The Respiratory System

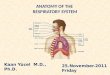
ANATOMY OF THE RESPIRATORY SYSTEM

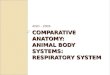
The Respiratory Tract:
The Lungs
Alveoli
TABLE OF CONTENT

1) Respiratory Tract:Nose through bronchi 2) The lungs.
THE RESPIRATORY SYSTEM CONSISTS OF:

The respiratory tract
further divided into the upper and lower respiratory tract

The upper respiratory tract from the nose through the pharynx

The lower respiratory tract (The Bronchial Tree)
from the larynx to tertiary bronchi

The Bronchial Tree

Alveoli
The Bronchial Tree Extends to Bronchioles and Alveoli

Bronchioles and Alveoli

Cartilage Plates
No Cartilage but Smooth Muscles
Bronchioles
Cartilage Ring
asthmaattack

Cross Section Longitudinal Section
Ciliary Lining of the Lower Respiratory Tract
Cilia

Electron Micrograph of Cilia

The cilia beat upward and drive the debris-laden mucus to the pharynx, where it is swallowed.

THE LUNGS

The Lungs overlap with the respiratory tract.
Secondary Bronchi
Tertiary Bronchi
Bronchioles
Alveoli
Bronchioles
Alveoli
Primary Bronchi
Inside Lungs

THE LUNGS
- consist of the left and the right lungs
- The left lung is divided into two lobes; the right into three.
- receives the
bronchus, blood
and lymphatic
vessels, and nerves
through its hilum.
- The bronchi
extend into alveoli

ALVEOLI

~700 SF surface area

Alveoli consists of :
1) type I alveolar cells (95%), thin
2) type II alveolar cells (5%), secrete surfactant.
3) macrophages (dust cells), defense

- Each alveolus is surrounded with a basket of capillaries.

surrounded with capillaries

The respiratory membrane:
1) the wall of the alveolus
2) the endothelial wall of the capillary
3) their fused basement membranes

Alveoli contain elastic fibers which helps expiration.

Low blood pressure keeps alveoli dry.

Gas exchange occurs only in alveoli.

Dead Space
- starts from nose to terminal bronchiole
- where there is no gas exchange
- ~ 150 mlterminal bronchiole

The Respiratory Tract:
The Lungs
Alveoli
ANATOMY OF THE RESPIRATORY SYSTEM
SUMMARY

ventilation
gas exchange
transport by blood
gas exchange

MECHANICS OF VENTILATION

Driving Force for Air Flow
Resistance to Airflow
Measurements of Ventilation
Alveolar Ventilation
TABLE OF CONTENTS

Terms:
inspiration or inhalation: breathing in
expiration or exhalation: breathing out

Driving Force for Air Flow
Airflow driven by the pressure difference between atmosphere (barometric pressure) and inside the lungs (intrapulmonary pressure).
760 mmHg

atmospheric pressure = 760 mmHg
Before inspiration

atmospheric pressure = 760 mmHg

atmospheric pressure = 760 mmHg

atmospheric pressure = 760 mmHg

Mechanism for the Change in Intrapulmonary pressure
Boyle’s Law:
Volume x Pressure = Constant
gas
P V

Volume Pressure Volume Pressure
Inspiration: Expiration:

Volume Pressure Volume Pressure
Inspiration: Expiration:
Can the lungs expand/shrink by
themselves?

1) The Diaphragm
2) External Intercostal Muscles
3) Internal Intercostal Muscles
4) The Abdominal Muscles
- the principal muscle of inspiration
- pulls the diaphragm down, increasing all three dimensions of the thoracic cage.
Major Respiratory Muscles
1) The Diaphragm
2) External Intercostal Muscles
- Inspiration muscles
- increases the anteroposterior and transverse dimensions of the chest.
1) The Diaphragm
2) External Intercostal Muscles
3) The Abdominal Muscles
- Expiration muscles
- pulls the diaphragm up, reducing the vertical dimension of the thoracic cage.
1) The Diaphragm
2) External Intercostal Muscles
3) The Abdominal Muscles
4) Internal Intercostal Muscles
- Extra Expiration muscles

Coupling Between Lungs and Thoracic Cage

Visceral pleura covers the surface of each lung; parietal pleura lines the chest cavity.
- The lungs and thoracic cage are coupled by the pleurae.
pleural cavity
- The two pleurae form the pleural cavity.
- The pleural fluid serves to reduce friction during chest expansion.
- Intrapleural pressure: The pressure in the pleural cavity is negative.

