t-test, None of them (t value=0.76, 0.68, 1.24, 0.98 and 1.01)showed significant differences at the 0.05 level. Their results indicatedthat there was no systematic non-response bias for the respondingsample. Table 1 summarizes the demographics of the respondents.
3.4. Measurement model
PLS is a structural equationmodeling (SEM) technique that employsa nonparametric and component-based approach for estimationpurposes. PLS allows latent variables to be modeled as either formativeor reflective constructs, and places minimal demands on sample sizeand residual distributions [11–13]. Theoretically, the sample size forexecuting PLS requires 10 times of the number of indicators associatedwith the most complex construct or the largest number of antecedentconstructs linking to an endogenous construct. When there are8 variables and each comprises 3–4 measuring items, the sample size(140 respondents) may not be large enough for a goodness of mode-fitwith AMOS technique. This study uses PLS to analyze the measurementmodel. PLS is the best analytical tool available to fit the requirement ofsmall sample size.
Construct validity is defined to comprise convergent and discriminantvalidities. First, convergent validity for a construct is assessed by threecriteria: (1) all item loadings (λ) in a construct should be larger than 0.70

Table 3Discriminant validity.
Construct PU PEOU SN PBC ATT BI PIIT PSA
Perceived usefulness (PU) 0.80Perceived ease of use (PEOU) 0.06 0.83Subjective norm (SN) 0.15 0.11 0.75Perceived behavioral control(PBC)
0.23 0.13 0.13 0.79
Attitude (ATT) 0.22 0.32 0.21 0.19 0.84Behavioral intention (BI) 0.30 0.28 0.15 0.16 0.15 0.80Personal innovativeness in IT(PIIT)
0.14 0.16 0.09 0.21 0.13 0.13 0.82
Personal service availability(PSA)
0.15 0.29 0.25 0.07 0.31 0.22 0.20 0.81
Diagonal value: square root of AVE and non-diagonal value: correlation
592 I.-L. Wu et al. / Decision Support Systems 51 (2011) 587–596
and statistically significant, (2) composite reliability for a construct shouldexceed 0.80 and can be interpreted like a Cronbach' α coefficient, and(3) average variance extracted (AVE) for a construct should be larger than0.50 [20]. Next, discriminant validity is assessed using the criterion thatthe square root of AVE for a construct shouldbe larger than its correlationswith other constructs [13,20]. Table 2 shows the indices of reliability andconvergent validities for the scale. Item loadings range from 0.84 to 0.96and are all significant at the 0.01 level. Composite reliabilities range from0.85 to 0.93, and AVE range from 0.82 to 0.90. These indices togetherindicate a high degree of convergent validity. Cronbach' α coefficientsrange from 0.87 to 0.93, which suggests a high level of reliability. Thecorrelationmatrix between constructs shows that the square root of AVEfor a construct is above its correlationswith other constructs, as indicatedin Table 3. The results suggest a high degree of discriminant validity.
4. Statistical analysis and hypotheses testing
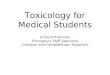
A structural model was built to examine the causal relationshipsamong the constructs in the research model. There are two steps inevaluating the structural model. First, we needed to estimate thestandardized path coefficients and their statistical significance fortesting the hypotheses. PLS does not provide a significance test orconfidence interval estimation. Bootstrapping analysis was used toestimate path coefficients, statistical significance, and relevantparameters, such as means, standard errors, item loadings and itemweights. We re-sampled 1000 times to obtain a stable result for theseanalyses. Second, the coefficient of determination (R2) for endogenousvariables was calculated to assess the predictive power of thestructural model. The coefficient of determination obtained fromPLS analysis was similar to that found in multiple regression analysis.Fig. 2 shows the testing results of the structural model.
For the components of TPB, attitude, perceived behavior control andsubjective norm are all reported to be the important antecedents ofbehavioral intention to usemobile healthcare (β=0.21, 0.25 and 0.24).Therefore, Hypotheses 1, 2, and 3 are all supported. For the componentsof TAM, perceived usefulness shows a significant positive impact onbehavioral intention to use (β=0.26). Hypothesis 4 is thus supported.Perceived usefulness is a significant determinant of attitude towardusing mobile healthcare (β=0.60). Hypothesis 5 is thus supported.Perceived ease of use reveals no significance in influencing attitude(β=0.16). Therefore, Hypothesis 6 is not supported. In contrast,perceived ease of use plays a critical role in determining perceivedusefulness (β=0.40). Hypothesis 7 is thus supported. In brief, the fourconstructs, attitude, perceived behavior control and subjective norm,and perceived usefulness, jointly explain 63% of variance in behavioralintention to use mobile healthcare (R2=0.63).
