Embed Size (px)
DESCRIPTION
Citation preview

ELECTROCARDIOGRAM

ELECTROCARDIOGRAM
The electrocardiogram (ECG) is an extracellular recording of electrical events occurring within the heart.
PLAN: – the methods used for measuring the electrical
activity– the cause of changes in the recorded electrical
activity– the basics of interpreting the normal ECG – electrical manifestations of abnormal electrical
activity

The ECG triaxial lead system
• All of the electrical fluctuations that occur during a cardiac cycle can be measured and recorded and comprise the electrocardiogram.
• The measuring device is an electrocardiograph.
• A complete clinical ECG uses both bipolar and unipolar leads.

Willem Einthoven
1893 Willem Einthoven introduces the term 'electrocardiogram' at a meeting of the Dutch Medical Association.
1885The first accurate recording of the electrocardiogram and its development as a clinical tool. Einthoven, using an improved electrometer, distinguishes five deflections which he names P, Q, R, S and T.
1924 Willem Einthoven wins the Nobel prize for inventing the electrocardiograph.

Willem Einthoven

The ECG triaxial lead system
• The heart (like the strip of cardiac muscle) is immersed in a volume conductor (body fluids), which will transmit any electrical activity from the source to the surface of the body.
• If the small electrical signal is amplified, the deflections can be measured using an appropriate recording device.

The ECG triaxial lead system
• The first such recordings were accomplished by Einthoven, who envisioned the heart as a current generator located at the center of an equilateral triangle.
• The corners of the triangle (in the frontal plane) are on the right and left shoulders and the symphysis pubis, and form a 60o angle between the adjacent sides of the triangle.

The ECG triaxial lead system• The limbs are continuous
with these sites and are more convenient attachment points.
• Therefore, Einthoven used the limbs as attachment points for his Limb Leads, of which there are three, all bipolar.

Triaxial Lead System
• Lead I records the potential difference between the left arm (+) and the right arm (-).
• Lead II measures the potential difference between the left leg (+) and right arm (-), and
• Lead III measures the difference between the left leg (+) and left arm (-).

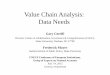
CARDIAC VECTORSA. Initial depolarization is from left to right in the interventricular septum (arrow 1). The head of the arrow represents the + end of the dipole so the recorded deflection is downward (moving away from + end of lead I).

CARDIAC VECTORS
B. The base of the septum is now depolarized; the wave spreads down the septum and from endo- to epicardium (arrow 2); the dipole is moving neither toward nor away from + pole of Lead I (recorder=0).

CARDIAC VECTORS
C. The right ventricle is now depolarized (it is thinner than the left, therefore there is less mass), the left ventricular mass is still depolarizing (arrow 3). The positive end of dipole is moving toward the positive pole of Lead I, therefore the deflection is positive.

CARDIAC VECTORS
D. Most of both ventricles are depolarized; the dipole is moving toward the base of the left ventricle (arrow 4) perpendicular to Lead I (neither toward nor away from). The recording is 0.

CARDIAC VECTORS
E. The last portion of the myocardium to depolarize (in this example) is the base of the posterior aspect of the left ventricle (arrow 5). The positive end of the dipole is moving away from the positive pole of Lead I. The deflection will be negative. When depolarization is complete, there will be no dipole and the recorder registers 0.

VECTOR LOOPS
The concept of instantaneous vectors is valuable because it helps visualize the spread of depolarization through the ventricular mass. If additional vectors at shorter time intervals (msec for instance) are examined (figure A), sequential instantaneous vectors 1-14 might occur if depolarization followed that path.

VECTOR LOOPS
Connecting the heads of the arrows representing these instantaneous vectors inscribes what is referred to as a vector loop, which indicates the path the wave takes (in this case). Other vector loops in the frontal plane might look like those shown in figure B.

THE MEAN ELECTRICAL AXIS
OF THE HEART
Resolving all of the instantaneous vectors yields a mean vector, which is the average direction the wave of depolarization takes as it travels through the ventricles. In the figure, panels C-E depict the graphic resolution of individual vectors 1 and 2 to produce the resultant vector (R). This vector yields information concerning direction and magnitude (the length of the arrow is proportional to the size of the dipole or mass). In panel E, the magnitude of vectors 1 and 2 is equal and they are progressing in opposite directions. Therefore, they cancel one another (R=0). The vector depicted in panel F is an estimate of the resolution of all the vectors.