Parietal pleura visceral pleura
Potential pleural cavity(negative intrapleural pressure)
lung
The thoracic cage is larger than the natural size of the lungs.
Generation of the negative intrapleural pressure

Parietal pleura visceral pleura
Potential pleural cavity(negative intrapleural pressure)
air
air
pneumathorax
lung

Conclusion
Lungs Thoracic Cagepleurae- pressure

Inspiration
Contraction of1) diaphragm
2) external intercostal muscles
The lungs are carried along.
Lung volume
pressure
Air flows in.
active

passive
Resting Expiration
Relaxation of1) diaphragm
2) external intercostal muscles
The lungs shrink.
Lung volume
pressure
Air flows out.

Forced Expiration
Relaxation of1) diaphragm 2) external
intercostal musclesand
Contraction ofabdominal, internal intercostal and other accessory respiratory
muscles.
Lung volume
pressure
Air flows out.
active

Driving Force for Air Flow
Atmosphere-lung pressure gradient
Major respiratory muscles
Coupling between lungs and thoracic cage
SUMMARY

Resistance to Airflow

TABLE OF CONTENTS Resistance
1) Alveolar Surface Tension
2) Elastic Resistance
3) Airway Resistance
Compliance

1) Alveolar Surface Tension
- generated by a thin film of liquid over the surface of alveolar epithelium,
- tends to cause a collapse of the alveoli,
- Resists against inspiration.

Alveoli
Alveolar surface tension is a resistance against inspiration.

- Surface tension is reduced by surfactant. ( type II alveolar epithelial cells)
Pre-term infants don't have enough surfactant.
type II surfactant

Resistance 1) Alveolar Surface Tension
2) Elastic Resistance
3) Airway Resistance- Against inspiration due to elastic fibers in the lungs and chest wall,
- Increases in pulmonary fibrosis.

Resistance 1) Alveolar Surface Tension
2) Elastic Resistance
3) Airway Resistance- Due to friction, affected by airway caliber.
- Against inspiration and expiration!
- Increases during asthma attack (smooth muscle contraction in bronchiole.

Resistance 1) Alveolar Surface Tension
2) Elastic Resistance
3) Airway Resistance
Compliance
- The reciprocal of resistance,
- An indicator of ease with which the lungs expand.

Measurements of Ventilation using Spirometer


Dead Space
inspiration expiration
Alveolar ventilation rate =(tidal volume – dead space) x resp freq (/min)

Restrictive disorders - (pulmonary fibrosis)
- compliance & vital capacity.
Changes in Spirometric Measures

- No change in respiratory volumes
- FEV1.
one-second forced expiratory volume
Obstructive disorders
Changes in Spirometric Measures

MECHANICS OF VENTILATION
SUMMARY
Driving Force for Air Flow
Resistance to Airflow
Measurements of Ventilation
Alveolar Ventilation

NEURAL CONTROL OF VENTILATION

Rhythm?

1) inspiratory center
- stimulates inspiration muscles.
2) expiratory center
- inhibits the inspiratory center,
- stimulates expiration muscles.
Center in the medulla oblongata

The pons fine-tunes ventilation.

Afferent Connections to the Respiratory Centers
the limbic system
Hypothalamus
Chemoreceptors the lungs

Chemoreceptor-initiated Reflexes
Peripheral chemoreceptors
- aortic and carotid bodies,
- monitor O2, CO2 and pH of the blood.
Central chemoreceptors
- close to the surface of the medulla oblongata,
- monitor the pH of the cerebrospinal fluid.

O2, CO2, or pH
stimulate chemoreceptors
reflex
frequency and depth of respiration
CHEMORECEPTOR-MEDIATED REFLEX

Voluntary Control
- the motor cortex,
- bypass the brainstem
respiratory centers,
- limited voluntary control.