The construct of PIIT indicates no significant influence on attitude(β=0.15). Therefore, Hypothesis 8 is not supported. Conversely, it is asignificant determinant of both perceived behavioral control andperceived ease of use (β=0.28, 0.33). Hypotheses 9 and 10 are thussupported. In summary, the three constructs, perceived usefulness,perceived ease of use, and PIIT, jointly explain 62% of variance in attitude
Table 2Reliability and convergent validity.
Construct No. of items Mean S.D.
Perceived usefulness 4 4.89 1.15Perceived ease of use 4 4.88 1.13Subjective norm 3 5.27 1.26Perceived behavioral control 3 4.78 1.23Attitude 3 5.31 1.11Behavioral intention 3 4.77 1.22Personal innovativeness in IT 4 5.08 1.12Personal service availability 3 4.52 1.26
towardusingmobile healthcare (R2=0.62).Next, PIIT singly explains 25%variance of perceived behavioral control with respect to using mobilehealthcare. The construct of PSA indicates as an important antecedent ofperceived usefulness (β=0.38). Hypothesis 11 is thus supported. Incontrast, it is not a significant influencer of perceived ease of use(β=0.13). Therefore, Hypothesis 12 is not supported. In a brief summary,the two constructs, perceived ease of use and PSA, together explain 69% ofvariance in perceived usefulness (R2=0.69). Next, the two uniquefeatures for mobile healthcare, PIIT and PSA, jointly explain 29% ofvariance in perceived ease of use (R2=0.29). Finally, regarding the twospecified control variables, hospital type was found to be significantlyassociatedwith behavioral intentionwhile provider type is not significantfor their correlation (β=0.30 and 0.14).
5. Findings and discussions
This current model indicates high explanatory power for behavioralintention to use mobile healthcare with R2=0.63. Similar TAM or TPB-based studies in the context of telemedicine technologies have reported inlower levels of predictive power, Yi et al. [68]with R2=0.57, Chau andHu[10]with R2=0.43, andHu et al. [26]with R2=0.44. Thismay be becausethe four antecedents of behavioral intention to use, that is, perceivedusefulness, attitude, perceived behavioral control, and subjective norm,are all significant in their influence. This alsowell confirms the importanceof an integration of TAMandTPBwith twoparticular factors, PIIT and PSA,in effectively determining the acceptance of mobile services in thehealthcare context.
Among these antecedents, perceived usefulness, in particular, playsthe samesignificant role as the threemajor components of TPB, attitude,perceived behavioral control, and subjective norm. Research on theissue of integrating TAM and TPB has shownmixed results in its impacton behavioral intention to use [66]. Moreover, perceived usefulness hasmuchgreater influence on attitude towardusingmobile healthcare thanperceived ease of use, (β=0.60 vs. 0.16). In brief, for the two findings,perceived usefulness is particularly important in encouraging the use ofmobile healthcare. The reason behind this may be due to the uniquerelevance of usingmobile healthcare in the patients' health and life. As a
Itemloading
Compositereliability
AVE Cronbach'α
0.92–0.96 0.93 0.90 0.930.90–0.94 0.91 0.86 0.920.85–0.92 0.88 0.85 0.880.84–0.89 0.85 0.82 0.870.86–0.88 0.88 0.83 0.890.88–0.90 0.90 0.85 0.900.89–0.90 0.90 0.85 0.900.84–0.91 0.88 0.83 0.90

PerceivedEase of use
PersonalInnovativeness
in IT
PerceivedBehavioral Control
BehavioralIntention
SubjectiveNorm
0.38*
0.13
0.40*
0.16Attitude
PerceivedService
Availability
PerceivedUsefulness
0.33*
0.60*
0.15
0.28*
0.21*
0.25*
0.24*
0.26*
Technology Acceptance Model
Theory of Planned Behavior
R2 = 0.63R2 = 0.62
R2 = 0.25
R2 = 0.29
R2 = 0.69
Hospital Type
Provider Type
0.30* 0.14
Fig. 2. Results of the structural model. Value on path: standardized coefficients (β), R2: Coefficient of determination and *pb0.01.