HEXAXIAL (SIX) LEAD SYSTEM
• Leads I-III provide information concerning events occurring only in the frontal plane of the body.
• Other leads are also used, which provide additional information concerning electrical activity as it spreads through the heart.
• The “V” leads are unipolar leads that compare voltage at the active electrodes with ground or zero.

HEXAXIAL (SIX) LEAD SYSTEM
The first three V leads to consider are those that bisect the 60o angles formed by Einthoven's three Limb Leads. The V lead bisecting the 60o angle between Leads I and III (figure A) is designated VL. The signal as originally measured was small and needed to be amplified or augmented and the lead is now designated aVL ('a' for augmented). The other leads are aVR (augmented V lead, right arm) and aVF (augmented V lead, foot).

HEXAXIAL (SIX) LEAD SYSTEM
The resultant vector would manifest itself on the hexaxial (six) lead system as follows: Lead I - 0 Lead II - upright Lead III - upright aVL - negative aVR - negative aVF - positive

AXIS OF ROTATION
The mean electrical axis of the heart, or angle of the mean electrical vector, is expressed in degrees as shown in the figure (sign indicates polarity of the lead, not direction of rotation). Thus the vector used in the previous example would be at 90o and fall within the normal range of rotation (between -30o and +110o). A resultant vector pointing directly to the left (3 o'clock position) would have an angle of rotation of 0o.

CHEST LEADS
The remaining six leads are recorded on the chest and are designated as V leads, V1-V6. The approximate position of these leads is shown in the figure A. The leads are unipolar and provide information concerning electrical activity of the heart in the transverse plane of the thorax.

CHEST LEADS
Envision the heart located in the center of a cylinder, with a wave of depolarization moving through the ventricles (figure B). With reference to this figure, and recalling that the active or exploring lead is at the position indicated, you should be able to predict whether the deflection will be upright or negative.


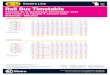
The Normal ECG • The upright or downward
deflection associated with ventricular depolarization provides information regarding the direction of depolarization, but there is much more to be gleaned from a recording of the ECG.
• Timing is everything, and how quickly (or slowly) the wave spreads through the heart yields information regarding the status of the muscle itself and of the conduction system.


The Normal ECGThe various waves and their causes are as follows:
• The P wave - caused by depolarization of the atria.
• The QRS complex (the shape will depend on the Lead being recorded) - caused by depolarization of the ventricles.
• The T wave - caused by repolarization of the ventricles.
Atria repolarize while the QRS is occurring, so no wave is evident.


The Normal ECG
PR interval
(0.12 - 0.21 sec)
The time required for depolarization to travel from the SA through the AV Node (in reality this is the P-Q interval).

The Normal ECG
QRS interval
(0.08-0.1 sec).
The time it takes for ventricles to depolarize.

The Normal ECG
The ST segment (duration variable). The interval when the ventricles are depolarized (loosely corresponds to phase 2 of the intracellular action potential).

The Normal ECG
QT interval (duration is variable). The interval from the beginning of ventricular depolarization to the end of ventricular repolarization.

The Normal ECG

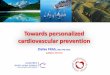
The Normal ECG
• This recording is made on a grid so that timing can be accurately determined. The grid is structured so that each small block is equal to 0.04 sec and 5 blocks are set off by heavy lines (not shown), which is therefore equal to 0.2 sec.
• A 1 millivolt calibration signal is also included to compare voltages generated by the heart (increased mass is proportional to increased amplitude of the QRS complex because the dipole is larger).


The Normal 12 Lead ECG
The general appearance of a recording from an individual with normal electrical activity illustrates a normal sinus rhythm in Leads I-III, in which P waves precede the QRS complex, a normal P-R interval (Augmented Leads) of 0.16 sec, normal QRS duration (V1-V5), of 0.08 sec, and normal voltage of approximately 1 mV.