GAS EXCHANGE in the LUNGS

ventilation
gas exchange
transport by blood
gas exchange

- The gas exchange between
alveolar air and the blood is via
diffusion of O2 and CO2.
- Diffusion of a gas is driven
by O2 and CO2 partial
pressure gradient.
PO2 = 40 mmHgPCO2 = 46 mmHg
PO2 = 104 mmHgPCO2 = 40 mmHg

The partial pressure of a gas refers to the share of the total pressure generated by a mixture of gases.
O2 CO2
N2
H2O
Total = 760 mmHg
5.3%40 mmHg
13.6%104 mmHg

PO2 = 40 mmHgPCO2 = 46 mmHg
PO2 = 104 mmHgPCO2 = 40 mmHg
Oxygen and carbon dioxide cross the respiratory membrane and the air-water interface easily.

Overview of Gas Exchange in the Lungs

Factors That Affect the Efficiency of Alveolar Gas Exchange
1. partial pressure
2. solubility
3. respiratory membrane thickness/area
4. ventilation-perfusion coupling

O2
CO2
N2
O2 CO2
N2
H2O
Total = 760 mmHgTotal = 760 mmHg
Air
a) High altitudeb) Hyperbaric chamberc) Obstructive disease
PO2104 mmHgPCO2 40 mmHg
1) Partial pressure

CO2 has a higher solubility than O2.
CO2 O2
Pressure Gradient 6 mmHg 64 mmHg
PO2104 mmHgPCO2 40 mmHg
2) Solubility
PO2 40 mmHgPCO2 46 mmHg
1) Partial pressure

2) Solubility
1) Partial pressure
3) Respiratory membrane thickness/area

4) Ventilation-perfusion Coupling
- average V-P ratio = 0.8
- autoregulated by:
2) Solubility
1) Partial pressure
3) Respiratory membrane thickness/area
PO2 and PCO2
causes:1) vasoconstriction of
pulmonary arterioles2) dilation of bronchioles

summary
1) Driving force for gas exchange
2) Factors that affect the efficiency of alveolar gas exchange

Gas transport by the blood

TABLE OF CONTENT
1) Carbon Dioxide Transport
2) Oxygen Transport

7% dissolved in the blood as a gas,
23% as carbamino-hemoglobin,
70% as carbonic acid in the plasma.
Carbon Dioxide Transport

Oxygen Transport
- About 98.5% of O2 in the blood are carried by hemoglobin.
- The rest is physically dissolved in plasma.

Blood Oxygen Content
- average 20 ml/dL
- determined by:
1) saturation of hemoglobin
2) content of hemoglobin
HypoventilationCO poisoning
anemia
Hypoxemia

Carbon monoxide competes with oxygen for hemebinding with a much higher affinity.
Problem: deoxygenate hemoglobin
Treatment: hyperbaric oxygen chamber

GAS EXCHANGE in the TISSUES
1. Carbon Dioxide Loading 2. Oxygen Unloading
How to dissociate?
O2

O2
PO2 dissociation
PCO2 dissociation
pH dissociation
DPG dissociation
(2,3-diphosphoglycerate)
Temperature dissociation
Dissociation of O2 from hemoglobin (HB) is affected by:

O2High PO2, low PCO2
association with HG
favor the loading of O2
In Lungs
100% saturated

High PCO2, low PO2,
low pH, DPG
dissociation of O2
from HG
favor the unloading
O2
In tissues

High PCO2, low PO2,
low pH, DPG
dissociation of O2
from HG
favor the unloading
O2
In tissues

Utilization Coefficient
- The amount of oxygen uptake by tissue versus the arterial blood oxygen content
blood
20 ml O2/dL
cellcell
cell cell cell
Utilization Coefficient = 4.4 ml / 20 ml = 22%
15.6 ml O2/dL
4.4 ml O2/dL

Function of Oxygen ?

with oxygenwithout oxygen
glucose
2 ATP 38 ATP

Can human beings produce oxygen?

Oxygen Toxicity
- Excessive oxygen generates hydrogen peroxide and free radicals, which destroy enzymes and damage nervous tissue.
- Oxidative toxicity with aging.

Hypercapnia
- PCO2 < 37 mmHg - caused by hyperventilation
Hypocapnia
- PCO2 > 43 mmHg - caused by hypoventilation (respiratory diseases)

Summary of the Respiratory System

ventilation
gas exchange
transport by blood
gas exchange

Oxyhemoglobin Dissociation Curve

Oxygen Dissociation & Temperature
Active tissue - more O2 released
PO2 (mmHg)

Oxygen Dissociation & pH
Bohr effect: release of O2 in response to low pH
Active tissue - more O2 released
Recommended