593I.-L. Wu et al. / Decision Support Systems 51 (2011) 587–596
result, healthcare professionals should cautiously evaluate its realusefulness in helping patient cares before it is actually used. Perceivedease of use indicates no significant effect on attitude toward usingmobile healthcare. Thismaybebecause the designs of user interfaces formobile services are in well-defined forms and are able to communicatewith medical professionals in a user-friendly manner. From a broaderperspective, a lack of variation in users' evaluations of user interfacesmay be a part of a well-defined form since the designs of user interfaceshave reached a level of maturity.
Next, this study importantly indicates that PIIT is not significant indeterminingattitude, but is significant in influencingperceivedbehavioralcontrol. The findings are particularly novel for the adoption of mobilehealthcarewhile attitude is usually reported as themajor produced effectin the literature. The findings also explain the above indication of thesimilar role played by perceived behavioral control in affecting behavioralintention touse.More specifically, the reasons to explain this are two-fold.First, while mobile healthcare has beenwidely advocated and recognizedby healthcare professionals in hospitals in order to improve healthcarequality recently, the major problem for determining the use of mobilehealthcare is not the favorable or unfavorable psychological states ofhealthcare professionals but externally physical forces or control factorsthat encourage their usage, such as the necessity of using innovations totreat patients in certain environments. Second, perceived behavioralcontrol is concernedwith beliefs about the presence of control factors thatmay facilitate or inhibit performanceof thebehavior [5], suchas computerself-efficacy and locus of control. Furthermore, potential userswith higherPITT tend to have favorable psychological states and are thus willing totake risks by trying out innovations [50,68]. Therefore, healthcareprofessionals with higher PIIT enforce their interests or psychologicalstates in favor of theuseofmobilehealthcare andas a result, theyperceivebetter control or ease in performing the adoption behavior.
Moreover, PSA, as an important determinant of using newtechnology, reveals significant effect on perceived usefulness and nosignificant effect on perceived ease of use. The findings areparticularly critical for the use of mobile healthcare since mostprofessionals still think that mobile healthcare is a type of emergingtechnology which is difficult to use. This may have an indication forencouraging the professionals to use this technology in the hospitals.The reasons for these results may be noted as below. For the former,mobile healthcare is closely related to the patients' life and itsusefulness for healthcare professionals is greatly dependent onwhether it can be regularly operated regardless of time and place.For the latter, the reasons may be similar to the above discussion
about perceived ease of use. While the designs of user interfaces formobile services provide mature and consistent forms for users, PSAmay not be an important determinant of perceived ease of use anymore at the current technological level.
Finally, a fewwords about the control variables are in order. The threehospital types, medical center, regional hospital, and local hospital, aresignificantly different in influencing behavioral intention. This indicatesthat larger hospitals (medical centers) are in a position to have highbehavioral intention to use mobile healthcare among medical personnel.The reasons behind thismay be explained as below. Larger hospitals havemore responsibility to guarantee quality of patient care in terms ofimproving customer care and administrative processes. Moreover, theypossess the resources and skills necessary to assimilate the innovationamong medical personnel efficiently and effectively. As a result, users ofmobile healthcare are more likely to adopt healthcare mobile in thesituation of both internal and external pressures. Next, the two providertypes, physicians and nurses, indicate no significant difference inimpacting behavioral intention. In other words, physicians and nurseshave no difference in behavioral intention to usemobile healthcare acrosshospital sizes. Twomajor reasons are discussed as below. First, the use ofmobile healthcare, while offering ubiquitous healthcare or healthcare toanyone, anytime, and anywhere, has increasingly become an importantworking concept for all healthcare professionals. Second, the features ofmobile healthcare have grown into more maturity recently for providingusefulness and usability (ease of use) for all healthcare professionals.
6. Conclusions and suggestions
In general, this study first integrated TAM and TPB to explain theadoption behavior in general IS settings. In particular, whileconsidering the context of mobile healthcare for healthcare profes-sionals, PIIT and PSA have been well indicated as importantantecedents of individual adoption. This study integrated the twoperspectives to propose a research model for exploring the adoptionof mobile healthcare in a complementary manner. First, this modelhas reported high explanatory power for the adoption of mobilehealthcare compared to previous studies. Next, there are several newfindings regarding the roles of TAM and TPB as well as PIIT and PSA.The components of TAM and TPB are all important in the adoption ofmobile healthcare. PIIT is particularly important to the perceivedbehavioral control toward using mobile healthcare as the control orfacilitating factor. PSA is crucial to the perceived usefulness in the

594 I.-L. Wu et al. / Decision Support Systems 51 (2011) 587–596
particular healthcare environment. These findings have importantimplications for both practitioners and researchers.