Left Ventricular Hypertrophy

ECG criteria for LVH• Normal thickness of the left ventricular
myocardium is from 0.6 to 1.1 cm (as measured at the very end of diastole).
• There are several sets of criteria used to diagnose LVH:
The Sokolow-Lyon index:- S in V1 + R in V5 or V6 (whichever is larger) ≥ 35 mm - R in aVL ≥ 11 mm
The Cornell criteria:- S in V3 + R in aVL > 28 mm (men) - S in V3 + R in aVL > 20 mm (women)

ARRHYTHMIAS • Under normal resting
conditions, the 'P' cells in the SA node reach threshold (and elicit an action potential) approximately 70 times per minute.
• The action potential is transmitted throughout the heart via the conduction system. If this is a regular occurrence, and every ventricular depolarization is preceded by atrial depolarization, the heart is said to have a sinus rhythm (the pacemaker is in the SA node).

Arrhythmias
• If the occurrence is irregular, but originates in the SA node, a sinus arrhythmia exists (Normal vs Sinus Arrhythmia ) Occasionally these pacemaker cells in the SA node reach threshold at a much slower rate and a sinus bradycardia may ensue (rate <60 beats per minute).
• Conversely, if the rhythm established by the 'P' cells is abnormally high (rate>100 beats per minute) a sinus tachycardia is said to exist.
• A 'normal' or sinus rhythm exists if the pacemaker is located in the SA node and the rate is between 60 and approximately 100 per minute.

AV block
First degree AV block
The PR interval exceeds 0.21 sec, but a P wave always precedes a QRS complex.


AV block
Second degree AV blockSome of the action potentials transit the AV node, some do not; a regular ratio exists, such as 2P's:1QRS; 3P's:1QRS, etc. (thus, 2:1, 3:1, 3:2, etc. AV block).


AV block
Third degree AV blockThere is no relationship between P waves and QRS complexes (also called complete heart block). A pacemaker develops in the ventricles and atria and ventricles each set their own rate, since no action potentials originating in the atria can get to the ventricles.

Complete AV block

Ectopic PacemakersIf the most rapid diastolic depolarization rate originates outside the SA node (sinus rhythm) or the AV node (nodal rhythm), an ectopic focus is said to exist. It can arise anywhere in the heart where the tissue has become hyperexcitable due to hypoxia, drugs, etc. This may lead to atrial fibrillation, a condition where small islands of atrial muscle (a few cells) behave independently of others (there may be thousands of such foci).

Ectopic Pacemakers• There is no synchronous depolarization (thus
no detectable P wave) and action potentials reach the AV node at completely random intervals. This causes a very erratic ventricular rhythm, with constantly changing R-R intervals.
• The rhythm is irregularly irregular, i.e., completely unpredictable (Atrial Fibrillation sound ).
• It may compromise ventricular pumping function, but is compatible with life.

Ectopic Pacemakers
If ventricular fibrillation occurs, however, it is fatal unless quickly stopped (defibrillation is accomplished). If an ectopic focus develops in the ventricular muscle, the shape of the QRS complex is usually bizarre, because depolarization occurs over aberrant pathways. An ectopic focus in the conduction system itself will produce a normal QRS complex because conduction time is normal. An occasional depolarization originating in the ventricle is referred to as a PVC Sound (premature ventricular contraction, a misnomer), whereas a run of such beats, if they occur in rapid succession, is referred to as paroxysmal ventricular tachycardia.

Conduction Defects of the His-Purkinje System
There may develop in the conduction system a Bundle Branch Block (BBB), which prevents the action potential from passing through that particular piece of tissue. As a result, the tissue distal to the block will not depolarize via the normal pathway, nor will the normal timing of depolarization occur.


Conduction Defects of the His-Purkinje System
The block may occur in the right bundle branch (RBBB), the left bundle branch (LBBB), or may only involve the anterior or posterior fascicles of the left bundle branch (hemiblock). The result is that
• a) activation of the ventricle distal to the block is delayed (the QRS duration increases),
• b) the mean electrical axis (vector) of the heart is shifted to the side of the block.


CLINICAL SIGNIFICANCE

THERE ARE 4 PRINCIPALECG INDICATORS OF ACUTE INFARCTION
1. ST segment elevation
2. T wave inversion 3. Development of
Q waves 4. Reciprocal ST
segment depression.



Thank YouFor YourAttention!