For the practitioners, healthcare professionals are very conserva-tive about trying new technologies since their work directly relates topatients' safety. They often adopt new technology with highconfidence only when skill level or knowledge seems stable andmature. These particular properties regularly impede the diffusion ofmobile healthcare. As a result, this study has shown that recognizingsome improvements of technological, organizational, and individualcharacteristics is critical in increasing the behavioral intention to usemobile healthcare by medical professionals. First, PSA is the initialdriving force determining behavioral intention to use through twolayers of mediators in terms of TAM beliefs, that is, perceivedusefulness and attitude. This description basically relates to aparticular technological issue in the adoption of mobile services.This means that to effectively encourage medical professionals to usemobile healthcare, the service provided should be well prepared inthe hospitals to enable pervasive and timely usage without anydifficulty.
Next, a TAM belief (perceived usefulness) and PIIT are shown tobe the underlying antecedents in determining behavioral intentionto use through the mediators of attitude and perceived behavioralcontrol, respectively. This means that both technological (perceivedusefulness) and individual issues (PIIT) are important for overcom-ing the impediment of usingmobile healthcare. For the technologicalaspect, the design of a mobile healthcare needs to first carefullyexamine the functional requirements of users and then, this systemis able to provide useful information for helping in the decisionmaking of medical professionals. For the individual aspect, thehospitals may provide incentives for encouraging medical profes-sionals to carry out their regular tasks in an innovative manner. Thiswould improve the willingness of individuals to take risks by tryingout innovations. Finally, the TPB components, attitude, perceivedbehavioral control, and subjective norm, involve relevant organiza-tional and individual issues for indicating their impact on theadoption of mobile services. The hospitals, as a type of anorganization's form, should be able to provide some trainingprograms for increasing the skill levels of employees and nurturingtheir confidence in facing new technologies as well as be able tocarefully plan and design certain interactive/coordinative programsfor employees in terms of their formal and informal communicationneeds in their work in order to establish the mechanism of mutualtrust and influence for their co-workers.
For the researchers, prior research on IT acceptance in general andmobile services in particular has been focused on the generalcomponents of TAM or TPB. This research considered the roles ofsystem services and personal traits in the innovation acceptance. Thisis because mobile healthcare with wireless features is an emergingtechnology for medical professionals in terms of high uncertainty insystem services, great change of their work styles, and real belief of itsusefulness. These considerations are particularly important for thecontext of mobile healthcare. We approached this from a broaderperspective in terms of considering various perspectives, includingthe attributes of organizations, individuals, technology, systemservices, and psychological states. The empirical findings have beenconfirmed to have higher predictive power compared to previousstudies. This will provide a new way of thinking for theoreticallydefining the antecedents of behavioral intention to use in the contextof mobile healthcare.
Furthermore, subsequent research can be based on this founda-tion. First, while the sample respondents of physician and nurses inthis study have been identified as new users of innovations,behavioral intention to use may change in terms of user levels ofexperience. Additional research can be conducted to examinedifferences of behavioral intentions as users become more aware ofmobile healthcare. Next, this study primarily develops a theoretical
framework and further empirically validates it with survey data.Future research can be redesigned with case studies to longitudinallyobserve the usefulness of this research framework in practice. Inaddition, while mobile healthcare in this study is still in its early use,our focus is on exploring the purpose of its use and types of tools froma more general perspective. After moving to a more mature stage, thesupport of specific clinic tasks from some types of mobile devices mayneed to be importantly identified for understanding the specificdecisions of users' behaviors. Future research can be extended basedon the specific features for deeply exploring intention to use mobilehealthcare.
Finally, although this research has produced some interestingresults, a number of limitations may be inherent in it. Many studieshave reported that gender difference plays a moderating role in therelationship between attitude, perceived behavioral control, orsubjective norm and behavioral intention to use. This study showedthat approximately 62.9% and 37.1% of the respondents were femaleand male, respectively. The result may not appropriately reflect thepopulation distribution of gender and cause a bias against the currentfindings. However, no systematic non-response bias was reportedamong the sample respondents in regard to gender. Accordingly, thebias wasminimized in an acceptably low degree. Second, the responserate for this survey was lower than desirable, despite the variousefforts to improve it. One of the reasons for this may be due to theinexperience of the respondents in using mobile healthcare and theywere reluctant to answer the questionnaire. However, the samplerespondents reported no systematic non-response bias and were wellrepresentative of the study sample. Finally, since medical doctorsfrom larger hospitals are always quite busy, some questionnaires mayhave been completed by subordinates and therefore, the data mayhave some biases.
Appendix A. Questionnaire
Part I
Basic information
Type of hospital:□Medical center□Regional hospital□Local hospitalBed size: □b500 □500–1000 □1000–1500 □N1501Position: □Physician □NurseGender: □Female □MaleWork experience:□b5 years□5–15 years□15–25 years□N25 yearsEducation level: □High school □College □Graduate □M.D.Age:□b30 yearsold□30–40 yearsold□40–50 yearsold□N50 yearsold
Part II
Perceived usefulnessPU1 Using mobile devices for wireless healthcare would improve
my work performance.PU2 Using mobile devices for wireless healthcare would improve
my work productivity.PU3 Using mobile devices for wireless healthcare would enhance
my work effectiveness.PU4 I find mobile devices for wireless healthcare to be useful in my
job.
Perceived ease of usePEOU1 My interactionwithmobile devices for wireless healthcare is
clear and understandable.PEOU2 My interaction with mobile devices for wireless healthcare
does not require a lot of mental effort.PEOU3 It is easy to get mobile devices for wireless healthcare to do
what I want it to do.PEOU4 It is easy to use mobile devices for wireless healthcare.

595I.-L. Wu et al. / Decision Support Systems 51 (2011) 587–596
AttitudeATT1 Using mobile devices for wireless healthcare would be a good
idea.ATT2 Using mobile devices for wireless healthcare would be a wise
idea.ATT3 I like the idea of using mobile devices for wireless healthcare.ATT4 Using mobile devices for wireless healthcare would be a
pleasant experience.
Perceived behavior controlPBC1 I would be able to use mobile devices for wireless healthcare
well for my job.PBC2 Using mobile devices for wireless healthcare are entirely
within my control.PBC3 I had the resources, knowledge and ability to use mobile
devices for wireless healthcare.
Subjective normSN1 People who are important to me would think that I should use
mobile devices for wireless healthcare.SN2 People who influence me would think that I should use mobile
devices for wireless healthcare.SN3 People whose opinions are valued to me would prefer that I
should use mobile devices for wireless healthcare.
Behavioral intentionBI1 Assuming I have access to mobile devices for wireless
healthcare, I intend to use it.BI2 Given that I have access to mobile devices for wireless
healthcare, I predict that I would use it.BI3 If I have access to mobile devices for wireless healthcare, I want
to use it as much as possible.
Personal innovativeness in ITPIIT1 If I heard about a new information technology, I would look for
ways to experiment with it.PIIT2 Among my peers, I am usually the first to try out new
information technologies.PIIT3 In general, I am not hesitant to try out new information
technologies.PIIT4 I like to experiment with new information technologies.
Perceived service availabilityPSA1 I would be able to usemobile devices for wireless healthcare at
anytime, from anywhere.PSA2 I would find mobile devices for wireless healthcare easily
accessible and portable.PSA3 Mobile devices for wireless healthcare would be available to
use whenever I need it.
References
[1] R. Agarwal, J. Prasad, A conceptual and operational definition of personalinnovativeness in the domain of information technology, Information SystemsResearch 9 (2) (1998) 204–215.
[2] R. Agarwal, J. Prasad, Are individual differences germane to the acceptance of newinformation technologies? Decision Sciences 30 (2) (1999) 361–391.
[3] R. Agarwal, V. Sambamurthy, R.M. Stair, Research report: the evolvingrelationship between general and specific computer self-efficacy—an empiricalassessment, Information Systems Research 11 (4) (2000) 418–430.
[4] I. Ajzen, The theory of planned behavior, Organizational behavior and humandecision processes 50 (2) (1991) 179–211.
[5] I. Ajzen, Perceived behavioral control, self-efficacy, locus of control, and the theoryof planned behavior, Journal of Applied Social Psychology 32 (4) (2002) 665–683.
[6] H. Asada, P. Shaltis, A. Reisner, S. Rhee, R. Hutchinson, Mobile monitoring withwearable photo-plethysmographic biosensors, IEEE Engineering in Medical andBiology Magazine 22 (3) (2003) 28–40.
[7] A. Bhattacherjee, Acceptance of e-commerce services: the case of electronicbrokerages, IEEE Transactions on System, Man and Cybernetics—Part A: Systemsand Humans 20 (4) (2000) 411–420.
[8] S. Chatterjee, S. Chakraborty, S. Sarker, S. Sarker, F.Y. Lau, Examining the successfactors for mobile work in healthcare: a deductive study, Decision SupportSystems 46 (3) (2009) 620–633.
[9] P.Y.K. Chau, P.J. Hu, Information technology acceptanceby individual professionals: amodel comparison approach, Decision Sciences 32 (4) (2001) 699–719.
[10] P.Y.K. Chau, P.J. Hu, Investigating healthcare professionals' acceptance oftelemedicine technology: an empirical test of competing theories, InformationManagement 39 (4) (2002) 297–311.
[11] W.W. Chin, Issues and opinion on structural equation modeling, MIS Quarterly 22(1) (1998) 7–16.
[12] W.W. Chin, The partial least squares approach to structural equation modeling, in:George A. Marcoulides (Ed.), Modern Methods for Business Research, LawrenceErlbaum Associates, Mahwah, NJ, 1998, pp. 295–336.
[13] W.W. Chin, B.L. Marcolin, P.R. Newsted, A partial least squares latent variablemodeling approach for measuring interaction effects: results from a Monte Carlosimulation study and an electronic mail emotion/adoption study, InformationSystems Research 14 (2) (2003) 189–217.
[14] F.D. Davis, Perceived usefulness, perceived ease of use, and user acceptance ofinformation technologies, MIS Quarterly 13 (3) (1989) 319–340.
[15] F.D. Davis, R.P. Bagozzi, P.R. Warshaw, User acceptance of computer technology: acomparison of two theoretical models, Management Science 35 (8) (1989) 982–1002.
[16] P. de Toledo, S. Jimenez, F. del Pozo, J. Roca, A. Alonso, C. Hernandez, Atelemedicine experience for chronic care in COPD, IEEE Transactions on IT inBiomedicine 10 (3) (2006) 567–573.
[17] W.H. DeLone, E.R. McLean, The DeLone andMcLean model of information systemssuccess: a ten-year update, Journal of Management Information Systems 19 (4)(2003) 9–30.
[18] M. Fishbein, I. Ajzen, Belief, attitude, intention, and behavior: an introduction to theoryand research, Reading Mass, Reading Mass, Addison-Wesley, Boston, MA, 1975.
[19] L.R. Flynn, R.E. Goldsmith, A validationof theGoldsmithandHofacker innovativenessscale, Educational and Psychological Measurement 53 (4) (1993) 1105–1116.
[20] C. Fornell, D.F. Larcker, Structural equation models with unobservable variablesand measurement error: algebra and statistics, Journal of Marketing Research 18(3) (1981) 382–388.
[21] J.A. Fox-Rushby, F. Foordb, Costs, effects and cost-effectiveness analysis of amobile maternal health care service in west Kiang, the Gambia, Health Policy 35(1996) 123–143.
[22] M.J. Gallivan, The influence of software developers' creative style on their attitudes toand assimilation of a software process innovation, Information Management 40 (5)(2003) 443–465.
[23] D. Gefen, M. Keil, The impact of developer responsiveness on perceptions ofusefulness and ease of use: an extension of the technology acceptance model,ACM SIGMIS Database 29 (2) (1998) 35–49.
[24] H. Gravelle, L. Siciliani, Optimal quality, waits and charges in health insurance,Journal of Health Economics 27 (2008) 663–674.
[25] S.-J. Hong, K.Y. Tam, Understanding the adoption of multipurpose informationappliances: the case of mobile data services, Information Systems Research 17 (2)(2006) 162–179.
[26] P.J. Hu, P.Y.K. Chau, S.O.R. Sheng, K.Y. Tam, Examining the technology acceptancemodel using physician acceptance of telemedicine technology, Journal ofManagement Information Systems 16 (2) (1999) 91–112.
[27] K. Hung, Y.T. Zhang, Implementation of a WAP-based telemedicine system forpatient monitoring, IEEE Transactions on IT in Biomedicine 7 (2) (2003) 101–107.
[28] C.M. Johnson, J.P. Turley, The significance of cognitive modeling in building healthcareinterface, International Journal of Medical Informatics 75 (2006) 163–172.
[29] E. Jovanov, A. O'Donnel, A. Morgan, B. Priddy, R. Hormigo, Prolonged telemetricmonitoring of heart rate variability using wireless intelligent sensors and amobilegateway, The Second Joint IEEE EMBS/BMES Conference, 2002, pp. 1875–1876.
[30] E. Karahanna, D.W. Straub, N.L. Chervany, Information technology adoption acrosstime: a cross-sectional comparison of pre-adoption and post-adoption beliefs, MISQuarterly 23 (2) (1998) 183–213.
[31] S. Khoor, K. Nieberl, K. Fugedi, E. Kail, Telemedicine ECG-telemetry with blue toothtechnology, Proceedings of the Computers in Cardiology, 2002, pp. 585–588.
[32] I. Korhonen, J. Parkka, M. Gils, Health monitoring in the home of the future, IEEEEngineering in Medical and Biology Magazine 22 (3) (2003) 66–73.
[33] B. Langland-Orban, L.C. Gapenski, W.B. Vogel, Differences in characteristics ofhospitals with sustained high and sustained low profitability, Hospital & HealthServices Administration 41 (3) (1996) 385–399.
[34] P. Lehoux, G. Daudelin, B. Poland, G.J. Andrews, D. Holmes, Designing a betterplace for patients: professional struggle surrounding satellite and mobile dialysisunits, Social Science & Medicine 65 (2007) 1536–1548.
[35] W. Lewis, R. Agarwal, V. Sambamurthy, Sources of influence on beliefs aboutinformation technology use: an empirical study of knowledge workers, MISQuarterly 27 (4) (2003) 657–678.
[36] C. Lin,M.Chiu, C.Hsiao,R. Lee, Y. Tsai, Awirelesshealthcare eservice systemforelderlywith dementia, IEEE Transactions on IT in Biomedicine 10 (4) (2006) 696–704.
[37] K. Liszka, M. Mackin, M. Lichter, D. York, D. Pillai, D. Rosenbaum, Keeping a beat onthe heart, IEEE Pervasive Computing Magazine 3 (4) (2004) 42–49.
[38] K. Mathieson, Predicting user intentions: comparing the technology acceptance modelwith the theory of planned behavior, Information Systems Research 2 (3) (1991)173–191.
[39] G.G. Mendoza, B.Q. Tran, In-home wireless monitoring of physiological data forheart failure patients, Proceedings of the Second Joint IEEE EMBS/BMESConference, 2002, pp. 1849–1850.
[40] D.F. Midgley, G.R. Dowling, Innovativeness: the concept and its measurement,Consumer Research 4 (4) (1978) 229–242.

596 I.-L. Wu et al. / Decision Support Systems 51 (2011) 587–596
[41] A. Oztekin, F.M. Pajouh, D. Delen, L.K. Swim, An RFID network designmethodologyfor asset tracking in healthcare, Decision Support Systems 49 (1) (2010) 100–109.
[42] J.K. Pollard, S. Rohman, M.E. Fry, A web-based mobile medical monitoring system,International Workshop on Intelligent Data Acquisition and Advanced ComputingSystems: Technology and Applications, 2001, pp. 32–35.
[43] S. Rhee, B.H. Yang, K. Chang, H.H. Asada, The ring sensor: a new ambulatorywearable sensor for twenty-four hour patient monitoring, Proceedings of the 20thAnnual IEEE International Conference on Engineering in Medicine and Biology,1998, pp. 1906–1909.
[44] C.K. Riemenschneider, D.A. Harrison, P.P. Mykytyn, Understanding IT adoptiondecisions in small business: integrating current theories, Information Management40 (4) (2003) 269–287.
[45] M.E. Rogers, Diffusion of Innovations, Fifth ed, NY: Free Press, New York, 2005.[46] P. Ross, Managing care through the air, IEEE Spectrum 41 (12) (2004) 26–31.[47] M.A. Sherman, G.J. Rath, J.L. Schofer, C.W.N. Thompson, Threats to the validity of
emergency medical services evaluation: a case study of mobile intensive careunits, Medical Care 107 (2) (1979) 127–183.
[48] L. Shi, Patient and hospital characteristics associated with average length of stay,Health Care Management Review 21 (2) (1996) 46–61.
[49] V. Stanford, Using pervasive computing to deliver elder care, IEEE PervasiveComputing Magazine 1 (1) (2002) 10–13.
[50] N.J. Taylor, Public grid computing participation: an exploratory study ofdeterminants, Information Management 44 (1) (2007) 12–21.
[51] S. Taylor, P.A. Todd, Understanding information technology usage: a test ofcompeting models, Information Systems Research 6 (2) (1995) 144–176.
[52] H.H. Teo, K.K. Wei, I. Benbasat, Predicting intention to adopt interorganizationallinkages: an institutional perspective, MIS Quarterly 27 (1) (2003) 19–49.
[53] J.B. Thatcher, M.L. Loughry, J. Lim, D.H. McKnight, Internet anxiety: an empiricalstudy of the effects of personality, beliefs, and social support, InformationManagement 44 (4) (2007) 353–363.
[54] J.Y.L. Thong, An integrated model of information systems adoption in smallbusinesses, Journal of Management Information Systems 15 (4) (1999) 187–214.
[55] Y.-J. Tu, W. Zhou, S. Piramuthu, Identifying RFID-embedded objects in pervasivehealthcare applications, Decision Support Systems 46 (2) (2009) 586–593.
[56] P. Varady, Z. Benyo, B. Benyo, An open architecture patient monitoring system usingstandard technologies, IEEE Transactions on IT in Biomedicine 6 (1) (2002) 95–98.
[57] U. Varshney, Location management for mobile commerce applications in wirelessInternet, ACM Transactions on Internet Technologies 3 (3) (2003) 221–232.
[58] U. Varshney, Pervasive healthcare and wireless health monitoring, MobileNetwork Applications 12 (2–3) (2007) 113–127.
[59] V. Venkatesh, Determinants of perceived ease of use: integrating control, intrinsicmotivation, and emotion into the technology acceptance model, InformationSystems Research 11 (4) (2000) 342–365.
[60] V. Venkatesh, F. Davis, A model of the antecedents of perceived ease of use:development and test, Decision Sciences 27 (3) (1996) 451–481.
[61] V. Venkatesh, F. Davis, A theoretical extension of the technology acceptancemodel: four longitudinal field studies, Management Science 46 (2) (2000)186–204.
[62] V. Venkatesh, M. Morris, G. Davis, F. Davis, Use acceptance of informationtechnology: toward a unified view, MIS Quarterly 27 (3) (2003) 425–478.
[63] R.Walczuch, J. Lemmink, S. Streukens, The effect of service employees' technologyreadiness on technology acceptance, Information Management 44 (2) (2007)206–215.
[64] G. Walker, O. Gish, Mobile Health Services: a study in cost-effectiveness, MedicalCare 15 (4) (1977) 267–276.
[65] J. Webster, J.J. Martochhio, Microcomputer playfulness: development of ameasure with workplace implications, MIS Quarterly 16 (2) (1992) 201–226.
[66] I.L. Wu, J.L. Chen, An extension of trust and TAM model with TPB in the initialadoption of on-line tax: an empirical study, International Journal of HumanComputer Studies 62 (6) (2005) 784–808.
[67] J.H. Wu, S.C. Wang, L.M. Lin, Mobile computing acceptance factors in thehealthcare industry: a structural model, International Journal of MedicalInformatics 76 (2007) 66–77.
[68] M.Y. Yi, J.D. Jackson, J.S. Park, J.C. Probst, Understanding information technologyacceptance by individual professionals: toward an integrative view, InformationManagement 43 (3) (2006) 350–363.
Ing-Long Wu is a professor in the Department of Information Management at NationalChung Cheng University. He gained a Bachelor in Industrial Management from NationalCheng-Kung University, a M.S. in Computer Science fromMontclair State University, and aPh.D. in Management from Rutgers, the State University of New Jersey. He has published anumber of papers in Journal of American Society for Information Science and Technology,Information & Management, Decision Support Systems, International Journal of HumanComputer Studies, Electronic Commerce Research and Applications, Behavior andInformation Technology, Information and Software Technology, Psychometrika, AppliedPsychological Measurement, and Journal of Educational and Behavioral Statistics. Hiscurrent research interests are in the areasof CRM, SCM, knowledgemanagement, evaluationof IT performance, and behaviors in IT usage.
Jhao-Yin Li is a research assistant in the Insititute of Information Science at AcademiaSinica inTaiwan.He received aBachelor degree in Statistics fromFu JenCatholicUniversityand a MBA in Information Management from National Chung Cheng University. He haspublished a number of papers inhealthcare sector. His current research interests are in theareas of IT adoption behaviors and knowledge management.
Chu-Ying Fu is a senior lecturer in the Department of Information Management atWuFeng Institute of Technology in Taiwan. She received aBachelor degree in PublicHealthfrom China Medical University and a M.S. in Computer Science from West MichiganUniversity. Her current research interests are in the areas of IT interaction behaviors and ITsystem design.
Recommended